{kind=link}
Portal vein
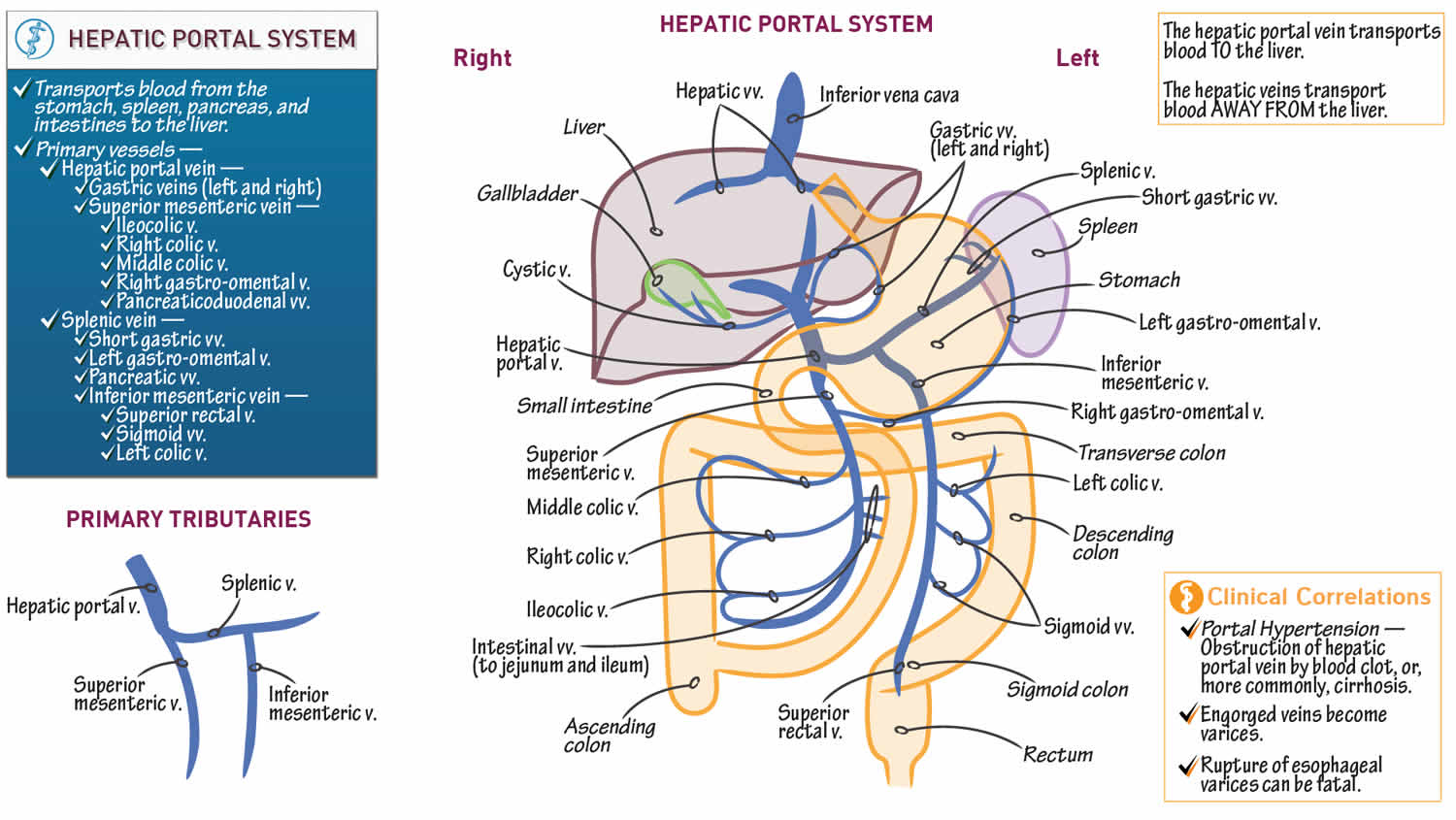
Portal vein sometimes referred to as the hepatic portal vein, is the main vessel in the portal venous system and drains blood from the gastrointestinal tract, spleen, pancreas, and gallbladder to the liver. The superior mesenteric and splenic veins unite to form the hepatic portal vein (see Figure 1). This special flow of venous blood, called the hepatic portal circulation. After passing through the liver for processing, blood drains into the hepatic veins, which empty into the inferior vena cava.
Portal vein anatomy
The portal vein usually measures approximately 8 cm in length in adults with a maximum diameter of 13 mm. The portal vein originates behind the neck of the pancreas where it is classically formed by the confluence of the superior mesenteric and splenic veins (the portovenous confluence), and also receives blood from the inferior mesenteric, gastric, and cystic veins.
Immediately before reaching the liver, the portal vein divides in the porta hepatis into left and right portal veins. The right portal vein divides into anterior (supplying segments V and VIII) and posterior (supplying segments VI and VII) branches. The left portal vein may be divided into transverse and umbilical portions, as delineated by the ligamentum venosum, and is mostly extrahepatic in course. The main branches of the left portal vein originate from the umbilical portion, and supply liver segments II, III, IV 1.
It ramifies further, forming smaller venous branches and ultimately portal venules. Each portal venule courses alongside a hepatic arteriole and the two vessels form the vascular components of the portal triad. These vessels ultimately empty into the hepatic sinusoids to supply blood to the liver.
75% of the blood supplied to the liver comes from the portal vein, but it only supplies 50% of the oxygen supply to the liver.
Portal vein variant anatomy
The overall incidence of portal vein variation is reported to be ~25% (range 20-30%), which should be recognized prior to procedures such as liver transplantation, complex hepatectomy and portal vein embolization 2:
- portal vein trifurcation (most common)
- portal vein divides into three branches: left portal vein, right anterior portal vein, and right posterior portal vein
- absent right portal vein (rare) 3
- right sectional portal veins originate independently from the common portal vein
- if the right anterior section portal vein branches higher from the common portal vein vs posterior sectional portal vein, the surgeon may mistake the posterior sectional portal vein for the right portal vein
- portal vein duplication (rare)
- absent left extrahepatic portal vein (rare) 3
- a single right portal vein originates from the porta hepatis, supplying the right hemiliver, then following an intrahepatic course with distalmost branches supplying the left liver.
There is an increased risk of bile duct hilar anatomical variation in the presence of portal vein variants.
Figure 1. Portal vein
Hepatic portal vein function
Like all portal systems, the hepatic portal vein delivers the digested nutrient-rich blood from your gastrointestinal tract into your liver for processing. The liver cells also break down toxins that enter the blood through the digestive tract. After passing through the liver sinusoids, the blood enters the hepatic veins and inferior vena cava, thereby reentering the general systemic circulation.
Portal vein embolization
Portal vein embolization is a technique used to selectively occlude the blood supply to one of the liver lobes, diverting portal blood flow to the other lobe, the future liver remnant.
This diversion will increase the size of the post-hepatectomy future liver remnant which improves surgical outcomes by preventing liver insufficiency. The minimum limit of the future liver remnant is 20–40% of total liver volume dependent on the presence of background liver disease 4.
Portal vein embolization is a procedure performed by interventional radiology.
Portal vein embolization indications
- Future liver remnant that would be too small for the patient’s body mass, post-hepatectomy (typically <20%)
- Elevated ICG-R15 serum values 15 minutes after injection
ICG (indocyanine green) binds to albumin and is excreted by the biliary system
elevated values imply decreased hepatic reserve - Patients who underwent hepatotoxic chemotherapy, if future liver remnant <30%
- Cirrhosis, Child-Pugh class A, ICG-R15 <10%, if future liver remnant <40%
- Patients with hepatic steatosis
- Concomitant pancreas resection and patients with diabetes due to poor post-hepatectomy hypertrophy rates
Portal vein embolization contraindications
- ipsilateral portal tumor thrombus precluding catheter placement
- clinically overt portal hypertension (procedure exacerbates portal hypertension)
Portal vein embolization procedure
Can be performed on an outpatient basis. The future liver remnant (on CT or MRI) should be obtained prior to undertaking this procedure.
Portal vein embolization technique
The right lobe is almost always targeted. The approach is usually through the right lobe, as well.
Different embolic agents have been used, including:
- n-butyl cyanoacrylate (NBCA)
- ethiodized oil
- fibrin glue
- ethanol
- microparticles (such as polyvinyl alcohol, PVA)
- microspheres followed by coils are used by some.
The portal vein can be approached surgically through a transileocolic approach, but interventional radiology usually approaches the portal vein transhepatically. Portal vein pressures are checked pre-procedure, to ensure that there is no portal hypertension.
Postprocedural care
- minor fluctuations in postprocedure liver function tests (50%)
- liver synthetic functions usually not affected
- nausea, fever, and pain are rare
Portal vein embolization complications
- reported 0% procedure-related mortality 5
- reported overall morbidity of 2.2% 5
- nontarget embolization
- complete portal vein thrombus
- risks similar to other transhepatic procedures
- hemobilia
- hemoperitoneum
- cholangitis
- subcapsular hematoma
- pneumothorax
Portal vein embolization prognosis
Patients with otherwise normal livers regenerate two weeks postprocedure at 12-21 cm³/ day (9 cm³/day for cirrhotic patients) 6. 2-4 weeks is usually enough for most patients with normal liver function (>4 weeks for patients with cirrhosis).
There is some evidence from volumetric analyzes to indicate that right portal vein embolization + segment 4 embolization results in a greater degree of hypertrophy of segments 2/3 than right portal vein embolization alone in patients with colorectal liver metastases and this may become the recommended strategy in those with a relatively low future liver remnant (<20%) and are planned to undergo an extended right hemihepatectomy 4.
Portal vein obstruction
Portal vein obstruction is a common complication of several metabolic and autoimmune diseases. It is most commonly the result of thrombosis of the portal vasculature, but it can also result from malignancies. Due to the vast range of diseases that result in portal vein obstruction, understanding the common causes, pathophysiologies, and relevant management is key to treating patients suffering from this disease.
The prevalence of portal vein obstruction varies in different populations. In patients with cirrhosis or portal hypertension, it is estimated to be anywhere between 1.6% and 15.8% 7. The incidence is higher where the cirrhosis results from alcohol use disorder or Hepatitis B infection. The prevalence is as low as 1% in patients with compensated liver cirrhosis 8, while as high as 25% in patients awaiting a liver transplant 9. Possible causes for the higher incidence in liver transplant patients include advanced underlying disease, immobility due to possibly worse ascites, and a higher degree of imbalance of clotting factors.
Portal vein obstruction causes
The causes of portal vein thrombosis can be divided into two categories; inherited and acquired.
Inherited portal vein thrombosis:
- Factor V Leiden mutation
- Prothrombin gene mutation
- Anti-thrombin III deficiency
- Protein C deficiency
- Protein S deficiency
Acquired portal vein thrombosis:
- Lupus anticoagulant syndrome
- Liver disease
- Iatrogenic
- Disseminated intravascular coagulation
- Burns
- Sepsis
- Malignancy
- Myeloproliferative disorders
- Peripartum
- Oral contraceptives
- Inflammatory states
Rare iatrogenic causes include bariatric surgery, radiofrequency ablation for hepatocellular carcinoma (liver cancer), or fine needle aspiration of pancreatic cancer 7.
Portal vein obstruction pathophysiology
The pathophysiology of portal vein obstruction depends upon the cause. In liver cirrhosis patients, endothelial dysfunction is implicated along with an imbalance of coagulation factors leading to a net hypercoagulable state. Blood samples of cirrhotic patients have been found to have high quantities of thrombin 10.
Similarly, stasis or low portal velocity has also been found to have an association with portal vein thrombosis 7. There could be an associated link with the use of beta blockers, but the results of a study demonstrating this link are yet to be replicated.
In cancer patients, the obstruction can occur due to thrombosis (from stasis or hypercoagulability caused by cancer) or direct invasion from a growing tumor.
Portal vein obstruction symptoms
Patients typically present with signs of portal hypertension. Although individual presentations vary depending on the cause, patients commonly demonstrate 11:
- Abdominal pain (91%)
- Fever (53%)
- Ascites (38%)
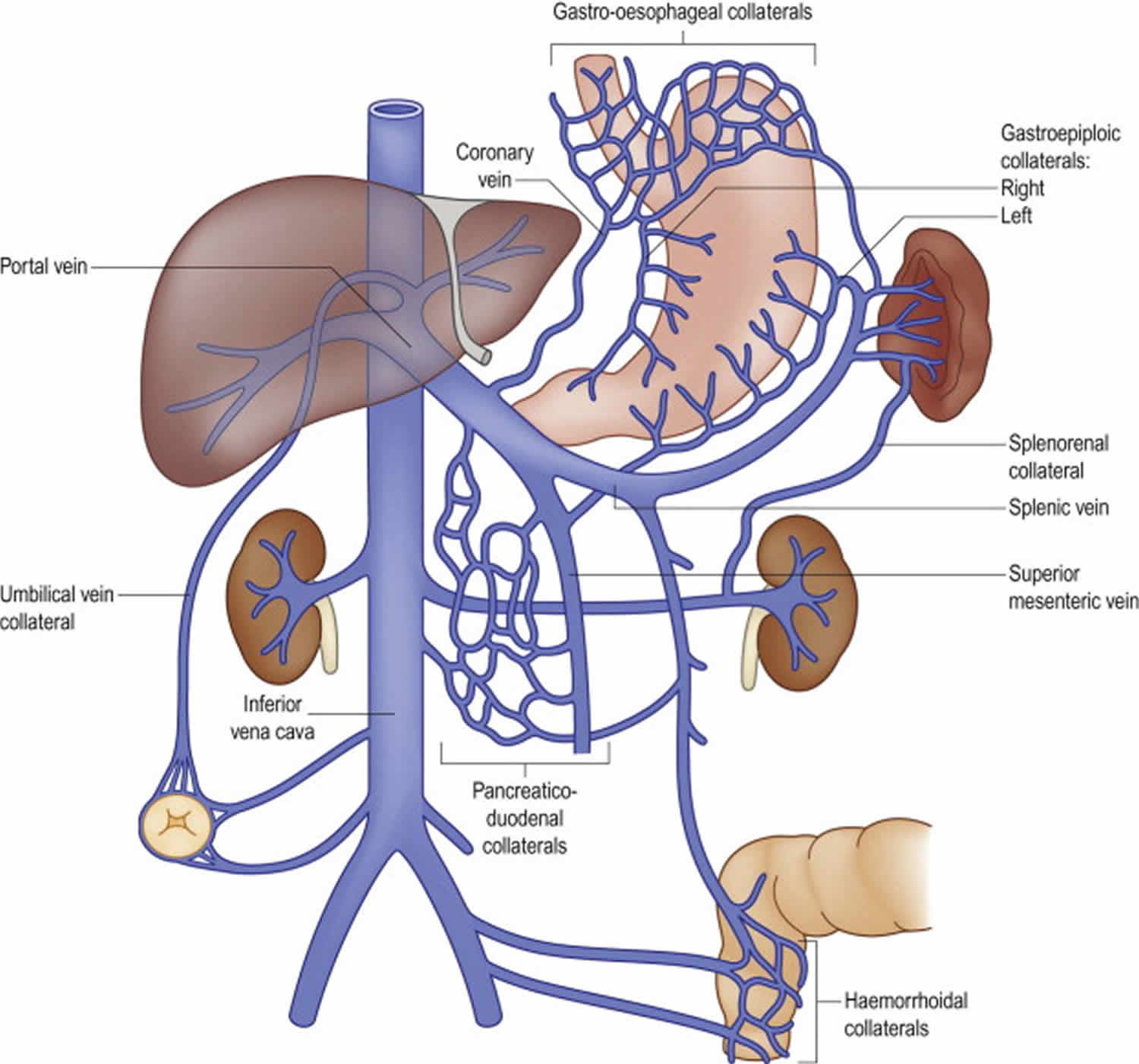
Depending upon the severity of the disease, splenomegaly will present in about 75 to 100% of patients. In patients with liver cirrhosis as the primary cause, signs such as spider angiomata and palmar erythema may be evident. If there has been longstanding portal hypertension, collaterals might be clinically evident with caput-medusae (umbilical veins), hemorrhoids (rectal veins), or in patients presenting with upper gastrointestinal bleeding from enlarged esophageal veins (varices).
In cases where malignancies are the primary cause, either from thrombus formation or direct invasion, clinical manifestations of the neoplasm could be prominent. In cases of pancreatic carcinoma, fatigue and jaundice are usually present. Similarly, jaundice is also present in hepatocellular carcinoma and cholangiocarcinoma. In patients with jaundice, associated pruritis is a common finding as well.
Portal vein obstruction complications
Complications of portal vein obstruction include:
Portal hypertension
- This can present in multiple forms, including ascites, variceal hemorrhage, or hypersplenism.
Mesenteric infarction
- Usually seen in acute portal vein thrombosis, leading to blockage of blood flow from the mesenteries.
Worsening hepatic function
- In patients with cirrhosis, portal vein obstruction can lead to worsening liver function.
Acute pylephlebitis
- Septic portal vein thrombosis can occur if there is a concurrent abdominal focus of infection (appendicitis, diverticulitis, etc.)
Portal vein obstruction diagnosis
When portal vein obstruction is suspected, several modalities can help confirm or exclude the diagnosis. The first line of investigation is Doppler ultrasound. Contrast-enhanced ultrasound seems to be superior to Doppler ultrasound for the characterization and further evaluation of portal vein obstruction 12.
Liver function tests are expected to be normal unless there is underlying liver disease. Other recommended blood tests should encompass extensive procoagulant factors workup, including antiphospholipid syndrome, protein C, S, antithrombin III levels, factor V, and Leiden mutation.
CT and MRI provide additional information such as the extension of thrombus, evidence of bowel infarction, and the status of adjacent organs. The sensitivity and specificity for MRI in detecting a primary portal vein thrombosis are 100% and 98%, respectively. MRI is valuable in determining the resectability of neoplasm involving the portal venous system and follow-up after therapeutic procedures 13.
Endoscopy is essential in patients with overt upper gastrointestinal bleeding and can be helpful in patients presenting with symptoms of gastritis. Esophageal varices are a common finding in patients with chronic portal vein obstruction. If identified early, esophageal varices can be cauterized or clipped to prevent potentially life-threatening hemorrhage.
Portal vein obstruction treatment
Treatment of thrombosis in cirrhosis patients can present a significant challenge as balancing anticoagulation with the risk of bleeding can be problematic. The Anticoagulation Forum recommends that cirrhotic patients with portal vein thrombosis should undergo endoscopic screening of esophageal varices and, if indicated, banding treatment should precede low molecular weight heparin (LMWH) treatment 14.
Choosing the right anticoagulant for a patient is difficult as well, as each agent has its benefits and risks. As cirrhotic patients have a raised international normalized ratio (INR) at baseline, monitoring warfarin treatment can be challenging. Despite some disadvantages, low molecular weight heparin and vitamin K antagonists have been successfully used to treat thrombosis in cirrhotic patients. According to the guidelines of the American Association for the Study of Liver Diseases, acute portal vein thrombosis should be treated for at least 3 months with low molecular weight heparin and switched to oral anticoagulant agents after patient stabilization. One study demonstrated partial or complete recanalization rates of up to 60% in cirrhotic patients treated early with low molecular weight heparin or vitamin K antagonists 15.
The use of vitamin K antagonists has been the object of study, but no target INR has been defined. The study quoted above used a target INR of 2.5 for the patient’s using warfarin. However, no data yet suggests what the goal INR should be for portal vein thrombosis patients treated with warfarin. With low molecular weight heparin being well-studied and not requiring monitoring, it might be the best option for some 16.
Despite recanalization, the possibility of recurrent DVT remains. One trial noted a recurrence rate of 38% after complete recanalization while another showed 27% 15.
Despite the interest in direct oral anticoagulants, there is insufficient data to recommend their use. There have been some in vitro and theoretical literature supporting their use, but studies establishing their safety and efficacy are lacking at the moment.
A transvenous intrahepatic portosystemic shunt (TIPS) is considered a highly effective and relatively safe treatment modality. In a recent study of 70 cirrhosis patients who received TIPS, partial and complete recanalization was found in 57% and 30% respectively 17. However, TIPS is associated with worse outcomes in liver transplant recipients. It is associated with increased post-transplant morbidity, graft loss, and mortality 18.
Other surgical modalities used in the treatment of portal vein occlusion associated with variceal bleeding include shunt surgery (such as splenorenal and mesogonadal) and the controversial Sugiura procedure. However, the Sugiura procedure is rarely an option 19.
One should keep in mind the possibility of liver nodules forming in patients undergoing shunt procedures. Such nodules are known to present in patients with congenital portosystemic shunts without liver disease 20.
For obstruction caused by local invasion, treatment of the underlying malignancy might be helpful. In patients with an obstruction due to pancreatic cancer, chemotherapy has led to recanalization and improvement in survival 21.
Portal vein obstruction prognosis
The overall prognosis is excellent, with 10-year mortality of 25% and an overall mortality rate of approximately 10%. In the presence of cirrhosis and malignancy, the prognosis is worse and is dependent upon the underlying condition.
Portal vein thrombosis
Portal vein thrombosis is a narrowing or blockage of the portal vein by a blood clot. Thrombosis can develop in the main body of the portal vein or its intrahepatic branches and may even extend to the splenic or superior mesenteric veins 22.
Portal vein thrombosis frequently occurs with cirrhosis of the liver 22. Portal vein thrombosis may also occur without an associated liver disease like malignancy, abdominal sepsis, pancreatitis, etc. The terminology of extra hepatic portal venous obstruction should be considered as a separate entity which refers to the development of portal cavernoma or collaterals around chronic portal vein thrombosis 22.
The prevalence of portal vein thrombosis in cirrhosis has been reported to be 0.6% to 16%, and more commonly reported in patients awaiting liver transplantation. portal vein thrombosis is seen in up to 35% of cirrhotic patients with hepatocellular carcinoma. The lifetime risk of portal vein thrombosis in the general population is reported to be 1% 7.
Portal vein thrombosis causes
Portal vein thrombosis, like thrombosis elsewhere, can occur due to disturbance of any one of the Virchow triad, and causes can be thought of in these terms 23:
Reduced flow / portal hypertension
- cirrhosis: most common
- hepatobiliary malignancies
- hepatocellular carcinoma (liver cancer)
- pancreatic ductal carcinoma, or other pancreatic neoplasms
- cholangiocarcinoma
- gastric carcinoma
- extrinsic compression by an adjacent tumor (bland thrombus) 24
Hypercoagulable state
- inherited prothrombotic conditions:
- protein S deficiency
- protein C deficiency
- factor V Leiden mutation
- antiphospholipid syndrome
- malignancy
- myeloproliferative disorders
- inflammatory bowel disease
- dehydration
- oral contraceptive pills
- pregnancy
- trauma
Endothelial disturbance
- local inflammation/infection (most common in some series) 25
- acute pancreatitis
- ascending cholangitis
- abdominal surgery
- perinatal omphalitis 26
Also, hepatocellular carcinoma (liver cancer) has a predilection for invading the portal vein, with tumor thrombus occluding the lumen 27.
The most common cause of portal vein thrombosis is liver cirrhosis. In a non-cirrhotic liver, portal vein thrombosis is mainly due to inherited or acquired pro-thrombotic states. Primary myeloproliferative disorders are the most common procoagulant state found. Other pro-thrombotic conditions that cause portal vein thrombosis include paroxysmal nocturnal hemoglobinuria, antiphospholipid syndrome, hyperhomocysteinemia, inherited pro-thrombotic disorders such as protein C, S and antithrombin 3 deficiencies, and less frequently, factor 5 Leiden mutation, factor 2 mutation, and methylenetetrahydrofolate reductase (MTHFR) gene mutation 28. Rare conditions that are associated with portal vein thrombosis are pregnancy, chronic inflammatory diseases, oral contraceptives, and malignancies with or without the above prothrombotic causes 29. Malignancy is responsible for portal vein thrombosis in around 25% of cases.
The intra-abdominal inflammatory conditions leading vascular endothelial injury can cause portal vein thrombosis. These include pancreatitis, cholangitis, appendicitis, and liver abscess. Local injury to portal venous axis following splenectomy, laparoscopic colectomy, or abdominal trauma with the above acquired or inherited pro-thrombotic conditions can lead to portal vein thrombosis.
Cause for extra hepatic portal venous obstruction in children is phlebosclerosis with thrombosis as a secondary event. Omphalitis, neonatal umbilical sepsis, umbilical vein cannulation, repeated abdominal infections, sepsis, abdominal surgery, and trauma later progress to extra hepatic portal venous obstruction 30.
Portal vein thrombosis pathophysiology
The pathophysiology of portal vein thrombosis encompasses one or more features of Virchow’s triad, which includes reduced portal blood flow, a hypercoagulable state, or vascular endothelial injury.
A confluence of splenic and superior mesenteric veins forms a portal vein, which carries blood from the spleen and small intestine to the liver. Patients with cirrhosis usually have slow blood flow through the severely scarred liver. Theses altered portal hemodynamics more likely to produce clot and can cause portal vein thrombosis.
Malignant portal vein obstruction is seen by direct vascular invasion by hepatocellular carcinoma, and cholangiocarcinoma or compression by tumor mass or lymph node are the other mechanisms involved.
Portal vein thrombosis symptoms
Portal vein thrombosis is asymptomatic in a majority of patients. Clinical presentation is often vague and non-specific. If extensive acute portal vein thrombosis is present, especially if the superior mesenteric venous system is also involved, then the presentation is likely to be with acute ischemic bowel, mimicking superior mesenteric artery occlusion.
Clinically portal vein thrombosis may be acute or chronic, although no time frame exists to distinguish acute from chronic portal vein thrombosis. Portal hypertension develops as a result of chronic obstruction to flow within the portal venous system. Portal hypertension can present with left upper quadrant abdominal fullness due to splenomegaly or upper gastrointestinal (GI) bleeding from esophageal or gastric varices.
Non-cirrhotic non-malignant acute portal vein thrombosis usually presents with abdominal pain (91%), fever (53%) and ascites (38%) 11. Extension of portal vein thrombus into a superior mesenteric vein may lead to intestinal ischemia, bowel infarction, ileus presenting as hematochezia, fever, and sepsis and is responsible for high mortality in this subset of patients.
If new portal vein thrombosis develops in people with cirrhosis, they present with hepatic decompensation in the form of ascites, jaundice or variceal bleeding. In patients with underlying cirrhosis, ascites usually develop when large amounts of fluids are given intravenously to treat massive bleeding from ruptured esophageal or gastric varices.
Patients with extra hepatic portal venous obstruction present with only portal hypertension-related complications like a well-tolerated upper GI bleed, splenomegaly, anemia, and thrombocytopenia or may be asymptomatic with incidental detection following an imaging procedure.
Portal vein thrombosis complications
Portal hypertension
Portal hypertension is responsible for the majority of the complications seen in patients with chronic portal vein thrombosis. It presents with splenomegaly, varices or ascites. Portal vein thrombosis commonly forms varices in sites other than the esophagus and stomach (ectopic varices).
Intestinal ischemia
Intestinal ischemia It is typically seen when acute portal vein thrombosis progresses to obstruction of mesenteric venous outflow with reflex arterial constriction and occlusion.
Septic Portal Vein Thrombosis
Septic portal vein thrombosis (acute pylephlebitis) occurs when portal vein thrombosis develops in a patient with an abdominal focus of an infection like appendicitis, diverticulitis, among others.
Portal Cholangiopathy
Portal cholangiopathy is a complication that may develop with longstanding portal vein thrombosis due to extrinsic compression of large bile ducts from venous collaterals around portal vein. It may progress to ischemic strictures of bile ducts presenting with obstructive jaundice and cholangitis 31.
Portal vein thrombosis diagnosis
Liver Function Tests
The liver functions are normal or near normal except if portal vein thrombosis occurs in a patient with cirrhosis. Portal hypertension due to chronic portal vein thrombosis may cause thrombocytopenia due to splenomegaly. Patients with portal biliopathy may show a rise in alkaline phosphatase and bilirubin.
Doppler Ultrasound
Doppler ultrasound is an investigation of choice with sensitivity and specificity ranging from 80% to 100% with an accuracy of 88% to 98%. It will show solid isoechoic or hypoechoic material within portal vein either filling the lumen partially or completely with the absence or reduced portal venous flow. Portal cavernoma will be seen as multiple tortuous small vessels replacing the portal vein suggestive of chronic portal vein thrombosis. Ultrasound will also pick up associated with splenomegaly. Contrast-enhanced ultrasound and endoscopic ultrasound are other modalities that have been found to be superior to ultrasound in demonstrating the presence or absence of flow in portal vein when it is very small.
Computed Tomography and Magnetic Resonance Imaging
CT and MRI provide additional information such as the extension of thrombus, evidence of bowel infarction and status of adjacent organs. CT scan with contrast also helps to distinguish bland thrombus from the malignant one. Bland thrombus is typically seen as a low density, non-enhancing defect within portal veins, while a tumor thrombus enhances following contrast administration with distension of vessel wall or intra-thrombus contrast enhancement due to neovascularization. The sensitivity and specificity of MRI for detecting the main portal vein thrombosis are 100% and 98%, respectively. It is valuable in determining the resectability of neoplasm involving the portal venous system and follow-up after therapeutic procedures.[6]. PET CT also has been shown to be helpful in differentiating benign and malignant portal vein obstruction.
Splenoportovenography
This is invasive, but now an obsolete procedure is done in the past which involves injecting dye in the splenic pulp and visualizing the splenoportal venous axis. It helps not only in diagnosing portal vein thrombosis but also identifying the patency of splenoportal axis for future splenorenal or mesocaval shunt surgery. In the pre-ultrasound/CT/MRI era, it was proved to be a safe procedure which also helped in measuring portal pressure.
Endoscopy
It is important to have an endoscopy in patients with portal vein thrombosis as portal hypertensive gastropathy is often present in the acute portal vein thrombosis with cancer or cirrhosis, while large ectopic/esophageal/gastric varices are present more often in patients with chronic portal vein thrombosis.
Procoagulant Workup
Once the diagnosis of portal vein thrombosis is made, the extensive investigation of prothrombotic disorders and local factors is recommended including antiphospholipid syndrome, protein C, S, antithrombin III levels, factor V, Leiden mutation, among others.
Portal vein thrombosis treatment
Anticoagulation
The aim of the treatment is to reverse or prevent advancement of thrombosis in the portal venous system and to treat complications of established portal vein thrombosis. There is a clear recommendation for the use of anticoagulation in non-cirrhotic acute portal vein thrombosis with good safety and efficacy data for both low molecular weight heparin new oral anticoagulants. However, the data in the setting of cirrhosis is limited. Anticoagulation is indicated with impending intestinal ischemia, decompensated liver disease awaiting liver transplantation, a compensated liver disease with a new diagnosis of acute portal vein thrombosis or portal vein thrombosis with asymptomatic mesenteric venous occlusion, while anticoagulation in non-transplant candidates with advanced liver disease and patients with portal cavernoma formation in the absence of thrombotic risk factors may not benefit survival. Enoxaparin was safe with no significant side effects or hemorrhagic events in cirrhosis. There is still not enough data with newer oral anticoagulants in cirrhosis as the majority are metabolized in the liver.
Thrombolysis
Thrombolytic therapy in very recent non-cirrhotic portal vein thrombosis can be done via indirect intraarterial infusion of tissue plasminogen activator, urokinase or streptokinase into the superior mesenteric artery (SMA) or directly via the catheter introduced into a portal vein either transhepatically or through transjugular approach 32. Prolonged catheterization of superior mesenteric artery may itself pose a risk of embolizing superior mesenteric artery and its arterial branches. Hence, direct access to portal vein via transjugular or percutaneous intrahepatic route is preferred mode as being less time-consuming and a more efficient technique with a requirement of a reduced dose of thrombolytics, thereby reducing the thrombolysis-related complications.
Thrombectomy
Surgical thrombectomy or mechanical thrombectomy by percutaneous transhepatic route is associated with recurrence of thrombosis from intimal or vascular trauma to the portal vein 33. Percutaneous transhepatic thrombo-aspiration within 72 hours has been done successfully in some patients.
Transvenous Intrahepatic Portosystemic Shunt
Transvenous intrahepatic portosystemic shunt (TIPS) placement in the setting of portal vein thrombosis is technically challenging for radiologists. However, when placed successfully, there is a possibility of achieving recanalization by disrupting the thrombus and mechanical thrombectomy.
Portal vein thrombosis prognosis
In acute non-cirrhotic portal vein thrombosis with an early diagnosis with improved diagnostic techniques and use of early anticoagulation, the 5-year survival rate has now improved to 85%. The outcome of portal vein thrombosis is good, and mortality primarily is due to an underlying cause or as consequences of portal hypertension. Acute portal vein thrombosis usually has a good prognosis if it does not progress to intestinal infarction. In chronic extrahepatic portal vein thrombosis, bleeding-related mortality is much lower due to preserved liver function compared to cirrhosis. In contrast, portal vein thrombosis in a patient with cirrhosis, 2-year survival is reduced by 55% secondary to hepatic dysfunction.
Portal vein hypertension
Portal hypertension is increased pressure within the portal venous system 34. Normal portal venous pressure is 5 to 10 millimeters of mercury. The portal venous pressure should never exceed the pressure within the inferior vena cava or the hepatic vein by 5 millimeters of mercury or more. A pressure gradient of 6 millimeters of mercury or more between the portal and hepatic veins (or inferior vena cava) suggests the presence of portal hypertension in most cases. This gradient is measured by determination of the hepatic venous pressure gradient. Portal hypertension develops when resistance to portal blood flow increases. This resistance often occurs within the liver, as in cirrhosis. It can also be outside of the liver, such as prehepatic in portal vein thrombosis or posthepatic in the case of constrictive pericarditis or Budd-Chiari syndrome. Identification of the level of resistance to portal blood flow allows determination of the cause of portal hypertension. Portal hypertension is the most frequent cause of hospitalization, variceal bleed, liver transplantation, and death in patients with cirrhosis.
Cirrhosis of the liver is the most prevalent cause of portal hypertension in the Western world. However, schistosomiasis is the most frequent cause in the African continent where schistosomiasis is endemic.
Portal vein hypertension causes
Numerous causes of portal hypertension exist. The cause can be classified as prehepatic, intrahepatic, or posthepatic reasons.
The common causes of pre-hepatic portal hypertension are either due to increased blood flow or obstruction within the portal vein or splenic vein. Instances of increased blood flow include idiopathic tropical splenomegaly, arterio-venous malformations, or fistula. A blockage within the portal or splenic vein may be due to thrombosis or to invasion or compression of these veins by the tumor.
Intrahepatic portal hypertension causes are classified into pre-sinusoidal, sinusoidal, or post-sinusoidal. Pre-sinusoidal intrahepatic causes can be produced by schistosomiasis, congenital hepatic fibrosis, early primary biliary cholangitis, sarcoidosis, chronic active hepatitis, and toxins such as vinyl chloride, arsenic, and copper. Sinusoidal causes arise from cirrhosis, alcoholic hepatitis, vitamin A intoxication, or cytotoxic drugs. Post-sinusoidal causes result from sinusoidal obstruction syndrome or veno-occlusive disease.
Finally, posthepatic portal hypertension causes can be at the level of the heart, hepatic vein, as in Budd-Chiari syndrome, or inferior vena cava. Posthepatic causes at the level of the heart are due to a rise in atrial pressure, as in constrictive pericarditis. If these causes occur the level of the inferior vena cava, it is due to stenosis, thrombosis, webs or tumor invasion.
Portal vein hypertension pathophysiology
The superior mesenteric vein and splenic vein join to form the portal vein. It drains into the liver before dividing into right and left portal veins into both lobes respectively. It supplies two-thirds of the blood to the liver. The portal vein pressure is typically between 1 to 4 millimeters of mercury more than hepatic vein pressure. This pressure differential enables blood to flow through the liver into the systemic circulation. The veins do not have valves. If there is resistance to the flow of blood in the portal venous tract, it leads to elevated portal venous pressure as seen in portal hypertension. The resistance occurs more commonly within the liver as seen in cirrhosis, but it can also be pre-hepatic or post-hepatic.
The increased resistance within the organ can be due to structural or dynamic changes. Structural changes are due to the alteration of the hepatic microcirculation. Such an alteration is caused by hepatic stellate cell activation and the resultant fibrosis, regenerative nodules, vascular occlusion, and angiogenesis. The increased production of endothelial vasoconstrictors and decreased release of vasodilators within the liver leads to sinusoidal constriction. Portal hypertension stemming from this is augmented and perpetuated by the increased blood flow within the splanchnic circulation. This increased blood flow is due to the increased release of splanchnic vasodilators because of increased shear stress and reduced effective arterial volume. Thus portal hypertension is a result of both increased resistance to portal venous flow and increased portal blood flow due to splanchnic vasodilation. When the portal pressure remains elevated, developing collaterals attempt to reduce it.
Portal vein hypertension symptoms
Patients usually have no symptoms until complications arise. Hematemesis from bleeding varices is the most common presentation. Melena without hematemesis can also be present. As cirrhosis is the most common cause of portal hypertension, patients may present with stigmata of cirrhosis. These include jaundice, gynecomastia, palmar erythema, spider nevi, testicular atrophy, ascites, pedal edema, or asterixis due to hepatic encephalopathy. Prominent abdominal wall veins may be visible, which is an attempt to divert the portal blood flow via the paraumbilical veins into the caval system. In caput medusae, the blood flow is away from the umbilicus. However, in inferior venacaval obstruction, the blood flow is toward the umbilicus to reach the superior venacaval system. A venous hum may be heard near the xiphoid process or umbilicus. Cruveilhier-Baumgarten syndrome is characterized by dilated abdominal wall veins and a low venous murmur at the umbilicus. An arterial systolic murmur is often due to hepatocellular carcinoma or alcoholic hepatitis. Splenomegaly is a reliable sign in the diagnosis of portal hypertension. If the spleen is not enlarged on physical examination or imaging studies, the diagnosis of portal hypertension should be questioned. The pancytopenia seen with hypersplenism is due to reticuloendothelial hyperplasia. Therefore, it cannot be reversed by the reduction of portal hypertension via a portocaval shunt. While a firm liver supports a diagnosis of cirrhosis, hepatomegaly does not correlate with the severity of portal hypertension.
Portal hypertension complications
Complications of portal hypertension include:
- Thrombocytopenia due to congestive hepatopathy
- Abdominal wall collaterals
- Variceal bleeding secondary to hemorrhage from gastroesophageal, anorectal, retroperitoneal, stomal, and other varices
- Acute bleeding or iron deficiency anemia due to chronic blood loss from portal hypertensive gastropathy, enteropathy, or coagulopathy
- Ascites
- Spontaneous bacterial peritonitis
- Hepatic hydrothorax
- Hepatorenal syndrome
- Hepatic encephalopathy
- Hepatopulmonary syndrome
- Portopulmonary hypertension
- Cirrhotic cardiomyopathy
Portal vein hypertension diagnosis
The diagnosis requires obtaining a good history and utilizing the relevant lab data. A complete blood count helps to distinguish the presence of thrombocytopenia which is secondary to hypersplenism and anemia from gastrointestinal blood loss. A complete metabolic panel identifies renal failure and liver enzyme elevation present in liver disease, viral hepatitis, and also hypoalbuminemia. A coagulation profile helps to identify the synthetic function of the liver. A prolonged prothrombin time, together with a low serum albumin level, reliably predicts hepatic synthetic function. Dopplers of portal vein can detect the presence of stenosis or thrombosis. An abdominal ultrasound can find evidence of cirrhosis of the liver, ascites, and splenomegaly. An endoscopy helps to look for the presence of varices. Finally, patients who present with ascites need paracentesis to determine their etiology, and to rule out spontaneous bacterial peritonitis.
Measurement of portal pressure is often not needed to make a diagnosis of portal hypertension in cases where clinical signs and symptoms are readily manifest. The patency of the portal and hepatic veins may be assessed by duplex Doppler ultrasound, magnetic resonance, or computed tomography angiography. Direct measurement of portal pressure is invasive, expensive, and complicated. The indirect method of portal pressure determination is thus the preferred method. It is often achieved by cannulation of the hepatic vein and measurement of free hepatic vein pressure, followed by balloon occlusion of the hepatic vein and measurement of the wedged hepatic vein pressure. These measurements are used to calculate the hepatic venous pressure gradient.
Portal vein hypertension treatment
Management of portal hypertension depends on its cause. If there are reversible causes, they should be attempted to be corrected. For example, if there is thrombosis in the portal vein or the inferior vena cava due to a hypercoagulable state, it needs anticoagulation.
Other treatment options are based on concurrent complications. Patients who have cirrhosis of the liver should undergo endoscopy to screen for varices. If large varices or varices with high-risk stigmata are present, the patient should start therapy with non-selective beta-blockers and/or endoscopic variceal ligation. Patients with an acute variceal bleed should receive endoscopic therapy or the placement of a transjugular intrahepatic portosystemic shunt. They should also start taking empiric antibiotics for prophylaxis against spontaneous bacterial peritonitis. Ascites treatments depend on the severity of the underlying liver disease and the patient’s response to therapy. These treatments include dietary sodium restriction, diuretics such as spironolactone in combination with furosemide, large volume paracentesis, transjugular intrahepatic portosystemic shunt placement, and liver transplantation. The definitive treatment for portal hypertension caused by cirrhosis is liver transplantation.
Portal vein hypertension prognosis
The prognosis depends on the underlying cause of portal hypertension.
References- Strasberg, Steven. Hepatic, biliary and pancreatic anatomy. In: Garden JO, Parks RW, ed. Hepatobiliary and Pancreatic Surgery. : Elsevier; 2013: 17-38.
- Sureka B, Patidar Y, Bansal K et-al. Portal vein variations in 1000 patients: surgical and radiological importance. Br J Radiol. 2015;88 (1055): 20150326. doi:10.1259/bjr.20150326
- Strasberg, Steven. Hepatic, biliary and pancreatic anatomy. In: Garden JO, Parks RW, ed. Hepatobiliary and Pancreatic Surgery. : Elsevier; 2013: 17-38
- Christopher J. Hammond, Saadat Ali, Hafizul Haq, Lorna Luo, Judith I. Wyatt, Giles J. Toogood, J. Peter A. Lodge, Jai V. Patel. Segment 2/3 Hypertrophy is Greater When Right Portal Vein Embolisation is Extended to Segment 4 in Patients with Colorectal Liver Metastases: A Retrospective Cohort Study. (2019) CardioVascular and Interventional Radiology. 42 (4): 552
- Abulkhir A, Limongelli P, Healey AJ et-al. Preoperative portal vein embolization for major liver resection: a meta-analysis. Ann. Surg. 2008;247 (1): 49-57. doi:10.1097/SLA.0b013e31815f6e5b
- Madoff DC, Hicks ME, Vauthey JN et-al. Transhepatic portal vein embolization: anatomy, indications, and technical considerations. Radiographics. 2002;22 (5): 1063-76. doi:10.1148/radiographics.22.5.g02se161063
- Mantaka A, Augoustaki A, Kouroumalis EA, Samonakis DN. Portal vein thrombosis in cirrhosis: diagnosis, natural history, and therapeutic challenges. Ann Gastroenterol. 2018 May-Jun;31(3):315-329
- Okuda K, Ohnishi K, Kimura K, Matsutani S, Sumida M, Goto N, Musha H, Takashi M, Suzuki N, Shinagawa T. Incidence of portal vein thrombosis in liver cirrhosis. An angiographic study in 708 patients. Gastroenterology. 1985 Aug;89(2):279-86
- Nonami T, Yokoyama I, Iwatsuki S, Starzl TE. The incidence of portal vein thrombosis at liver transplantation. Hepatology. 1992 Nov;16(5):1195-8.
- Delahousse B, Labat-Debelleix V, Decalonne L, d’Alteroche L, Perarnau JM, Gruel Y. Comparative study of coagulation and thrombin generation in the portal and jugular plasma of patients with cirrhosis. Thromb. Haemost. 2010 Oct;104(4):741-9
- Plessier A, Darwish-Murad S, Hernandez-Guerra M, Consigny Y, Fabris F, Trebicka J, Heller J, Morard I, Lasser L, Langlet P, Denninger MH, Vidaud D, Condat B, Hadengue A, Primignani M, Garcia-Pagan JC, Janssen HL, Valla D., European Network for Vascular Disorders of the Liver (EN-Vie). Acute portal vein thrombosis unrelated to cirrhosis: a prospective multicenter follow-up study. Hepatology. 2010 Jan;51(1):210-8
- Danila M, Sporea I, Popescu A, Șirli R. Portal vein thrombosis in liver cirrhosis – the added value of contrast enhanced ultrasonography. Med Ultrason. 2016 Jun;18(2):218-33.
- Lin J, Zhou KR, Chen ZW, Wang JH, Wu ZQ, Fan J. Three-dimensional contrast-enhanced MR angiography in diagnosis of portal vein involvement by hepatic tumors. World J. Gastroenterol. 2003 May;9(5):1114-8
- Ageno W, Beyer-Westendorf J, Garcia DA, Lazo-Langner A, McBane RD, Paciaroni M. Guidance for the management of venous thrombosis in unusual sites. J. Thromb. Thrombolysis. 2016 Jan;41(1):129-43
- Delgado MG, Seijo S, Yepes I, Achécar L, Catalina MV, García-Criado A, Abraldes JG, de la Peña J, Bañares R, Albillos A, Bosch J, García-Pagán JC. Efficacy and safety of anticoagulation on patients with cirrhosis and portal vein thrombosis. Clin. Gastroenterol. Hepatol. 2012 Jul;10(7):776-83
- Amitrano L, Guardascione MA, Menchise A, Martino R, Scaglione M, Giovine S, Romano L, Balzano A. Safety and efficacy of anticoagulation therapy with low molecular weight heparin for portal vein thrombosis in patients with liver cirrhosis. J. Clin. Gastroenterol. 2010 Jul;44(6):448-51
- Luca A, Miraglia R, Caruso S, Milazzo M, Sapere C, Maruzzelli L, Vizzini G, Tuzzolino F, Gridelli B, Bosch J. Short- and long-term effects of the transjugular intrahepatic portosystemic shunt on portal vein thrombosis in patients with cirrhosis. Gut. 2011 Jun;60(6):846-52
- Englesbe MJ, Schaubel DE, Cai S, Guidinger MK, Merion RM. Portal vein thrombosis and liver transplant survival benefit. Liver Transpl. 2010 Aug;16(8):999-1005
- Selzner M, Tuttle-Newhall JE, Dahm F, Suhocki P, Clavien PA. Current indication of a modified Sugiura procedure in the management of variceal bleeding. J. Am. Coll. Surg. 2001 Aug;193(2):166-73
- Pupulim LF, Vullierme MP, Paradis V, Valla D, Terraz S, Vilgrain V. Congenital portosystemic shunts associated with liver tumours. Clin Radiol. 2013 Jul;68(7):e362-9.
- Jaseanchiun W, Kato H, Hayasaki A, Fujii T, Iizawa Y, Tanemura A, Murata Y, Azumi Y, Kuriyama N, Kishiwada M, Mizuno S, Usui M, Sakurai H, Isaji S. The clinical impact of portal venous patency ratio on prognosis of patients with pancreatic ductal adenocarcinoma undergoing pancreatectomy with combined resection of portal vein following preoperative chemoradiotherapy. Pancreatology. 2019 Mar;19(2):307-315
- Samant H, Garfield K. Portal Vein Thrombosis. [Updated 2019 Mar 18]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK534157
- Janssen HL, Wijnhoud A, Haagsma EB et-al. Extrahepatic portal vein thrombosis: aetiology and determinants of survival. Gut. 2001;49 (5): 720-4. doi:10.1136/gut.49.5.720
- Wolfgang Dähnert. Radiology Review Manual. (2011) ISBN: 9781609139438
- Sheen CL, Lamparelli H, Milne A et-al. Clinical features, diagnosis and outcome of acute portal vein thrombosis. QJM. 2000;93 (8): 531-4. doi:10.1093/qjmed/93.8.531
- Chawla YK, Bodh V. Portal vein thrombosis. (2015) Journal of clinical and experimental hepatology. 5 (1): 22-40. doi:10.1016/j.jceh.2014.12.008
- Lee JK. Computed body tomography with MRI correlation. Lippincott Williams & Wilkins. (2006) ISBN:0781745268
- Salembier A, Verhamme M, Verhamme P, Van Moerkercke W. Acute non-cirrhotic portal vein thrombosis : review. Acta Gastroenterol. Belg. 2018 Apr-Jun;81(2):318-322
- Denninger MH, Chaït Y, Casadevall N, Hillaire S, Guillin MC, Bezeaud A, Erlinger S, Briere J, Valla D. Cause of portal or hepatic venous thrombosis in adults: the role of multiple concurrent factors. Hepatology. 2000 Mar;31(3):587-91
- Chawla YK, Bodh V. Portal vein thrombosis. J Clin Exp Hepatol. 2015 Mar;5(1):22-40
- Gebreselassie A, Bukhari M, Awan A, Khashab M. Recurrent Biliary Obstruction Secondary to Portal Biliopathy and the Role of Cholagioscopy: A Case Report. Cureus. 2018 Jan 09;10(1):e2046
- Wolter K, Decker G, Kuetting D, Trebicka J, Manekeller S, Meyer C, Schild H, Thomas D. Interventional Treatment of Acute Portal Vein Thrombosis. Rofo. 2018 Aug;190(8):740-746
- Rosenqvist K, Ebeling Barbier C, Rorsman F, Sangfelt P, Nyman R. Treatment of acute portomesenteric venous thrombosis with thrombectomy through a transjugular intrahepatic portosystemic shunt: a single-center experience. Acta Radiol. 2018 Aug;59(8):953-958
- Oliver TI, John S. Hypertension, Portal. [Updated 2018 Oct 27]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK507718