What is thyroid function test
Thyroid function test is used to check how well your thyroid is working and to find the cause of problems such as hyperthyroidism or hypothyroidism. The thyroid is a small, butterfly-shaped gland in the front of your neck that makes two thyroid hormones: thyroxine (T4) and triiodothyronine (T3). Thyroid hormones control how your body uses energy, so they affect nearly every organ in your body, even your heart.
Thyroxine (T4) and triiodothyronine (T3) circulate almost entirely bound to specific transport proteins, and there are some situations which these proteins could change their level in the blood, producing also changes in the thyroxine (T4) and triiodothyronine (T3) levels (it happens frequently during pregnancy, women who take control birth pills, etc).
The thyroid function test usually includes:
- TSH (thyroid-stimulating hormone) – to test for hypothyroidism, hyperthyroidism and to monitor treatment for a thyroid disorder. Thyroid stimulating hormone (TSH) is produced by the pituitary gland and is part of the body’s feedback system to maintain stable amounts of the thyroid hormones thyroxine (T4) and triiodothyronine (T3) in the blood. When thyroid hormone levels decrease, the pituitary is stimulated to release TSH. Thyroid stimulating hormone (TSH) in turn stimulates the production and release of T4 and T3 by the thyroid gland. When the system is functioning normally, thyroid production turns on and off to maintain constant blood thyroid hormone levels.
- T4 (thyroxine) – to test for hypothyroidism and hyperthyroidism; may also be used to monitor treatment. Another measurement done to assess the thyroid status of patients is the “Free T4” measurement. The Free T4 avoids any change the proteins could have, giving us a more accurate value for the T4 level (see below).
- Free T3 or total T3 (triiodothyronine) – to test for hyperthyroidism; may also be used to monitor treatment
The total T4 and total T3 tests have been used for many years, but they can be affected by the amount of protein available in the blood to bind to the hormone. The free T4 and free T3 tests are not affected by protein levels and are thought by many to be more accurate reflections of thyroid hormone function. In most cases, the free T4 test has replaced that of the total T4 test. However, some professional guidelines recommend the total T3 test, so either total T3 or free T3 test may be used to assess thyroid function.
Thyroid blood tests help health care professionals diagnose thyroid diseases such as:
- Hyperthyroidism—when thyroid hormone levels are too high
- Graves’ disease, the most common cause of hyperthyroidism
- Hypothyroidism—when thyroid hormones levels are too low
- Hashimoto’s disease, of the most common cause of hypothyroidism
- Thyroid nodules and thyroid cancer
Your doctor will start with blood tests and may also order imaging tests.
In the past, thyroid function panel tests were more common. More recently, however, the practice has been to order, where possible, one initial or screening test and then follow up with additional testing, if needed, to reduce the number of unnecessary tests. With thyroid testing, one strategy is to screen with a TSH test and then order additional tests if the results are abnormal or if clinical suspicions warrant.
It is important to note that thyroid tests are a “snapshot” of what is occurring within a dynamic system. An individual person’s total T4, free T4, total T3, free T3, and/or TSH results may vary and may be affected by:
- Increases, decreases, and changes (inherited or acquired) in the proteins that bind T4 and T3
- Pregnancy
- Estrogen and other drugs
- Liver disease
- Systemic illness
- Resistance to thyroid hormones
- Pituitary dysfunction
What other tests may be ordered in addition to a thyroid function test?
Blood tests that may be performed in addition to a thyroid function test may include:
- Thyroid antibodies – to help differentiate different types of thyroiditis and identify autoimmune thyroid conditions
- Calcitonin – to help detect the presence of excessive calcitonin production as can occur with C-cell hyperplasia and medullary thyroid cancer
- Thyroglobulin – to monitor treatment of thyroid cancer
- Thyroxine-binding globulin (TBG) – to evaluate patients with abnormal T4 and T3 levels.
Is fasting required for thyroid blood test?
No fasting or test preparation is needed for thyroid blood test. Certain medications can interfere with the thyroid blood tests, so tell the health practitioner about any drugs being taken.
What is reverse T3?
Reverse T3 (RT3 or REVT3) is a biologically inactive form of T3. Normally, when T4 is converted to T3 in the body, a certain percentage of the T3 is in the form of RT3. When the body is under stress, such as during a serious illness, thyroid hormone levels may be outside of normal ranges even though there is no thyroid disease present. RT3 may be elevated in non-thyroidal conditions, particularly the stress of illness. It is generally recommended that thyroid testing be avoided in hospitalized patients or deferred until after a person has recovered from an acute illness. Use of the RT3 test remains controversial, and it is not widely requested.
How does the thyroid gland function?
The major thyroid hormone secreted by the thyroid gland is thyroxine, also called T4 because it contains four iodine atoms. To exert its effects, thyroxine (T4) is converted to triiodothyronine (T3) by the removal of an iodine atom. This occurs mainly in the liver and in certain tissues where T3 acts, such as in the brain. The amount of T4 produced by the thyroid gland is controlled by another hormone, which is made in the pituitary gland located at the base of the brain, called thyroid stimulating hormone (abbreviated TSH). The amount of thyroid stimulating hormone (TSH) that the pituitary sends into the blood stream depends on the amount of T4 that the pituitary sees. If the pituitary sees very little T4, then it produces more TSH to tell the thyroid gland to produce more T4. Once the T4 in the blood stream goes above a certain level, the pituitary’s production of TSH is shut off. In fact, the thyroid and pituitary act in many ways like a heater and a thermostat. When the heater is off and it becomes cold, the thermostat reads the temperature and turns on the heater. When the heat rises to an appropriate level, the thermostat senses this and turns off the heater. Thus, the thyroid and the pituitary, like a heater and thermostat, turn on and off. This is illustrated in the Figure 1 below.
Control of Thyroid Hormone Secretion
Thyrotropin-releasing hormone (TRH) from the hypothalamus and thyroid-stimulating hormone (TSH) from the anterior pituitary stimulate secretion of thyroid hormones, as shown in Figure 1:
- Low blood levels of triiodothyronine (T3) and thyroxine (T4) or low metabolic rate stimulate the hypothalamus to secrete thyrotropin-releasing hormone (TRH).
- Thyrotropin-releasing hormone (TRH) enters the hypothalamic–hypophyseal portal system and flows to the anterior pituitary, where it stimulates thyrotrophs to secrete thyroid stimulating hormone (TSH).
- Thyroid stimulating hormone (TSH) stimulates virtually all aspects of thyroid follicular cell activity, including iodide trapping, hormone synthesis and secretion, and growth of the follicular cells.
- The thyroid follicular cells release triiodothyronine (T3) and thyroxine (T4) into the blood until the metabolic rate returns to normal.
- An elevated level of triiodothyronine (T3) inhibits release of TRH and TSH (negative feedback inhibition).
Conditions that increase ATP demand—a cold environment, hypoglycemia, high altitude, and pregnancy—increase the secretion of the thyroid hormones.
Figure 1. Control of Thyroid Hormone Secretion
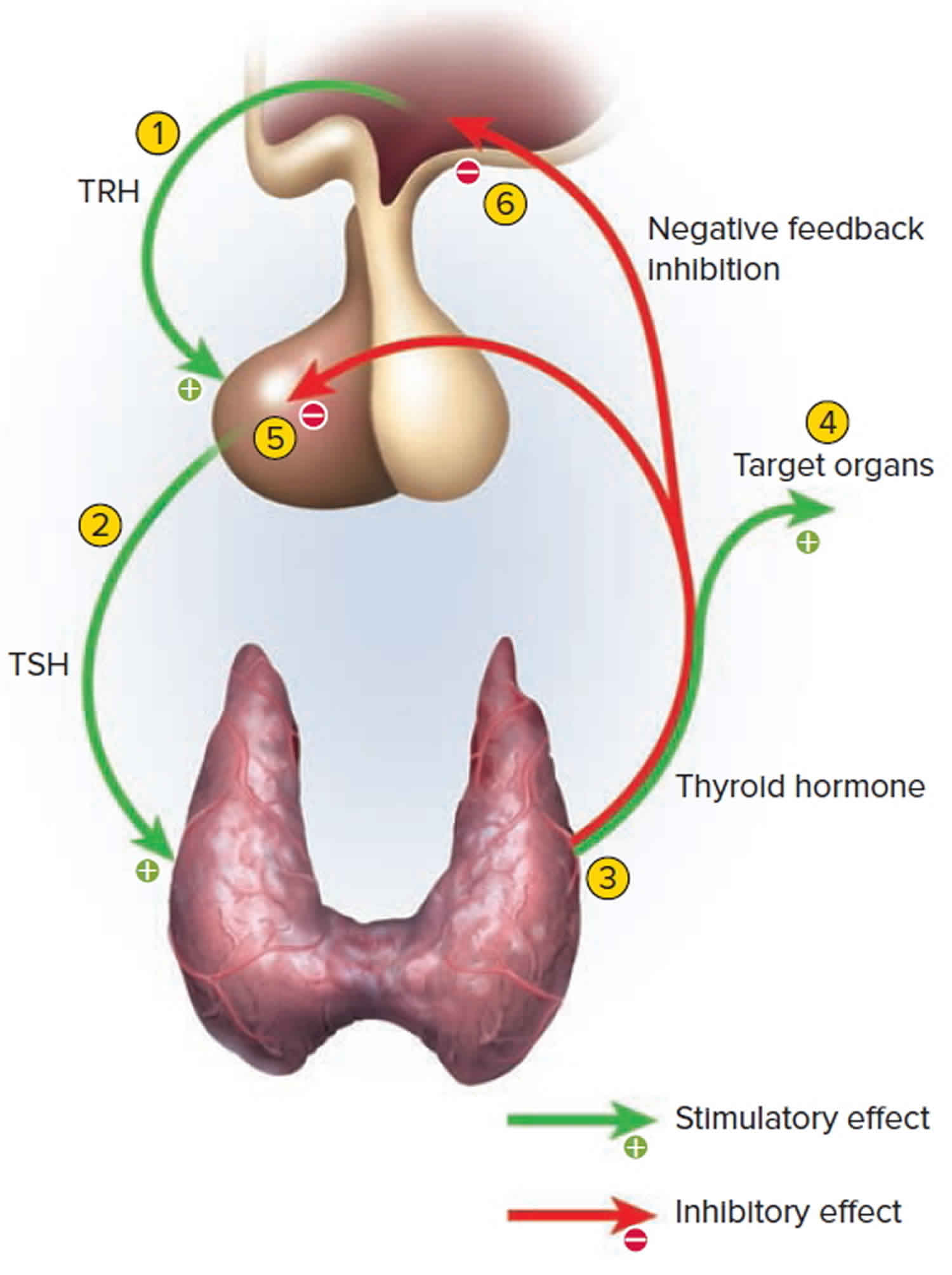
Footnote: Negative Feedback Inhibition of the Anterior Pituitary Gland by the Thyroid Gland
What imaging tests do doctors use to diagnose and find the cause of thyroid disease?
Your health care professional may order one or more imaging tests to diagnose and find the cause of thyroid disease. A trained technician usually does these tests in your doctor’s office, outpatient center, or hospital. A radiologist, a doctor who specializes in medical imaging, reviews the images and sends a report for your health care professional to discuss with you.
Thyroid ultrasound
Ultrasound of the thyroid is most often used to look for, or more closely at, thyroid nodules. Thyroid nodules are lumps in your neck. Ultrasound can help your doctor tell if the nodules are more likely to be cancerous.
For an ultrasound, you will lie on an exam table and a technician will run a device called a transducer over your neck. The transducer bounces safe, painless sound waves off your neck to make pictures of your thyroid. The ultrasound usually takes around 30 minutes.
Thyroid scan
Health care professionals use a thyroid scan to look at the size, shape, and position of the thyroid gland. This test uses a small amount of radioactive iodine to help find the cause of hyperthyroidism and check for thyroid nodules. Your health care professional may ask you to avoid foods high in iodine, such as kelp, or medicines containing iodine for a week before the test.
For the scan, a technician injects a small amount of radioactive iodine or a similar substance into your vein. You also may swallow the substance in liquid or capsule form. The scan takes place 30 minutes after an injection, or up to 24 hours after you swallow the substance, so your thyroid has enough time to absorb it.
During the scan, you will lie on an exam table while a special camera takes pictures of your thyroid. The scan usually takes 30 minutes or less.
Thyroid nodules that make too much thyroid hormone show up clearly in the pictures. Radioactive iodine that shows up over the whole thyroid could mean you have Graves’ disease.
Even though only a small amount of radiation is needed for a thyroid scan and it is thought to be safe, you should not have this test if you are pregnant or breastfeeding.
Radioactive iodine uptake test
A radioactive iodine uptake test (RAIU), also called a thyroid uptake test, can help check thyroid function and find the cause of hyperthyroidism. The thyroid “takes up” iodine from the blood to make thyroid hormones, which is why this is called an uptake test. Your health care professional may ask you to avoid foods high in iodine, such as kelp, or medicines containing iodine for a week before the test.
For this test, you will swallow a small amount of radioactive iodine in liquid or capsule form. During the test, you will sit in a chair while a technician places a device called a gamma probe in front of your neck, near your thyroid gland. The probe measures how much radioactive iodine your thyroid takes up from your blood. Measurements are often taken 4 to 6 hours after you swallow the radioactive iodine and again at 24 hours. The test takes only a few minutes.
If your thyroid collects a large amount of radioactive iodine, you may have Graves’ disease, or one or more nodules that make too much thyroid hormone. You may have this test at the same time as a thyroid scan.
Even though the test uses a small amount of radiation and is thought to be safe, you should not have this test if you are pregnant or breastfeeding.
What tests do doctors use if I have a thyroid nodule?
If your health care professional finds a nodule or lump in your neck during a physical exam or on thyroid imaging tests, you may have a fine needle aspiration biopsy to see if the lump is cancerous or noncancerous.
For this test, you will lie on an exam table and slightly bend your neck backward. A technician will clean your neck with an antiseptic and may use medicine to numb the area. An endocrinologist who treats people with endocrine gland problems like thyroid disease, or a specially trained radiologist, will place a needle through the skin and use ultrasound to guide the needle to the nodule. Small samples of tissue from the nodule will be sent to a lab for testing. This procedure usually takes less than 30 minutes. Your health care professional will talk with you about the test result when it is available.
Thyroid function blood test
Doctors may order one or more blood tests to check your thyroid function. Tests may include thyroid stimulating hormone (TSH), thyroxine (T4), triiodothyronine (T3), and thyroid antibody tests.
Thyroid blood test normal range
Total thyroxine (T4)
Pediatric
- 0-5 days of age: 5.0-18.5 mcg/dL
- 6 days-2 months: 5.4-17.0 mcg/dL
- 3-11 months: 5.7-16.0 mcg/dL
- 1-5 years: 6.0-14.7 mcg/dL
- 6-10 years: 6.0-13.8 mcg/dL
- 11-19 years: 5.9-13.2 mcg/dL
Adult (> or =20 years): 4.5-11.7 mcg/dL
- Values of more than 11.7 mcg/dL in adults or more than the age-related cutoffs in children are seen in hyperthyroidism and patients with acute thyroiditis.
- Values below 4.5 mcg/dL in adults or below the age-related cutoffs in children are seen in hypothyroidism, myxedema, cretinism, chronic thyroiditis, and occasionally, subacute thyroiditis.
- Increased total thyroxine (T4) is seen in pregnancy and patients who are on estrogen medication. These patients have increased total T4 levels (increased thyroxine-binding globulin: TBG levels).
- Decreased total T4 is seen in patients on treatment with anabolic steroids, or nephrosis (decreased TBG levels).
- A thyrotropin-releasing hormone stimulation test may be required for certain cases of hyperthyroidism.
Clinical findings are necessary to determine if thyroid-stimulating hormone, TBG, or free T4 testing is needed.
Free thyroxine (FT4)
Pediatric
- 0-5 days of age: 0.9-2.5 ng/dL
- 6 days-2 months: 0.9-2.2 ng/dL
- 3-11 months: 0.9-2.0 ng/dL
- 1-5 years: 1.0-1.8 ng/dL
- 6-10 years: 1.0-1.7 ng/dL
- 11-19 years: 1.0-1.6 ng/dL
Adult (> or =20 years of age): 0.9-1.7 ng/dL
Total triiodothyronine (T3)
Pediatric
- 0-5 days of age: 73-288 ng/dL
- 6 days-2 months: 80-275 ng/dL
- 3-11 months: 86-265 ng/dL
- 1-5 years: 92-248 ng/dL
- 6-10 years: 93-231 ng/dL
- 11-19 years: 91-218 ng/dL
Adult (> or =20 years): 80-200 ng/dL
- Triiodothyronine (T3) is not a reliable marker for hypothyroidism.
- T3 is not useful for general screening of the population without a clinical suspicion of hyperthyroidism. Therapy with amiodarone can lead to depressed T3 values.
- Triiodothyronine (T3) values >200 ng/dL in adults or > age related cutoffs in children are consistent with hyperthyroidism or increased thyroid hormone-binding proteins.
- Abnormal levels (high or low) of thyroid hormone-binding proteins (primarily albumin and thyroid-binding globulin) may cause abnormal T3 concentrations in normal thyroid patients.
- Phenytoin, phenylbutazone, and salicylates cause release of T3 from the binding proteins, thus leading to a reduction in the total T3 hormone level at normal free T3 levels.
- Autoantibodies to thyroid hormones can interfere with the assay.
- Binding protein anomalies may cause values that deviate from the expected results. Pathological concentrations of binding proteins can lead to results outside the reference range, although the patient may be in a euthyroid state. Free T3 or free T4 testing is indicated in these cases.
- Some patients who have been exposed to animal antigens, either in the environment or as part of treatment or imaging procedures, may have circulating antianimal antibodies present. These antibodies may interfere with the assay reagents to produce unreliable results.
Free triiodothyronine (FT3)
- Age > or =1 year: 2.8-4.4 pg/mL
Normally triiodothyronine (T3) circulates tightly bound to thyroxine-binding globulin and albumin. Only 0.3% of the total T3 is unbound (free); the free fraction is the active form.
- Free triiodothyronine (T3) is a second- or third-level test of thyroid function; it provides further confirmation of hyperthyroidism, supplementing the tetraiodothyronine (T4), sensitive thyrotropin (sTSH), and total T3 assays
- In hyperthyroidism, both thyroxine (tetraiodothyronine; thyroxine: T4) and T3 levels (total and free) are usually elevated, but in a small subset of hyperthyroid patients (T3 toxicosis) only T3 is elevated. Generally, free T3 (FT3) measurement is not necessary since total T3 will suffice. However, FT3 levels may be required to evaluate clinically euthyroid patients who have an altered distribution of binding proteins (eg, pregnancy, dysalbuminemia).
- Some investigators recommend the FT3 assay for monitoring thyroid replacement therapy, although its clinical role is not precisely defined.
Thyroid stimulating hormone (TSH)
Thyroid stimulating hormone (TSH) normal levels:
Pediatric
- 0-5 days age: 0.7-15.2 mIU/L
- 6 days-2 months: 0.7-11.0 mIU/L
- 3-11 months: 0.7-8.4 mIU/L
- 1-5 years: 0.7-6.0 mIU/L
- 6-10 years: 0.6-4.8 mIU/L
- 11-19 years: 0.5-4.3 mIU/L
Adults (> or =20 years): 0.3-4.2 mIU/L
The ability to quantitate circulating levels of TSH is important in evaluating thyroid function. It is especially useful in the differential diagnosis of primary (thyroid) from secondary (pituitary) and tertiary (hypothalamus) hypothyroidism. In primary hypothyroidism, TSH levels are significantly elevated, while in secondary and tertiary hypothyroidism, TSH levels are low or normal.
For diagnostic purposes, the results should always be assessed in conjunction with the patient’s medical history, clinical examination and other findings.
- In primary hypothyroidism, thyroid-stimulating hormone (TSH) levels will be elevated. In primary hyperthyroidism, TSH levels will be low.
- Elevated or low TSH in the context of normal free thyroxine (FT4) is often referred to as subclinical hypo- or hyperthyroidism, respectively.
- Thyrotropin-releasing hormone (TRH) stimulation differentiates all types of hypothyroidism by observing the change in patient TSH levels in response to TRH. Typically, the TSH response to thyrotropin-releasing hormone (TRH) stimulation is exaggerated in cases of primary hypothyroidism, absent in secondary hypothyroidism, and delayed in tertiary hypothyroidism. Most individuals with primary hyperthyroidism have TSH suppression and do not respond to thyrotropin-releasing hormone (TRH) stimulation with an increase in TSH over their basal value.
- Sick, hospitalized patients may have falsely low or transiently elevated TSH.
Thyroid stimulating hormone (TSH) test
The best way to initially test thyroid function is to measure the thyroid stimulating hormone (TSH) level in a blood sample. A high TSH level indicates that the thyroid gland is failing because of a problem that is directly affecting the thyroid (primary hypothyroidism). The opposite situation, in which the TSH level is low, usually indicates that the person has an overactive thyroid that is producing too much thyroid hormone (hyperthyroidism). Occasionally, a low TSH may result from an abnormality in the pituitary gland, which prevents it from making enough thyroid stimulating hormone (TSH) to stimulate the thyroid (secondary hypothyroidism). In most healthy individuals, a normal TSH value means that the thyroid is functioning normally.
For these tests, a health care professional will draw blood from your arm and send it to a lab for testing. Your doctor will talk to you about your test results.
thyroid stimulating hormone (TSH) test
Health care professionals usually check the amount of thyroid stimulating hormone (TSH) in your blood first. Thyroid stimulating hormone (TSH) is a hormone made in the pituitary gland that tells the thyroid how much thyroxine (T4) and triiodothyronine (T3) to make.
- A high TSH level most often means you have hypothyroidism, or an underactive thyroid. This means that your thyroid isn’t making enough hormone. As a result, the pituitary keeps making and releasing TSH into your blood.
- A low TSH level usually means you have hyperthyroidism, or an overactive thyroid. This means that your thyroid is making too much hormone, so the pituitary stops making and releasing TSH into your blood.
If the TSH test results are not normal, you will need at least one other test to help find the cause of the problem.
Thyroxine (T4) tests
Thyroxine (T4) circulates in the blood in two forms:
- T4 bound to proteins that prevent the T4 from entering the various tissues that need thyroid hormone.
- Free T4, which does enter the various target tissues to exert its effects. The free T4 fraction is the most important to determine how the thyroid is functioning, and tests to measure this are called the Free T4 (FT4) and the Free T4 Index (FT4I or FTI). Individuals who have hyperthyroidism will have an elevated FT4 or FTI, whereas patients with hypothyroidism will have a low level of FT4 or FTI.
A high blood level of thyroxine (T4) may mean you have hyperthyroidism. A low level of T4 may mean you have hypothyroidism.
Combining the thyroid stimulating hormone (TSH) test with the Free T4 (FT4) or Free T4 Index (FTI) accurately determines how the thyroid gland is functioning.
The finding of an elevated thyroid stimulating hormone (TSH) and low Free T4 or Free T4 Index indicates primary hypothyroidism due to disease in the thyroid gland. A low TSH and low Free T4 or Free T4 Index indicates hypothyroidism due to a problem involving the pituitary gland. A low TSH with an elevated Free T4 or Free T4 Index is found in individuals who have hyperthyroidism.
In some cases, high or low thyroxine (T4) levels may not mean you have thyroid problems. If you are pregnant or are taking oral contraceptives , your thyroid hormone levels will be higher. Severe illness or using corticosteroids—medicines to treat asthma, arthritis, skin conditions, and other health problems—can lower T4 levels. These conditions and medicines change the amount of proteins in your blood that “bind,” or attach, to T4. Bound T4 is kept in reserve in the blood until it’s needed. “Free” T4 is not bound to these proteins and is available to enter body tissues. Because changes in binding protein levels don’t affect free T4 levels, many healthcare professionals prefer to measure Free T4 (FT4).
Triiodothyronine (T3) test
Triiodothyronine (T3) tests are often useful to diagnosis hyperthyroidism or to determine the severity of the hyperthyroidism. If your health care professional thinks you may have hyperthyroidism even though your thyroxine (T4) level is normal, you may have a triiodothyronine (T3) test to confirm the diagnosis. Sometimes T4 is normal yet T3 is high, so measuring both T4 and T3 levels can be useful in diagnosing hyperthyroidism.
Patients who are hyperthyroid will have an elevated T3 level. In some individuals with a low TSH, only the T3 is elevated and the Free T4 or Free T4 Index is normal. Triiodothyronine (T3) testing rarely is helpful in the hypothyroid patient, since it is the last test to become abnormal. Patients can be severely hypothyroid with a high TSH and low Free T4 or Free T4 Index, but have a normal T3. In some situations, such as during pregnancy or while taking birth control pills, high levels of total T4 and T3 can exist. This is because the estrogens increase the level of the binding proteins. In these situations, it is better to ask both for TSH and free T4 for thyroid evaluation.
Thyroid antibody tests
The immune system of the body normally protects us from foreign invaders such as bacteria and viruses by destroying these invaders with substances called antibodies produced by blood cells known as lymphocytes. In many patients with hypothyroidism or hyperthyroidism, lymphocytes make antibodies against their thyroid that either stimulate or damage the thyroid gland. Two common antibodies that cause thyroid problems are directed against thyroid cell proteins: thyroid peroxidase (anti-thyroid peroxidase antibody or TPO) and thyroglobulin (anti-thyroglobulin antibody or TgAb).
Measuring levels of thyroid antibodies may help diagnose an autoimmune thyroid disorder such as Graves’ disease—the most common cause of hyperthyroidism—and Hashimoto’s disease—the most common cause of hypothyroidism. Thyroid antibodies are made when your immune system attacks the thyroid gland by mistake. Your health care professional may order thyroid antibody tests if the results of other blood tests suggest thyroid disease. For example, positive anti-thyroid peroxidase and/or anti-thyroglobulin antibodies in a patient with hypothyroidism make a diagnosis of Hashimoto’s thyroiditis. If the antibodies are positive in a hyperthyroid patient, the most likely diagnosis is autoimmune thyroid disease.
Thyroid function test interpretation
If the feedback system involving the thyroid gland is not functioning properly due to one of a variety of disorders, then increased or decreased amounts of thyroid hormones may result. When TSH concentrations are increased, the thyroid will make and release inappropriate amounts of T4 and T3 and the person may experience symptoms associated with hyperthyroidism. If there is decreased production of thyroid hormones, the person may experience symptoms of hypothyroidism.
The following table summarizes some examples of typical test results and their potential meaning.
The most common causes of thyroid dysfunction are autoimmune-related. Graves disease causes hyperthyroidism and Hashimoto thyroiditis causes hypothyroidism. Both hyper- and hypothyroidism can also be caused by thyroiditis, thyroid cancer, and excessive or deficient production of TSH.
Table 1. Thyroid function blood test results and interpretation
| TSH | T4 | T3 | Interpretation |
|---|---|---|---|
| High | Normal | Normal | Mild (subclinical) hypothyroidism |
| High | Low | Low or normal | Hypothyroidism |
| Low | Normal | Normal | Mild (subclinical) hyperthyroidism |
| Low | High or normal | High or normal | Hyperthyroidism |
| Low | Low or normal | Low or normal | Nonthyroidal illness; pituitary (secondary) hypothyroidism |
| Normal | High | High | Thyroid hormone resistance syndrome (a mutation in the thyroid hormone receptor decreases thyroid hormone function) |
The above test results alone are not diagnostic but will prompt a health practitioner to perform additional testing to investigate the cause of the excess or deficiency and thyroid disorder. As examples, the most common cause of hyperthyroidism is Graves disease and the most common cause of hypothyroidism is Hashimoto thyroiditis.





{kind=link}