What is pilomatrixoma
Pilomatrixoma also called pilomatricoma or ‘calcifying epithelioma of Malherbe’ is an uncommon, benign (harmless) hair follicle tumor derived from hair matrix cells. Pilomatrixoma usually manifests as a solitary, asymptomatic, firm nodule.
Pilomatrixoma is most often diagnosed in young children but may also affect adults 1. Pilomatrixoma appears to be slightly more common in females than males.
Recommended treatment is surgical excision. Multiple pilomatrixomas have been observed, mainly in association with myotonic dystrophy 2. Pilomatrix carcinoma is a rare condition 3.
What is pilomatrixoma carcinoma?
Pilomatrixoma carcinoma or pilomatrix carcinoma is a rare hair follicle tumor that occurs from a malignant transformation of a benign pilomatricoma. It wasn’t until 1980 when a review of several cases of biologically aggressive pilomatrixoma confirmed the malignant transformation of these normally benign tumors. Since then there have only been about 90 reported cases of pilomatrix carcinoma. Some of these cases of pilomatrix carcinoma have arisen as a solitary lesion de novo. There is a high risk of recurrence after surgical excision and malignant features are often found in recurrent lesions.
Other names for pilomatrix carcinoma include pilomatricarcinoma and or pilomatrical carcinoma.
Lesions of pilomatrix carcinoma are often found on the head and neck regions and vary in size from 1-10 cm. Unlike their benign counterpart where lesions are most often diagnosed in young children of both sex, the malignant variety is twice as likely to appear in white middle-aged men.
Lung metastases has been described and may occur years after the initial diagnosis.
How is pilomatrixoma carcinoma diagnosed?
Although pilomatrix carcinoma share some histological features with benign pilomatrixoma, they may also have the following additional features:
- Frequent and abnormal mitosis
- Central or intratumoral necrosis
- Infiltration of skin and soft tissue
- Infiltration of blood and lymphatic system
The diagnosis of pilomatrix carcinoma is based on histological examination and the presence of the additional features from skin biopsy.
A MRI scan (magnetic resonance imaging) of the lesion may be required to determine the local spread of the tumour. Palpation of lymph nodes and a CT scan may also be performed to search for lung and liver metastases.
What is the treatment of pilomatrixoma carcinoma?
Due to the potential for metastasis to various sites, complete surgical excision with wide margins (2-3cm) is the recommended treatment. Mohs micrographic surgery may be used to ensure better margin control. Incomplete resections have led to local recurrences.
Adjuvant radiotherapy also has been used, but potential benefits are not well defined.
What causes pilomatrixoma?
The cause of pilomatrixoma is now known to be due to a localized mutation in a hair matrix cell. An overactive proto-oncogene called BCL-2 suggests the normal process of cell death is suppressed, and mutations in CTNNB1 in most cases suggest loss of regulation of a protein complex called beta-catenin/LEF-1.
More recently, investigators have demonstrated that the proliferating cells of human pilomatrixomas show prominent staining with antibodies directed against LEF-1 (a marker for hair matrix cells). Evidence also indicates that S100 proteins can be used as biochemical markers in characterization of pilomatrixomas 4. These data provide biochemical support of morphological evidence that these tumors are derived from hair matrix cells. Furthermore, investigators have shown that at least 75% of persons with pilomatrixomas who have examined have mutations in the gene CTNNB1; these data directly implicate beta-catenin/LEF-1 misregulation as the major cause of hair matrix cell tumorigenesis in humans 5.
Pilomatrixoma signs and symptoms
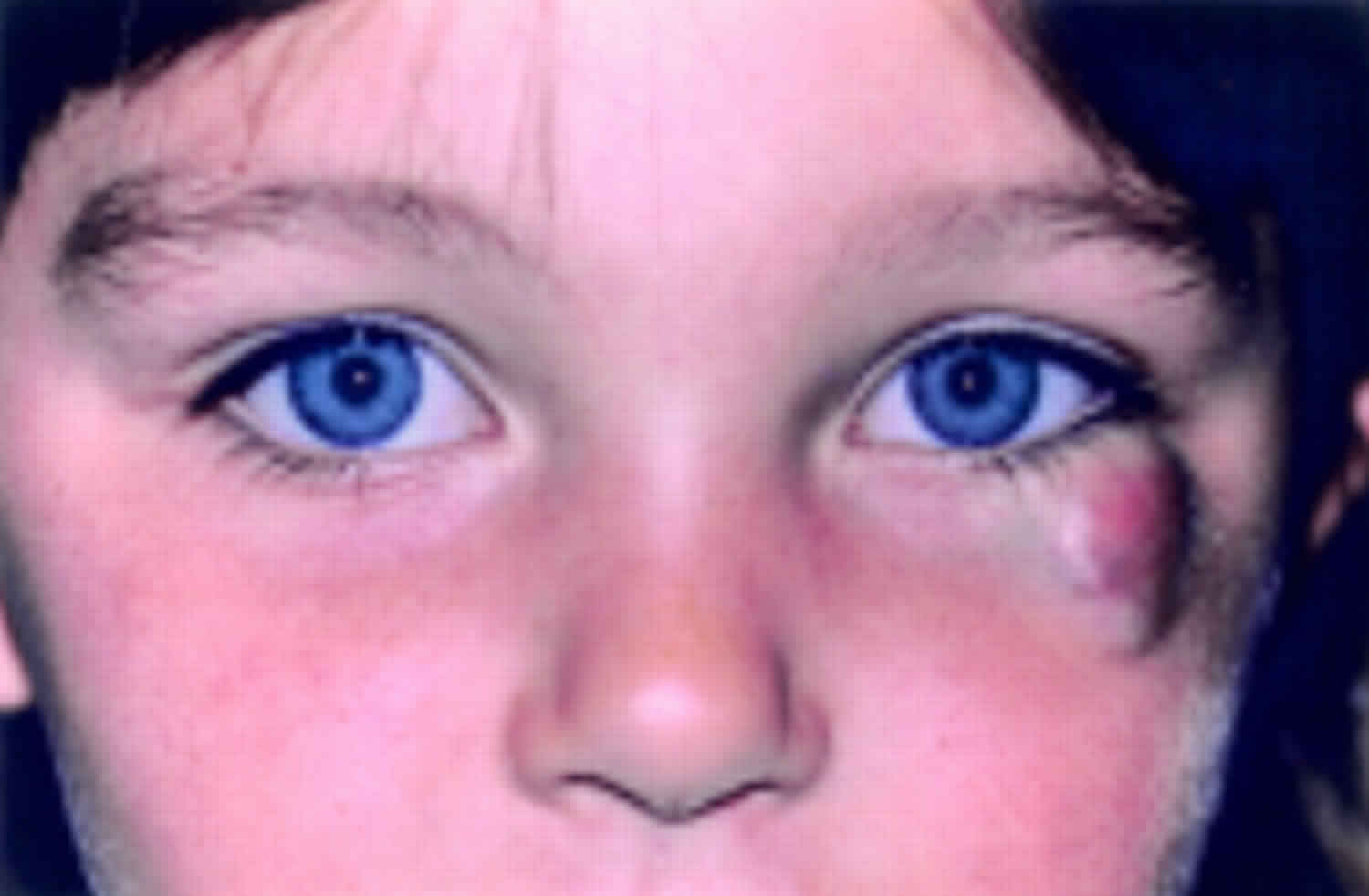
Pilomatrixoma presents as a single skin-colored or purplish lesion. Patients usually present with a solitary nodule that has been slowly growing over several months or years. Patients are usually asymptomatic, but some report pain during episodes of inflammation or ulceration. Rapid growth is rare, but reports indicate one lesion reaching 35 mm in 8 months and another reaching 1 cm in 2 weeks. Occurrence in more than one member of the same family is rare and is usually observed in association with myotonic dystrophy.
- They are usually found on the head and neck, but they may occur on any site.
- They don’t usually cause any symptoms, but they may be tender.
- They may be skin colored, white or red.
- They may be regular or irregular in shape.
- Most pilomatrixomas are 5–10 mm in diameter.
- They may remain stable for years or slowly grow in size up to several centimeters in diameter.
- Pilomatrixoma is characterized by calcification within the lesion, which makes it feel hard and bony, and often results in an angulated shape (the ‘tent’ sign).
Approximately 50% of the lesions occur on the head and neck, especially the cheek, preauricular area, eyelids, forehead, scalp, and lateral and posterior neck 6. Eyelid lesions may mimic chalazion 7. Lesions can also occur on the upper and lower extremities and trunk 8. One lesion was observed in the middle ear and another in the ovary 9.
Most lesions measure 0.5-3 cm, but, rarely, giant lesions up to 15 cm are reported. Patients usually have a single, firm, stony, hard nodule. Lesions are usually the color of the normal skin, but reddish-purple lesions have been observed (probably resulting from hemorrhage). Stretching of the overlying skin can give the lesion a multifaceted, angulated appearance known as the “tent sign,” likely due to calcification in the lesion.
One lesion showed the “dimple sign,” which is often associated with dermatofibromas. Unusual morphological variants include perforating, cystic, bullous, lymphangiectatic, hornlike, keratoacanthomalike, pigmented, and lesions that show anetodermalike changes on the surface 10.
Pilomatrixoma complications
Complications of pilomatrixoma are rare. However, occasionally they grow to giant size (several centimeters in diameter), and pilomatrixoma carcinoma (cancer) has been very rarely reported.
A few cases have been reported of multiple pilomatrixomas in association with the rare neurological condition myotonic dystrophy. Individual cases have also been reported of pilomatrixomas arising in patients with a variety of other genetic disorders. The vast majority are not associated with any other abnormality.
How is the diagnosis of pilomatrixoma made?
If pilomatrixoma is suspected, dermoscopy may be helpful, showing a central whitish or grayish-blue structureless area. Erythema and telangiectasia are sometimes observed.
If the nature of the skin lesions is uncertain, ultrasound scan may be recommended. The scan of pilomatrixoma is described as a doughnut within the dermis (mid layer of the skin) with a tail (the tail denotes calcification). Alternatively, the calcification may be detected by X-ray.
A biopsy will help to establish the cause of the lesion. Alternatively the whole lesion can be removed, providing both diagnosis and treatment. The histology of pilomatrixoma is striking. It may show a sharply demarcated tumor surrounded by a fibrous capsule or a poorly demarcated tumor without capsule. There are darkly stained ‘basophilic’ cells and ‘shadow’ cells with missing nuclei. Calcium deposits are found in most lesions.
Pilomatrixoma treatment
Pilomatrixomas are usually surgically excised. They do not disappear by themselves, and if incompletely removed, they may recur.
Pilomatrixoma prognosis
Pilomatrixomas are not associated with mortality. Very large tumors (≤ 18 cm) can cause considerable discomfort but are uncommon 11. Pilomatrix carcinomas are also uncommon, but they are locally invasive and can cause visceral metastases and death.
- Demircan M, Balik E. Pilomatricoma in children: a prospective study. Pediatr Dermatol. 1997 Nov-Dec. 14(6):430-2.[↩]
- Geh JL, Moss AL. Multiple pilomatrixomata and myotonic dystrophy: a familial association. Br J Plast Surg. 1999 Mar. 52(2):143-5.[↩]
- Sable D, Snow SN. Pilomatrix carcinoma of the back treated by mohs micrographic surgery. Dermatol Surg. 2004 Aug. 30(8):1174-6.[↩]
- Kizawa K, Toyoda M, Ito M, Morohashi M. Aberrantly differentiated cells in benign pilomatrixoma reflect the normal hair follicle: immunohistochemical analysis of Ca-binding S100A2, S100A3 and S100A6 proteins. Br J Dermatol. 2005 Feb. 152(2):314-20.[↩]
- Lazar AJ, Calonje E, Grayson W, et al. Pilomatrix carcinomas contain mutations in CTNNB1, the gene encoding beta-catenin. J Cutan Pathol. 2005 Feb. 32(2):148-57.[↩]
- Rotenberg M, Laccourreye O, Cauchois R, Laccourreye L, Putterman M, Brasnu D. Head and neck pilomatrixoma. Am J Otolaryngol. 1996 Mar-Apr. 17(2):133-5.[↩]
- Hada M, Meel R, Kashyap S, Jose C. Eyelid pilomatrixoma masquerading as chalazion. Can J Ophthalmol. 2017 Apr. 52 (2):e62-e64.[↩]
- Schweitzer WJ, Goldin HM, Bronson DM, Brody PE. Solitary hard nodule on the forearm. Pilomatricoma. Arch Dermatol. 1989 Jun. 125(6):828-9, 832.[↩]
- Alfsen GC, Strom EH. Pilomatrixoma of the ovary: a rare variant of mature teratoma. Histopathology. 1998 Feb. 32(2):182-3.[↩]
- Fender AB, Reale VF, Scott GA. Anetodermic pilomatricoma with perforation. J Am Acad Dermatol. 2008 Mar. 58(3):535-6.[↩]
- Pilomatrixoma. https://emedicine.medscape.com/article/1058965-overview[↩]





{kind=link}