Rinne test
Rinne test is a hearing test used to evaluate the conductive hearing loss in one ear 1. Rinne test compares perception of sounds, as transmitted by air or by sound conduction through the mastoid. Thus, one can quickly suspect conductive hearing loss. The Rinne test differentiates sounds transmitted by air conduction from those transmitted through the mastoid by bone conduction. A Rinne test should be done with a Weber test to detect a sensorineural hearing loss and thus confirm the nature of hearing loss 2. It is important to note that the Weber and Rinne tests are screening tests and do not replace formal audiometry.
In addition, the validity of the Rinne test as a screening test is often questioned. The Rinne test is not sensitive in differentiating conductive and sensorineural loss causes of total sensorineural or severe unilateral hearing loss. False negatives are common in such situations. In any situation where there is a question about the Rinne test, the patient must be referred to an ear, nose, and throat (ENT) surgeon for formal audiometry.
The other important fact about the Rinne test is that the technique is not uniform. The orientation of the tuning fork and its exact placement vary from individual to individual. All physicians who perform the Rinne test must pay attention to the orientation of the tines of the tuning fork with respect to the long axis of the external auditory canal when testing for air conduction.
Rinne test bone conduction technique
- Place the vibrating tuning fork (512 Hz) on the mastoid process.
- The patient should be asked to cover the opposite ear with their hand.
- The patient should report when the sound can no longer be heard
- Then move the vibrating tuning fork over the ear canal to the ear without touching it.
- The patient should indicate when air conduction of the sound can no longer be heard.
Figure 1. Rinne test

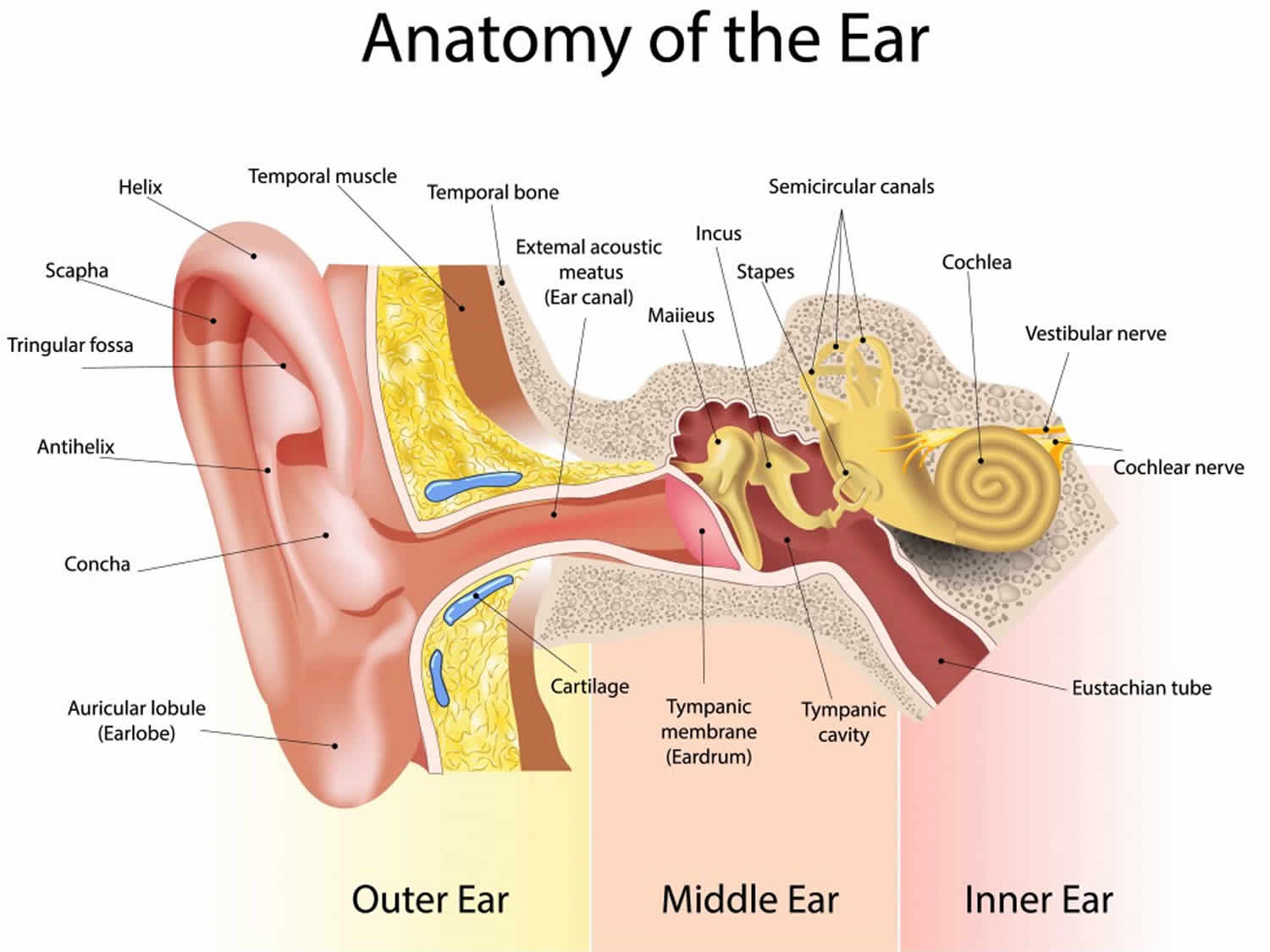
Ear hearing anatomy
The ear anatomically consists of the sound-conducting system (outer and middle ear) and sound-transducing system (the cochlea).
- The outer ear: Pinna and external ear canal
- The middle ear: Tympanic membrane, ossicular chain (malleus, incus, stapes) and middle ear space
- The inner ear: Cochlea (organ of hearing), vestibular labyrinth (organ of balance)
The purpose of the outer ear is to direct sounds onto the tympanic membrane. The sound vibrations are then transmitted through the middle ear via the ossicular chain before it reaches the cochlea. The cochlea plays an important role in transducing these vibrations into nerve impulses via the auditory nerve (vestibulocochlear nerve) which is then delivered along the central pathways to the auditory cortex where it is processed and perceived as sound. This pathway is termed air conduction. However, sound can also be transmitted via bone conduction where vibrations are transmitted via the skull and delivered directly to the cochlea which is buried within the temporal bone.
Hearing loss may occur due to interruption at any point along these pathways.
Figure 2. Ear anatomy
Rinne test results
The Rinne test is performed by placing a vibrating tuning fork (512 Hz) initially on the mastoid, then next to the ear and asking which sound is loudest. Air conduction uses the apparatus of the ear (pinna, eardrum and ossicles [malleus, incus, and stapes]) to amplify and direct the sound whereas bone conduction bypasses some or all of these and allows the sound to be transmitted directly to the inner ear albeit at a reduced volume, or via the bones of the skull to the opposite ear.
- Air conduction (AC) uses the apparatus of the ear (eardrum, pinna, and ossicles) to amplify and direct the sound.
- Bone conduction (BC) allows the vibration sound to be transmitted to the inner ear. There is reduced volume transmitted by to the bones of the skull to the other ear.
Before performing the Rinne test, it is important to know that in normal hearing, air conduction (AC) that is greater than bone conduction (BC). This means that the individual will be able to hear the tuning fork when it is placed near the outer ear, even after that are no longer able to hear it when held against the mastoid.
In a normal ear, air conduction (AC) is better than bone conduction (BC)
- Air conduction (AC) > bone conduction (BC), and this is called a positive Rinne test.
- Air conduction should be better than bone conduction, and air conduction should persist twice as long as bone, this is a “positive test.”
- No conductive hearing loss
In conductive hearing loss, bone conduction (BC) is better than air conduction (AC)
- Bone conduction (BC) > air conduction (AC), a negative Rinne test.
In sensorineural hearing loss, bone conduction and air conduction are both equally depreciated, maintaining the relative difference of:
- Air conduction (AC) > bone conduction (BC), and this is called a positive Rinne test.
In total sensorineural hearing loss patients there may be a false negative Rinne test
- In this case the sound of the tuning fork is transmitted across the skull via bone conduction and is perceived by the patient’s contralateral ear. This is termed a false-negative Rinne test.
Rinne test interpretation
The tuning fork (512 Hz) will be perceived as being louder when placed at the external auditory meatus.
- Rinne Positive: The patient is positive on that side (the ossicular chain is doing what it should be doing, acting as an amplifier). If the bone conduction through the mastoid process is heard louder than through the air, then the patient is Rinne negative. This is always abnormal.
- If the patient has negative or abnormal Rinne negative, air vibrations are not being transmitted across the external auditory canal, the tympanic membrane, the ossicular chain, or the oval window.
Causes in the external auditory canal:
- Wax in the external canal
- Otitis externa or outer ear canal infection
- Foreign body in ear canal
Causes due to the tympanic membrane (eardrum):
- Perforation of the drum due to trauma or infection
Causes in the middle ear:
- Infection (acute otitis media) in the middle ear
- Serous otitis media (glue ear) can result from repeated episodes of acute otitis media.
Causes at the oval window:
- Otosclerosis results in the failure of transmission of sound from the stapes through the oval window due to abnormal bone growth.
A patient with profound sensorineural deafness may have a false negative Rinne. With complete loss of innervation to that ear, the patient will not hear anything from the tuning fork on the mastoid or near the canal. The patient sound transmission through their skull to the other ear on the other side and they may not be able to identify in which ear they hear the sound.
It seems that bone conduction is better than air conduction, but the ear is nonfunctional.
The way to determine the difference between a true and a false Rinne negative test is to perform Weber test.
False Negative Rinne test
Sometimes the Rinne test may be falsely negative in the following situations:
- Total unilateral sensorineural hearing loss. For example, if the left ear is completely dead, on testing, the bone conduction on the left, the sound waves travel to the good right ear, and the sounds are louder when the tuning fork is held next to the external auditory meatus on the side being tested (left). The patient, in this case, will state that bone conduction is louder than air conduction, giving a falsely negative Rinne test.
Weber test
Weber test is a quick screening test to detect unilateral conductive and sensorineural hearing loss 2. The Weber test is a test of lateralization and is of most value useful in those with an asymmetrical hearing loss. Weber test can detect unilateral (one-sided) conductive hearing loss and unilateral sensorineural hearing loss. The outer and middle ear mediate conductive hearing. The inner ear mediates sensorineural hearing. The Weber test is always combined with the Rinne test to detect the location and nature of hearing loss.
In the Weber test a tuning fork (either 256 or 512 Hz) is struck and the stem of the fork is placed on the top of the patient’s skull – equal distance from the patient’s ears, in the middle of the forehead – equal distance from the patient’s ears or above the upper lip over the teeth. The patient is asked to report in which ear the sound is heard louder.
Performing Weber Test 3
- Place the vibrating tuning fork on the vertex (other common sites used are the midline of the forehead, bridge of the nose, and chin), equidistant from both ears. These vibrations will be conducted through the skull and reach the cochlea.
- Ask the patient whether it is heard loudest in either one side or the midline (e.g., “Is the sound louder in your right ear, left ear, or the middle?”)
In clinical practice, the 512-Hz tuning fork has traditionally been preferred. At this frequency, it provides the best balance of time of tone decay and tactile vibration. Lower-frequency tuning forks like the 256-Hz tuning fork provide greater tactile vibration. In other words, they are better felt than heard. However, evidence suggests that the 256-Hz provides better reliability when compared to the 512-Hz 4. Higher-frequency tuning forks, for example, the 1024-Hz tuning fork, have a shorter tone decay time.
A patient with a unilateral sensorineural hearing loss would hear the sound loudest in the unaffected ear, because the affected ear is less effective at picking up sound even if it is transmitted directly by conduction into the inner ear.
Weber test is most useful in individuals with hearing that is different between the two ears. Weber test cannot confirm normal hearing because it does not measure sound sensitivity in a quantitative manner. Hearing defects affecting both ears equally, as in presbycusis will produce an apparently normal test result.
The inner ear is more sensitive to sound via air conduction than bone conduction (in other words, air conduction is better than bone conduction).
In the presence of a purely unilateral conductive hearing loss, there is a relative improvement in the ability to hear a bone-conducted sound. This can be explained by the following:
- Masking effect: The sound heard via the affected ear has less environmental noise reaching the cochlea via air conduction (for example, the environmental noise is masked) as compared to the unaffected ear which receives sounds from both bone conduction and air conduction. Therefore, the affected ear is more sensitive to bone-conducted sound.
- Occlusion effect: Most of the sound transmitted via bone conduction travels through to the cochlea. However, some of the low-frequency sounds dissipate out of the canal. A conductive hearing loss (in other words, when an occlusion is present) will, therefore, prevent external dissipation of these frequencies and lead to increased cochlear stimulation and increased loudness in the affected ear.
In the presence of sensorineural hearing loss, the sound will be perceived louder in the unaffected ear which has the better cochlear.
Figure 3. Weber test

Weber test interpretation
Normal hearing
- Weber test does not demonstrate lateralization: In a normal subject, the sound should be heard in the middle and equally on both sides.
- Rinne test: Normal/positive in both ears [Air conduction (AC) greater than bone conduction (BC)]
Unilateral sensorineural hearing loss
- Weber test lateralizes to the unaffected ear, in other words, it is heard louder in the better ear.
- Rinne test: Normal/positive on the affected ear [air conduction (AC) greater than bone conduction (BC)]; normal/positive on the unaffected ear (AC greater than BC)
Note: an abnormal/negative response on the affected ear [bone conduction (BC) greater than air conduction (AC)] can also occur in a severe sensorineural hearing loss, also called a dead ear. This is termed a “false negative.” Rinne “true negative” only occurs if there is a conductive hearing loss element. However, when testing a dead ear, the bone conduction is perceived to be heard louder than air conduction due to cross-over of bone conduction detected by the opposite normal-functioning cochlear, resulting in a Rinne false negative.
Unilateral conductive hearing loss
- Weber test lateralizes to the affected ear, in other words, it is heard louder in the poorer ear.
- Rinne test: Abnormal/negative on the affected ear [bone conduction (BC) greater than air conduction (AC)]; normal/positive on the unaffected ear [air conduction (AC) greater than bone conduction (BC)]
A patient with a unilateral (one-sided) conductive hearing loss would hear the tuning fork loudest in the affected ear. This is because the conduction problem masks the ambient noise of the room, whilst the well-functioning inner ear picks the sound up via the bones of the skull causing it to be perceived as a louder sound than in the unaffected ear. Another theory, however, is based on the occlusion effect described by Tonndorf et al in 1966. Lower frequency sounds (as made by the 512Hz fork) that are transferred through the bone to the ear canal escapes from the canal. If an occulusion is present, the sound cannot escape and appears louder on the ear with the conductive hearing loss
Conductive hearing loss can be mimicked by plugging one ear with a finger and performing the Rinne and Weber tests, which will help clarify the above.
Symmetrical conductive hearing loss
- Weber test does not demonstrate lateralization
- Rinne test: Abnormal/negative on the affected ear [bone conduction (BC) greater than air conduction (AC)]
- Kong EL, Fowler JB. Rinne Test. [Updated 2019 Jun 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK431071[↩]
- Wahid NWB, Attia M. Weber Test. [Updated 2019 Feb 19]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK526135[↩][↩]
- Recommended procedure for Rinne and Weber tuning-fork tests. British Society of Audiology. Br J Audiol. 1987 Aug;21(3):229-30.[↩]
- Browning GG, Swan IR, Chew KK. Clinical role of informal tests of hearing. J Laryngol Otol. 1989 Jan;103(1):7-11.[↩]





{kind=link}