
Tic douloureux
Tic douloureux also called trigeminal neuralgia, is a chronic pain condition that causes extreme, sporadic, sudden burning or shock-like face pain. The term “tic douloureux” was given by the French physician Nicolaus Andre in 1756, because of the facial spasms, that can sometimes accompany the severe pain attacks 1. Trigeminal neuralgia is often described as a sharp shooting pain or like having an electric shock in the jaw, teeth or gums. The pain happens in short, unpredictable attacks that seldom lasts more than a few seconds or a minute or two per episode. The attacks stop as suddenly as they start. But trigeminal neuralgia can progress and cause longer, more-frequent bouts of searing pain. In most cases, trigeminal neuralgia affects just one side of the face, with the pain usually felt in the lower part of the face. Very occasionally the pain can affect both sides of the face, although not usually at the same time.
The intensity of pain can be physically and mentally incapacitating. People with tic douloureux may experience attacks of pain regularly for days, weeks or months at a time. In severe cases attacks may happen hundreds of times a day. Although sometimes debilitating, the disorder is not life-threatening. Spontaneous remission is possible, but most patients have episodic attacks over many years.
Tic douloureux pain is typically felt on one side of the jaw or cheek. Episodes can last for days, weeks, or months at a time and then disappear for months or years. In the days before an episode begins, some patients may experience a tingling or numbing sensation or a somewhat constant and aching pain. The attacks often worsen over time, with fewer and shorter pain-free periods before they recur. The intense flashes of pain can be triggered by vibration or contact with the cheek (such as when shaving, washing the face, or applying makeup), brushing teeth, eating, drinking, talking, or being exposed to the wind. Tic douloureux occurs most often in people who are older than 50, but it can occur at any age and very rarely seen in children 2. Trigeminal neuralgia affects 4 to 13 per 100,000 people annually. Women are affected more compared to men. The male-to-female prevalence ratio ranges from 1 to 1.5 to 1 to 1.7. The lifetime prevalence in population-based studies was estimated to be about 0.16% to 0.3% 3.
Trigeminal neuralgia is generally sporadic, although there have been reports of the disease occurring in several members of the same family, perhaps because of an inherited pattern of blood vessel formation. The presumed cause of tic douloureux or trigeminal neuralgia is a blood vessel pressing on the trigeminal nerve in the head as it exits the brainstem. Tic douloureux may be part of the normal aging process but in some cases it is the associated with another disorder, such as multiple sclerosis or other disorders characterized by damage to the myelin sheath that covers certain nerves.
The development of trigeminal neuralgia in a young person should raise suspicion for multiple sclerosis. The prevalence of tic douloureux or trigeminal neuralgia in patients with multiple sclerosis is between 1 and 6.3%, making it the most common associated disease 4. It is also reported that patients with hypertension have a slightly higher incidence of tic douloureux compared to the general population 1. There is no racial predilection 4.
Trigeminal nerve anatomy
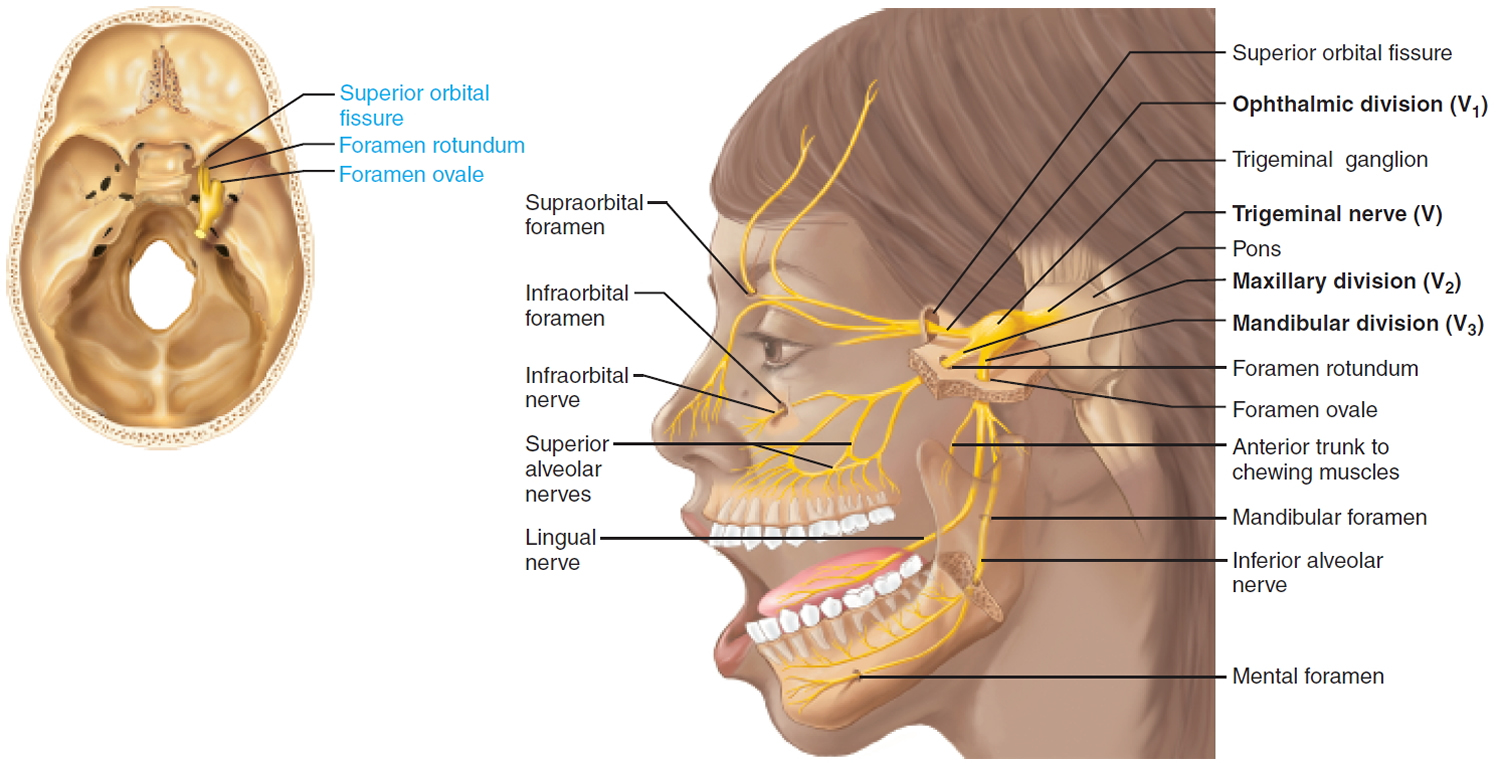
The trigeminal nerve is the fifth cranial nerve (CN V). It is responsible for the sensory supply of the face and the motor and sensory supply to the muscles of mastication. The trigeminal nerve (trigeminal = threefold) starts at the pons and divides into three branches 5:
- Ophthalmic (V1): Supplies the eye, upper eyelid, and the forehead
- Maxillary (V2): Supplies lower eyelid, cheek, nostril, upper lip, and upper gum
- Mandibular (V3): Supplies the lower lip, lower gum, jaw and the muscles of mastication
The trigeminal nerve is mixed nerve and it is the general somatic sensory nerve of the face for touch, temperature, and pain. The mandibular division supplies somatic motor innervation to the chewing muscles.
Sensory function:
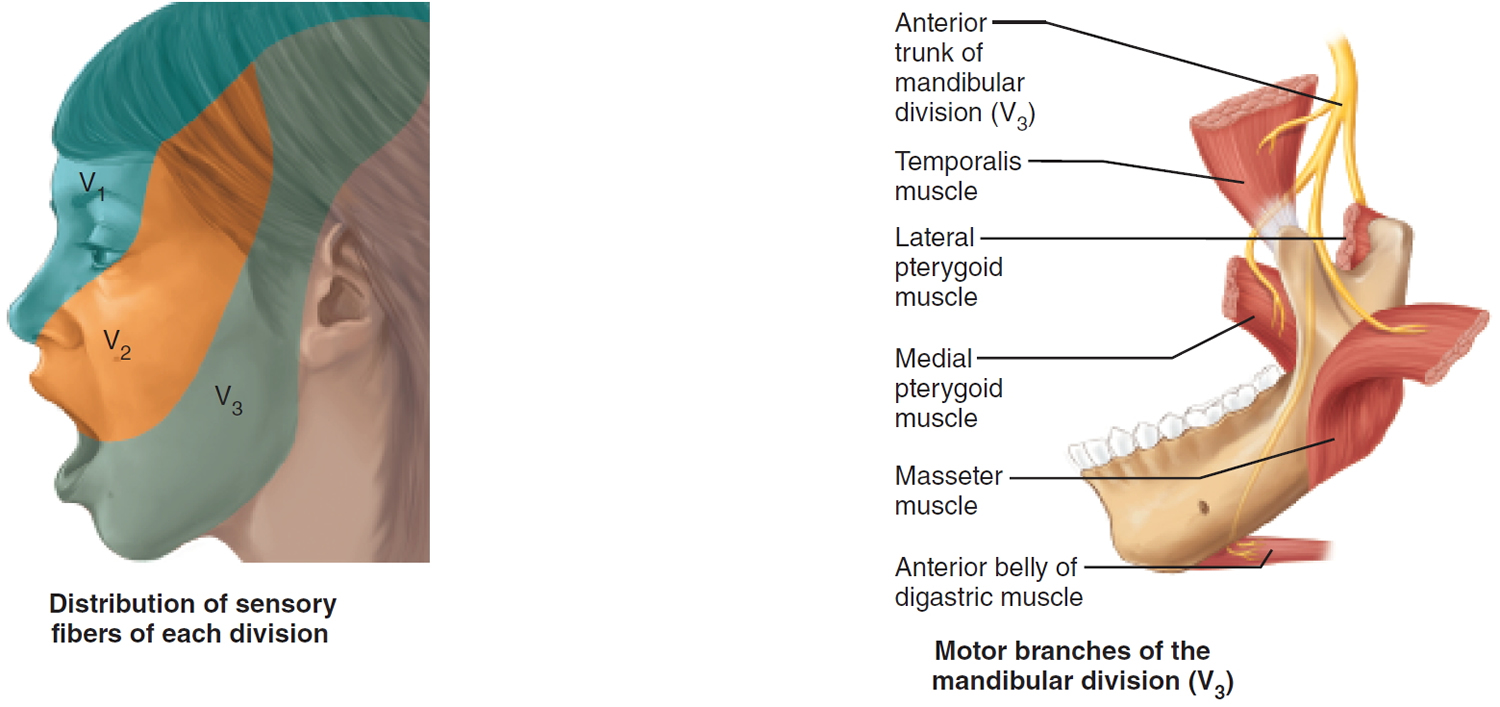
- V1 General somatic sensation from skin of anterior scalp and forehead, upper eyelid and nose, nasal cavity mucosa, cornea, and lacrimal gland.
- V2 General somatic sensation from skin of cheek, upper lip, and lower eyelid, nasal cavity mucosa, palate, upper teeth.
- V3 General somatic sensation from skin of chin and temporal region of scalp, anterior tongue and lower teeth.
Somatic motor function: V3 Innervate the muscles of mastication: temporalis, masseter, pterygoids, anterior belly of digastric. Afferent proprioceptor fibers return from these muscles.
Clinical significance: Anesthesia for Upper and Lower Jaws. Dentists desensitize upper and lower jaws by injecting local anesthetic (such as Novocain) into alveolar branches of the maxillary and mandibular divisions of the trigeminal nerve, respectively. This blocks pain-transmitting fibers from the teeth, and the surrounding tissues become numb.
Origin: Sensory receptors in skin and mucosa of face. Motor fibers from trigeminal motor nucleus in pons.
Pathway: Cell bodies of sensory neurons of all three divisions located in the large trigeminal ganglion. Fibers extend to trigeminal nuclei in the pons.
Through the Skull: V1 Superior orbital fissure. Cutaneous Branch: Supraorbital foramen.
Through the Skull: V2 Foramen rotundum. Cutaneous Branch: Infraorbital foramen.
Through the Skull: V3 Foramen ovale and Mandibular foramen. Cutaneous Branch: Mental foramen.
Figure 1. Trigeminal nerve (fifth cranial nerve)
Tic douloureux causes
In tic douloureux or trigeminal neuralgia, the trigeminal nerve’s function is disrupted. Most cases of trigeminal neuralgia are due to the compression of the trigeminal nerve root, within a few millimeters of its entry into the pons. Usually, the problem is contact between a normal blood vessel — in this case, an artery or a vein — and the trigeminal nerve at the base of your brain. This contact puts pressure on the nerve and causes it to malfunction. Between 80% and 90% of the cases of tic douloureux are caused by compression by an adjacent artery or a vein 6. The blood vessel, which has been mostly implicated in about 75% to 80% of the cases, is the superior cerebellar artery. Other blood vessels that are known to cause tic douloureux include the anterior inferior cerebellar artery, the vertebral artery, and the petrosal vein.
Some of the other causes of nerve compression include meningioma, acoustic neuroma, epidermoid cyst, and rarely by an arteriovenous malformation or a saccular aneurysm.
Tic douloureux can occur as a result of aging, or it can be related to multiple sclerosis (reported in about 2% to 4% of patients with tic douloureux) 7 or a similar disorder that damages the myelin sheath protecting certain nerves. Trigeminal neuralgia can also be caused by a tumor compressing the trigeminal nerve.
Some people may experience trigeminal neuralgia due to a brain lesion or other abnormalities. In other cases, surgical injuries, stroke or facial trauma may be responsible for trigeminal neuralgia.
Tic douloureux triggers
Attacks of tic douloureux can be triggered by certain actions or movements, such as:
- talking
- smiling
- chewing
- brushing your teeth
- washing your face
- a light touch or touching your face
- shaving
- putting on make-up
- swallowing
- eating
- drinking
- kissing
- a cool breeze or air conditioning
- head movements
- vibrations, such as walking or traveling in a car
However, pain can happen spontaneously with no trigger whatsoever.
Tic douloureux classification
Tic douloureux is divided into classic tic douloureux, secondary tic douloureux and idiopathic tic douloureux in the International Classification of Headache Disorders, Third Edition 8:
- Classic trigeminal neuralgia: This includes tic douloureux related to vascular compression.
- Secondary trigeminal neuralgia: This includes tic douloureux due to a tumor along the trigeminal nerve or tic douloureux due to an underlying disease like multiple sclerosis.
- Idiopathic trigeminal neuralgia: This is when the cause is unknown.
Considering the symptomatic aspect, trigeminal neuralgia can classify as 2:
- Type 1 – Presence of paroxysmal pain alone
- Type 2 – Paroxysmal pain along with constant pain in the background
The pain in trigeminal neuralgia occurs in paroxysms and is usually maximal at or near onset. Sometimes, with severe pain, facial muscle spasms can be seen. Hence, trigeminal neuralgia is also known as ‘tic douloureux.’
The majority of the patients describe the pain as electric shock-like pain, lasting from one to several seconds. Pain in trigeminal neuralgia is typically unilateral. Occasionally, it is bilateral, but very rarely occurs simultaneously on both sides 9. The pain episodes rarely occur during sleep.
V2 and V3 divisions of the trigeminal nerve are usually involved in the pain distribution 8. When the V1 subdivision is involved, mild autonomic symptoms like lacrimation, rhinorrhea, and conjunctival injection can be seen. However, isolated V1 division involvement is very rare and is seen in less than 5% of patients with trigeminal neuralgia 10.
Trigger zones may be present in the distribution of the affected nerve. These are usually located near the midline. They have been mostly reported in the nasal and perioral regions. trigeminal neuralgia pain is triggered by lightly touching these zones 11. Patients with trigeminal neuralgia are usually aware of these zones and avoid any stimulation of them. All patients with trigeminal neuralgia may not have trigger zones, but trigger zones are nearly pathognomonic for trigeminal neuralgia.
Other triggers reported causing trigeminal neuralgia paroxysms include brushing teeth, shaving, washing the face, smoking, chewing, talking, grimacing, or exposure to cold air 10.
In younger patients, who present with symptoms of trigeminal neuralgia, other neurological conditions like multiple sclerosis should merit consideration in the differentials. Such patients should be asked about other neurological symptoms like focal weakness, vision changes, dizziness, and ataxia.
In patients with trigeminal neuralgia, the physical examination is generally normal. Hence, the physicians should perform a detailed physical examination of the head, neck, eyes, ears, teeth, mouth, and the temporomandibular joint to rule out other causes of facial pain. The finding of typical trigger zones is suggestive of trigeminal neuralgia.
In patients with classic trigeminal neuralgia, the neurologic examination is normal. Hence, physical examination showing a sensory loss in trigeminal nerve distribution, loss of corneal reflex, or weakness in facial muscles should prompt the physician to consider secondary trigeminal neuralgia and other differentials.
Several patients with trigeminal neuralgia complain of toothache and pain with brushing teeth. A detailed oral examination can help in differentiating the dental causes of pain from trigeminal neuralgia.
Primary trigeminal neuralgia
Evidence suggests that in up to 95% of cases, trigeminal neuralgia is caused by pressure on the trigeminal nerve close to where it enters the brain stem, the lowest part of the brain that merges with the spinal cord. This type of trigeminal neuralgia is known as primary trigeminal neuralgia.
In most cases the pressure is caused by an artery or vein squashing (compressing) the trigeminal nerve. These are normal blood vessels that happen to come into contact with the nerve at a particularly sensitive point.
It’s not clear why this pressure can cause painful attacks in some people but not others, as not everyone with a compressed trigeminal nerve will experience pain.
It may be that, in some people, the pressure on the nerve wears away its protective outer layer (myelin sheath), which may cause pain signals to travel along the nerve. However, this does not fully explain why some people have periods without symptoms (remission), or why pain relief is immediate after a successful operation to move the blood vessels away from the nerve.
Secondary trigeminal neuralgia
Secondary trigeminal neuralgia is the term used when trigeminal neuralgia is caused by another medical condition or problem, including:
- a tumor
- a cyst – a fluid-filled sac
- arteriovenous malformation – an abnormal tangle of arteries and veins
- multiple sclerosis (MS) – a long-term condition that affects the nervous system
- facial injury
- damage caused by surgery including dental surgery
Tic douloureux pathophysiology
Most cases of trigeminal neuralgia are due to trigeminal nerve compression. It is believed that tic douloureux is related to nerve demyelination occurring around the site of compression. The mechanism of how demyelination leads to the symptoms of tic douloureux is not known. It is thought to be due to the ectopic impulse generation set up by the demyelinated lesion, thereby causing ephaptic transmission 12. The ephaptic link between fibers involved in pain generation and fibers mediating light touch could account for the precipitation of shock-like pains in the facial trigger zone by light tactile stimulation.
A triggered episode followed by refractory periods and a single stimulus leading to trains of painful sensations indicates the possible role of the central pain mechanism in tic douloureux. Altered grey matter in the sensory and motor cortex has also been described 13.
Some theories describe demyelination secondary to vascular compression of the nerve root by tortuous or aberrant vessels. Radiologic and pathologic studies have demonstrated the proximity of the trigeminal nerve root to such vessels. The vessel mostly implicated is the superior cerebellar artery 14. This hypothesis is further strengthened by the relief of symptoms following surgeries to separate the offending vessels from the nerve.
According to the bio-resonance hypothesis, when the vibration frequency of the trigeminal nerve and the surrounding structures come close to each other, the trigeminal nerve fibers are damaged, leading to abnormal transmission of impulse, thereby resulting in facial pain 15.
Multiple other conditions like amyloid infiltration, bony compression, arteriovenous malformation and small infarcts in the medulla and pons, have been described to cause tic douloureux.
Tic douloureux symptoms
Tic douloureux (trigeminal neuralgia) symptoms may include one or more of these patterns:
- Episodes of severe, shooting or jabbing pain that may feel like an electric shock
- Spontaneous attacks of pain or attacks triggered by things such as touching the face, chewing, speaking or brushing teeth
- Bouts of pain lasting from a few seconds to several minutes
- Episodes of several attacks lasting days, weeks, months or longer — some people have periods when they experience no pain
- Constant aching, burning feeling that may occur before it evolves into the spasm-like pain of trigeminal neuralgia
- Pain in areas supplied by the trigeminal nerve, including the cheek, jaw, teeth, gums, lips, or less often the eye and forehead
- Pain affecting one side of the face at a time, though may rarely affect both sides of the face
- Pain focused in one spot or spread in a wider pattern
- Attacks that become more frequent and intense over time
The main symptom of tic douloureux is sudden attacks of severe, sharp, shooting facial pain that last from a few seconds to about 2 minutes.
The pain is often described as excruciating, like an electric shock. The attacks can be so severe that you’re unable to do anything while they’re happening.
Trigeminal neuralgia usually affects one side of the face. In some cases it can affect both sides, although not usually at the same time.
The pain can be in the teeth, lower jaw, upper jaw or cheek. Less commonly the pain can also be in the forehead or eye.
You may sense when an attack is about to happen, although they usually start unexpectedly.
After the most severe pain has subsided you may experience a slight ache or burning feeling. You may also have a constant throbbing, aching or burning sensation between attacks.
You may experience regular episodes of pain for days, weeks or months at a time. Sometimes the pain may disappear completely and not return for several months or years. This is known as remission.
In severe cases of tic douloureux the attacks may happen hundreds of times a day and there may be no periods of remission.
Tic douloureux complications
- The pain in trigeminal neuralgia is so severe and debilitating that the patients can develop depression, if not adequately treated.
- Patients with severe pain associated with facial twitches can become socially withdrawn due to embarrassment and fear of an impending attack.
- Patients treated with anticonvulsant drugs over the long term can have adverse drug effects.
- Microvascular decompression and percutaneous neurosurgical procedures can pose surgical risks.
- Some patients permanently develop facial numbness on the affected side.
- Occasionally, patients develop corneal anesthesia and jaw weakness.
- Anesthesia dolorosa is seen in a few patients. It is an intractable facial dysesthesia, which can be more disabling than original trigeminal neuralgia.
The chief complication in tic douloureux is the adverse effects and toxicity experienced routinely with long-term use of anticonvulsant agents. Another complication is the waning efficacy over several years of these drugs in controlling neuralgia, necessitating the addition of a second anticonvulsant, which may cause more drug-related adverse reactions.
Failure to diagnose a brainstem tumor and bone marrow aplasia as an idiosyncratic adverse effect of carbamazepine are common pitfalls to avoid.
Standard care must be applied to invasive procedures, which are most subject to potential claims. Percutaneous neurosurgical procedures and microvascular decompression procedures pose risks of long-term complications. Perioperative risks also exist. Moreover, patients may have to wait for weeks or months after the operation for relief, and some find relief only for 1-2 years and then must weigh the option of a second operation.
Some patients permanently lose sensation over a portion of the face or mouth. Occasionally, patients may suffer jaw weakness and/or corneal anesthesia. Corneal ulceration can result because of trophic disturbances from nerve deafferentation.
After any invasive treatments, reactivation of a herpes simplex infection is not uncommon.
The worst complication is anesthesia dolorosa, an intractable facial dysesthesia, which may be more disabling than the original trigeminal neuralgia. This dysesthesia may be caused by procedures and, sometimes, surgery.
Tic douloureux diagnosis
Tic douloureux can be difficult to diagnose. The diagnosis of trigeminal neuralgia should be considered in all patients with unilateral facial pain. Accurate and prompt diagnosis is important because the pain of trigeminal neuralgia can be severe. Your doctor will try to identify the problem by asking about your symptoms and ruling out other conditions that could be responsible for your pain.
Your doctor will diagnose tic douloureux mainly based on your description of the pain, including:
- Type. Pain related to tic douloureux is sudden, shock-like and brief.
- Location. The parts of your face that are affected by pain will tell your doctor if the trigeminal nerve is involved.
- Triggers. Trigeminal neuralgia-related pain usually is brought on by light stimulation of your cheeks, such as from eating, talking or even encountering a cool breeze.
Your doctor may conduct many tests to diagnose tic douloureux and determine underlying causes for your condition, including:
- A neurological examination. Touching and examining parts of your face can help your doctor determine exactly where the pain is occurring and — if you appear to have tic douloureux — which branches of the trigeminal nerve may be affected. Reflex tests also can help your doctor determine if your symptoms are caused by a compressed nerve or another condition.
- Magnetic resonance imaging (MRI). MRI of the brain is preferred over CT, as the MRI helps in evaluating small adjacent lesions as well. Your doctor may order an MRI scan of your head to determine if multiple sclerosis or a tumor is causing tic douloureux. In some cases, your doctor may inject a dye into a blood vessel to view the arteries and veins and highlight blood flow (magnetic resonance angiogram).
Your facial pain may be caused by many different conditions, so an accurate diagnosis is important. Your doctor may order additional tests to rule out other conditions.
There are certain diagnostic criteria established by the International Classification of Headache Disorders, Third Edition 8, which can help in the diagnosis of trigeminal neuralgia. These criteria are as follows 8:
- A) Recurrent paroxysms of facial pain unilaterally in the distribution of trigeminal nerve and fulfilling criteria B and C.
- B) Pain has the following characteristics:
- Pain lasting a fraction of a second to about 2 minutes
- Pain with severe intensity
- Electrick-shock like or shooting pain with sharp quality
- C) Innocuous stimuli precipitate the pain in the affected distribution
- D) No alternative ICHD-3 diagnosis better explaining the symptoms
The subtypes of trigeminal neuralgia are defined by International Classification of Headache Disorders, Third Edition as follows 8:
- Classic trigeminal neuralgia: This is secondary to neuromuscular compression and fulfilling the criteria above. This requires demonstration of the compression on an MRI or during the surgery for neuromuscular compression, with associated morphological changes in the trigeminal nerve root.
- Secondary trigeminal neuralgia: This is defined as trigeminal neuralgia secondary to an underlying disease. Some of the reported causes are multiple sclerosis, arteriovenous malformation, and cerebellopontine angle tumor.
- Idiopathic trigeminal neuralgia: This is defined as trigeminal neuralgia with no abnormalities seen on MRI or electrophysiological tests.
Neuroimaging studies like MRI Brain or CT Head can help in identifying causes like cerebellopontine angle tumor or multiple sclerosis, which can cause secondary trigeminal neuralgia 16. Magnetic resonance imaging or high-resolution MRI can help in identifying vascular compression as the cause in classic trigeminal neuralgia 17. A targeted MRI, which is a high-resolution MRI, can be performed with or without gadolinium contrast. This can give a detailed picture of the blood vessels and the brain. This is called FIESTA sequences in some MR machines. In these machines, sections as thin as 1 mm can be taken in a coronal plane, without any skips in between the images. This way, the imaging of the entire course of the trigeminal nerve can be obtained, and the offending vessel causing compression can be identified.
Hence, though trigeminal neuralgia is a clinical diagnosis, MRI of the brain with and without contrast is recommended to rule out a structural brain lesion in all patients with clinically suspected trigeminal neuralgia. It is also important to note that patients less than 40 years of age, patients with bilateral symptoms, and with the sensory loss on physical examination are at a higher risk of secondary trigeminal neuralgia.
Medical history
Because trigeminal neuralgia is a clinical diagnosis, the patient’s history is critical in the evaluation. Patients with trigeminal neuralgia present with a primary description of recurrent episodes of unilateral facial pain. Attacks last only seconds and may recur infrequently or as often as hundreds of times each day; they rarely occur during sleep. The pain is generally severe, and is described as a stabbing, sharp, shock-like, or superficial pain in the distribution of one or more of the trigeminal nerve divisions. Patients generally are asymptomatic between episodes, although some patients with long-standing trigeminal neuralgia have a persistent dull ache in the same area.
Talking, smiling, chewing, teeth brushing, and shaving have all been implicated as triggers for the pain. Even a breeze touching the face may cause a paroxysm of pain in some patients. In trigger zones—small areas near the nose or mouth in patients with trigeminal neuralgia—minimal stimulation initiates a painful attack. Patients with trigeminal neuralgia can pinpoint these areas and will assiduously avoid any stimulation of them. Not all patients with trigeminal neuralgia have trigger zones, but trigger zones are nearly pathognomonic for this disorder.
The patient’s history is also important for ruling out other causes of facial pain. Because of the association between trigeminal neuralgia and multiple sclerosis, patients should be asked about other neurologic symptoms, particularly those common in multiple sclerosis (e.g., ataxia, dizziness, focal weakness, unilateral vision changes). An evaluation for other diagnoses is indicated in younger patients, because classical trigeminal neuralgia is unusual in persons younger than 40 years 18.
Trigeminal neuralgia pain is nearly always unilateral. In rare cases of bilateral trigeminal neuralgia, individual attacks are usually unilateral, with distinct episodes involving each side of the face at separate times. Symptoms are always confined to the trigeminal nerve distribution, with most cases involving the second or third division, or both. The asymptomatic period between attacks is important to distinguish classical trigeminal neuralgia from other causes of facial pain, as well as from symptomatic trigeminal neuralgia. Patients with trigeminal neuralgia have stereotyped attacks; a change in the location, severity, or quality of the pain should alert the physician to the possibility of an alternative diagnosis.
Physical examination
The physical examination in patients with trigeminal neuralgia is generally normal. Therefore, physical examination in patients with facial pain is most useful for identifying abnormalities that point to other diagnoses. The physician should perform a careful examination of the head and neck, with an emphasis on the neurologic examination. The ears, mouth, teeth, and temporomandibular joint (TMJ) should be examined for problems that might cause facial pain.
The finding of typical trigger zones verifies the diagnosis of trigeminal neuralgia. Patients with classical trigeminal neuralgia have a normal neurologic examination. Sensory abnormalities in the trigeminal area, loss of corneal reflex, or evidence of any weakness in the facial muscles should prompt the physician to consider symptomatic trigeminal neuralgia or another cause of the patient’s symptoms.
Tic douloureux tests
Laboratory studies generally are not helpful in patients with typical symptoms of trigeminal neuralgia. Occasionally, TMJ or dental radiographs may be useful when TMJ syndrome or dental pain is in the differential diagnosis.
Magnetic resonance imaging (MRI) of the brain is useful to look for multiple sclerosis, tumors, or other causes of symptomatic trigeminal neuralgia, and it should be performed in the initial evaluation of all patients presenting with trigeminal neuralgia symptoms. One study found that specific clinical variables may be helpful in determining the likely utility of MRI, which may be useful in prioritizing MRI studies when there is limited MRI capacity 19. Some studies have indicated that MRI may predict surgery outcomes based on findings of neurovascular contact or the volume of the affected trigeminal nerve 20.
One recent study demonstrated that trigeminal reflex testing could distinguish classical from symptomatic trigeminal neuralgia with a sensitivity of 96 percent and a specificity of 93 percent 21. Trigeminal reflex testing involves electrical stimulation of the divisions of the trigeminal nerve and measurement of the response with standard electromyography apparatus. This testing is not readily available to most physicians, and its indications and clinical utility are still unclear.
Tic douloureux treatment
The management options for patients with trigeminal neuralgia depends on a variety of factors, including age, general health, disease severity, and the underlying cause. The decision should be taken after a thorough discussion with the patient and other doctors involved in the care of the patient.
Tic douloureux treatment usually starts with medications, and some people don’t need any additional treatment. However, over time, some people with the condition may stop responding to medications, or they may experience unpleasant side effects. For those people, injections or surgery provide other tic douloureux treatment options.
If your condition is due to another cause, such as multiple sclerosis, your doctor will treat the underlying condition.
Medications
The first-line treatment for patients with classic trigeminal neuralgia and idiopathic trigeminal neuralgia is pharmacologic therapy. To treat tic douloureux, your doctor usually will prescribe medications to lessen or block the pain signals sent to your brain.
- Anticonvulsants. Doctors usually prescribe carbamazepine (Tegretol, Carbatrol, others) for tic douloureux, and it’s been shown to be effective in treating the condition 5. Carbamazepine is usually started at a low dose and the dose is gradually increased until it controls the pain. Dosages used have ranged from 100 to 2,400 mg per day, with most patients responding to 200 to 800 mg per day in two or three divided doses. Carbamazepine controls pain for most people in the early stages of the disease. However, in some patients, the effectiveness of carbamazepine decreases over time. Possible side effects of carbamazepine include drowsiness, dizziness, double vision, and nausea. In patients with Asian ancestry, before starting carbamazepine, testing for HLA-B*15:02 allele is recommended, as its presence increases the risk of development of toxic epidermal necrolysis or Stevens-Johnson syndrome 22.
- Other anticonvulsant drugs that may be used to treat tic douloureux include oxcarbazepine (Trileptal), lamotrigine (Lamictal) and phenytoin (Dilantin, Phenytek). Oxcarbazepine is a newer drug and is being increasingly used as first-line therapy for trigeminal neuralgia in patients who do not respond to or who cannot tolerate carbamazepine. Possible side effects include double vision and dizziness. It can also cause hyponatremia. Oxcarbazepine should also be avoided in patients with HLA-B*15:02 allele.
- Other drugs, including clonazepam (Klonopin), gabapentin (Neurontin, Gralise, others), lamotrigine, phenytoin (Dilantin), and valproic acid (Depakene), also may be used 23, 24. If the anticonvulsant you’re using begins to lose effectiveness, your doctor may increase the dose or switch to another type. Side effects of anticonvulsants may include dizziness, confusion, drowsiness and nausea. Also, carbamazepine can trigger a serious drug reaction in some people, mainly those of Asian descent, so genetic testing may be recommended before you start carbamazepine.
- Newer drugs like eslicarbazepine, an active metabolite of oxcarbazepine, and the new Nav1.7 blocker, vixotrigine, are being explored for the pain relief in trigeminal neuralgia 5.
- Antispasmodic agents. Muscle-relaxing agents such as baclofen (Gablofen, Lioresal) may be used alone or in combination with carbamazepine. Baclofen in dosages of 10 to 80 mg daily has been shown to be useful 25. Side effects may include confusion, dizziness, sedation, nausea, drowsiness and dyspepsia.
- Botox injections 26. Small studies have shown that onabotulinumtoxinA (Botox) injections may reduce pain from tic douloureux for some patients, particularly the middle-aged and the elderly, who are no longer helped by medications or who cannot tolerate medical therapy due to their side effects 27. However, more research needs to be done before this treatment is widely used for this condition.
Patients with secondary trigeminal neuralgia also can respond well to pharmacotherapy. However, it is recommended to treat the underlying lesion or disease.
Surgery
Patients who are refractory to medical therapy can be considered for surgery.
Surgical options for tic douloureux include:
- Microvascular decompression 28. This is one of the most common procedures used to treat trigeminal neuralgia. Microvascular decompression is beneficial for patients with trigeminal neuralgia, where compression of the nerve root is the cause. This procedure involves relocating or removing blood vessels that are in contact with the trigeminal root to stop the nerve from malfunctioning. During microvascular decompression, your doctor makes an incision behind your ear on the side of your pain. Then, through a small hole in your skull, your surgeon moves any arteries that are in contact with the trigeminal nerve away from the nerve, and places a soft cushion between the nerve and the arteries. If a vein is compressing the nerve, your surgeon may remove it. Doctors may also cut part of the trigeminal nerve (neurectomy) during this procedure if arteries aren’t pressing on the nerve. Microvascular decompression can successfully eliminate or reduce pain most of the time, but pain can recur in some people. Microvascular decompression has some risks, including decreased hearing, facial weakness, facial numbness, a stroke or other complications. Most people who have this procedure have no facial numbness afterward. In some patients, this procedure can result in sustained pain relief for greater than 10 years. Though this is the most effective procedure, it is also the most invasive one. Some of the complications associated with it are decreased hearing, cerebellar hematoma, CSF leaks, infarction, and facial weakness. It is believed to be the most effective long term surgical treatment available currently for patients with trigeminal neuralgia 29.
- Brain stereotactic radiosurgery (Gamma knife) 30. In this procedure, a surgeon directs a focused dose of ionizing radiation to the root of your trigeminal nerve. This procedure uses radiation to damage the trigeminal nerve and reduce or eliminate pain. Relief occurs gradually and may take up to a month. Brain stereotactic radiosurgery is successful in eliminating pain for the majority of people. If pain recurs, the procedure can be repeated. As this is one of the least invasive procedures, it can be repeated in patients who have a recurrence of pain. Some of the associated complications can be facial sensory loss, facial numbness and paresthesias 31.
Other procedures may be used to treat tic douloureux, such as a rhizotomy. In a rhizotomy, your surgeon destroys nerve fibers to reduce pain, and this causes some facial numbness. Types of rhizotomy include 32:
- Glycerol injection. During this procedure, your doctor inserts a needle through your face and into an opening in the base of your skull. Your doctor guides the needle into the trigeminal cistern, a small sac of spinal fluid that surrounds the trigeminal nerve ganglion — where the trigeminal nerve divides into three branches — and part of its root. Then, your doctor will inject a small amount of sterile glycerol, which damages the trigeminal nerve and blocks pain signals. This procedure often relieves pain. However, some people have a later recurrence of pain, and many experience facial numbness or tingling.
- Balloon compression. In balloon compression, your doctor inserts a hollow needle through your face and guides it to a part of your trigeminal nerve that goes through the base of your skull. Then, your doctor threads a thin, flexible tube (catheter) with a balloon on the end through the needle. Your doctor inflates the balloon with enough pressure to damage the trigeminal nerve and block pain signals. Balloon compression successfully controls pain in most people, at least for a period of time. Most people undergoing this procedure experience at least some transient facial numbness.
- Radiofrequency thermal lesioning. This procedure selectively destroys nerve fibers associated with pain. While you’re sedated, your surgeon inserts a hollow needle through your face and guides it to a part of the trigeminal nerve that goes through an opening at the base of your skull. Once the needle is positioned, your surgeon will briefly wake you from sedation. Your surgeon inserts an electrode through the needle and sends a mild electrical current through the tip of the electrode. You’ll be asked to indicate when and where you feel tingling. When your neurosurgeon locates the part of the nerve involved in your pain, you’re returned to sedation. Then the electrode is heated until it damages the nerve fibers, creating an area of injury (lesion). If your pain isn’t eliminated, your doctor may create additional lesions. Radiofrequency thermal lesioning usually results in some temporary facial numbness after the procedure. Pain may return after three to four years.
- Peripheral neurectomy and nerve block. The neurectomy can be performed on peripheral branches of trigeminal nerve like the supraorbital, infraorbital, lingual, and the alveolar nerves 33. This can be accomplished by alcohol injection, incision, cryotherapy, or radiofrequency lesioning. Peripheral neurectomy can be safe in elderly patients in remote and rural areas, where neurosurgical facilities are not readily available 34. However, the evidence regarding these peripheral techniques for trigeminal neuralgia is inconclusive.
Avoiding triggers
Identifying triggers and avoiding them can also help. The painful attacks of trigeminal neuralgia can sometimes be brought on, or made worse, by certain triggers, so it may help to avoid these triggers if possible.
For example, if your pain is triggered by wind, it may help to wear a scarf wrapped around your face in windy weather. A transparent dome-shaped umbrella can also protect your face from the weather.
If your pain is triggered by a draught in a room, avoid sitting near open windows or the source of air conditioning.
Avoid hot, spicy or cold food or drink if these seem to trigger your pain. Using a straw to drink warm or cold drinks may also help prevent the liquid coming into contact with painful areas of your mouth.
It’s important to eat nourishing meals, so consider eating mushy foods or liquidising your meals if you’re having difficulty chewing.
Certain foods seem to trigger attacks in some people, so you may want to consider avoiding things such as caffeine, citrus fruits and bananas.
Alternative medicine
Alternative treatments for tic douloureux generally haven’t been as well-studied as medications or surgical procedures, so there’s often little evidence to support their use. However, some people have found improvement with treatments, such as acupuncture, biofeedback, chiropractic, and vitamin or nutritional therapy. Be sure to check with your doctor before trying an alternative treatment because it may interact with your other treatments.
Tic douloureux prognosis
Trigeminal neuralgia is not a life-threatening condition and the course is variable 1. Correct diagnosis and proper management can be beneficial to the patients and leads to a good prognosis. After an initial attack, it’s possible for the pain to improve or even disappear altogether for several months or years at a time (remission), although these periods tend to get shorter with time. Thereafter the attacks may become more frequent, more easily triggered, disabling, and may require long-term medication. Some people may then develop a more continuous aching, throbbing or burning sensation, sometimes accompanied by the sharp attacks. Thus, trigeminal neuralgia course is typically one of clusters of attacks that wax and wane in frequency. Exacerbations most commonly occur in the fall and spring.
Living with trigeminal neuralgia can be very difficult. It can have a significant impact on a person’s quality of life, resulting in problems such as weight loss, isolation and depression.
Because of the variety of treatment options available, having tic douloureux or trigeminal neuralgia doesn’t necessarily mean you’re doomed to a life of pain. Doctors usually can effectively manage trigeminal neuralgia with medications, injections or surgery.
Among the best clinical predictors of a symptomatic form are sensory deficits upon examination and a bilateral distribution of symptoms (but the absence thereof is not a negative predictor). Young age is a moderate predictor, but a fair degree of overlap exists. Lack of therapeutic response and V1 distribution are poor predictors.
Although trigeminal neuralgia is not associated with a shortened life, the morbidity associated with the chronic and recurrent facial pain can be considerable if the condition is not controlled adequately. This condition may evolve into a chronic pain syndrome, and patients may suffer from depression and related loss of daily functioning. Individuals may choose to limit activities that precipitate pain, such as chewing, possibly losing weight in extreme circumstances. In addition, the severity of the pain may lead to suicide.
Living with tic douloureux
Living with tic douloureux can be very difficult and your quality of life can be significantly affected. Trigeminal neuralgia may affect your interaction with friends and family, your productivity at work, and the overall quality of your life.
You may feel like avoiding activities such as washing, shaving or eating so you do not trigger the pain, and the fear of pain may mean you avoid social activities.
However, it’s important to try to live a normal life and be aware that becoming undernourished or dehydrated can make the pain worse.
The emotional strain of living with repeated episodes of pain can lead to psychological problems, such as depression. During periods of extreme pain some people may even consider suicide. Even when pain-free, you may live in fear of the pain returning.
You may find encouragement and understanding in a support group. Group members often know about the latest treatments and tend to share their own experiences. If you’re interested, your doctor may be able to recommend a group in your area.
How to manage chronic pain
Exercise
Choose an exercise that won’t put too much strain on yourself.
Good options include:
- walking
- swimming
- using an exercise bike
- dancing, yoga or pilates
- most daily activities and hobbies
Activity and stretching needs to become part of your lifestyle so you routinely do exercise a little and often.
Try to be active every day instead of only on the good days when you’re not in so much pain. This may reduce the number of bad days you have and help you feel more in control.
But try to avoid overdoing it on good days and paying for this by having more bad days.
Go to work despite the pain
It’s important to try to stay in work even though you’re in pain. Research shows that people become less active and more depressed when they don’t work. Being at work will distract you from the pain, and in most cases, won’t make your pain worse.
Talk to your supervisor or boss about the parts of your job that may be difficult to begin with, but stress that you want to be at work.
If you have to stay off work for a while, try to get back as soon as possible.
If you have been off work for 4 to 6 weeks, plan with your doctor, therapist or employer how and when you can return.
You could go back to work gradually. For instance, you might start with 1 day a week and gradually increase the time you spend at work.
You could also agree changes to your job or pattern of work if it helps – a health and safety rep or occupational health department may be useful here.
Physical therapy
Pain experts often recommend a short course of physical therapy. This helps you to move better, relieves your pain, and makes daily tasks and activities like walking, going up stairs or getting in and out of bed easier.
Physical therapy for persistent pain can involve manipulation, stretching exercises and pain-relief exercises.
Physical therapy is usually delivered by a physiotherapist, chiropractor or osteopath, or in some cases, an occupational therapist.
Physiotherapists can give you advice on the right type of exercise and activity. Occupational therapists can support you with environmental changes that can help you remain in work and function better at home.
If you have physical therapy, you should begin to feel the benefits after a few sessions.
- Shankar Kikkeri N, Nagalli S. Trigeminal Neuralgia. [Updated 2020 Jul 5]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK554486[↩][↩][↩]
- Yadav YR, Nishtha Y, Sonjjay P, Vijay P, Shailendra R, Yatin K. Trigeminal Neuralgia. Asian J Neurosurg. 2017 Oct-Dec;12(4):585-597.[↩][↩]
- Mueller D, Obermann M, Yoon MS, Poitz F, Hansen N, Slomke MA, Dommes P, Gizewski E, Diener HC, Katsarava Z. Prevalence of trigeminal neuralgia and persistent idiopathic facial pain: a population-based study. Cephalalgia. 2011 Nov;31(15):1542-8.[↩]
- Katusic S, Beard CM, Bergstralh E, Kurland LT. Incidence and clinical features of trigeminal neuralgia, Rochester, Minnesota, 1945–1984. Ann Neurol. 1990;27(1):89–95.[↩][↩]
- Gambeta E, Chichorro JG, Zamponi GW. Trigeminal neuralgia: An overview from pathophysiology to pharmacological treatments. Mol Pain. 2020 Jan-Dec;16:1744806920901890[↩][↩][↩]
- Bašić Kes V, Zadro Matovina L. Accommodation to Diagnosis of Trigeminal Neuralgia. Acta Clin Croat. 2017 Mar;56(1):157-161.[↩]
- Truini A, Prosperini L, Calistri V, Fiorelli M, Pozzilli C, Millefiorini E, Frontoni M, Cortese A, Caramia F, Cruccu G. A dual concurrent mechanism explains trigeminal neuralgia in patients with multiple sclerosis. Neurology. 2016 May 31;86(22):2094-9.[↩]
- Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. Cephalalgia. 2018 Jan;38(1):1-211.[↩][↩][↩][↩][↩]
- Zakrzewska JM, Linskey ME. Trigeminal neuralgia. BMJ. 2014 Feb 17;348:g474.[↩]
- Maarbjerg S, Gozalov A, Olesen J, Bendtsen L. Trigeminal neuralgia–a prospective systematic study of clinical characteristics in 158 patients. Headache. 2014 Nov-Dec;54(10):1574-82.[↩][↩]
- Di Stefano G, Maarbjerg S, Nurmikko T, Truini A, Cruccu G. Triggering trigeminal neuralgia. Cephalalgia. 2018 May;38(6):1049-1056.[↩]
- Maarbjerg S, Di Stefano G, Bendtsen L, Cruccu G. Trigeminal neuralgia – diagnosis and treatment. Cephalalgia. 2017 Jun;37(7):648-657.[↩]
- Desouza DD, Moayedi M, Chen DQ, Davis KD, Hodaie M. Sensorimotor and Pain Modulation Brain Abnormalities in Trigeminal Neuralgia: A Paroxysmal, Sensory-Triggered Neuropathic Pain. PLoS ONE. 2013;8(6):e66340.[↩]
- Thomas KL, Vilensky JA. The anatomy of vascular compression in trigeminal neuralgia. Clin Anat. 2014 Jan;27(1):89-93.[↩]
- Jia DZ, Li G. Bioresonance hypothesis: a new mechanism on the pathogenesis of trigeminal neuralgia. Med. Hypotheses. 2010 Mar;74(3):505-7.[↩]
- Borges A, Casselman J. Imaging the trigeminal nerve. Eur J Radiol. 2010 May;74(2):323-40.[↩]
- Tai AX, Nayar VV. Update on Trigeminal Neuralgia. Curr Treat Options Neurol. 2019 Jul 31;21(9):42.[↩]
- Cruccu G, Biasiotta A, Galeotti F, et al. Diagnosis of trigeminal neuralgia: a new appraisal based on clinical and neurophysiological findings. In: Cruccu G, Hallett M, eds. Brainstem Function and Dysfunction. Amsterdam, the Netherlands: Elsevier; 2006:171–186.[↩]
- Majoie CB, Hulsmans FJ, Castelijns JA, et al. Symptoms and signs related to the trigeminal nerve: diagnostic yield of MR imaging. Radiology. 1998;209(2):557–562.[↩]
- Kuncz A, Vörös E, Barzó P, et al. Comparison of clinical symptoms and magnetic resonance angiographic (MRA) results in patients with trigeminal neuralgia and persistent idiopathic facial pain. Medium-term outcome after microvascular decompression of cases with positive MRA findings. Cephalalgia. 2006;26(3):266–276.[↩]
- Cruccu G, Biasotta A, Galeotti F, Ianetti GD, Truini A, Gronseth G. Diagnostic accuracy of trigeminal reflex testing in trigeminal neuralgia. Neurology. 2006;66(1):139–141.[↩]
- Dean L. Carbamazepine Therapy and HLA Genotype. In: Pratt VM, McLeod HL, Rubinstein WS, Scott SA, Dean LC, Kattman BL, Malheiro AJ, editors. Medical Genetics Summaries [Internet]. National Center for Biotechnology Information (US); Bethesda (MD): Oct 14, 2015.[↩]
- Scrivani SJ, Mathews ES, Maciewicz RJ. Trigeminal neuralgia. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005;100(5):527–538.[↩]
- Cheshire WP. Defining the role for gabapentin in the treatment of trigeminal neuralgia: a retrospective study. J Pain. 2002;3(2):137–142.[↩]
- Fromm GH, Terrence CF, Chattha AS. Baclofen in the treatment of trigeminal neuralgia: double-blind study and long-term follow-up Ann Neurol. 1984;15(3):240–244.[↩]
- Burmeister J, Holle D, Bock E, Ose C, Diener HC, Obermann M. Botulinum neurotoxin type A in the treatment of classical Trigeminal Neuralgia (BoTN): study protocol for a randomized controlled trial. Trials. 2015 Dec 03;16:550[↩]
- Wu S, Lian Y, Zhang H, Chen Y, Wu C, Li S, Zheng Y, Wang Y, Cheng W, Huang Z. Botulinum Toxin Type A for refractory trigeminal neuralgia in older patients: a better therapeutic effect. J Pain Res. 2019;12:2177-2186.[↩]
- Wei Y, Pu C, Li N, Cai Y, Shang H, Zhao W. Long-Term Therapeutic Effect of Microvascular Decompression for Trigeminal Neuralgia: Kaplan-Meier Analysis in a Consecutive Series of 425 Patients. Turk Neurosurg. 2018;28(1):88-93.[↩]
- Shi J, Qian Y, Han W, Dong B, Mao Y, Cao J, Guan W, Zhou Q. Risk Factors for Outcomes After Microvascular Decompression for Trigeminal Neuralgia. World Neurosurg. 2020 Apr;136:e559-e566.[↩]
- Taich ZJ, Goetsch SJ, Monaco E, Carter BS, Ott K, Alksne JF, Chen CC. Stereotactic Radiosurgery Treatment of Trigeminal Neuralgia: Clinical Outcomes and Prognostic Factors. World Neurosurg. 2016 Jun;90:604-612.e11.[↩]
- Baschnagel AM, Cartier JL, Dreyer J, Chen PY, Pieper DR, Olson RE, Krauss DJ, Maitz AH, Grills IS. Trigeminal neuralgia pain relief after gamma knife stereotactic radiosurgery. Clin Neurol Neurosurg. 2014 Feb;117:107-111.[↩]
- Staudt MD, Joswig H, Pickett GE, MacDougall KW, Parrent AG. Percutaneous glycerol rhizotomy for trigeminal neuralgia in patients with multiple sclerosis: a long-term retrospective cohort study. J. Neurosurg. 2019 Apr 12;:1-9.[↩]
- Yuvaraj V, Krishnan B, Therese BA, Balaji TS. Efficacy of Neurectomy of Peripheral Branches of the Trigeminal Nerve in Trigeminal Neuralgia: A Critical Review of the Literature. J Maxillofac Oral Surg. 2019 Mar;18(1):15-22.[↩]
- Ali FM, Prasant M, Pai D, Aher VA, Kar S, Safiya T. Peripheral neurectomies: A treatment option for trigeminal neuralgia in rural practice. J Neurosci Rural Pract. 2012 May;3(2):152-7.[↩]





{kind=link}