What is peristalsis
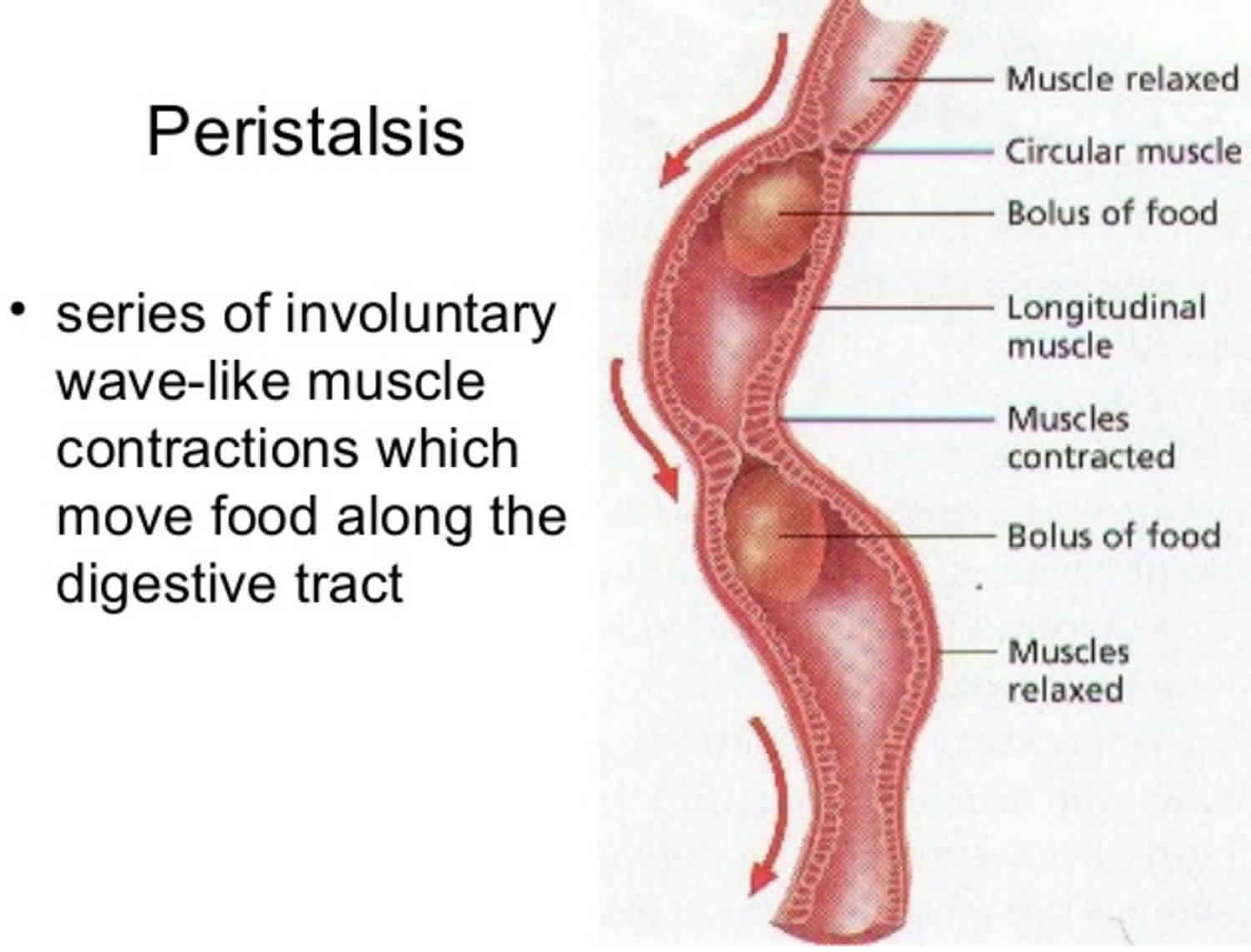
Peristalsis is the rhythmic motion of smooth muscles in the intestine or other tubular organs characterized by the alternate contraction and relaxation of the smooth muscles that propel the contents onward. Peristalsis is also described as a wavelike ring of contraction that moves material along the digestive tract or the alimentary canal. In peristalsis, a ring of contraction occurs in the wall of the tube. At the same time, the muscular wall just ahead of the ring relaxes. As the peristaltic wave moves along the tube, it pushes the tubular contents ahead of it (see Figure 1). Generally, in peristalsis, the area ahead of the contents is relaxed, and the area behind the contents is undergoing peristaltic contraction which allows for the contents to be propelled forward. In much of a digestive tract such as the human gastrointestinal tract, smooth muscle tissue contracts in sequence to produce a peristaltic wave, which propels a ball of food (called a bolus while in the esophagus and upper gastrointestinal tract and chyme in the stomach) along the tract. Peristaltic movement comprises relaxation of circular smooth muscles, then their contraction behind the chewed material to keep it from moving backward, then longitudinal contraction to push it forward.
Smooth Muscle Cells
There are two major types of smooth muscle: multiunit and visceral. In multiunit smooth muscle, the muscle cells are separate rather than organized into sheets. Smooth muscle of this type is found in the irises of the eyes and in the walls of blood vessels. Typically, multiunit smooth muscle tissue contracts only in response to stimulation by neurons or certain hormones.
Visceral smooth muscle is composed of sheets of spindle-shaped cells in close contact with one another. This more common type of smooth muscle is found in the walls of hollow organs, such as the stomach, intestines, urinary bladder, and uterus.
Visceral smooth muscle displays rhythmicity, a pattern of repeated contractions. Rhythmicity is due to self-exciting cells that deliver spontaneous impulses periodically into surrounding muscle tissue. When one cell is stimulated, the impulse may excite adjacent cells, which in turn stimulate still others. These two features—rhythmicity and transmission of impulses from cell to cell—are largely responsible for the wavelike motion, called peristalsis, that helps force the contents of certain tubular organs along their lengths. Peristalsis occurs in other tubular structures, such as the gastrointestinal tract from the esophagus to the anus and the ureters, bile ducts, and uterine tubes; in the esophagus peristalsis is controlled by the medulla oblongata. For example, distension of the esophagus with food or the colon with feces, evokes peristalsis (a wave of contraction) that propels the contents along the esophagus (see Figures 2 and 3).
Smooth muscle exhibits a reaction called the stress–relaxation (or receptive-relaxation) response. When stretched, it briefly contracts and resists, but then relaxes. The significance of this response is apparent in the urinary bladder. If the stretched bladder contracted and did not soon relax, it would expel urine almost as soon as it began to fill, thus failing to store the urine until an opportune time.
Figure 1. Peristalsis
Peristalsis function
Peristalsis is an automatic and important process. Peristalsis moves:
- Food through the digestive system.
- Urine from the kidneys into the bladder
- Bile from the gallbladder into the duodenum
Peristalsis is a normal function of the body. Peristalsis can sometimes be felt in your belly (abdomen) as gas moves along.
Where does peristalsis occur?
Esophageal peristalsis
Presence of a bolus (ball of food) in the pharynx triggers receptors which relay signals that eventually induce esophageal peristalsis and LES (lower esophageal sphincter) relaxation. After food is chewed into a bolus, it is swallowed and moved through the esophagus. During swallowing (deglutition) food moves through the esophagus into the stomach via peristalsis. Smooth muscles contract behind the bolus to prevent it from being squeezed back into the mouth. Then rhythmic, unidirectional waves of contractions work to rapidly push the food into the stomach. The migrating motor complex helps trigger peristaltic waves. This process works in one direction only and its sole esophageal function is to move food from the mouth into the stomach (the migrating motor complex also functions to clear out remaining food in the stomach to the small bowel, and remaining particles in the small bowel into the colon) 1.
In the esophagus, two types of peristalsis occur:
- First, there is a primary peristaltic wave, which occurs when the bolus enters the esophagus during swallowing. The primary peristaltic wave forces the bolus down the esophagus and into the stomach in a wave lasting about 8–9 seconds. The wave travels down to the stomach even if the bolus of food descends at a greater rate than the wave itself, and continues even if for some reason the bolus gets stuck further up the esophagus.
- In the event that the bolus gets stuck or moves slower than the primary peristaltic wave (as can happen when it is poorly lubricated), stretch receptors in the esophageal lining are stimulated and a local reflex response causes a secondary peristaltic wave around the bolus, forcing it further down the esophagus, and these secondary waves continue indefinitely until the bolus enters the stomach. The process of peristalsis is controlled by the medulla oblongata. Esophageal peristalsis is typically assessed by performing an esophageal motility study.
During vomiting, the propulsion of food up the esophagus and out the mouth comes from contraction of the abdominal muscles; peristalsis does not reverse in the esophagus.
Figure 2. Esophageal peristalsis
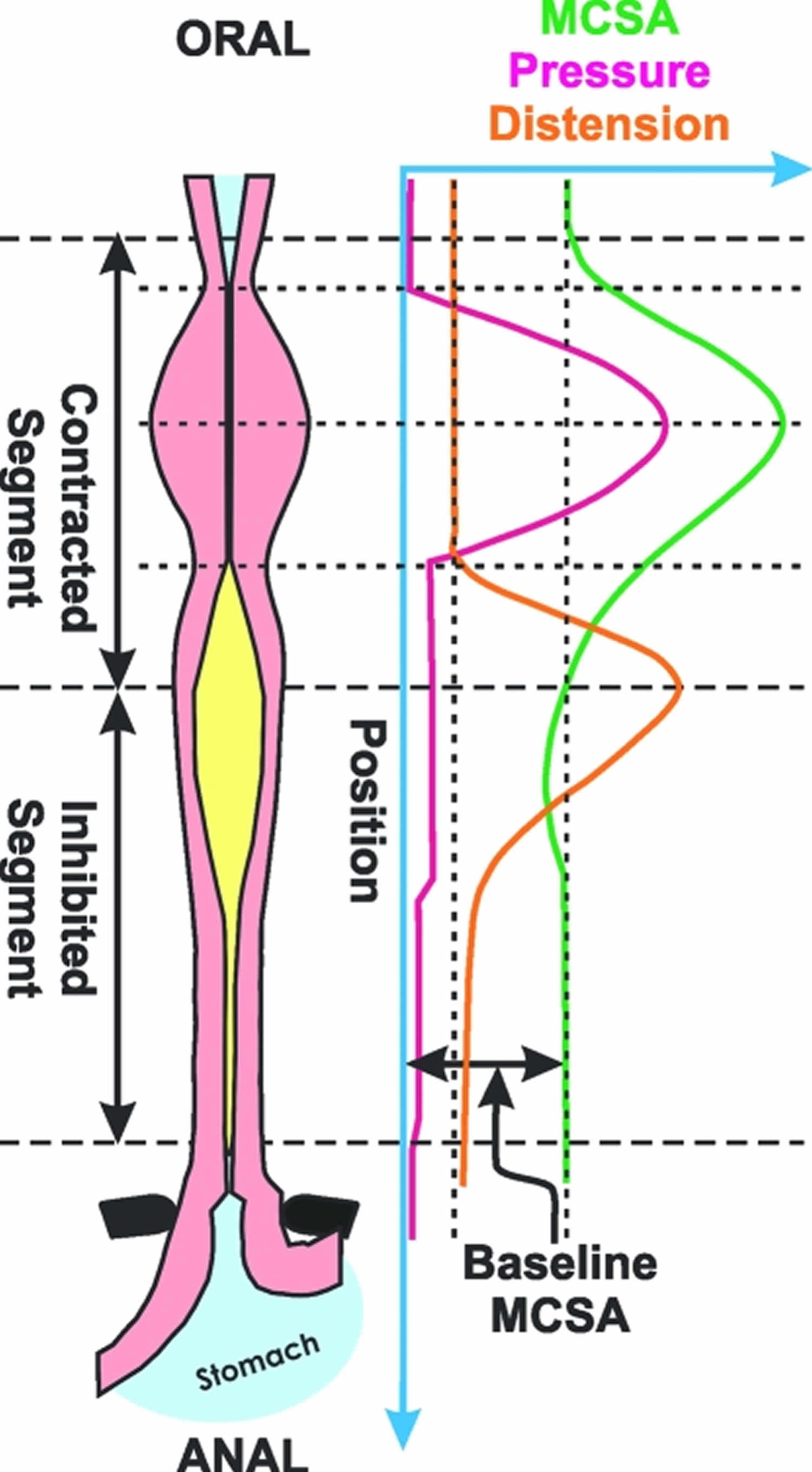
Footnote: Schematic of contraction and distension during swallow-induced peristalsis. Note that the pressure and muscle cross-sectional area (MCSA), surrogate markers of circular and longitudinal muscle contractions, respectively, precede distension. The latter marches distally in front of the onset of contraction wave in a peristaltic fashion.
[Source 2 ]Figure 3. Esophageal peristalsis
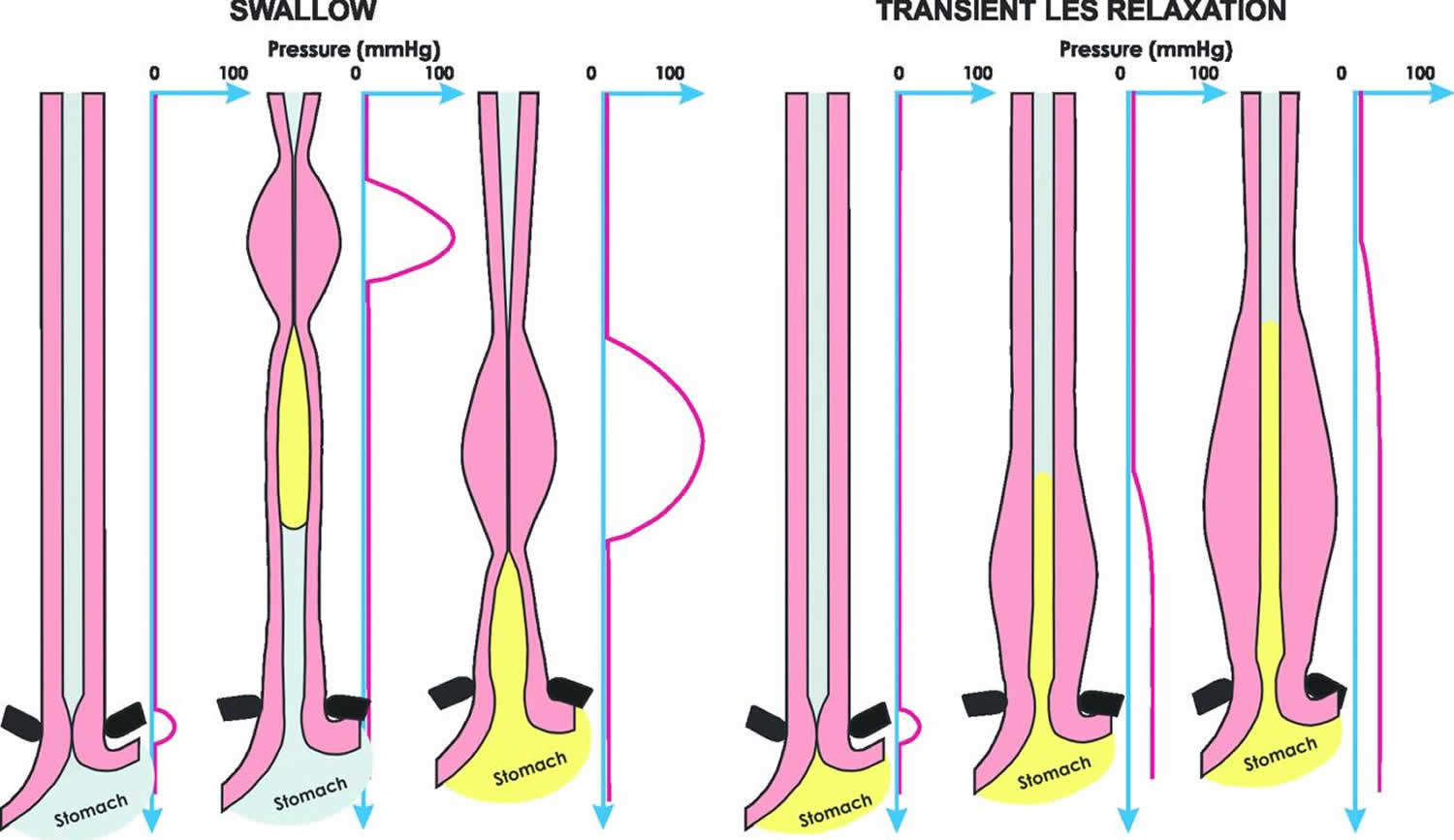
Footnote: Patterns of longitudinal muscle contraction during peristalsis and transient LES (lower esophageal sphincter) relaxation. Peristaltic contraction is associated with an aborally traversing simultaneous contraction of the circular and longitudinal muscle of the esophagus. On the other hand, transient lower esophageal sphincter relaxation is associated with contraction of the longitudinal muscle of the distal esophagus, in the absence of circular muscle contraction.
[Source 3 ]Gastric peristalsis
The emptying of your stomach results from a grinding and pumping action consisting of rings of circular smooth muscle contractions that propagate from the main body (corpus) to the antrum, pushing digesta into the duodenum 4. This process has been described as gastric peristalsis 5 and occurs also in isolated preparations of stomach 6. The gastric contractions are generated by slow waves in the smooth muscle, which occur in the absence of neural activity and are thus regarded as myogenic 4. The source of myogenic activity in the digestive tract has been tracked down to the interstitial cells of Cajal, which act as pacemakers, generating slow waves in the smooth muscle 7.
Gastric emptying depends on functional coupling of slow waves between the corpus and antrum, to allow slow waves initiated in the gastric corpus to propagate to the pyloric sphincter and generate gastric peristalsis 8.
In intact stomach the circular smooth muscle contractions propagate anally at speeds of millimeters per second, whereas the contraction appears quasi-instantaneously around the circumference, propagating at speeds of centimeters per second 4. The anal propagation has been explained by the well-established mechanism of coupled pacemakers entrained by the higher oral frequencies. Gastric slow waves in the corpus have the highest frequency and quite surprisingly, appear to be generated by the interstitial cells of Cajal in the circular smooth muscle 9. Given that signals within the interstitial cells of Cajal in the circular smooth muscle propagate at similar milimeter per second speeds in all directions 10, a major question arises as to how signals from the network of pacemaker cells generate both anal propagation at low speed and circumferential propagation at a higher speed. An additional path of conduction of signals in the circumferential direction was suspected to be at play to generate the full spatio-temporal pattern of gastric peristalsis 11.
In summary, Edwards and Hirst 12 concluded that the anal propagation of the ring contractions in the antrum occurs by propagation of signals within the interstitial cells of Cajal in the smooth muscle network, with concomitant generation of slow waves in the underlying circular smooth muscle of the antrum at the greater curvature. In turn the slow waves, generated in the circular smooth muscle, are subsequently conducted circumferentially at a much faster speed via the circular muscle bundles and their interstitial cells of Cajal in the circular smooth muscle, to produce ring contractions. The signals that are still propagated circumferentially within the interstitial cells of Cajal in the myenteric plexus layer appear to be redundant or ineffective.
Small intestine
Once processed and digested by the stomach, the milky chyme is squeezed through the pyloric sphincter into the small intestine.
The two types of movements occur in the small intestine—segmentations and a type of peristalsis called migrating motility complexes—are governed mainly by the myenteric plexus.
- Segmentation is a type of peristalsis with alternating contractions of circular smooth muscle fibers that produce segmentation and resegmentation of sections of small intestine; mixes chyme with digestive juices and brings food into contact with mucosa for absorption.
- Migrating motility complex is a type of peristalsis with waves of contraction and relaxation of circular and longitudinal smooth muscle fibers passing the length of the small intestine; moves chyme toward ileocecal sphincter.
Segmentations are localized, mixing contractions that occur in portions of intestine distended by a large volume of chyme. Segmentations mix chyme with the digestive juices and bring the particles of food into contact with the mucosa for absorption; they do not push the intestinal contents along the tract. A segmentation starts with the contractions of circular muscle fibers in a portion of the small intestine, an action that constricts the intestine into segments. Next, smooth muscle fibers that encircle the middle of each segment also contract, dividing each segment again. Finally, the smooth muscle fibers that first contracted relax, and each small segment unites with an adjoining small segment so that large segments are formed again. As this sequence of events repeats, the chyme sloshes back and forth. Segmentations occur most rapidly in the duodenum, about 12 times per minute, and progressively slow to about 8 times per minute in the ileum. This movement is similar to alternately squeezing the middle and then the ends of a capped tube of toothpaste.
After most of a meal has been absorbed, which lessens distension of the wall of the small intestine, segmentation stops and peristalsis begins. The type of peristalsis that occurs in the small intestine, termed a migrating motility complex, begins in the lower portion of the stomach and pushes chyme forward along a short stretch of small intestine before dying out. The migrating motility complex slowly migrates down the small intestine, reaching the end of the ileum in 90–120 minutes. Then another migrating motility complex begins in the stomach. Altogether, chyme remains in the small intestine for 3–5 hours.
Large intestine
The passage of chyme from the ileum into the cecum is regulated by the action of the ileocecal sphincter. Normally, the valve remains partially closed so that the passage of chyme into the cecum usually occurs slowly. Immediately after a meal, a gastroileal reflex intensifies peristalsis in the ileum and forces any chyme into the cecum. The hormone gastrin also relaxes the sphincter. Whenever the cecum is distended, the degree of contraction of the ileocecal sphincter intensifies.
Movements of the colon begin when substances pass the ileocecal sphincter. Because chyme moves through the small intestine at a fairly constant rate, the time required for a meal to pass into the colon is determined by gastric emptying time. As food passes through the ileocecal sphincter, it fills the cecum and accumulates in the ascending colon.
One movement characteristic of the large intestine is haustral churning. In this process, the haustra remain relaxed and become distended while they fill up. When the distension reaches a certain point, the walls contract and squeeze the contents into the next haustrum. Peristalsis also occurs, although at a slower rate (3–12 contractions per minute) than in more proximal portions of the tract. A final type of movement is mass peristalsis, a strong peristaltic wave that begins at about the middle of the transverse colon and quickly drives the contents of the colon into the rectum. Because food in the stomach initiates this gastrocolic reflex in the colon, mass peristalsis usually takes place three or four times a day, during or immediately aft er a meal.
Lymphatic system
The human lymphatic system has no central pump. Instead, lymph circulates through peristalsis in the lymph capillaries, as well as valves in the capillaries, compression during contraction of adjacent skeletal muscle, and arterial pulsation.
Sperm
During ejaculation, the smooth muscle in the walls of the vas deferens contracts reflexively in peristalsis, propelling sperm from the testicles to the urethra 13.
- Marieb, Elaine N. & Hoehn, Katja “Human Anatomy & Physiology” 8th Ed., Benjamin Cummings/Pearson, 2010[↩]
- Abrahao et al., Neurogastroenterol Motility 2010 Nov 17; doi: 10.1111/j.1365-2982.2010.01624[↩]
- Babaei et al., Gastroenterology 2008;134:1322–31.[↩]
- Costa M. All together now: from pacemakers to gastric peristalsis. J Physiol. 2006;571(Pt 1):1. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1805650/[↩][↩][↩]
- Sanders KN, Publicover NG. Handbook of Physiology, Section 6 The Gastrointestinal System. Part 1. Bethesda, MA: Americal Physiological Society; 1989. pp. 187–216.[↩]
- Video-based spatio-temporal maps for analysis of gastric motility in vitro: effects of vagal stimulation in guinea-pigs. Berthoud HR, Hennig G, Campbell M, Volaufova J, Costa M. Neurogastroenterol Motil. 2002 Dec; 14(6):677-88.[↩]
- A case for interstitial cells of Cajal as pacemakers and mediators of neurotransmission in the gastrointestinal tract. Sanders KM. Gastroenterology. 1996 Aug; 111(2):492-515.[↩]
- Forrest AS, Hennig GW, Jokela-Willis S, Park CD, Sanders KM. Prostaglandin regulation of gastric slow waves and peristalsis. Am J Physiol Gastrointest Liver Physiol. 2009;296(6):G1180-90. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2697952/[↩]
- Atypical slow waves generated in gastric corpus provide dominant pacemaker activity in guinea pig stomach. Hashitani H, Garcia-Londoño AP, Hirst GD, Edwards FR. J Physiol. 2005 Dec 1; 569(Pt 2):459-65.[↩]
- Propagation of pacemaker activity in the guinea-pig antrum. Hennig GW, Hirst GD, Park KJ, Smith CB, Sanders KM, Ward SM, Smith TK. J Physiol. 2004 Apr 15; 556(Pt 2):585-99.[↩]
- Regional variation in contribution of myenteric and intramuscular interstitial cells of Cajal to generation of slow waves in mouse gastric antrum. Hirst GD, Beckett EA, Sanders KM, Ward SM. J Physiol. 2002 May 1; 540(Pt 3):1003-12.[↩]
- An electrical analysis of slow wave propagation in the guinea-pig gastric antrum. Edwards FR, Hirst GD. J Physiol. 2006 Feb 15; 571(Pt 1):179-89.[↩]
- William O. Reece (21 March 2013). Functional Anatomy and Physiology of Domestic Animals. John Wiley & Sons. pp. 451–. ISBN 978-1-118-68589-1.[↩]





{kind=link}