Split brain syndrome
Split-brain syndrome also called callosal disconnection syndrome, condition characterized by a cluster of neurological abnormalities arising from the partial or complete severing or lesioning of the corpus callosum, the bundle of nerves that connects the right and left hemispheres of the brain.
The corpus callosum is the main route for communication between both cerebral hemispheres 1. In ‘split-brain’ patients, the corpus callosum has been surgically cut to alleviate intractable, severe epilepsy 2. Among the first to characterize split-brain syndrome was American neurobiologist Roger Wolcott Sperry 3, who in the 1960s studied human split-brain subjects and contributed to the discovery that the left and right hemispheres of the brain carry out specialized duties. For this work, Sperry received a share of the 1981 Nobel Prize for Physiology or Medicine. What Sperry found was that severing the corpus callosum leads to a curious phenomenon (Figure 1): when an object is presented in the right visual field, the patient responds correctly verbally and with his/her right hand. However, when an object is presented in the left visual field the patient verbally states that he/she saw nothing, and identifies the object accurately with the left hand only 4. This is concordant with the human anatomy; the right hemisphere receives visual input from the left visual field and controls the left hand, and vice versa 5. Moreover, the left hemisphere is generally the site of language processing 6. Thus, severing the corpus callosum seems to cause each hemisphere to gain its own consciousness 7. The left hemisphere is only aware of the right visual half-field and expresses this through its control of the right hand and verbal capacities, while the right hemisphere is only aware of the left visual field, which it expresses through its control of the left hand.
The studies demonstrated that the left and right hemispheres are specialized in different tasks. The left side of the brain is normally specialized in taking care of the analytical and verbal tasks. The left side speaks much better than the right side, while the right half takes care of the space perception tasks and music, for example. The right hemisphere is involved when you are making a map or giving directions on how to get to your home from the bus station. The right hemisphere can only produce rudimentary words and phrases, but contributes emotional context to language. Without the help from the right hemisphere, you would be able to read the word “pig” for instance, but you wouldn’t be able to imagine what it is.
Each hemisphere is still able to learn after the split brain operation but one hemisphere has no idea about what the other hemisphere has experienced or learned. Today, new methods and technology in split brain operation make it possible to cut off only a tiny portion and not the whole of the corpus callosum of patients.
Corpus callosotomy is a surgical procedure that sections the corpus callosum, resulting in either the partial or complete disconnection between the two hemispheres. It is typically used as a last resort measure in treatment of intractable epilepsy. The modern procedure typically involves only the anterior third of the corpus callosum; however, if the epileptic seizures continue, the following third is lesioned prior to the remaining third if the seizures persist. This results in a complete callosotomy in which most of the information transfer between hemispheres is lost.
Due to the functional mapping of the corpus callosum, a partial callosotomy has less detrimental effects because it leaves parts of the corpus callosum intact. There is little functional plasticity observed in partial and complete callosotomies on adults, the most neuroplasticity is seen in young children but not in infants 8.
It is known that when the corpus callosum is severed during an experimental procedure, the experimenter can ask each side of the brain the same question and receive two different answers. When the experimenter asks the right visual field/left hemisphere what they see the participant will respond verbally, whereas if the experimenter asks the left visual field/right hemisphere what they see the participant will not be able to respond verbally but will pick up the appropriate object with their left hand 9.
Although it is not fully understood whether the processing of specific tasks is dependent on both hemispheres of the brain, the two hemispheres appear to each have some control over certain tasks. The left hemisphere, for example, is generally responsible for analytical tasks, such as calculating and reading. In many individuals, it is also the dominant centre for speech and language (though the right hemisphere is involved in language processing to a minor extent). In general, the right hemisphere is more efficient at dealing with spatial tasks, such as navigating a maze or reading a map, than the left hemisphere. The two hemispheres, however, routinely communicate with one another through the corpus callosum. This connection further serves as the conduit through which certain sensory signals are transmitted from one side of the body to the contralateral (opposite) side of the brain and through which motor control is effected in the reverse direction (i.e., the right hemisphere controls the left side of the body, and vice versa).
Figure 1. Split brain syndrome
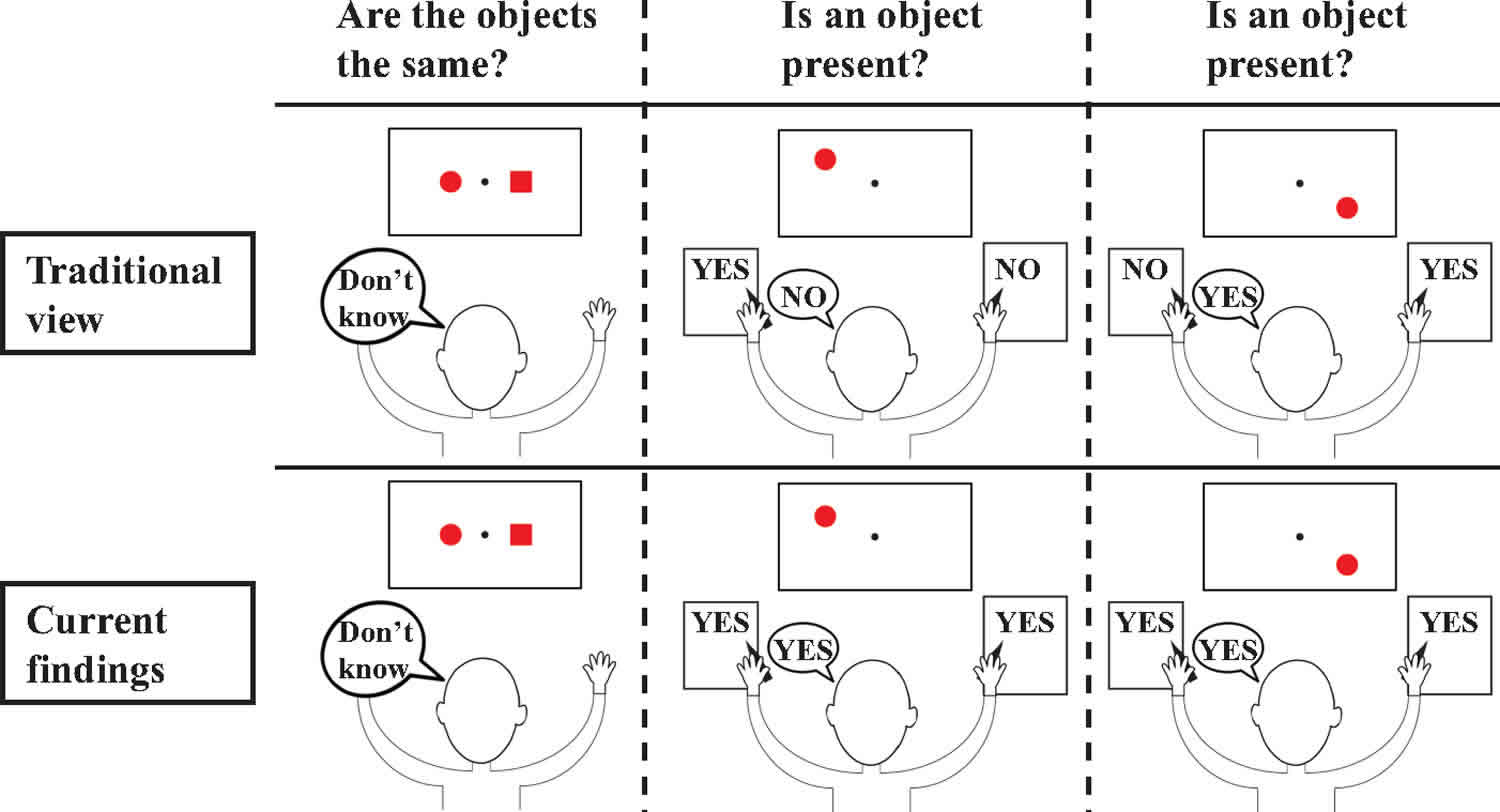
Footnote: A depiction of the traditional view of the split brain syndrome (top) versus what we actually found in two split-brain patients across a wide variety of tasks (bottom). The canonical idea of split-brain patients is that they cannot compare stimuli across visual half-fields (left), because visual processing is not integrated across hemispheres. However, another key element of the traditional view is that split-brain patients can only respond accurately to stimuli in the left visual field with their left hand and to stimuli in the right visual field with their right hand and verbally. This is not what Pinto et al found. Across a wide variety of tasks, they observed that split-brain patients could reliably indicate presence, location, orientation and identity of stimuli throughout the entire visual field regardless of how they responded.
[Source 2 ]Role of the corpus callosum
The corpus callosum is a structure in the brain along the longitudinal fissure that facilitates much of the communication between the two hemispheres and its main function is in allowing for communication between the brain’s right and left hemispheres. This structure is composed of white matter: millions of axons that have their dendrites and terminal buttons projecting in both the right and left hemisphere. However, there is evidence that the corpus callosum may also have some inhibitory functions 10. Post-mortem research on human and monkey brains show that the corpus callosum is functionally organized. It proves that the right hemisphere is superior for detecting faces 11. This organization results in modality-specific regions of the corpus callosum that are responsible for the transfer of different types of information. Research has revealed that the anterior midbody transfers motor information, the posterior midbody transfers somatosensory information, the isthmus transfers auditory information and the splenium transfers visual information 12. Although much of the interhemispheric transfer occurs at the corpus callosum, there are trace amounts of transfer via subcortical pathways.
Studies of the effects on the visual pathway on split-brained patients has revealed that there is a redundancy gain (the ability of target detection to benefit from multiple copies of the target) in simple reaction time. In a simple response to visual stimuli, split-brained patients experience a faster reaction time to bilateral stimuli than predicted by model 13. A model proposed by Iacoboni et al. 14 suggests split-brained patients experience asynchronous activity that causes a stronger signal, and thus a decreased reaction time. Iacoboni also suggests there exists dual attention in split-brained patients, which is implying that each cerebral hemisphere has its own attentional system 15. An alternative approach taken by Reuter-Lorenz et al. 16 suggests that enhanced redundancy gain in the split brain is primarily due to a slowing of responses to unilateral stimuli, rather than a speeding of responses to bilateral ones. It is important to note that the simple reaction time in split-brained patients, even with enhanced redundancy gain, is slower than the reaction time of normal adults.
Pinto et al 2 with two patients, and across a wide variety of tasks, have shown that severing the cortical connections between the two hemispheres does not seem to lead to two independent conscious agents within one brain. Instead, they observed that patients without a corpus callosum were able to respond accurately to stimuli appearing anywhere in the visual field, regardless of whether they responded verbally, with the left or the right hand—despite not being able to compare stimuli between visual half-fields, and despite finding separate levels of performance in each visual half-field for labeling or matching stimuli. This raises the intriguing possibility that even without massive communication between the cerebral hemispheres, and thus increased modularity, unity in consciousness and responding is largely preserved.
This preserved unity of consciousness may be especially challenging for the two currently most dominant theories of consciousness, the Global Workspace theory 17 and the Integration Information theory 18. A core assumption of the Global Workspace theory is that cortical broadcasting of selected information by the ‘global workspace’ leads to consciousness. Thus severing of the corpus callosum, which prevents broadcasting of information across hemispheres, seems to exclude the emergence of one global workspace for both hemispheres. Rather, it seems that without a corpus callosum either two independent global workspaces emerge, or only one hemisphere will have a global workspace, while the other does not. In either case, an integrated global workspace, and thus preserved conscious unity, seems to be difficult to fit into this framework.
Also for Integration Information theory, conscious unity in the split-brain syndrome seems to be challenging. According to the Integration Information theory the richness of integration of information (called φ, defined by how much information is represented, and how integrated the information is) determines the level of consciousness. Moreover, only if the combined φ of two subsystems is larger than the φ per system, then the two subsystems combine to form one conscious entity. After removal of the corpus callosum, which all but eliminates communication between the cerebral hemispheres, integration of information is larger within each hemisphere than between hemispheres. Thus, according to the Integration Information theory, in the split-brain syndrome φ per hemisphere is larger than the combined φ, thus leading to two independent conscious systems rather than one conscious agent 19.
It thus seems that the current results provide a challenge for the Global Workspace and the Integrated Information theory of consciousness. However, the current results may fit well with the local recurrent processing theory of consciousness 20. This theory claims that local recurrent interactions between neural areas (for example between V1 and V5 in the visual system) are enough to create consciousness, even if these interactions are not part of a larger integrated network, and do not project their outcomes to a central processing unit. Thus, according to this theory, even in healthy subjects, relatively isolated processing in one hemisphere can lead to normal visual experiences. Therefore, the local recurrent processing theory suggests that consciousness in split-brain patients may be similar to consciousness in healthy subjects (and thus equally unified).
Split brain experiments
Sperry and his students 3 showed that if the two hemispheres of the brain are separated by severing the corpus callosum (the large band of fibers that connects them), the transfer of information between the hemispheres ceases, and the coexistence in the same individual of two functionally different brains can be demonstrated. The findings contradicted the generally held view – again based on misinterpretation of evidence – that sectioning of the corpus callosum produced no definite behavioral effects. The probable explanation is that the two hemispheres, although separated from one another, are usually in agreement, so that no obvious conflict results. By means of ingenious tests, however, Sperry and his group showed that definite behavioral phenomena can be demonstrated following the brain-splitting operation.
Sperry started this investigation with cats and monkeys, but later extended it to human beings when patients became available whose hemispheres had been surgically separated in order to control intractable epilepsy. It was with these patients that he was able to show that a conscious mind exists in each hemisphere. The left hemisphere is the one with speech, as had been known, and it is dominant in all activities involving language, arithmetic, and analysis. The right hemisphere, although mute and capable only of simple addition (up to about 20) is superior to the left hemisphere in, among other things, spatial comprehension – in understanding maps, for example, or recognizing faces. Until these patients were studied, it had been doubted whether the right hemisphere was even conscious. By devising ways of communicating with the right hemisphere, Sperry could show that this hemisphere is, to quote him: “indeed a conscious system in its own right, perceiving, thinking, remembering, reasoning, willing, and emoting, all at a characteristically human level, and … both the left and the right hemisphere may be conscious simultaneously in different, even in mutually conflicting, mental experiences that run along in parallel” 3
Dr. Sperry used a tachistoscope to present visual information to one hemisphere or the other. The tachistoscope requires people to focus on a point in the center of their visual field. Because each half of the visual field projects to the opposite site of the brain (crossing in the optic chiasm), it is possible to project a picture to either the right hemisphere or the left hemisphere.
Say a “typical” (language in the LEFT hemisphere) split-brain patient is sitting down, looking straight ahead and is focusing on a dot in the middle of a screen. Then a picture of a spoon is flashed to the right of the dot. The visual information about the spoon crosses in the optic chiasm and ends up in the LEFT HEMISPHERE. When the person is asked what the picture was, the person has no problem identifying the spoon and says “Spoon.” However, if the spoon had been flashed to the left of the dot (see the picture), then the visual information would have traveled to the RIGHT HEMISPHERE. Now if the person is asked what the picture was, the person will say that nothing was seen!! But, when this same person is asked to pick out an object using only the LEFT hand, this person will correctly pick out the spoon. This is because touch information from the left hand crosses over to the right hemisphere – the side that “saw” the spoon. However, if the person is again asked what the object is, even when it is in the person’s hand, the person will NOT be able to say what it is because the right hemisphere cannot “talk.” So, the right hemisphere is not stupid, it just has little ability for language – it is “non-verbal.”
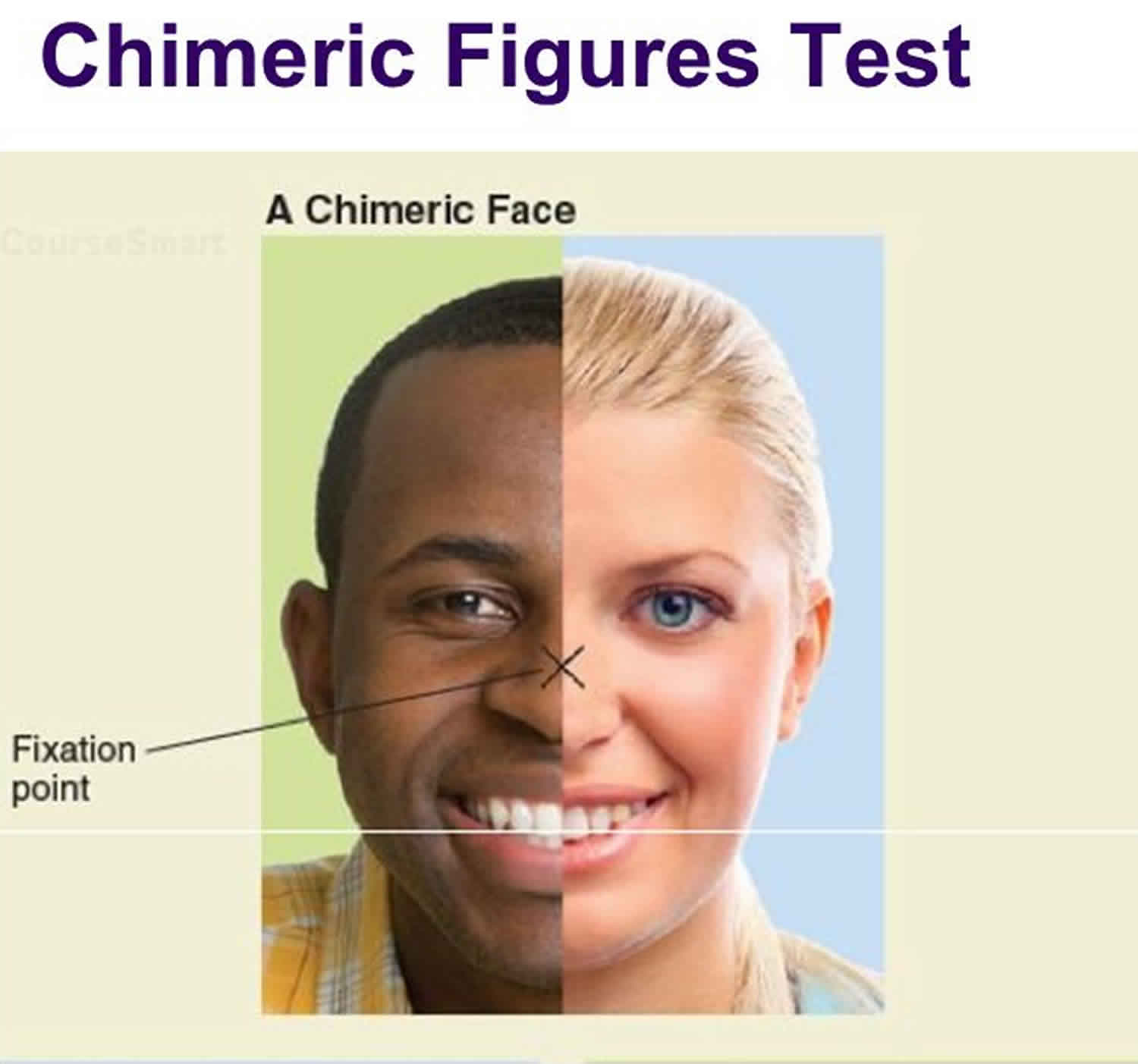
Another type of experiment performed with split brain patients uses chimeric figures (Figure 2). In this figure, the face on the left is a woman and the face on the right is a man. Therefore, if the patient focuses on the dot in the middle of the forehead, the visual information about the woman’s face will go to the right cerebral hemisphere and information about the man’s face will go to the left hemisphere. When a split brain patient is asked to point to a whole, normal picture of the face that was just seen, the patient will usually pick out the woman’s picture (remember, the information about the woman’s face went to the RIGHT cerebral hemisphere). However, if the patient is required to say whether the picture was a man or a woman, the patient will SAY that the picture was of a man. Therefore, depending on what the patient is required to do, either the right or left hemisphere will dominate. In this case, when speech is not required, the right hemisphere will dominate for recognition of faces.
Before different types of brain surgery, it is important to identify which cerebral hemisphere is dominant for language so that the neurosurgeon can avoid damaging speech areas. One way to test which hemisphere is dominant for language is with a procedure called the Wada Test. During this test, a fast acting anesthetic called sodium amytal (amobarbital) is injected into the right or left carotid artery. The right artery supplies the right cerebral hemisphere and the left artery supplies the left cerebral hemisphere. Therefore, either the right or left hemisphere can be “put to sleep” temporarily. If the left hemisphere is put to sleep in people who have language ability in the left hemisphere, then when asked to speak, they cannot. However, if the right hemisphere is put to sleep, then these people will be able to speak and answer questions. (Remember too that because the right hemisphere controls muscles on the left side, people will not be able to move the left side of their bodies.)
Another way to test for language representation in the brain is to electrically stimulate the cerebral cortex. A neurosurgeon can place an electrode on various areas of the exposed brain of an awake patient during surgery. The patient can say what he or she feels and thinks. Placement of the electrode on the brain does NOT hurt because the brain itself does not have any receptors for pain. In people who have left side dominance for language, electrical stimulation of various locations on the left cerebral cortex will interfere with speech.
Figure 2. Chimeric figures
Split-brain syndrome causes
The primary cause of split-brain syndrome is intentional severing of the corpus callosum, partially or completely, through a surgical procedure known as corpus callosotomy. Rarely performed in the 21st century (having been replaced largely by drug treatments and other procedures), this operation is reserved as a last measure of treatment for extreme and uncontrollable forms of epilepsy in which violent seizures spread from one side of the brain to the other. By preventing the propagation of seizure activity across the hemispheres, corpus callosotomy can greatly improve the patient’s quality of life. However, following the operation, patients develop acute hemispheric disconnection symptoms that last for days or weeks and chronic symptoms that often are permanent.
Less-common causes of split-brain syndrome include stroke, infectious lesion, tumour, or ruptured artery. Many of these events result in varying degrees of spontaneous damage to the corpus callosum. The syndrome can also be caused by multiple sclerosis and in rare instances by agenesis of the corpus callosum, in which the connection fails to develop or develops incompletely. (Lesions in the corpus callosum also occur in patients with Marchiafava-Bignami disease, a rare alcoholism-related condition, but the more global brain damage associated with this disease leads to stupor, seizures, and coma, rather than the features typical of split-brain syndrome.)
Split brain symptoms
Many patients with split-brain syndrome retain intact memory and social skills. Split-brain patients also maintain motor skills that were learned before the onset of their condition and require both sides of the body; examples include walking, swimming, and biking. They can also learn new tasks that involve either parallel or mirrored movements of their fingers or hands. They cannot, however, learn to perform new tasks that require interdependent movement of each hand, such as learning to play the piano, where both hands must work together to produce the desired music. Eye movements also remain coordinated.
Since information cannot be directly shared between the two hemispheres, split-brain patients display unusual behaviors, particularly concerning speech and object recognition. For instance, when blindfolded a split-brain patient may not be able to name a familiar object that is held in the left hand, because information for the sense of touch is relayed from the left side of the body to the right hemisphere, which typically has a weak language centre. Without an intact corpus callosum, a person cannot access verbal information in the left hemisphere as long as the object remains in the left hand. For the same reason, the patient may have difficulty using the left hand to execute verbal commands; the inability to respond to commands with motor activity is a form of apraxia. To compensate for deficiencies in touch recognition by the left hand and left-hand apraxia, the patient (still blindfolded) may hold the object in the right hand, which relays information to the left hemisphere, providing access to the patient’s dominant verbal bank and enabling him to speak the name of the object. Upon hearing the name of a given object, the patient may also use the left hand to retrieve it; this presumably is because auditory information is processed by both hemispheres. The diffuse nature by which sounds and smells are processed across the brain appears to underlie other problems experienced by split-brain patients. For example, patients are unable to name odors presented to the right nostril, though the left hand can point out the source. Some symptoms of chronic disconnection can improve with time.
Memory
It is known that the right and the left hemisphere have different functions when it comes to memory. The right hemisphere is better at recognizing objects and faces, recalling knowledge that the individual has already learned, or recalling images already seen. The left hemisphere is better at mental manipulation, language production, and semantic priming but was more susceptible to memory confusion than the right hemisphere 21. The main issue for individuals that have undergone a callosotomy is that because the function of memory is split into two major systems, the individual is more likely to become confused between knowledge they already know and information that they have only inferred 21.
In tests, memory in either hemisphere of split-brained patients is generally lower than normal, though better than in patients with amnesia, suggesting that the forebrain commissures are important for the formation of some kinds of memory. This suggests that posterior callosal sections that include the hippocampal commissures cause a mild memory deficit (in standardised free-field testing) involving recognition 22.
Control
In general, split-brained patients behave in a coordinated, purposeful and consistent manner, despite the independent, parallel, usually different and occasionally conflicting processing of the same information from the environment by the two disconnected hemispheres. When two hemispheres receive competing stimuli at the same time, the response mode tends to determine which hemisphere controls behavior 23.
Often, split-brained patients are indistinguishable from normal adults. This is due to the compensatory phenomena; split-brained patients progressively acquire a variety of strategies to get around their interhemispheric transfer deficits.
Attention
Experiments on covert orienting of spatial attention using the Posner paradigm confirm the existence of two different attentional systems in the two hemispheres 24. The right hemisphere was found superior to the left hemisphere on modified versions of spatial relations tests and in locations testing, whereas the left hemisphere was more object based 25. The components of mental imagery are differentially specialized: the right hemisphere was found superior for mental rotation 26, the left hemisphere superior for image generation 27. It was also found that the right hemisphere paid more attention to landmarks and scenes whereas the left hemisphere paid more attention to exemplars of categories.
- Wahl M, Lauterbach-Soon B, Hattingen E, Jung P, Singer O, Volz S et al. Human motor corpus callosum: topography, somatotopy, and link between microstructure and function. J Neurosci 2007; 27: 12132–8.[↩]
- Yair Pinto, David A. Neville, Marte Otten, Paul M. Corballis, Victor A. F. Lamme, Edward H. F de Haan, Nicoletta Foschi, Mara Fabri, Split brain: divided perception but undivided consciousness, Brain, Volume 140, Issue 5, May 2017, Pages 1231–1237, https://doi.org/10.1093/brain/aww358[↩][↩][↩]
- Sperry RW. Hemisphere deconnection and unity in conscious awareness. Am Psychol 1968; 23: 723.[↩][↩][↩]
- Wolman D. A tale of two halves. Nature, 2012; 483: 260–3.[↩]
- Sakata H, Taira M. Parietal control of hand action. Curr Opin Neurobiol 1994; 4: 847–56.[↩]
- Vigneau M, Beaucousin V, Herve P, Duffau H, Crivello F, Houde O et al. Meta-analyzing left hemisphere language areas: phonology, semantics, and sentence processing. Neuroimage 2006; 30: 1414–32.[↩]
- Sperry R. Consciousness, personal identity and the divided brain. Neuropsychologia 1984; 22: 661–73.[↩]
- Concha, Luis; Donald Gross; Matt Wheatley; Christian Beaulieu (2006). “Diffusion Tensor Imaging of Time-Dependent Axonal and Myelin Degradation after Corpus Callosotomy in Epilepsy Patients”. NeuroImage. 32 (3): 1090–1099. doi:10.1016/j.neuroimage.2006.04.187[↩]
- Raven, Peter (2014). Biology. New York: McGraw-Hill. ISBN 9780073383071[↩]
- O’Shea R. P. (2003). “Binocular rivalry in split-brain observers”. Journal of Vision. 3 (10): 610–615. doi:10.1167/3.10.3[↩]
- Mooshagian, Eric (2008). “Anatomy of the Corpus Callosum reveals its Function”. Journal of Neuroscience. 28 (7): 1535–1536. doi:10.1523/JNEUROSCI.5426-07.2008[↩]
- Risse GL, Gates J, Lund G, Maxwell R, Rubens A (1989). “Inter-hemispheric transfer in patients with incomplete section of the corpus callosum: anatomic verification with magnetic resonance imaging”. Arch Neurol. 46 (4): 437–43. doi:10.1001/archneur.1989.00520400097026[↩]
- Corballis M. C.; Corballis P. M.; Fabri M. (2003). “Redundancy gain in simple reaction time following partial and complete callosotomy”. Neuropsychologia. 42: 71–81. CiteSeerX 10.1.1.503.8952. doi:10.1016/s0028-3932(03)00152-0[↩]
- Iacoboni M.; Fried I.; Zaidel E. (1994). “Callosal transmission time before and after partial commissurotomy”. NeuroReport. 5 (18): 2521–2524. doi:10.1097/00001756-199412000-00029[↩]
- Arguin M.; Lassonde M.; Quattrini A.; Del Pesce M.; Foschi N.; Papo I. (2000). “Divided visuo-spatial attention systems with total and anterior callosotomy”. Neuropsychologia. 38 (3): 283–291. doi:10.1016/s0028-3932(99)00077-9[↩]
- Reuter-Lorenz P. A.; Nozawa G.; Gazzaniga M. S.; Hughes H. C. (1995). “Fate of neglected targets: a chronometric analysis of redundant target effects in the bisected brain”. Journal of Experimental Psychology: Human Perception and Performance. 21 (2): 211–230. doi:10.1037/0096-1523.21.2.211[↩]
- Baars BJ. Global workspace theory of consciousness: toward a cognitive neuroscience of human experience. Prog Brain Res 2005; 150: 45–53.[↩]
- Tononi G, Koch C. Consciousness: here, there and everywhere? Philos Trans R Soc Lond B Biol Sci 2015; 370. pii: 2014.0167[↩]
- Tononi G. Consciousness, information integration, and the brain. Prog Brain Res 2005; 150, 109–26.[↩]
- Block N. Consciousness, accessibility, and the mesh between psychology and neuroscience. Behav Brain Sci 2007; 30: 481–99.[↩]
- Metcalfe, Janet; Margaret Funnell; Michael Gazzanuga (1995). “Right-Hemisphere Memory Superiority:Studies of Split-brain Patient”. Psychological Science. 6 (3): 157–164. doi:10.1111/j.1467-9280.1995.tb00325.x[↩][↩]
- Tramo MJ, Baynes K, Fendrich R, Mangun GR, Phelps EA, Reuter- Lorenz PA, Gazzaniga MS (1995): Hemispheric specialization and interhemispheric integration: Insights from experiments with commissurotomy patients. In: Epilepsy and the Corpus Callosum 2. Reeves AG, Roberts DW, eds. New York: Plenum, pp. 263-295[↩]
- Levy J, Trevarthen C (IC)76: Metacontrol of hemispheric function in human split-brain patients. J Exp Psvchol (HP&P) 2:299-312 Reeves AG, Roberts DW, eds. (1995): Epilepsy and the Corpus Callosum 2. New York: Plenum[↩]
- Zaidel E (1994): Interhemispheric transfer in the split brain: Long term status following complete cerebral commissurotomy. In: Human Laterality, Davidson RH, Hugdahl K, eds. Cambridge, MA: MIT Press, pp. 491-532[↩]
- Nebes RD, ed. (1990): The commissurotomized brain. In: Handbook of Neuropsychology, vol. 4, section 7, Boiler F, Grafman J, eds. Amsterdam: Elsevier, pp. 3-168[↩]
- Sergent Justine; Corballis Michael C (1989). “Categorization of disoriented faces in the cerebral hemispheres of normal and commissurotomized subjects”. Journal of Experimental Psychology: Human Perception and Performance. 15 (4): 701–710. doi:10.1037/0096-1523.15.4.701[↩]
- Farah Martha J (1986). “The laterality of mental image generation: A test with normal subjects”. Neuropsychologia. 24 (4): 541–551. doi:10.1016/0028-3932(86)90098-9[↩]





{kind=link}