
What is pleurisy
Pleurisy also called pleuritis is an inflammation of the pleura, a large, thin sheet of tissue that wraps around the outside of your lungs and lines the inside of your chest cavity (Figures 1 and 2) 1, 2. These two large, thin layers of tissue called the pleura separate your lungs from your chest wall. One layer wraps around the outside of the lungs (visceral pleura). The other layer lines the inner chest wall (parietal pleura). The visceral pleura does not contain pain receptors, whereas the parietal pleura is innervated by somatic nerves that sense pain due to trauma or inflammation. Between these two layers is a very thin space called the pleural space, that’s usually filled with a very small amount of fluid that helps the two layers of the pleura glide smoothly past each other as your lungs breathe air in and out. The layers act like two pieces of smooth satin gliding past each other, allowing your lungs to expand and contract when you breathe without any resistance from the lining of the chest wall. Pleurisy occurs when the two layers of the pleura become irritated and inflamed, rubbing against each other like two pieces of sandpaper, producing sharp chest pain when you inhale and exhale. Pleuritic pain is usually worse when you breathe or cough and lessens or stops when you hold your breath. Pleurisy is usually caused by a chest infection – either a viral infection such as influenza or a bacterial infection such as pneumonia. Other causes of pleurisy include autoimmune diseases such as rheumatoid arthritis and systemic lupus erythematosus (SLE), heart and lung diseases, with 30% to 40% of cases classified as idiopathic or unknown cause 3.
Studies of pleuritic chest pain have shown that pulmonary embolism is the most common life-threatening cause and the source of the pain 5% to 21% of the time 4, 5. A recent prospective trial of 7,940 patients evaluated for pulmonary embolism revealed that pleuritic-type chest pain was significantly associated with confirmed pulmonary embolism 6. The most commonly occurring symptoms of pulmonary embolism were shortness of breath (dyspnea) and pleuritic chest pain in 73% and 66% of patients, respectively 4.
Pleuritic pain occurs in nearly 90% of patients with pneumothorax and 50% of those with community-acquired pneumonia 7. A recent study revealed that when surgical pleural biopsy is used to investigate the cause of pleurisy, 56% of cases are attributed to neoplastic diseases, including mesothelioma (23%), lung cancer (16%), and lymphoma (2.5%) 8. Infectious diseases account for 24%, with tuberculosis leading at 16.2%, followed by parapneumonic pleural effusion (3.6%), empyema (3.5%), nontuberculous mycobacteriosis (0.5%), and paragonimiasis or lung fluke disease, a parasitic infection caused by eating raw or undercooked crabs or crayfish containing lung fluke (trematode) larvae, most commonly Paragonimus westermani (0.1%). Autoimmune diseases account for 2.8% of pleural biopsy findings, with rheumatoid arthritis (1.3%) and systemic lupus erythematosus (SLE) (0.3%) being the most common 8. Pleurisy is the initial symptom in 10% of systemic lupus erythematosus (SLE) patients and occurs at some stage in 40% to 60% systemic lupus erythematosus (SLE) patients. Symptomatic pleurisy is also relatively common in rheumatoid arthritis; while 70% of patients show pleural effusion in autopsy studies, only 3% to 5% experience symptoms 9, 10, 11. Recent studies indicate that the lymph nodes and pleura are the most commonly involved extrapulmonary sites in tuberculosis 7, 12, 13.
The main symptom of pleurisy is a sharp or stabbing knife-like pain in your chest that gets worse when you breathe in deeply, cough, sneeze or laugh. The pain may stay in one place or it may spread to your shoulder or back. Sometimes it becomes a fairly constant dull ache. Depending on what’s causing the pleurisy, you may have other symptoms, such as:
- Shortness of breath
- A cough
- Fever and chills
- Rapid, shallow breathing
- Unexplained weight loss
- A sore throat followed by pain and swelling in your joints
Some people also get a pleural effusion, which is when the inflammation causes a large build-up of fluid between the linings of the lung and chest wall.
This can help relieve the symptoms of pleurisy because the linings no longer rub against each other. However, it can also cause compression of the lungs, leading to breathing problems.
Treatment of pleurisy involves pain control and treating the underlying cause. For example, if bacterial pneumonia is the cause, an antibiotic can be prescribed to manage the infection. If the cause is a viral infection, pleurisy may go away on its own.
The pain and inflammation associated with pleurisy is usually treated with nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen (Advil, Motrin IB, others). Occasionally, your doctor may prescribe corticosteroid medication. Corticosteroids should be reserved for patients who are intolerant of nonsteroidal anti-inflammatory drugs (NSAIDs). Corticosteroids are also used in the treatment of tuberculous pleurisy and have been shown to result in some reduction in effusions and symptoms, but they have not demonstrated improvements in mortality 14.
The outcome of pleurisy treatment depends on the seriousness of the underlying cause. Early diagnosis and treatment of the condition that caused pleurisy can help you feel better. Depending on the cause and the condition, you may make a full recovery.
Figure 1. Pleuritic chest pain diagnostic algorithm
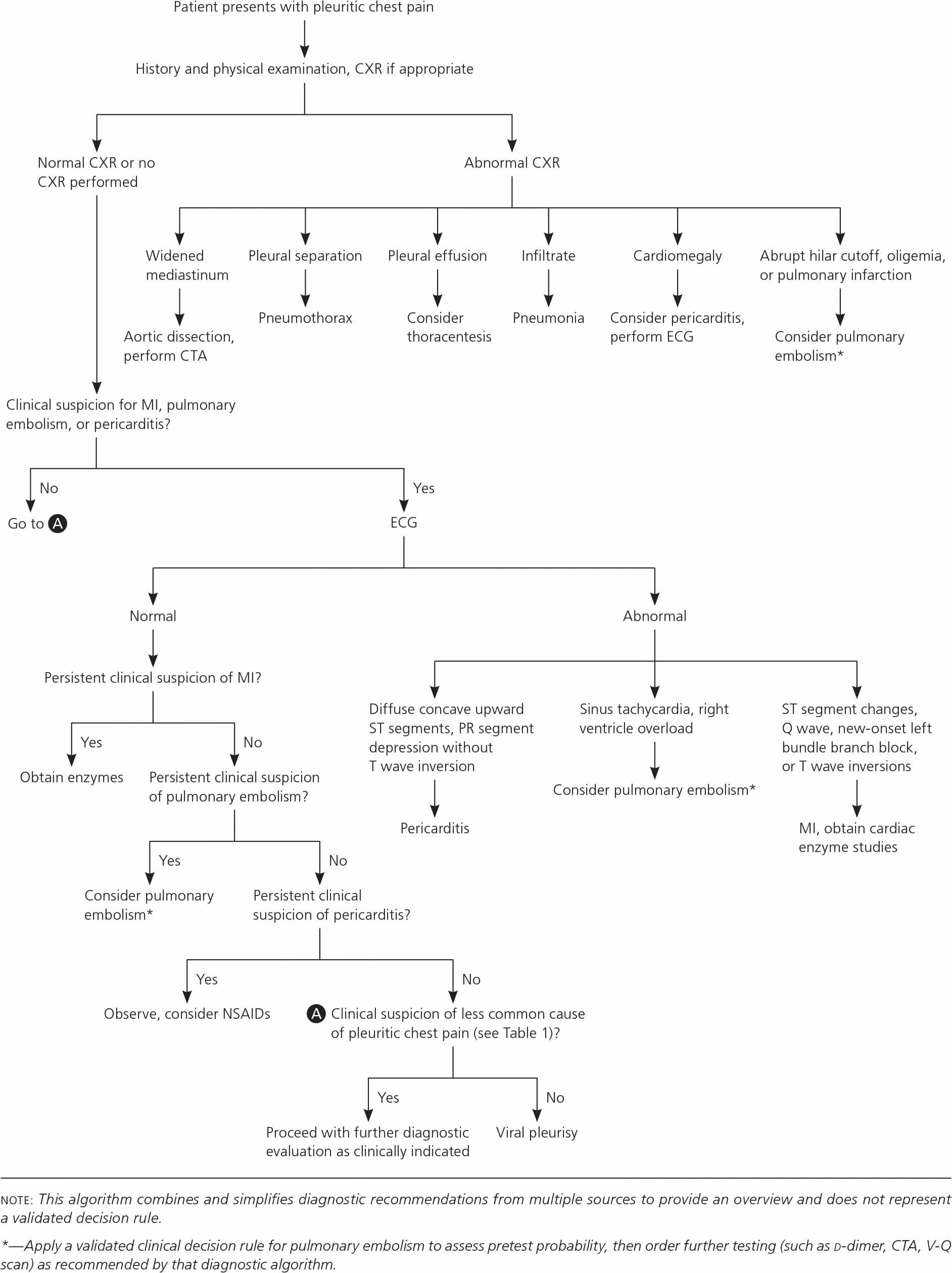
Abbreviations: CTA = computed tomography angiography; CXR = chest radiography; ECG = electrocardiography; MI = myocardial infarction; NSAID = nonsteroidal anti-inflammatory drug; V-Q = ventilation-perfusion.
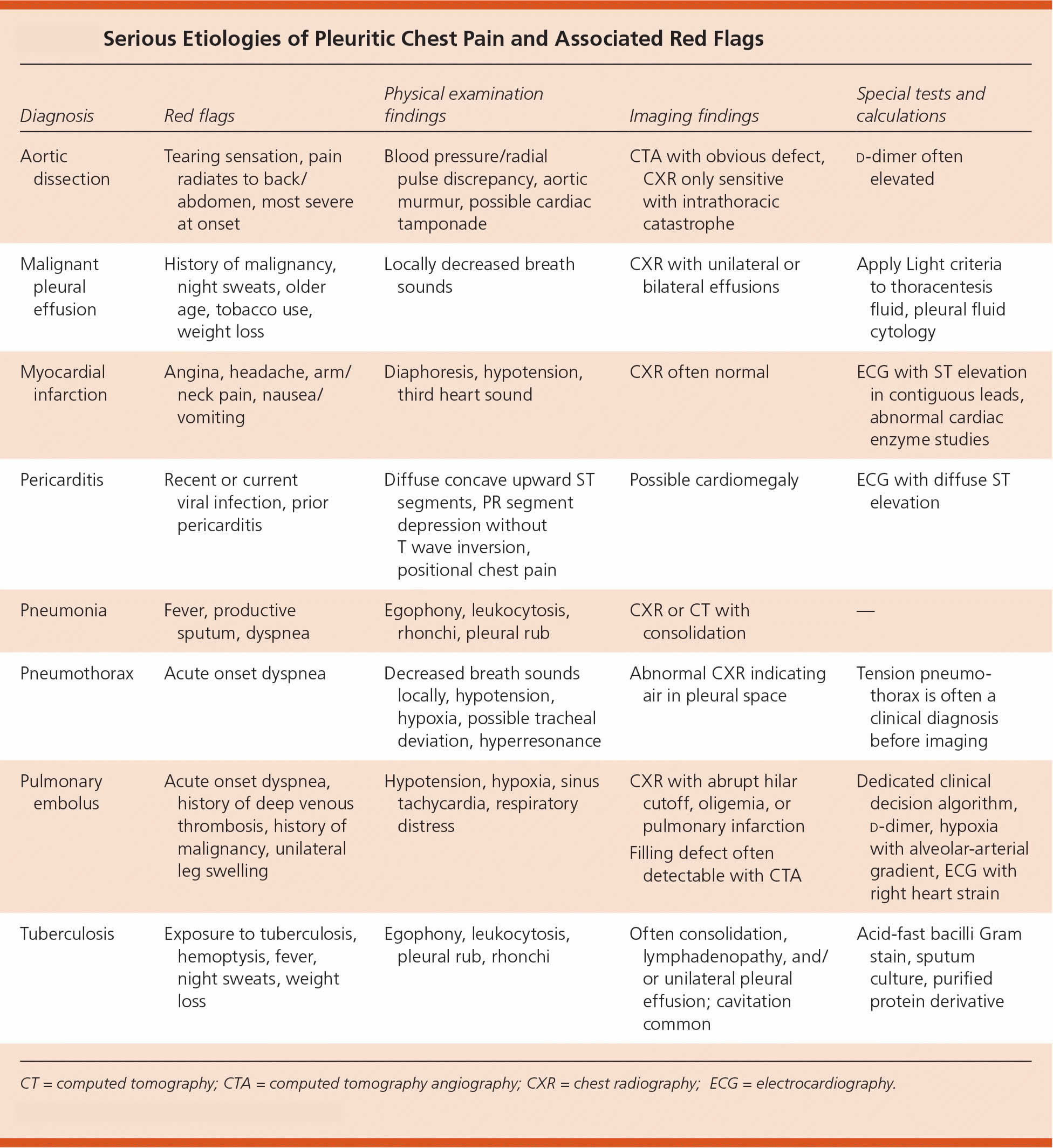
[Source 2 ]Figure 2. Pleuritic chest pain life-threatening causes and red flags
How do you get pleurisy?
You can get pleurisy when inflammation from your lungs — caused by a virus, bacteria or other illness — moves into your pleural space (the potential space between the two layers of the pleura, visceral and parietal pleura that surrounds the lungs), causing them to swell up and rub against each other. This can also happen if there’s a blockage like a tumor or damage to your lung.
Is pleurisy contagious?
Depends on the cause of your pleurisy. Pleurisy caused by the flu or bacterial infection is contagious.
Who does pleurisy affect?
Anyone can get pleurisy, but you’re at a higher risk if you:
- Are over 65.
- Have a condition that causes inflammation in your body like an autoimmune disease (a disease in which your immune system mistakenly attacks your own healthy cells, tissues, and organs, leading to inflammation and damage in your body).
- Take medications that cause inflammation in your body.
- Have tumors or scarring in your lungs.
How serious is pleurisy?
Pleurisy can be mild or very serious. It depends on what’s causing it and whether you have additional complications.
Can pleurisy go away on its own?
If pleurisy is caused by a virus, it can go away on its own as you get over being sick. More serious underlying causes such as cancer or other illnesses need to be treated before pleurisy will get better.
How long does pleurisy last?
Recovery and how long does pleurisy last depends on the cause of the pleurisy. In most cases of pleuritic chest pain from viral infection, pain and symptoms will resolve within two to four weeks.
Health problems that may develop from pleurisy include:
- Breathing difficulty
- Fluid buildup between chest wall and lung (pleural effusion)
- Complications from the original illness.
Can you get pleurisy more than once?
Yes. If you have an illness that puts you at risk for pleural inflammation, you might get pleurisy more than once.
Human lungs
The lungs are soft, spongy, cone-shaped organs in the thoracic (chest) cavity. The lungs consist largely of air tubes and spaces. The balance of the lung tissue, its stroma, is a framework of connective tissue containing many elastic fibers. As a result, the lungs are light, soft, spongy, elastic organs that each weigh only about 0.6 kg (1.25 pounds). The elasticity of healthy lungs helps to reduce the effort of breathing.
The left and right lungs are situated in the left and right pleural cavities inside the thoracic cavity. They are separated from each other by the heart and other structures of the mediastinum, which divides the thoracic cavity into two anatomically distinct chambers. As a result, if trauma causes one lung to collapse, the other may remain expanded. Below the lungs, a thin, dome-shaped muscle called the diaphragm separates the chest from the abdomen. When you breathe, the diaphragm moves up and down, forcing air in and out of the lungs. The thoracic cage encloses the rest of the lungs.
Each lung occupies most of the space on its side of the thoracic cavity. A bronchus and some large blood vessels suspend each lung in the cavity. These tubular structures enter the lung on its medial surface.
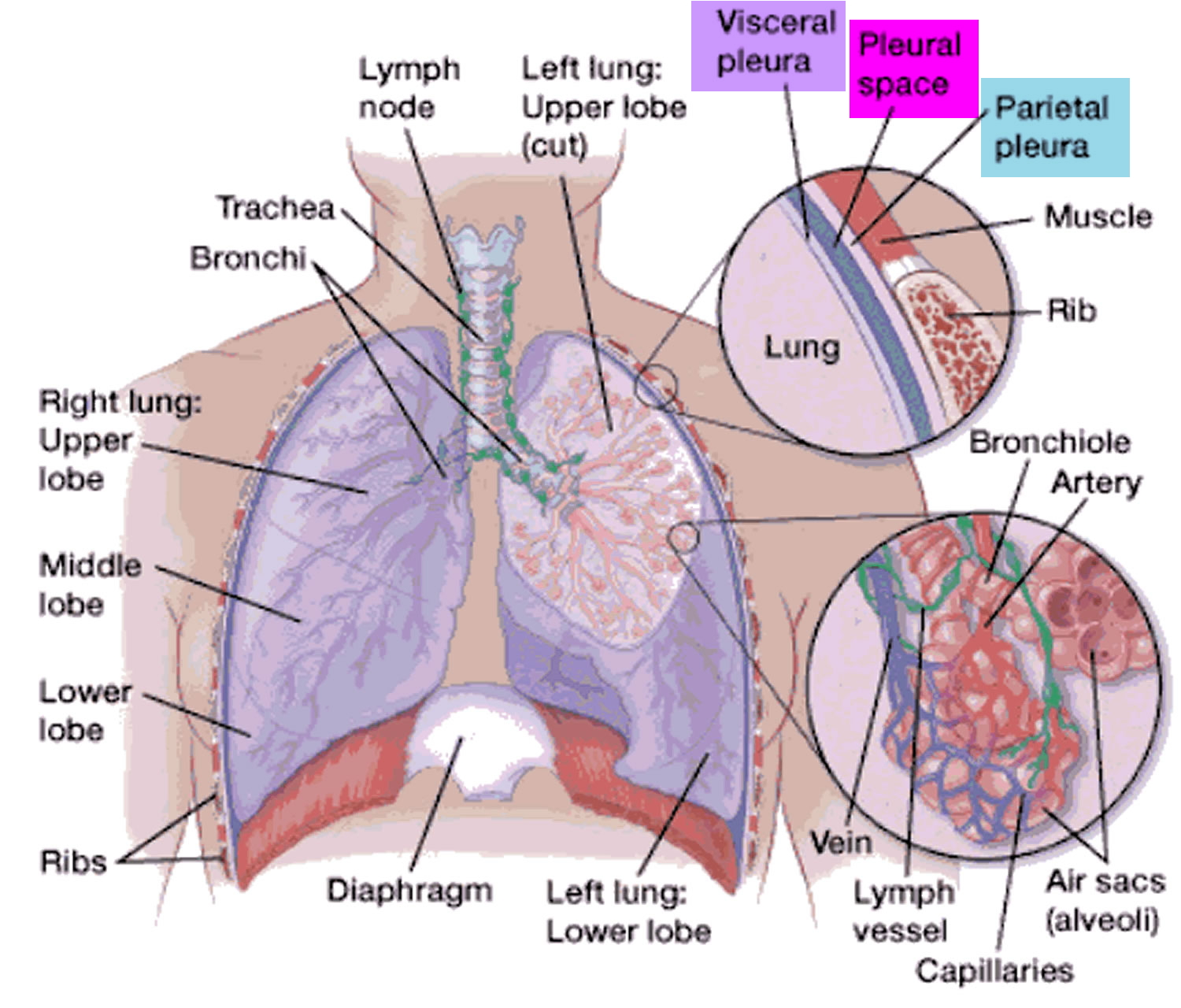
Parietal refers to a membrane attached to the wall of a cavity; visceral refers to a membrane that is deeper—toward the interior—and covers an internal organ, such as a lung. Within the thoracic (chest) cavity, the compartments that contain the lungs, on either side of the mediastinum, are lined with a membrane called the parietal pleura. A similar membrane, called the visceral pleura, covers each lung.
The parietal and visceral pleural membranes are separated only by a thin film of watery fluid (serous fluid), which they secrete. Although no actual space normally exists between these membranes, the potential space between them is called the pleural cavity.
A thin lining layer called the pleura surrounds the lungs. The pleura protects your lungs and helps them slide back and forth against the chest wall as they expand and contract during breathing. A layer of serous membrane, the visceral pleura, firmly attaches to each lung surface and folds back to become the
parietal pleura. The parietal pleura, in turn, borders part of the mediastinum and lines the inner wall of the thoracic cavity and the superior surface of the diaphragm.
Figure 3. Lungs anatomy and pleural space
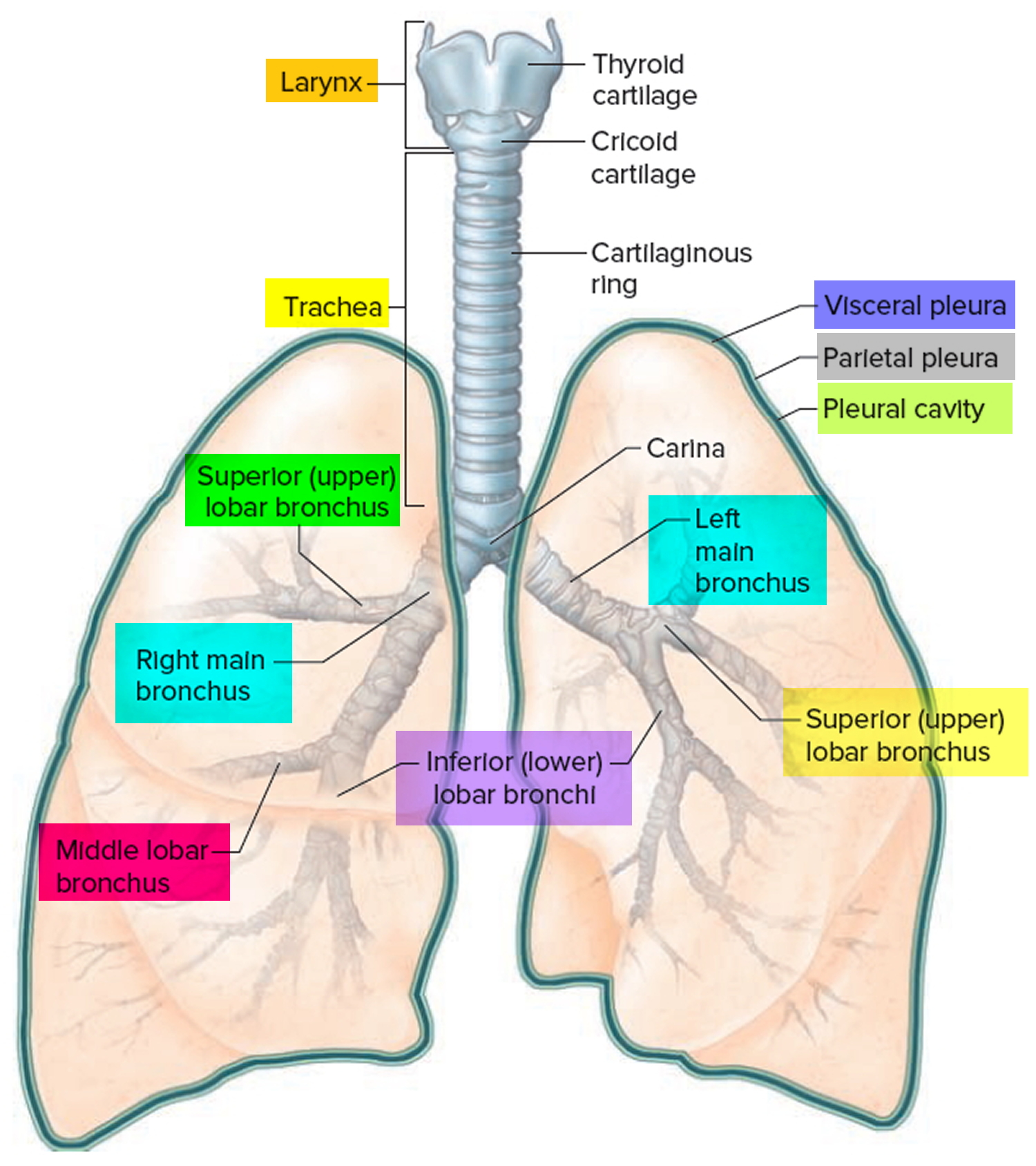
Figure 4. Lungs pleura and pleural cavity
Pleurisy causes
Most cases of pleurisy are caused by a virus, such as the flu (influenza) virus 1, 2.
Less common causes of pleurisy include:
- Bacterial infections, such as pneumonia and tuberculosis, and infections from parasites
- Common bacterial infections that can lead to pleurisy 2, 15, 16:
- Empyema
- Tuberculosis
- Legionellae
- Bacterial pneumonia
- Spontaneous bacterial pleuritis
- Mediterranean spotted fever also known as boutonneuse fever, is a tick-borne rickettsial disease caused by Rickettsia conorii and transmitted by the brown dog tick (Rhipicephalus sanguineus), primarily found in the Mediterranean Basin, Southern Europe, Africa, and the Middle East
- Parasitic causes, such as amebiasis and paragonimiasis caused by consuming undercooked crab or crayfish infected with Paragonimus westermani, are potential contributors to pleurisy 17.
- Common bacterial infections that can lead to pleurisy 2, 15, 16:
- Viral causes of pleurisy 2:
- Fungal infection
- A blood clot that travels through the blood vessels to the lungs (pulmonary embolism)
- Chest injury – if the ribs are bruised or fractured, the pleura can become inflamed
- Cancer, such as lung cancer, lymphoma, and mesothelioma
- Autoimmune conditions, such as rheumatoid arthritis and lupus. Additional autoimmune or inflammatory conditions causing pleurisy include 18:
- Ankylosing spondylitis
- Collagen vascular disease
- Reactive eosinophilic pleuritis
- Sjögren syndrome
- Chest and heart surgery, especially coronary artery bypass grafting (CABG)
- Certain medications
- Rib fracture
- Lung diseases, such as chronic obstructive pulmonary disease (COPD), pneumothorax, hemothorax, pulmonary embolism, pleural effusion, pulmonary adhesions, lymphangioleiomyomatosis or asbestosis
- Inflammatory bowel disease (IBD) e.g., Crohn’s disease 19
- Certain inherited diseases, such as sickle cell disease or Familial Mediterranean fever, an inherited condition that often causes fever and swelling in the abdomen or lungs.
- Kidney conditions
- Chronic kidney disease (CKD)
- Renal capsule hematoma 20
Other causes of pleurisy include chest injuries, pancreatitis (an inflamed pancreas), and reactions to certain medicines and recreational drugs such as cocaine, heroin, and methadone 21. Reactions to certain medicines can cause a condition similar to lupus. These medicines include isoniazid, hydralazine, nitrofurantoin, and cyclophosphamide.
Sometimes doctors can’t find the cause of pleurisy (idiopathic).
Pleurisy symptoms
The signs and symptoms of pleurisy might include:
- Sharp or stabbing knife-like pain chest pain that worsens when you breathe, cough or sneeze
- Shortness of breath — because you are trying to minimize breathing in and out
- A cough — only in some cases
- A fever — only in some cases
Pain caused by pleurisy also might affect your shoulders or back.
You may have other conditions along with pleurisy, including:
- Partial lung collapse (atelectasis).
- Excess fluid around your lungs (pleural effusion).
- Pus collecting around your lungs (empyema).
In some cases of pleurisy, fluid builds up in the small space between the two layers of tissue (pleural space). This is called pleural effusion. When there is a fair amount of fluid, pleuritic pain lessens or disappears because the two layers of pleura are no longer in contact. A large amount of fluid in the pleural space can create pressure, compressing your lung to the point that it partially or completely collapses. This makes breathing difficult and might cause you to cough. The extra fluid can also become infected. This is called an empyema – a collection of pus in the space between the lung and the inner surface of the chest wall (pleural space). An empyema is often accompanied by fever.
Pleurisy complications
The potential complications of pleurisy vary widely and are closely tied to its underlying cause.
Cardiovascular disease complications:
- Papillary muscle rupture
- Left ventricular free wall rupture
- Interventricular septum rupture
- Acute and chronic heart failure
- Death
- Arrhythmias and conduction abnormalities
- Post-cardiac injury syndrome
- Cardiac tamponade
Lung disease complications:
- Shock
- Recurrence
- Pneumonia
- Stroke
- Pulmonary hypertension
- Respiratory failure
- Empyema
- Atelectasis
- Tension pneumothorax
- Hemopneumothorax is when blood and air enter your pleural space and put pressure around your lungs
Autoimmune conditions complications:
- Cholesterol effusions
- Lung entrapment
Infectious disease complications:
- Sepsis
- Empyema
- Pneumothorax
- Cancer associated with tuberculosis
- Bronchiectasis
- Broncholithiasis a condition characterized by the presence of calcified or ossified material, often originating from calcified lymph nodes, within the tracheobronchial tree, potentially causing airway obstruction and inflammation
- Acute respiratory distress syndrome (ARDS)
- Venous thromboembolism
- Chronic pulmonary aspergillosis 22
- Pleural lymphoma associated with longstanding chronic pleural infection 23, 24
- Bronchopleural fistula
- Pleural fibrosis is the scarring, thickening and stiffening of the pleura (the membrane surrounding the lungs) due to inflammation or exposure to irritants like asbestos, leading to scar tissue accumulation and potentially restricting lung function
Kidney disease complications:
- Constrictive pleural thickening
- Pulmonary embolism
- Empyema
- Pulmonary edema
Drug-Induced Pleural Disease complications:
- Hypoxia
- Pulmonary embolism
- Pleural fibrosis is the scarring, thickening and stiffening of the pleura (the membrane surrounding the lungs) due to inflammation or exposure to irritants like asbestos, leading to scar tissue accumulation and potentially restricting lung function
Pleurisy diagnosis
Your doctor will find out if you have pleurisy or another pleural disorder by taking a detailed medical history and doing a physical exam with a stethoscope and several diagnostic tests, including:
- Blood tests. A blood test might tell your doctor if you have an infection. Other blood tests also might detect an autoimmune disorder, such as rheumatoid arthritis or lupus. In these conditions, pleurisy can be the first sign.
- Arterial blood gas tests, which show how well your lungs are taking in oxygen. For this test, a blood sample is taken from an artery, usually in your wrist. The blood’s oxygen and carbon dioxide levels are checked. This test shows how well your lungs are taking in oxygen.
- Chest X-ray. A chest X-ray can show if your lungs are fully inflating or if there is air or fluid between the lungs and ribs. Your doctor might recommend a special type of chest X-ray in which you lie on your side (decubitus chest X-ray).
- Computerized tomography (CT) scan. In a CT scan, a computer translates information from X-rays into images of thin sections (slices) of your chest, producing more-detailed images. A chest CT scan can show if there is a blood clot in the lung or find other causes of pleuritic pain.
- Ultrasound. This imaging method uses high-frequency sound waves to produce precise images of structures within your body. Your doctor might use ultrasound to determine whether you have a pleural effusion.
- Electrocardiogram (ECG or EKG). Your doctor might recommend this heart-monitoring test to rule out certain heart problems as a cause for your chest pain.
Medical history
The time course of the onset of symptoms is the most useful historical information for narrowing the differential diagnosis. Most potentially deadly causes of pleuritic chest pain (i.e., pulmonary embolism, heart attack, aortic dissection, and pneumothorax) typically have an acute onset over minutes 2. In contrast, less immediately life-threatening causes of pleuritic chest pain (e.g., infection, cancer, inflammatory processes) progress over hours to days or weeks 25. Pain that worsens when you’re supine (lying on your back with your face upwards) and lessens when you’re upright and leaning forward should prompt consideration for pericarditis 26, 27, 25. True shortness of breath (dyspnea) should also increase suspicion for a pulmonary embolus, pneumothorax, or pneumonia 28, 29, 30. It is clinically useful to distinguish true shortness of breath (dyspnea) from patient-perceived dyspnea caused by a desire to suppress respirations to avoid pain 31, 32.
Cardiac symptoms such as diaphoresis, nausea, and palpitations should be elucidated. Pain that is described as sharp and stabbing is typical of noncardiac chest pain 31. Radiation of pain to the shoulders or arms has a positive likelihood ratio of 4.07 for acute myocardial infarction 31. In contrast, pain that radiates to the back and is maximal in intensity at onset is more commonly associated with aortic dissection than cardiac ischemia 31.
Cough, fever, and sputum production should prompt evaluation for community-acquired pneumonia. Symptoms such as weight loss, malaise, night sweats, or arthralgias indicate chronic inflammatory causes of pleuritic chest pain, such as tuberculosis infection, rheumatoid arthritis, or malignancy. A family history of similar symptoms increases the likelihood of rare diagnoses such as familial Mediterranean fever. A medication history that includes the use of drugs with a high risk of adverse pulmonary effects should raise concerns for a pharmacologic reaction. A sickle cell crisis must be considered in any patient with known sickle cell disease.
Physical examination
Tachycardia or tachypnea may be present with any of the serious causes of pleuritic chest pain but should raise suspicion for pulmonary embolism, pneumothorax, or myocardial infarction 2. Patients may demonstrate shallower breaths as they attempt to avoid deep breathing that triggers pain 32. Likewise, hypotension and a markedly widened pulse pressure should raise concerns for aortic dissection or severe myocardial infarction. Fever increases the likelihood of infection.
Pleural inflammation, or pleurisy, causes roughening of the smooth surfaces of the parietal and visceral pleurae. As these surfaces rub against each other with normal inspiration and expiration, a scratching sound or friction rub may be heard. This may also occur in 4% of patients with pneumonia or pulmonary embolism 33. Pneumonia with lung consolidation may also lead to decreased breath sounds, rales, and egophony. In contrast, pneumothorax could lead to hyperresonance on lung examination.
In new-onset heart failure due to large myocardial infarction, cardiac examination may show an extra heart sound (third S3 or fourth S4 heart sound). A friction rub may be heard over the heart in severe cases of pericarditis. Patients may present with an initial normal examination even when serious conditions are present. The absence of a clear diagnosis warrants additional diagnostic testing.
Diagnostic tests
Most patients presenting with pleuritic chest pain will require imaging with chest X-ray to fully define their diagnosis 30. If pleural fluid is seen on a chest X-ray, the fluid can be aspirated and examined for additional clues about the source of the pleuritic chest pain 34, 35 Lung ultrasonography can guide thoracentesis, as well as localize a small pneumothorax and identify other pulmonary conditions 36, 37.
When a cardiac or vascular source is considered, electrocardiography (ECG), cardiac enzyme studies, and echocardiography are useful tests. Widespread ST segment elevation is a typical electrocardiographic finding in pericarditis 38, 39. In the case of infection, a complete blood count, serology, and cultures of blood, sputum, or pleural fluid may be indicated. A validated clinical decision rule for pulmonary embolism should be employed to guide the use of additional tests such as d-dimer assays, ventilation-perfusion scans, or computed tomography angiography 40, 41, 42, 43. Figure 2 above integrates red flag symptoms of serious causes of pleuritic chest pain, physical examination, and diagnostic findings to aid in the evaluation of pleuritic chest pain.
Diagnostic tests might include:
- Thoracentesis. To remove fluid for laboratory analysis, your doctor might suggest thoracentesis. In this procedure, your doctor injects a local anesthetic between your ribs to the area where fluid was seen on your imaging studies. Next your doctor inserts a needle through your chest wall between your ribs to remove fluid for laboratory analysis. Your doctor might insert the needle with the help of ultrasound guidance.
- Thoracoscopy or pleuroscopy. If tuberculosis or cancer is a suspected cause of your condition, your doctor might perform a procedure that allows for direct visualization inside your chest to look for any abnormalities or to obtain a tissue sample (biopsy) if needed.
- Biopsy. Your doctor may suspect that tuberculosis or cancer has caused fluid to build up in your pleural space. If so, he or she may want to look at a small piece of the pleura under a microscope. To take a tissue sample, your doctor may do one of the following procedures:
- Insert a needle into your chest to remove a small sample of the pleura’s outer layer.
- Insert a tube with a light on the end (endoscope) into tiny cuts in your chest wall so that he or she can see the pleura. Your doctor can then snip out small pieces of tissue. This procedure must be done in a hospital. You’ll be given medicine to make you sleep during the procedure.
- Snip out a sample of the pleura through a small cut in your chest wall. This is called an open pleural biopsy. It’s usually done if the sample from the needle biopsy is too small for an accurate diagnosis. This procedure must be done in a hospital. You’ll be given medicine to make you sleep during the procedure.
Your doctor will look at the fluid under a microscope to determine what’s causing the fluid buildup. If the fluid is infected, treatment involves antibiotics and draining the fluid. If the infection is tuberculosis or from a fungus, treatment involves long-term use of antibiotics or antifungal medicines. If the fluid is caused by tumors of the pleura, it may build up again quickly after it’s drained. Sometimes antitumor medicines will prevent further fluid buildup. If they don’t, the doctor may seal the pleural space.
Pleurisy treatment
Treatments used in pleurisy and pleural effusion focus primarily on the underlying cause.
How to treat pleurisy
To relieve symptoms, your doctor may recommend:
- Acetaminophen or non-steroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, to control pain
- Codeine-based cough syrups to control a cough
- Lying on the painful side to make you more comfortable. It seems strange, but lying on the side of your chest that hurts may also help reduce the pain.
- Breathing deeply and coughing to clear mucus as the pain eases
- Getting plenty of rest.
The outcome of pleurisy treatment depends on the seriousness of the underlying disease. If the condition that caused pleurisy is diagnosed and treated early, a full recovery is typical.
Treating the underlying cause of pleurisy
If your pleurisy is caused by a viral infection, it’ll usually get better on its own after a few days.
If it’s caused by a bacterial infection, you’ll need antibiotics. Depending on the severity of your symptoms, this may be either tablets or injections.
If your symptoms are particularly severe or you’re already in poor health, you may need to be admitted to hospital.
Treating pleural effusion
In some cases, pleurisy causes a build-up of excess fluid around the lungs called pleural effusion.
Pleural effusion can lead to shortness of breath that gets progressively worse. This is more likely if pleurisy is caused by pulmonary embolism or a bacterial infection.
If pleural effusion doesn’t clear up as your pleurisy is treated or you’re very short of breath, the fluid may need to be drained by inserting a needle or tube through the chest wall.
A procedure called thoracentesis is used to remove fluid from the pleural space. The doctor inserts a needle or a thin, hollow, plastic tube through the ribs in the back of your chest into your chest wall. A syringe is attached to draw fluid out of your chest.
- If your doctor needs to remove a lot of fluid, he or she may use a chest tube. Your doctor will inject a painkiller into the area of your chest wall where the fluid is. He or she will then insert a plastic tube into your chest between two ribs. The tube will be connected to a box that suctions out the fluid. Your doctor will use a chest x ray to check the tube’s position.
- Your doctor also can use a chest tube to drain blood and air from the pleural space. This process can take several days. The tube will be left in place, and you’ll likely stay in the hospital during this time.
This can be done under general anesthetic or local anesthetic. You may need to stay in hospital for a few days if a lot of fluid has to be drained away.
The fluid sample that was removed during thoracentesis will be checked under a microscope. This can tell your doctor what’s causing the fluid buildup, and he or she can decide the best way to treat it.
If the fluid is infected, treatment will involve antibiotics and drainage. If you have tuberculosis or a fungal infection, treatment will involve long-term use of antibiotics or antifungal medicines.
If tumors in the pleura are causing fluid buildup, the fluid may quickly build up again after it’s drained. Sometimes antitumor medicines will prevent further fluid buildup. If they don’t, your doctor may seal the pleural space. Sealing the pleural space is called pleurodesis.
For this procedure, your doctor will drain all of the fluid out of your chest through a chest tube. Then he or she will push a substance through the chest tube into the pleural space. The substance will irritate the surface of the pleura. This will cause the two layers of the pleura to stick together, preventing more fluid from building up.
Chemotherapy or radiation treatment also may be used to reduce the size of the tumors.
If heart failure is causing fluid buildup, treatment usually includes diuretics (medicines that help reduce fluid buildup) and other medicines.
Pleurisy treatment at home
The following steps might help relieve symptoms related to pleurisy:
- Take medication. Take medication such as ibuprofen (Advil, Motrin IB, others) as needed to relieve pain and inflammation.
- Get plenty of rest. Find the position that causes you the least discomfort and try to stay in it. Even when you start to feel better, be careful not to overdo it.
- Don’t smoke. Smoking can cause more irritation to your lungs. If you smoke and can’t quit on your own, ask your healthcare provider for help.
Pleurisy prognosis
Your prognosis (outlook) for pleurisy depends on what’s causing it and the effectiveness of your treatment. If your pleurisy is caused by infection, it should go away as you get better. If it’s caused by an ongoing illness like cancer or an autoimmune disease, you may always have some risk of pleurisy coming back. Very rarely, pleurisy has life-threatening complications.
Infectious causes
Viral pleuritis is generally self-limited, with symptoms typically resolving within a few days or weeks 1. People with bacterial pleural infections usually improve with appropriate antibiotic treatment. The reported 30-day mortality rate for bacterial infections is 10.5%, with 1-year mortality nearing 19% 44. Recent studies indicate that affected patients face an increased risk of thromboembolic events (a condition where a blood clot or thrombus breaks off and travels through the bloodstream to obstruct a blood vessel) due to significant inflammation, prolonged hospitalizations, frequent comorbidities, and the need for operative interventions 45.
Autoimmune conditions
The prognosis of lupus pleuritis is generally good 1. However, the prognosis of pleuritis associated with rheumatoid arthritis varies 1. While many patients experience spontaneous resolution within 3 months, some may develop persistent effusion and pleural thickening. Anti-inflammatory therapy does not appear to be effective in resolving rheumatoid pleuritis 1.
Cancer
Cancer causing pleural disease is associated with a poor prognosis. A study in patients with malignant mesothelioma showed a median survival of just 13 months following diagnosis 46.
Lung conditions
The presence of a pleural effusion is linked to increased mortality, with 15% of patients dying within 30 days and 32% within 1 year of hospital admission 47. However, with early treatment, the mortality rate for pulmonary embolism decreases from 30% to 8%.
Heart and blood vessel conditions
Acute heart attack has a mortality rate of 30%, with nearly 50% of deaths occurring before patients reach the hospital 1. Early reperfusion through fibrinolysis or percutaneous coronary intervention within 90 minutes of arrival, along with preserved left ventricular function and short- and long-term treatment with beta-blockers, aspirin, and angiotensin-converting enzyme inhibitors, all contribute to improved survival 1. The strongest predictor of a poor outcome is poorly preserved left ventricular function 48.
Additional factors that worsen mortality include:
- Older age
- Diabetes
- Delayed reperfusion
- Elevated B-type natriuretic (BNP) peptide and high-sensitivity C-reactive protein (CRP)
- Depression
- Involvement of lead aVR on ECG 49.
- Presence of heart failure or pulmonary edema
- History of cerebrovascular disease or peripheral vascular disease
- Elevated thrombolysis in myocardial infarction risk score for unstable angina/non–ST-elevation acute coronary syndrome
The thrombolysis in myocardial infarction (heart attack) risk score includes 7 factors, including age 65 or older, 3 or more risk factors for cardiac disease, previous coronary disease, ST-segment deviation of 0.5 mm or more, 2 or more episodes of angina in the last 24 hours, aspirin use within the prior week, and elevated cardiac enzyme levels 50.
The overall prognosis for Dressler syndrome also known as postmyocardial infarction syndrome, is a form of secondary pericarditis (inflammation of the sac surrounding the heart) that occurs after heart damage, often following a heart attack or cardiac surgery, and is believed to be an immune-mediated response and viral or bacterial pericarditis is generally good, with most patients recovering within a few weeks to 3 months. However, cancer invasion of the pericardium has a poor prognosis, with survival rarely extending beyond 12 to 18 months 1.
Kidney conditions
Patients with uremic pleuritis generally fare well with more aggressive hemodialysis and, if necessary, thoracentesis 1. However, approximately 20% may experience persistent effusion and develop fibrinous lung disease 51.
Drug-Induced Lung Disease
The prognosis of medication-induced pleuritis depends on the medication and the severity of the lung disease 1. Outcomes for drug-induced lupus pleuritis and pleural effusions are generally good, with symptoms resolving within months after discontinuing the offending medication 1. However, other forms of pulmonary toxicity have variable mortality rates. For example, methotrexate-induced pulmonary toxicity carries a 13% mortality rate 52. Pulmonary fibrosis due to cyclophosphamide has a 50% mortality rate, while patients with acute respiratory distress syndrome caused by amiodarone have a 10% mortality rate 53.
- Hunter MP, Goldin J, Regunath H. Pleurisy. [Updated 2024 Nov 14]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK558958[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Reamy BV, Williams PM, Odom MR. Pleuritic Chest Pain: Sorting Through the Differential Diagnosis. Am Fam Physician. 2017 Sep 1;96(5):306-312. https://www.aafp.org/pubs/afp/issues/2017/0901/p306.html[↩][↩][↩][↩][↩][↩][↩][↩]
- Castaniere I, Tonelli R, Fantini R, Marchioni A, Garofalo M, Clini EM, Cerri S. The encaged lung: rapidly progressive idiopathic pleurisy. Oxf Med Case Reports. 2018 Aug 9;2018(8):omy041. doi: 10.1093/omcr/omy041[↩]
- Hogg K, Dawson D, Mackway-Jones K. Outpatient diagnosis of pulmonary embolism: the MIOPED (Manchester Investigation Of Pulmonary Embolism Diagnosis) study. Emerg Med J. 2006 Feb;23(2):123-7. doi: 10.1136/emj.2005.027110[↩][↩]
- Hull RD, Raskob GE, Carter CJ, et al. Pulmonary Embolism in Outpatients With Pleuritic Chest Pain. Arch Intern Med. 1988;148(4):838–844. doi:10.1001/archinte.1988.00380040078014[↩]
- Courtney DM, Kline JA, Kabrhel C, Moore CL, Smithline HA, Nordenholz KE, Richman PB, Plewa MC. Clinical features from the history and physical examination that predict the presence or absence of pulmonary embolism in symptomatic emergency department patients: results of a prospective, multicenter study. Ann Emerg Med. 2010 Apr;55(4):307-315.e1. doi: 10.1016/j.annemergmed.2009.11.010[↩]
- Brims FJ, Davies HE, Lee YC. Respiratory chest pain: diagnosis and treatment. Med Clin North Am. 2010 Mar;94(2):217-32. doi: 10.1016/j.mcna.2010.01.003[↩][↩]
- Hara K, Yamasaki K, Tahara M, Ikegami H, Nishida C, Muramutsu K, Fujino Y, Matsuda S, Fushimi K, Mukae H, Yatera K. Epidemiologic evaluation of pleurisy diagnosed by surgical pleural biopsy using data from a nationwide administrative database. Thorac Cancer. 2022 Apr;13(8):1136-1142. doi: 10.1111/1759-7714.14368[↩][↩]
- Dinwiddie R, Sonnappa S. Systemic diseases and the lung. Paediatr Respir Rev. 2005 Sep;6(3):181-9. doi: 10.1016/j.prrv.2005.06.007[↩]
- Shaw M, Collins BF, Ho LA, Raghu G. Rheumatoid arthritis-associated lung disease. Eur Respir Rev. 2015 Mar;24(135):1-16. doi: 10.1183/09059180.00008014[↩]
- Light RW. Pleural effusion due to pulmonary emboli. Curr Opin Pulm Med. 2001 Jul;7(4):198-201. doi: 10.1097/00063198-200107000-00006[↩]
- Ozbay B, Uzun K. Extrapulmonary tuberculosis in high prevalence of tuberculosis and low prevalence of HIV. Clin Chest Med. 2002 Jun;23(2):351-4. doi: 10.1016/s0272-5231(02)00002-3[↩]
- Rolo M, González-Blanco B, Reyes CA, Rosillo N, López-Roa P. Epidemiology and factors associated with Extra-pulmonary tuberculosis in a Low-prevalence area. J Clin Tuberc Other Mycobact Dis. 2023 May 12;32:100377. doi: 10.1016/j.jctube.2023.100377[↩]
- Engel ME, Matchaba PT, Volmink J. Corticosteroids for tuberculous pleurisy. Cochrane Database Syst Rev. 2007 Oct 17;(4):CD001876. doi: 10.1002/14651858.CD001876.pub2. Update in: Cochrane Database Syst Rev. 2017 Mar 14;3:CD001876. doi: 10.1002/14651858.CD001876.pub3[↩]
- Yu S, Gao Y, Lu J, Zhang G, Chen X, Zhang R, Kong W, Shang L. Clinical profiles and related factors in tuberculosis patients with positive sputum smear mycobacterium tuberculosis tests. Sci Rep. 2024 Sep 2;14(1):20376. doi: 10.1038/s41598-024-71403-5[↩]
- Kamus L, Roquebert B, Allyn J, Allou N, Valance D, Simon C, Jaffar-Bandjee MC, Descours G, Jarraud S, Miltgen G. Severe bilateral pleuropneumonia caused by Legionella sainthelensi: a case report. BMC Infect Dis. 2021 Sep 17;21(1):966. doi: 10.1186/s12879-021-06651-1[↩]
- Mbaye PS, Koffi N, Camara P, Burgel PR, Hovette P, Klotz F. Manifestations pleuropulmonaires de l’amibiase [Pleuropulmonary manifestations of amebiasis]. Rev Pneumol Clin. 1998 Dec;54(6):346-52. French[↩]
- Bouros D, Pneumatikos I, Tzouvelekis A. Pleural involvement in systemic autoimmune disorders. Respiration. 2008;75(4):361-71. doi: 10.1159/000119051[↩]
- Ahmed HK, Hiwa DS, Tahir SH, Ali RM, Gharib DT, Asaad HR, Hamahussein KF, Mohammed AA, Najar KA, Kakamad FH. Crohn’s disease presenting with pleural effusion: a case report. Oxf Med Case Reports. 2024 Oct 10;2024(10):omae113. doi: 10.1093/omcr/omae113[↩]
- Wang L, Qiu Z, Zhan S, Shi G, He W, Cen Z, Xu F, Tian W, Li D. Case report: Page kidney with multiple serosal effusions caused by bilateral spontaneous renal subcapsular hemorrhage. Front Med (Lausanne). 2024 Jan 24;11:1290470. doi: 10.3389/fmed.2024.1290470[↩]
- Bontempo LJ, Magidson PD, Hayes BD, Martinez JP. Acute Pulmonary Injury after Inhalation of Free-Base Cocaine: A Case Report. J Acute Med. 2017 Jun 1;7(2):82-86. doi: 10.6705/j.jacme.2017.0702.007[↩]
- Ocansey BK, Otoo B, Adjei A, Gbadamosi H, Kotey FCN, Kosmidis C, Afriyie-Mensah JS, Denning DW, Opintan JA. Chronic pulmonary aspergillosis is common among patients with presumed tuberculosis relapse in Ghana. Med Mycol. 2022 Sep 9;60(9):myac063. doi: 10.1093/mmy/myac063[↩]
- Iuchi K, Aozasa K, Yamamoto S, Mori T, Tajima K, Minato K, Mukai K, Komatsu H, Tagaki T, Kobashi Y, et al. Non-Hodgkin’s lymphoma of the pleural cavity developing from long-standing pyothorax. Summary of clinical and pathological findings in thirty-seven cases. Jpn J Clin Oncol. 1989 Sep;19(3):249-57.[↩]
- Narimatsu H, Ota Y, Kami M, Takeuchi K, Suzuki R, Matsuo K, Matsumura T, Yuji K, Kishi Y, Hamaki T, Sawada U, Miyata S, Sasaki T, Tobinai K, Kawabata M, Atsuta Y, Tanaka Y, Ueda R, Nakamura S. Clinicopathological features of pyothorax-associated lymphoma; a retrospective survey involving 98 patients. Ann Oncol. 2007 Jan;18(1):122-128. doi: 10.1093/annonc/mdl349[↩]
- Nadal JA, Murray JF, Mason RJ. Textbook of Respiratory Medicine. 4th ed. Philadelphia, Pa.: Saunders-Elsevier; 2005.[↩][↩]
- Peterson TA, Turner SP, Dolezal KA. Acute Pericarditis: Rapid Evidence Review. Am Fam Physician. 2024 May;109(5):441-446. https://www.aafp.org/pubs/afp/issues/2024/0500/acute-pericarditis.html[↩]
- Marinella MA. Electrocardiographic manifestations and differential diagnosis of acute pericarditis. Am Fam Physician. 1998 Feb 15;57(4):699-704. https://www.aafp.org/pubs/afp/issues/1998/0215/p699.html[↩]
- Sahn SA, Heffner JE. Spontaneous pneumothorax. N Engl J Med. 2000 Mar 23;342(12):868-74. doi: 10.1056/NEJM200003233421207[↩]
- Perrier A, Roy PM, Aujesky D, Chagnon I, Howarth N, Gourdier AL, Leftheriotis G, Barghouth G, Cornuz J, Hayoz D, Bounameaux H. Diagnosing pulmonary embolism in outpatients with clinical assessment, D-dimer measurement, venous ultrasound, and helical computed tomography: a multicenter management study. Am J Med. 2004 Mar 1;116(5):291-9. doi: 10.1016/j.amjmed.2003.09.041[↩]
- Metlay JP, Kapoor WN, Fine MJ. Does This Patient Have Community-Acquired Pneumonia? Diagnosing Pneumonia by History and Physical Examination. JAMA. 1997;278(17):1440–1445. doi:10.1001/jama.1997.03550170070035[↩][↩]
- Swap CJ, Nagurney JT. Value and limitations of chest pain history in the evaluation of patients with suspected acute coronary syndromes. JAMA. 2005 Nov 23;294(20):2623-9. doi: 10.1001/jama.294.20.2623. Erratum in: JAMA. 2006 May 17;295(19):2250.[↩][↩][↩][↩]
- Lanham DA, Taylor AN, Chessell SJ, Lanham JG. Non-cardiac chest pain: a clinical assessment tool. Br J Hosp Med (Lond). 2015 May;76(5):296-300. doi: 10.12968/hmed.2015.76.5.296[↩][↩]
- Miniati M, Prediletto R, Formichi B, Marini C, Di Ricco G, Tonelli L, Allescia G, Pistolesi M. Accuracy of clinical assessment in the diagnosis of pulmonary embolism. Am J Respir Crit Care Med. 1999 Mar;159(3):864-71. doi: 10.1164/ajrccm.159.3.9806130[↩]
- Shen-Wagner J, Gamble C, MacGilvray P. Pleural Effusion: Diagnostic Approach in Adults. Am Fam Physician. 2023 Nov;108(5):464-475. https://www.aafp.org/pubs/afp/issues/2023/1100/pleural-effusion.html[↩]
- Light RW. Clinical practice. Pleural effusion. N Engl J Med. 2002 Jun 20;346(25):1971-7. doi: 10.1056/NEJMcp010731[↩]
- Ding W, Shen Y, Yang J, He X, Zhang M. Diagnosis of pneumothorax by radiography and ultrasonography: a meta-analysis. Chest. 2011 Oct;140(4):859-866. doi: 10.1378/chest.10-294[↩]
- Volpicelli G, Cardinale L, Berchialla P, Mussa A, Bar F, Frascisco MF. A comparison of different diagnostic tests in the bedside evaluation of pleuritic pain in the ED. Am J Emerg Med. 2012 Feb;30(2):317-24. doi: 10.1016/j.ajem.2010.11.035[↩]
- Lange RA, Hillis LD. Clinical practice. Acute pericarditis. N Engl J Med. 2004 Nov 18;351(21):2195-202. doi: 10.1056/NEJMcp041997. Erratum in: N Engl J Med. 2005 Mar 17;352(11):1163.[↩]
- Hiratzka LF, Bakris GL, Beckman JA, et al; American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines; American Association for Thoracic Surgery; American College of Radiology; American Stroke Association; Society of Cardiovascular Anesthesiologists; Society for Cardiovascular Angiography and Interventions; Society of Interventional Radiology; Society of Thoracic Surgeons; Society for Vascular Medicine. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM Guidelines for the diagnosis and management of patients with thoracic aortic disease. A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology,American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons,and Society for Vascular Medicine. J Am Coll Cardiol. 2010 Apr 6;55(14):e27-e129. doi: 10.1016/j.jacc.2010.02.015. Erratum in: J Am Coll Cardiol. 2013 Sep 10;62(11):1039-40.[↩]
- Wells PS, Anderson DR, Rodger M, Stiell I, Dreyer JF, Barnes D, Forgie M, Kovacs G, Ward J, Kovacs MJ. Excluding pulmonary embolism at the bedside without diagnostic imaging: management of patients with suspected pulmonary embolism presenting to the emergency department by using a simple clinical model and d-dimer. Ann Intern Med. 2001 Jul 17;135(2):98-107. doi: 10.7326/0003-4819-135-2-200107170-00010[↩]
- Kline JA, Courtney DM, Kabrhel C, Moore CL, Smithline HA, Plewa MC, Richman PB, O’Neil BJ, Nordenholz K. Prospective multicenter evaluation of the pulmonary embolism rule-out criteria. J Thromb Haemost. 2008 May;6(5):772-80. doi: 10.1111/j.1538-7836.2008.02944.x[↩]
- Lucassen WA, Douma RA, Toll DB, Büller HR, van Weert HC. Excluding pulmonary embolism in primary care using the Wells-rule in combination with a point-of care D-dimer test: a scenario analysis. BMC Fam Pract. 2010 Sep 13;11:64. doi: 10.1186/1471-2296-11-64[↩]
- Le Gal G, Righini M, Roy PM, Sanchez O, Aujesky D, Bounameaux H, Perrier A. Prediction of pulmonary embolism in the emergency department: the revised Geneva score. Ann Intern Med. 2006 Feb 7;144(3):165-71. doi: 10.7326/0003-4819-144-3-200602070-00004[↩]
- Addala DN, Bedawi EO, Rahman NM. Parapneumonic Effusion and Empyema. Clin Chest Med. 2021 Dec;42(4):637-647. doi: 10.1016/j.ccm.2021.08.001[↩]
- Ala-Seppälä HM, Ukkonen MT, Lehtomäki AI, Pohja ES, Nieminen JJ, Laurikka JO, Khan JA. High Occurrence of Thrombo-Embolic Complications During Long-Term Follow-up After Pleural Infections-A Single-Center Experience with 536 Consecutive Patients Over 17 Years. Lung. 2020 Aug;198(4):671-678. doi: 10.1007/s00408-020-00374-x[↩]
- Saunders J, Ashton M, Hall C, Laird B, MacLeod N. Pain management in patients with malignant mesothelioma: challenges and solutions. Lung Cancer (Auckl). 2019 Apr 2;10:37-46. doi: 10.2147/LCTT.S192558[↩]
- Kookoolis AS, Puchalski JT, Murphy TE, Araujo KL, Pisani MA. Mortality of Hospitalized Patients with Pleural Effusions. J Pulm Respir Med. 2014 Jun;4(3):184. doi: 10.4172/2161-105X.1000184[↩]
- Kim H, Lee KY, Choo EH, Hwang BH, Kim JJ, Kim CJ, Chang K, Hong YJ, Kim JH, Ahn Y, Choi Y; KAMIR‐NIH Investigators. Long-Term Risk of Cardiovascular Death in Patients With Mildly Reduced Ejection Fraction After Acute Myocardial Infarction: A Multicenter, Prospective Registry Study. J Am Heart Assoc. 2024 Sep 17;13(18):e034870. doi: 10.1161/JAHA.124.034870[↩]
- Alherbish A, Westerhout CM, Fu Y, White HD, Granger CB, Wagner G, Armstrong PW. The forgotten lead: does aVR ST-deviation add insight into the outcomes of ST-elevation myocardial infarction patients? Am Heart J. 2013 Aug;166(2):333-9. doi: 10.1016/j.ahj.2013.05.018[↩]
- Amsterdam EA, Wenger NK, Brindis RG, Casey DE Jr, Ganiats TG, Holmes DR Jr, Jaffe AS, Jneid H, Kelly RF, Kontos MC, Levine GN, Liebson PR, Mukherjee D, Peterson ED, Sabatine MS, Smalling RW, Zieman SJ. 2014 AHA/ACC Guideline for the Management of Patients with Non-ST-Elevation Acute Coronary Syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014 Dec 23;64(24):e139-e228. doi: 10.1016/j.jacc.2014.09.017. Epub 2014 Sep 23. Erratum in: J Am Coll Cardiol. 2014 Dec 23;64(24):2713-4. Dosage error in article text.[↩]
- McGraw MD, Galambos C, Stillwell PC. Uremic pleuritis: A case report and review of recurrent exudative pleural effusions in children. Pediatr Pulmonol. 2017 Sep;52(9):E52-E54. doi: 10.1002/ppul.23708[↩]
- Jakubovic BD, Donovan A, Webster PM, Shear NH. Methotrexate-induced pulmonary toxicity. Can Respir J. 2013 May-Jun;20(3):153-5. doi: 10.1155/2013/527912[↩]
- Teerakanok J, Tantrachoti P, Chariyawong P, Nugent K. Acute Amiodarone Pulmonary Toxicity After Surgical Procedures. Am J Med Sci. 2016 Dec;352(6):646-651. doi: 10.1016/j.amjms.2016.08.013[↩]





{kind=link}