
Swimmer’s shoulder
Swimmer’s shoulder is the term used to describe the problem of shoulder pain in the competitive swimmer 1. Swimmer’s shoulder incidence is reported as approximately 35% in elite and senior level swimmers 2. Swimmer’s shoulder can represent numerous shoulder pathologies and these include impingement syndrome, rotator cuff tendinitis, labral injuries, instability secondary to ligamentous laxity or muscle imbalance/dysfunction, neuropathy from nerve entrapment, and anatomic variants 3. Swimmers have a significant potential for shoulder injuries due to the unique nature of the different strokes involved in swimming as well as the high volume of repetitions needed during training 3. Swimming is an unusual sport in that the shoulders and upper extremities are used for locomotion, while at the same time requiring above average shoulder flexibility and range of motion (ROM) for maximal efficiency. This is often associated with an undesirable increase in joint laxity. Furthermore, it is performed in a fluid medium, which offers more resistance to movement than air. This combination of unnatural demands can lead to a spectrum of overuse injuries seen in the swimmer’s shoulder, the most common of which is rotator cuff tendinitis.
Shoulder anatomy
The shoulder girdle is made up of 3 bones (the scapula, clavicle, and proximal humerus), 2 joints (the glenohumeral and acromioclavicular joints), and numerous ligaments, muscles, and tendons. The subacromial bursa overlies the rotator cuff and can provide it with some mechanical protection from the bony acromion above in the face of impingement.
The key ligaments are the glenohumeral ligaments (inferior, middle, superior), which are thickened regions of the joint capsule, of which the inferior glenohumeral ligament is most important. Their role is to help stabilize the glenohumeral joint, in support of the rotator cuff muscles.
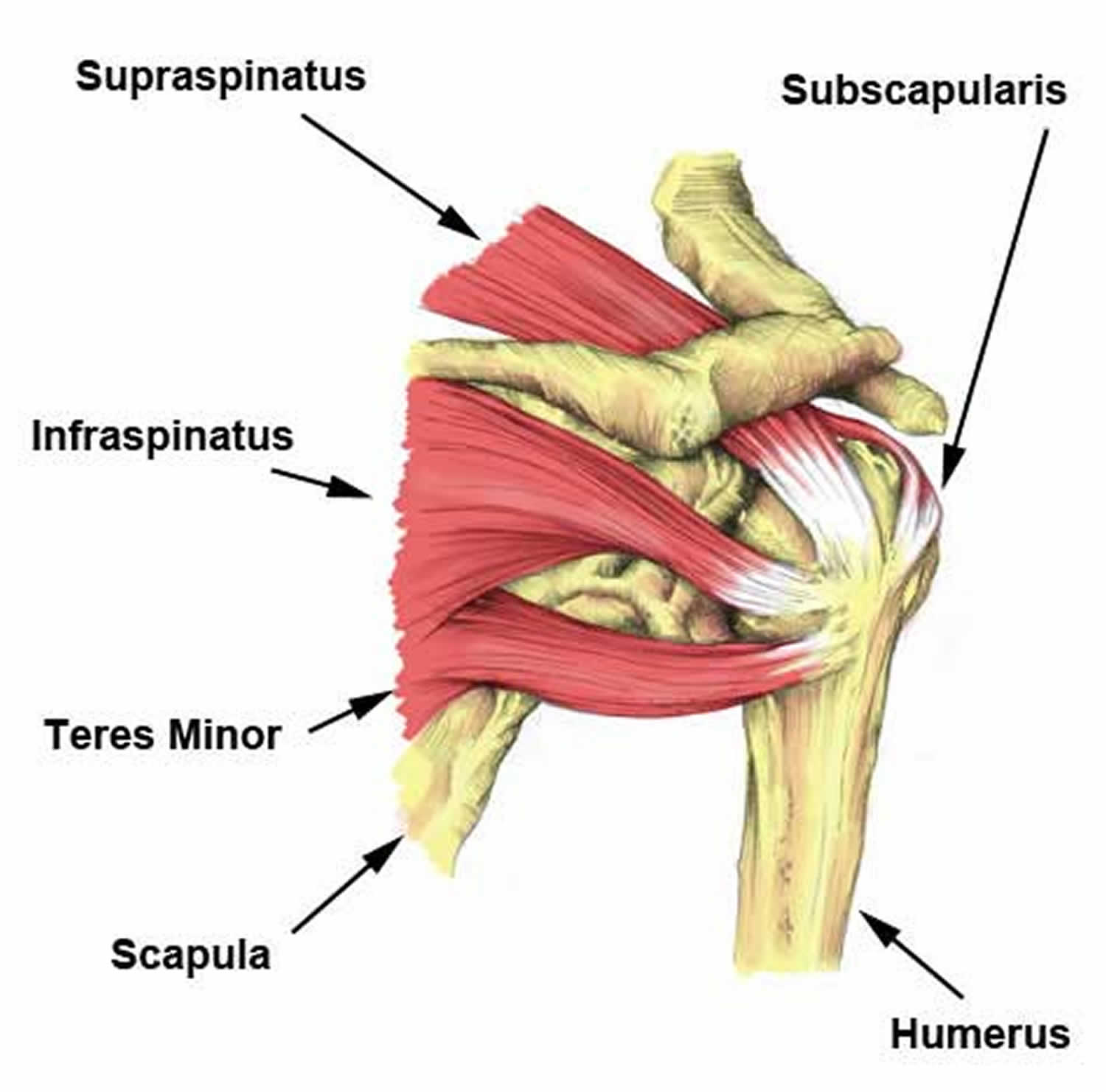
The key muscle group of the shoulder is the rotator cuff, made up of (from anterior to posterior) the subscapularis, supraspinatus, infraspinatus, and teres minor. The primary role of the rotator cuff is to function as the dynamic and functional stabilizer of the glenohumeral joint. The long head of the biceps tendon, located between the subscapularis and supraspinatus, also assists the rotator cuff in stabilizing the glenohumeral joint. These muscles and their tendons can be overused and injured in shoulder dominant activities such as swimming, with the most commonly injured portion of the cuff being the supraspinatus. On the other hand, the “power muscles” of the shoulders, including the latissimus dorsi, pectoralis, and deltoid, are responsible for moving the arm through space or water, but only infrequently sustain significant injury.
Finally, the trapezius, levator scapulae, rhomboids, and serratus anterior muscles stabilize and position the scapula and shoulder girdle, and are therefore very important to the swimming stroke. Without a stable platform from which to work, the shoulder and arm cannot function efficiently. Fortunately, they also are only occasionally the source of significant injury in the swimmer.
Figure 1. Shoulder anatomy
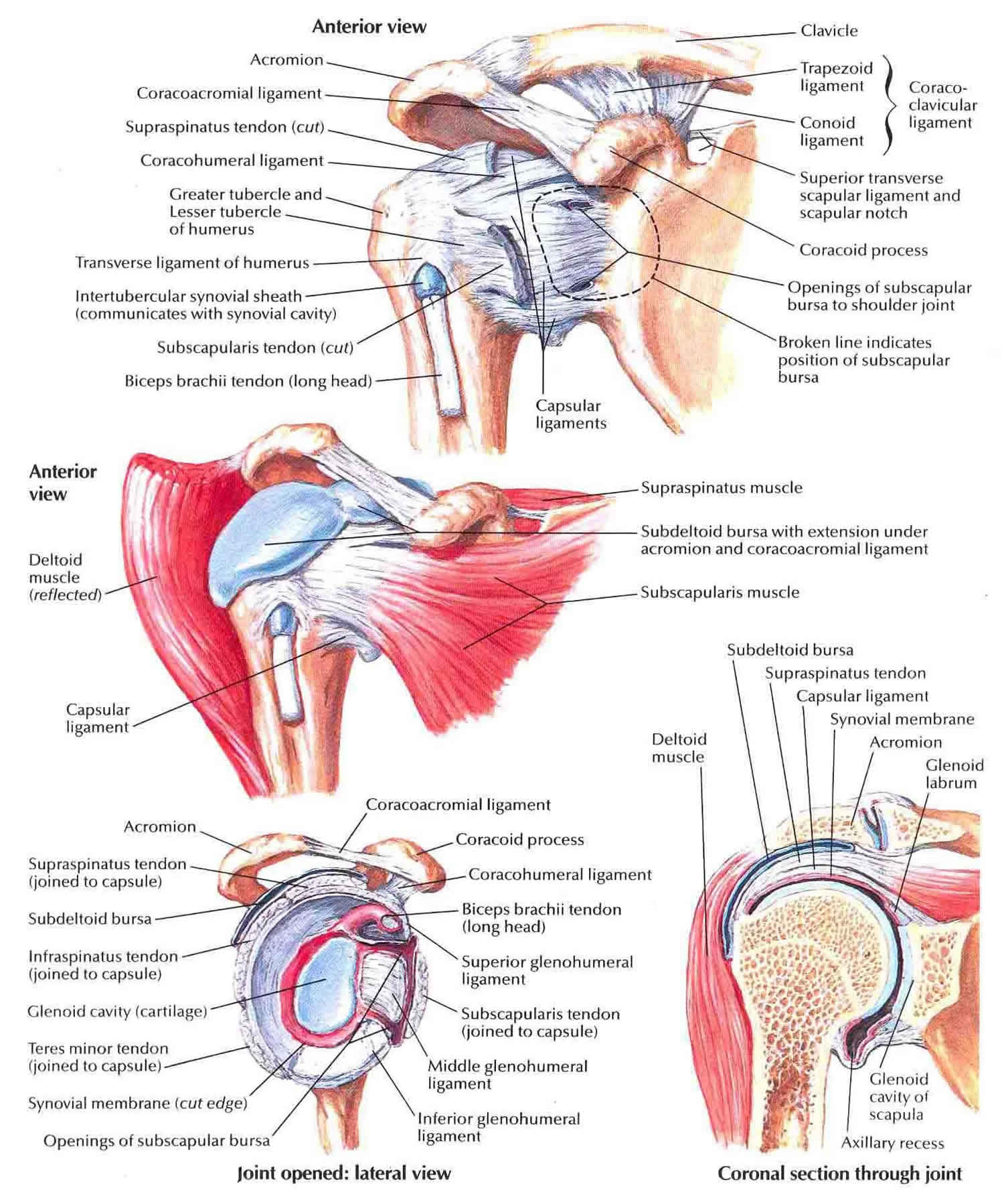
Figure 2. Rotator cuff muscles and tendons

Swimmer’s shoulder causes
Swimming is a unique activity because it requires primarily the upper body for the propulsive force, with 90% of the driving force provided primarily by the torque generated from the shoulder. To swim at an elite level, each swimmer must log between 60,000 and 80,000 meters per week, which is equivalent to 30,000 strokes per arm. Fundamentally, the swim stroke requires the shoulder to move to range-of-motion (ROM) extremes while tremendous muscular force is exerted upon the shoulder 4.
As the shoulder is pushed to its limits in terms of strength and endurance, the rotator cuff muscles generally fatigue before the power muscles, allowing micromotion and subluxation of the humeral head. This, in turn, decreases stroke efficiency, while leading to injuries of the rotator cuff, biceps tendon, and glenoid labrum.
Superior subluxation of the humeral head is particularly problematic as it can impinge the rotator cuff tendons against the acromion above, leading to tendinitis and/or tears. The overlying subacromial bursa (also referred to as the subdeltoid bursa) often becomes inflamed, leading to painful bursitis.
Swimmer’s shoulder prevention
If you are at risk of rotator cuff injuries or if you’ve had a rotator cuff injury in the past, daily shoulder stretches and strengthening exercises can help prevent future injury.
Most people exercise the front muscles of the chest, shoulder and upper arm, but it is equally important to strengthen the muscles in the back of the shoulder and around the shoulder blade to optimize shoulder muscle balance. Your doctor or a physical therapist can help you plan an exercise routine.
A structured rotator cuff strengthening program during the off-season and a gradual increase in training at the beginning of the season can help prevent the occurrence of swimmer’s shoulder. Avoiding rotator cuff fatigue through proper mechanics and conditioning is the key to preventing injury. Knowing the signs and symptoms of rotator cuff fatigue and tendinitis can help the physician, trainer, and coach determine when a swimmer should rest his or her shoulder.
Shoulder exercises for swimmers
Swimmer’s shoulder symptoms
Shoulder impingement pain
Shoulder impingement pain commonly causes local swelling and tenderness in the front of the shoulder. You may have pain and stiffness when you lift your arm. There may also be pain when the arm is lowered from an elevated position.
Beginning symptoms may be mild. Patients frequently do not seek treatment at an early stage. These symptoms may include:
- Minor pain that is present both with activity and at rest
- Pain radiating from the front of the shoulder to the side of the arm
- Sudden pain with lifting and reaching movements
- Athletes in overhead sports may have pain when throwing or serving a tennis ball
As the problem progresses, the symptoms increase:
- Pain while sleeping at night
- Loss of strength and motion
- Difficulty doing activities that place the arm behind the back, such as buttoning or zippering
If the pain comes on suddenly, the shoulder may be severely tender. All movement may be limited and painful.
Rotator cuff injury symptoms
The pain associated with a rotator cuff injury may:
- Be described as a dull ache deep in the shoulder
- Disturb sleep, particularly if you lie on the affected shoulder
- Make it difficult to comb your hair or reach behind your back
- Be accompanied by arm weakness
Symptoms of a rotator cuff injury include pain and tenderness in the shoulder, pain on elevating the arm, weakness of the shoulder, and pain when sleeping on the affected side. Pain from the tear may cause awakening at night. Testing of the range of movement and strength of the shoulder, along with special directed tests, can help the doctor determine which of the muscles or tendons has been torn. Sometimes rotator cuff tears can be without symptoms.
A torn cuff may make the shoulder weak, and make daily activities more difficult. It is a common injury, particularly in people over 40 years old. A tear in the rotator cuff will disrupt the normal functioning of the cuff itself and, depending on the severity of the tear, can result in a range of symptoms. Tears may be partial or full thickness, and occur as the result of an injury, or occur as part of the degenerative process.
A partial tear involves the tendon, but does not completely sever it. In some cases, fraying of the tendon can result in a partial tear, and progress to a complete, full thickness tear.
A complete or full thickness tear often occurs at or near the attachment of the tendon to the arm bone, or humerus and may cause significant disability, particularly in younger people.
Swimmer’s shoulder diagnosis
A thorough physical examination is imperative for diagnosing a swimmer’s shoulder pain. The shoulders should be checked for atrophy and symmetry, the range of motion should be measured. Special attention should be paid to scapular positioning at rest and symmetry in motion to assess for abnormal motion. Strength testing likely will produce pain, and in advanced cases, the shoulder may fail to resist the examiner’s force.
Special testing may provide further insight. The apprehension/relocation test and sulcus signs provide insight into instability. The Hawkins test is a useful and sensitive exam in the diagnosis of subacromial impingement. In patients with positive laxity test results, the examiner also should check other joints for laxity to rule out a generalized condition 5.
Plain radiographs are obtained initially to rule out any abnormal anatomic variations. Following evaluation by a sports medicine physician, an MRI may be ordered to better identify pathology in the muscles, tendons, ligaments, and cartilage or to exclude other structural causes, such as labral cysts. Although many shoulder diagnoses can be reached based on the physical examination alone, MRI is useful in confirming a diagnosis or when shoulder pain appears to have more than one source. An MRI arthrogram can be considered when a labral or tendon tear is suspected, Although imaging is an important part of the diagnosis, caution is warranted in interpreting imaging because repetitive motion creates asymptomatic pathology in many athletes.
Procedures
Subacromial injection
This can be a useful test in the older swimmer who has failed to respond to rest and rehabilitation, suggesting a partial or complete rotator cuff tear. Termed an impingement test when performed with lidocaine alone, a subacromial injection can be both diagnostic as well as therapeutic when a corticosteroid (eg, methylprednisolone) is added.
Immediate relief of pain following the injection (as evidenced by a negative Neer test result) would suggest an injury of the rotator cuff and/or the overlying bursa.
The addition of a corticosteroid to the injection can give the athlete a prolonged period of pain relief, lasting weeks or months, during which time a rotator cuff strengthening program can be instituted.
Intra-articular injection
This can be a diagnostic as well as therapeutic procedure. Injection is within the glenohumeral joint with lidocaine alone or with a corticosteroid (eg, methylprednisolone, triamcinolone).
The addition of a corticosteroid to the injection can give the athlete a prolonged period of pain relief if the derangement is intra-articular in nature.
Swimmer’s shoulder treatment
Nonsurgical management
Eliminating acute inflammation is the priority in shoulder rehabilitation. After a swimmer, first experiences pain, ice, non-steroidal anti-inflammatory drugs (NSAIDs), and rest can prevent progression. If pain continues or worsens, a 7-day to 10-day course of non-steroidal anti-inflammatory drugs (NSAIDs) and rest is ideal but often proves difficult if the injury occurs during the middle or late part of the season. At a minimum, effort should be made to reduce yardage to below the point of pain. For swimmers with impingement, tendinitis, or scapular dyskinesis, a subacromial and/or glenohumeral corticosteroid injection may be beneficial diagnostically and for pain reduction 6.
Stretches that focus on the posterior capsule are important for preventing and reversing shoulder impingement. When they are coupled with overstretching of the anterior capsule, swimmers can create imbalances that worsen impingement. The swimmer can stretch the posterior capsule by horizontally adducting the arm and using the contralateral arm to pin it against the body.
Disproportionately increased adduction strength and internal rotation are unavoidable consequences of swimming. Overdevelopment of the pectoralis major and latissimus dorsi muscle groups creates a force that displaces the humeral head anteriorly, leading to joint instability. Additionally, rotator cuff strengthening will lead to muscular balance restoration, which will reduce or eliminate impingement. As muscle endurance and strength improve, sport-mimicking exercises can be attempted, followed by low-yardage workouts at slow speeds, as long as the swimmer is pain-free, and progressing slowly until the swimmer can return to competition 7.
Swimmer’s shoulder physical therapy
Pain relief, which is the first goal of treatment, involves resting the shoulder. In most cases, the athlete should stop or significantly decrease his or her swimming activities. A physical therapist can help modify shoulder and activities to help avoid re-aggravation of the rotator cuff. Anti-inflammatory treatment in the form of regular icing and nonsteroidal anti-inflammatory medications should also be instituted until the athlete is pain free.
The second goal of treatment is to restore normal strength in the rotator cuff. Regaining strength can be accomplished with a supervised exercise program for the rotator cuff using relatively light weights (2-3 lb, up to a maximum of 5 lb) and high repetitions (12-20 reps per set). These exercises can be performed on a daily basis or every other day.
Working with a physical therapist can be helpful, particularly one with expertise in treating shoulder injuries and swimmers, who can help the athlete transition from dry land exercises to swimming. The addition of therapist-administered therapeutic modalities, such as ultrasound, phonophoresis, iontophoresis, or electrical stimulation can help further reduce pain and inflammation during the acute phase of injury.
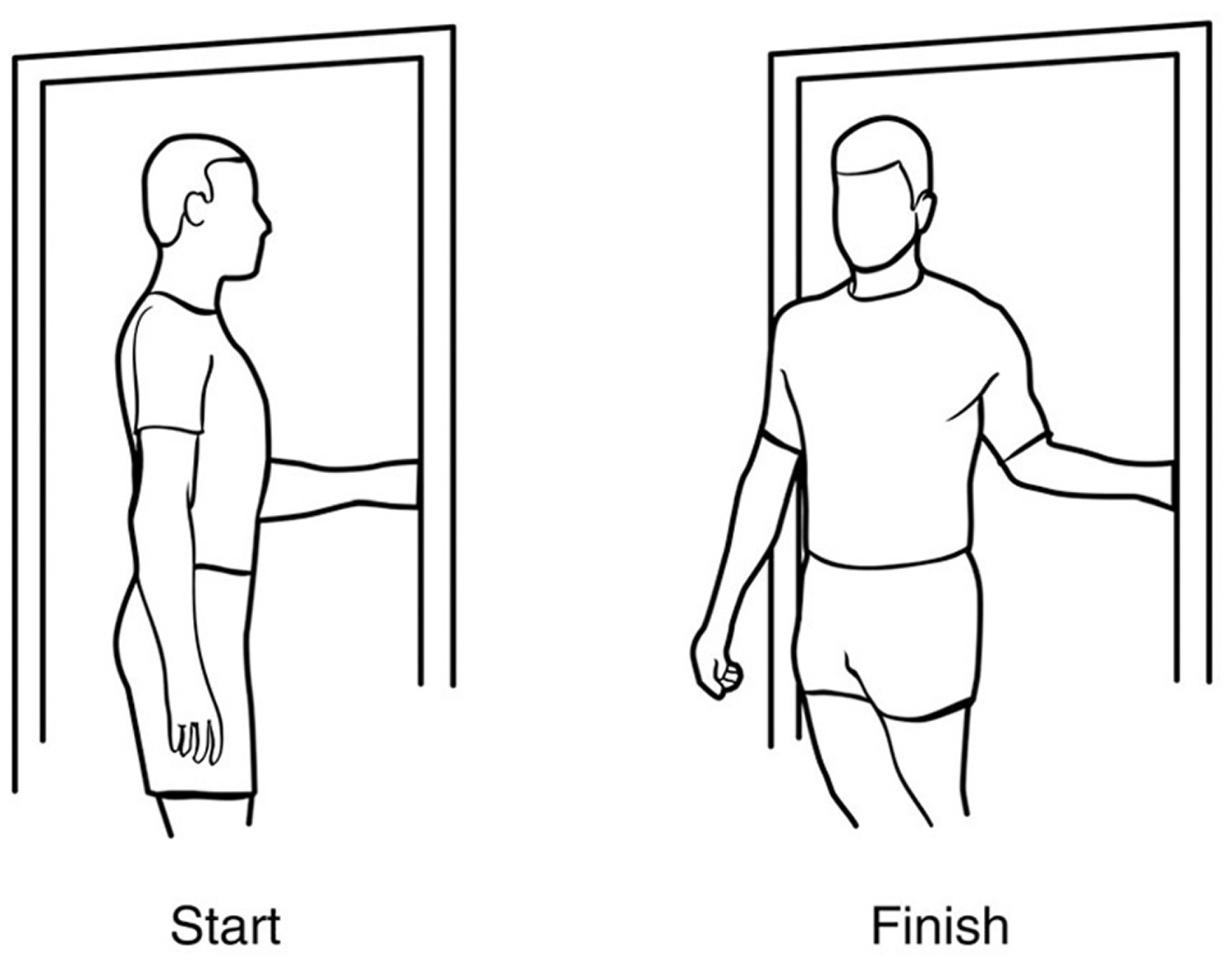
External rotation — passive stretch
Stand in a doorway and bend your affected arm 90 degrees to reach the doorjamb. Keep your hand in place and rotate your body as shown in the illustration (Figure 2). Hold for 30 seconds. Relax and repeat.
Figure 2. Swimmer’s shoulder exercise – external rotation passive stretch
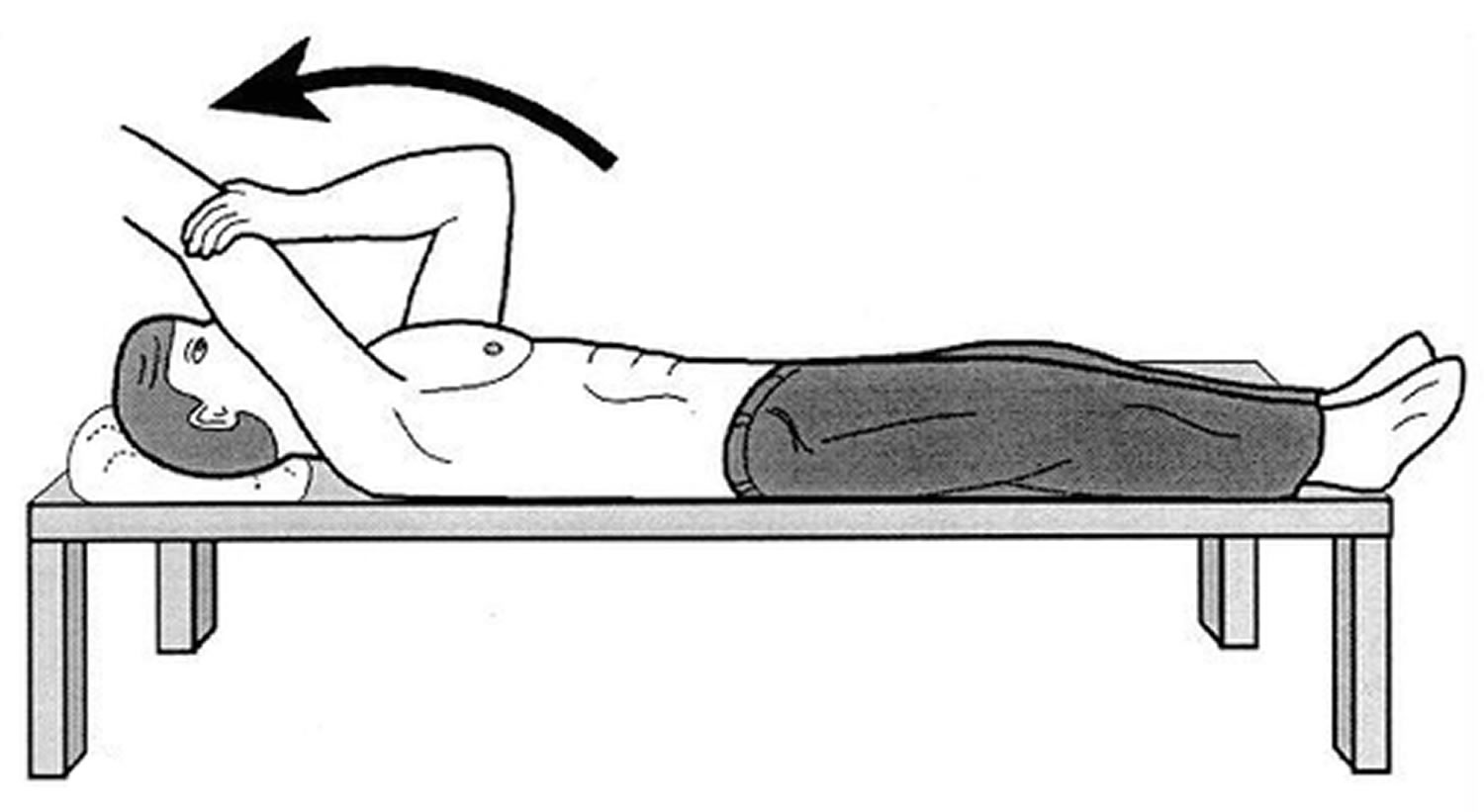
Forward flexion — supine position
Lie on your back with your legs straight. Use your unaffected arm to lift your affected arm overhead until you feel a gentle stretch. Hold for 15 seconds and slowly lower to start position. Relax and repeat.
Figure 3. Swimmer’s shoulder exercise – forward flexion in supine position
 Crossover arm stretch
Crossover arm stretchGently pull one arm across your chest just below your chin as far as possible without causing pain. Hold for 30 seconds. Relax and repeat.
Figure 4. Swimmer’s shoulder exercise – crossover arm stretch

Surgical management
Surgical intervention is considered in athletes who continue to have shoulder pain after a minimum of 6 months of guided rest and rehabilitation.. An athlete may elect symptomatic management rather than surgery so that he or she may continue competing until the pain begins to interfere with daily life. For swimmers with persistent multidirectional instability, a capsular plication or inferior capsular shift procedure should be considered. However, athletes should be aware that training volumes may need to be reduced permanently to avoid pain.
The surgical procedure should include an examination under anesthesia to determine the degree of laxity, a diagnostic arthroscopy (to look for labral or rotator cuff tears and capsular laxity), and, when indicated, a surgical tightening of the lax capsule (capsulorrhaphy). In the older athlete, a subacromial decompression is typically performed if there is arthroscopic evidence of impingement.
For swimmers with a labral tear in whom nonsurgical treatment has failed, the next treatment option is labral debridement or repair.
The athlete should be cautioned about the postsurgical trade-off of increased shoulder stability for some loss of flexibility, resulting in difficulty in returning to swimming at the same level as before the injury.
Baker et al 8 determined arthroscopic management of symptomatic multidirectional instability in 40 athletes (mean age: 19.1 years; 24 males; 16 females) could successfully return them to sports with a high rate of success. At a mean of 33.5 months follow-up, the mean American Shoulder and Elbow Surgeons score was 91.4 of 100 (range, 59.9-100), and the mean Western Ontario Shoulder Instability postoperative percentage score was 91.1 of 100 (range, 72.9-100) 8. Full or satisfactory range of motion was reported in 91% of the patients, normal or slightly decreased strength was noted in 98%, and 86% of the athletes had little or no limitation on returning to their sport.
In 2 studies by the same investigators, conservative treatment was compared with capsular shift in patients with multidirectional instability of the shoulder.
Using electromyography, Illyes et al 9 compared the muscle activity in patients who received conservative therapy (n = 34) and those who underwent capsular shift with postoperative rehabilitation (n = 31) with the muscle activity of individuals stable shoulder joints (n = 50) before and after treatment during pull, push, and elevation of upper extremities and during overhead throw. The investigators found that the post-therapy characteristics of the muscle patterns of both treatment groups were similar to the healthy control group. However, whereas the conservative therapy restored muscular control, the open capsular shift treatment combined with postoperative conservative rehabilitation resolved the patients’ labrous ligamentous abnormalities and restored muscular control 9.
Kiss et al 10 compared the kinematic parameters and the on-off muscle patterns of patients with multidirectional instability treated by physiotherapy (n = 32) or by capsular shift and postoperative physiotherapy (n = 19) before and after treatment during elevation in the scapular plane. Both treatment groups’ results were compared with those of 25 healthy individuals. Patients with multidirectional instability had different scapulothoracic and glenohumeral rhythms as well as increased relative displacement between the scapular and humeral rotation centers relative to the healthy subjects.
Although physiotherapy strengthened the rotator cuff, biceps brachii, triceps brachii, and deltoid muscles, as well as increased the neuromuscular control of the shoulder joints in patients with multidirectional instability, it did not restore the alteration in shoulder kinematics in these patients 10. However, capsular shift and postoperative physiotherapy angulation at 60º of scapulothoracic and glenohumeral rhythms restored the relative displacement between the scapular and humeral rotation centers as well as the duration of muscular activity.
Rehabilitation program
A capsulorrhaphy usually requires immobilization in an arm sling or immobilizer for 4-6 weeks to allow the capsule to heal in the surgically-tightened position. This is then followed by a rotator cuff strengthening program in physical therapy. Passive range of motion is typically restricted during this time so as not to stretch out the capsule. Range of motion commonly returns on its own with exercise and normal shoulder use. One can expect about 50-75% of the normal shoulder motion to return by 3 months and 100% of motion by 6 months following successful surgery. Modified stroke work can begin once the athlete achieved a minimum of 80% of normal motion and strength in the shoulder. Return to competitive swimming is anticipated between 6 and 12 months following surgery.
The maintenance phase is the final phase of rehabilitation. The athlete should be independent with a strengthening program as instructed by his or her athletic trainer or physical therapist. The therapist and coach should both be involved in re-assessment of swimming mechanics and stroke technique, addressing any errors to prevent recurrence of injury.
Return to swim
The athlete is allowed to return to swimming on a gradual basis once he is completely pain free, has a full range of motion, and has normal strength of the rotator cuff, as compared to the opposite shoulder. Return to swimming should preferably occur under the guidance of a physical therapist or athletic trainer, and swim coach.
Swimmer’s shoulder prognosis
Swimmer’s shoulder should expect a full recovery with appropriate rest and rotator cuff rehabilitation is good. Surgery is seldom required except in the most recalcitrant cases.
- Swimmer’s shoulder. https://emedicine.medscape.com/article/93213-overview[↩]
- Matzkin E, Suslavich K, Wes D. Swimmer’s Shoulder: Painful Shoulder in the Competitive Swimmer. J Am Acad Orthop Surg. 2016 Aug;24(8):527-36.[↩]
- Gossman W, Nickerson M, Varacallo M. Swimmer’s Shoulder. [Updated 2019 Jun 4]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470589[↩][↩]
- Demarie S, Chirico E, Gianfelici A, Vannozzi G. Anaerobic capacity assessment in elite swimmers through inertial sensors. Physiol Meas. 2019 May 09[↩]
- De Martino I, Rodeo SA. The Swimmer’s Shoulder: Multi-directional Instability. Curr Rev Musculoskelet Med. 2018 Jun;11(2):167-171.[↩]
- Kancherla VK, Heckman DS, Carolan GF. Luxatio erecta humeri in the swimmer’s shoulder: A combination of ligamentous laxity and motion dyskinesis. J Emerg Trauma Shock. 2016 Jan-Mar;9(1):39-40.[↩]
- de Almeida MO, Hespanhol LC, Lopes AD. PREVALENCE OF MUSCULOSKELETAL PAIN AMONG SWIMMERS IN AN ELITE NATIONAL TOURNAMENT. Int J Sports Phys Ther. 2015 Dec;10(7):1026-34.[↩]
- Baker CL 3rd, Mascarenhas R, Kline AJ, et al. Arthroscopic treatment of multidirectional shoulder instability in athletes: a retrospective analysis of 2- to 5-year clinical outcomes. Am J Sports Med. 2009 Sep. 37(9):1712-20.[↩][↩]
- Illyes A, Kiss J, Kiss RM. Electromyographic analysis during pull, forward punch, elevation and overhead throw after conservative treatment or capsular shift at patient with multidirectional shoulder joint instability. J Electromyogr Kinesiol. 2009 Dec. 19(6):e438-47.[↩][↩]
- Kiss RM, Illyes A, Kiss J. Physiotherapy vs. capsular shift and physiotherapy in multidirectional shoulder joint instability. J Electromyogr Kinesiol. 2009 Oct 13. epub ahead of print.[↩][↩]





{kind=link}