Splenomegaly
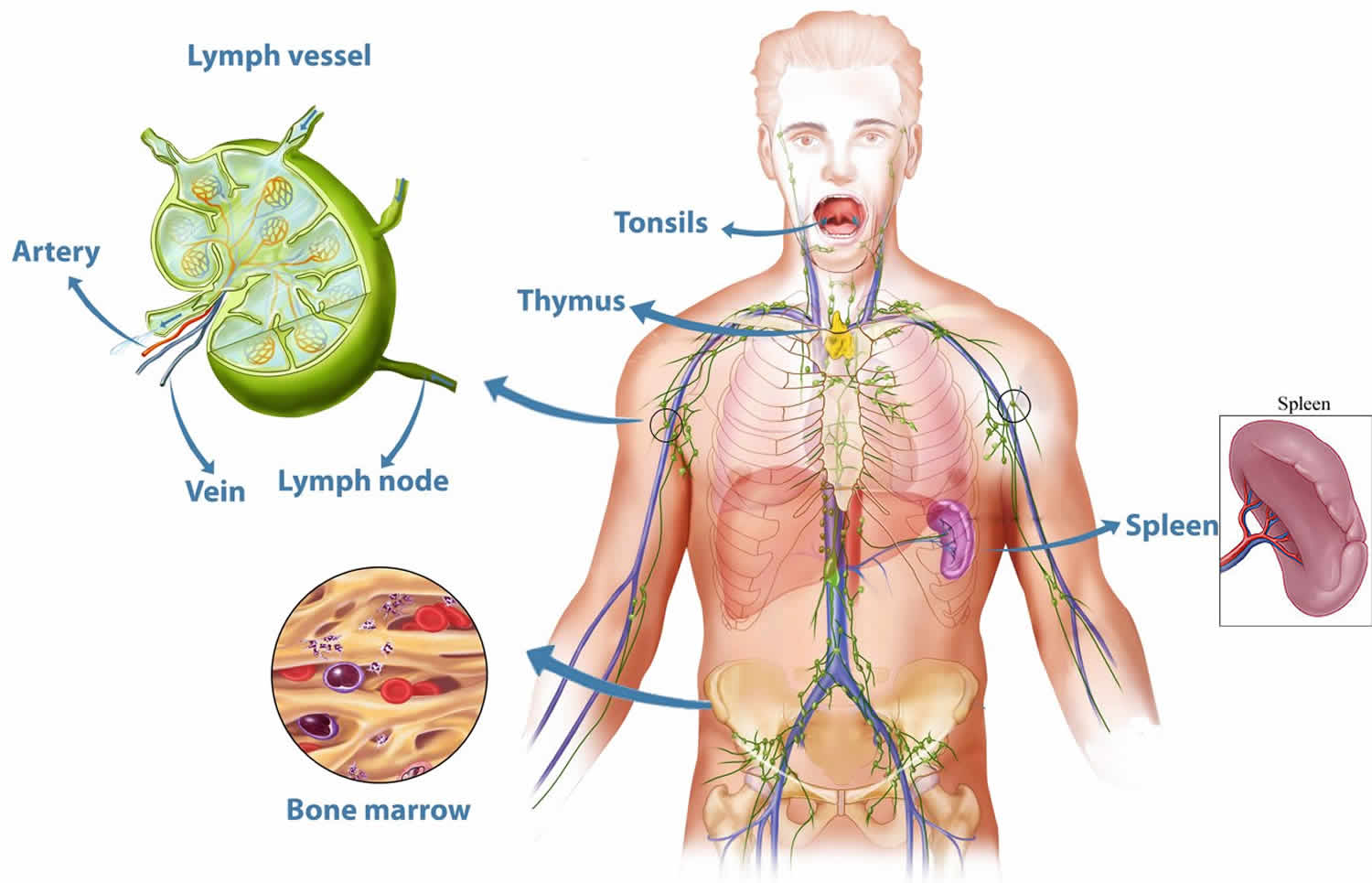
Splenomegaly is a medical term for an enlarged spleen by size or weight 1. Splenomegaly can be caused by many conditions including infections, liver disease, diseases of the blood or lymphatic system and some cancers. Your spleen is an organ that is a part of the lymphatic system. Your spleen filters the blood and maintains healthy red and white blood cells and platelets. It also plays a role in immune function.
The major functions of the spleen include clearance of abnormal red blood cells (erythrocytes), removal of microorganisms and antigens as well as the synthesis of immunoglobulin G (IgG). The spleen also synthesizes the immune system peptides properdin and tuftsin. Also, approximately one-third of circulating platelets are stored in the spleen.
Splenomegaly is a rare condition, with an estimated prevalence of approximately 2% of the total United States population. In adults, there has been no reported predominance in prevalence based on ethnicity, gender, or age.
An enlarged spleen usually doesn’t cause symptoms. Splenomegaly is often discovered during a routine physical exam. Your spleen is an organ located just below your left rib cage. Your doctor generally can’t feel a normal-sized spleen in adults but can feel an enlarged spleen. Your doctor will likely request imaging and blood tests to help identify the cause.
The normal position of the spleen is within the peritoneal cavity in the left upper quadrant adjacent to ribs nine through 12. The normal sized spleen abuts the stomach, colon, and left kidney A normally sized spleen measures up to 11 cm in craniocaudal length. A length of 11 cm to 20 cm indicates splenomegaly, and a length greater than 20 cm is definitive of massive splenomegaly. The normal weight of the adult spleen is 70 g to 200 g, spleen weight of 400 g to 500 g indicates splenomegaly and spleen weight greater than 1000 g is definitive of massive splenomegaly. The normal sized spleen is usually not palpable in adults. However, it may be palpable due to variations in body habitus and chest wall anatomy.
Treatment for splenomegaly focuses on the underlying condition that’s causing it 2. Surgically removing an enlarged spleen isn’t usually the first treatment, but is sometimes recommended.
How your spleen works
Your spleen is tucked under your rib cage next to your stomach on the left side of your abdomen. It’s a soft, spongy organ that performs several critical jobs. Your spleen:
- Filters out and destroys old, damaged blood cells
- Prevents infection by producing white blood cells (lymphocytes) and acting as a first line of defense against disease-causing organisms
- Stores red blood cells and platelets, which help your blood clot
An enlarged spleen affects each of these vital functions. As your spleen grows larger, it filters normal red blood cells as well as abnormal ones, reducing the number of healthy cells in your bloodstream. It also traps too many platelets.
Excess red blood cells and platelets eventually can clog your spleen and affect normal functioning. An enlarged spleen may even outgrow its own blood supply, which can damage or destroy sections of the organ.
Splenomegaly causes
Causes of splenomegaly
- Cirrhosis and other diseases affecting the liver (hepatitis)
- Heart failure
- Portal or hepatic vein thrombosis
- Malignancies and blood cancers (including lymphoma, acute and chronic leukemia, myeloproliferative disorders, metastatic solid tumors, and hemolytic anemias)
- Infectious (including infection with Epstein Barr virus, cytomegalovirus, HIV, salmonella, Brucella, Tuberculosis, malaria, toxoplasma, and leishmania)
- Bacterial infections, such as syphilis or an infection of your heart’s inner lining (endocarditis)
- Infiltrative disease (including Gaucher’s disease, Amyloid, Niemann-Pick disease and Glycogen storage diseases)
- Miscellaneous (including sarcoidosis, systemic lupus erythematous, Felty’s syndrome, metastases, abscess, trauma, hemangiomas, rare drug reactions (RhoGam) and cysts)
The mechanism underlying splenic enlargement varies based on the cause. In the case of acute infectious illness, the spleen performs increased work in clearing antigens and producing antibodies and increases the number of reticuloendothelial cells contained within the spleen. These increased immune functions may result in splenic hyperplasia. In the case of liver disease and congestion, underlying illness causes increased venous pressure causing congestive splenomegaly. Extramedullary hematopoiesis exhibited in myeloproliferative disorders can lead to splenic enlargement (infiltrative splenomegaly) 3.
Splenic sequestration crisis is a life-threatening illness common in pediatric patients with homozygous sickle cell disease and beta thalassemia. Up to 30% of these children may develop splenic sequestration crisis with a mortality rate of up to 15%. This crisis occurs when splenic vaso-occlusion causes a large percentage of total blood volume to become trapped within the spleen. Clinical signs include severe, rapid drop in hemoglobin leading to hypovolemic shock and death. Pediatric patients with sickle cell disease and beta thalassemia experience multiple splenic infarcts, resulting in splenic fibrosis and scarring. Over time, this leads to a small, auto infarcted spleen typically by the time patients reach adulthood. Splenic sequestration crisis can only occur in functioning spleens which may be why this crisis is rarely seen in adults. However, late adolescent or adult patients in this group who maintain splenic function may develop splenic sequestration crisis.
Risk factors for enlarged spleen
Anyone can develop an enlarged spleen at any age, but certain groups are at higher risk, including:
- Children and young adults with infections, such as mononucleosis
- People who have Gaucher’s disease, Niemann-Pick disease, and several other inherited metabolic disorders affecting the liver and spleen
- People who live in or travel to areas where malaria is common
Splenomegaly symptoms
There are usually no symptoms from an enlarged spleen in some cases.
Symptoms of splenomegaly include:
- Hiccups
- Inability to eat a large meal
- Feeling full without eating or after eating only a small amount from the enlarged spleen pressing on your stomach
- Pain or fullness in the left upper abdomen that may spread to the left shoulder
- Anemia
- Fatigue
- Frequent infections
- Easy bleeding
Commonly, patients will present with symptoms due to the underlying illness causing splenomegaly. Constitutional symptoms such as weakness, weight loss, and night sweats suggest malignant illness. Patients with splenomegaly due to acute infection may present with fever, rigors, generalized malaise, or focal infectious symptoms. Patients with underlying liver disease may present with symptoms related to alcohol abuse or hepatitis. Symptoms of anemia (lightheadedness, dyspnea, or exertion), easy bruising, bleeding, or petechiae may indicate splenomegaly due to underlying hemolytic process.
See your doctor promptly if you have pain in your left upper abdomen, especially if it’s severe or the pain gets worse when you take a deep breath.
Splenomegaly complications
Potential complications of an enlarged spleen are:
- Infection. An enlarged spleen can reduce the number of healthy red blood cells, platelets and white cells in your bloodstream, leading to more frequent infections. Anemia and increased bleeding also are possible.
- Ruptured spleen. Even healthy spleens are soft and easily damaged, especially in car crashes. The possibility of rupture is much greater when your spleen is enlarged. A ruptured spleen can cause life-threatening bleeding into your abdominal cavity.
Splenomegaly diagnosis
An enlarged spleen is usually detected during a physical exam. Your doctor can often feel it by gently examining your left upper abdomen. However, in some people — especially those who are slender — a healthy, normal-sized spleen can sometimes be felt during an exam.
Your doctor may confirm the diagnosis of an enlarged spleen with one or more of these tests:
- Blood tests, such as a complete blood count to check the number of red blood cells, white blood cells and platelets in your system
- Ultrasound or computerized tomography (CT) scan to help determine the size of your spleen and whether it’s crowding other organs
- Magnetic resonance imagining (MRI) to trace blood flow through the spleen
Imaging tests aren’t always needed to diagnose an enlarged spleen. But if your doctor recommends imaging, you generally don’t need any special preparation for an ultrasound or MRI.
If you’re having a CT scan, however, you may need to refrain from eating before the test. If you need to prepare, your doctor will let you know well in advance.
Finding the cause
Sometimes you may need more testing to find the cause of an enlarged spleen, including liver function tests and a bone marrow exam. These tests can provide more-detailed information about your blood cells than can blood drawn from a vein.
A sample of solid bone marrow is sometimes removed in a procedure called a bone marrow biopsy. Or you may have a bone marrow aspiration, which removes the liquid portion of your marrow. In many cases, both procedures are performed at the same time (bone marrow exam).
Both the liquid and solid bone marrow samples are usually taken from the pelvis. A needle is inserted into the bone through an incision. You’ll receive either general or local anesthesia before the test to ease discomfort.
A needle biopsy of the spleen is very rare because of the risk of bleeding.
Occasionally, your doctor may recommend surgery to remove your spleen when there’s no identifiable cause for the enlargement. After surgical removal, the spleen is examined under a microscope to check for possible lymphoma of the spleen.
Splenomegaly treatment
Treatment for an enlarged spleen focuses on the underlying problem and protecting the patient from complications of splenomegaly itself. For example, if you have a bacterial infection, treatment will include antibiotics.
Patients with splenomegaly from any cause are at increased risk of splenic rupture, and increased attention must be made to protect the patient from abdominal trauma. Treatment ranges from abdominal injury avoidance in the young healthy patient with splenomegaly due to infectious mononucleosis, to splenectomy of a massively enlarged spleen in a patient with Hairy cell leukemia. Likewise, the prognosis is largely dependent on underlying disease state 4.
Patients who undergo splenectomy are at increased risk of overwhelming infection due to encapsulated organisms such as Haemophilus influenzae, Streptococcus pneumoniae, and Neisseria meningitidis. They should receive vaccinations against these organisms. Careful attention must be paid to post-splenectomy patients presenting with febrile illnesses as they may require more aggressive, empiric antibiotic therapy.
Watchful waiting
If you have an enlarged spleen but don’t have any symptoms and the cause can’t be found, your doctor may suggest watchful waiting. You’ll have to see your doctor for reevaluation in six to 12 months or sooner if you develop any symptoms.
Spleen removal surgery
If an enlarged spleen causes serious complications or the cause can’t be identified or treated, surgical removal of your spleen (splenectomy) may be an option. In chronic or critical cases, surgery may offer the best hope for recovery.
Elective spleen removal requires careful consideration. You can live an active life without a spleen, but you’re more likely to contract serious or even life-threatening infections after spleen removal. Sometimes radiation can shrink your spleen so that you can avoid surgery.
Reducing infection risk after surgery
After spleen removal, certain steps can help reduce your risk of infection, including:
- A series of vaccinations both before and after the splenectomy. These include the pneumococcal (Pneumovax 23), meningococcal and haemophilus influenzae type b (Hib) vaccines, which protect against pneumonia, meningitis and infections of the blood, bones and joints. You’ll also need the pneumococcal vaccine every five years after surgery.
- Taking penicillin or other antibiotics after your operation and anytime you or your doctor suspects the possibility of an infection.
- Calling your doctor at the first sign of a fever, because this may indicate an infection.
- Avoiding travel to parts of the world where certain diseases, such as malaria, are common.
Lifestyle changes
In rare cases, an injury can rupture the spleen. If you have splenomegaly, your health care provider may advise you to avoid contact sports. Your provider will tell you what else you need to do to take care of yourself and any medical condition.
Avoid contact sports — such as soccer, football and hockey — and limit other activities as recommended by your doctor. Modifying your activities can reduce the risk of a ruptured spleen.
It’s also important to wear a seat belt. If you’re in a car accident, a seat belt can help prevent injury to your spleen.
Finally, be sure to keep your vaccinations up to date because your risk of infection is increased. That means at least an annual flu shot, and a tetanus, diphtheria and pertussis booster every 10 years. Ask your doctor if you need any additional vaccines.
- Chapman J, Azevedo AM. Splenomegaly. [Updated 2019 May 6]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430907[↩]
- Nguyen Y, Stirnemann J, Belmatoug N. [Gaucher disease: A review]. Rev Med Interne. 2019 May;40(5):313-322.[↩]
- Palmiere C, Tettamanti C, Scarpelli MP, Tse R. The forensic spleen: Morphological, radiological, and toxicological investigations. Forensic Sci. Int. 2018 Oct;291:94-99.[↩]
- Saab S, Brown RS. Management of Thrombocytopenia in Patients with Chronic Liver Disease. Dig. Dis. Sci. 2019 Apr 22[↩]





{kind=link}