What is a urethra
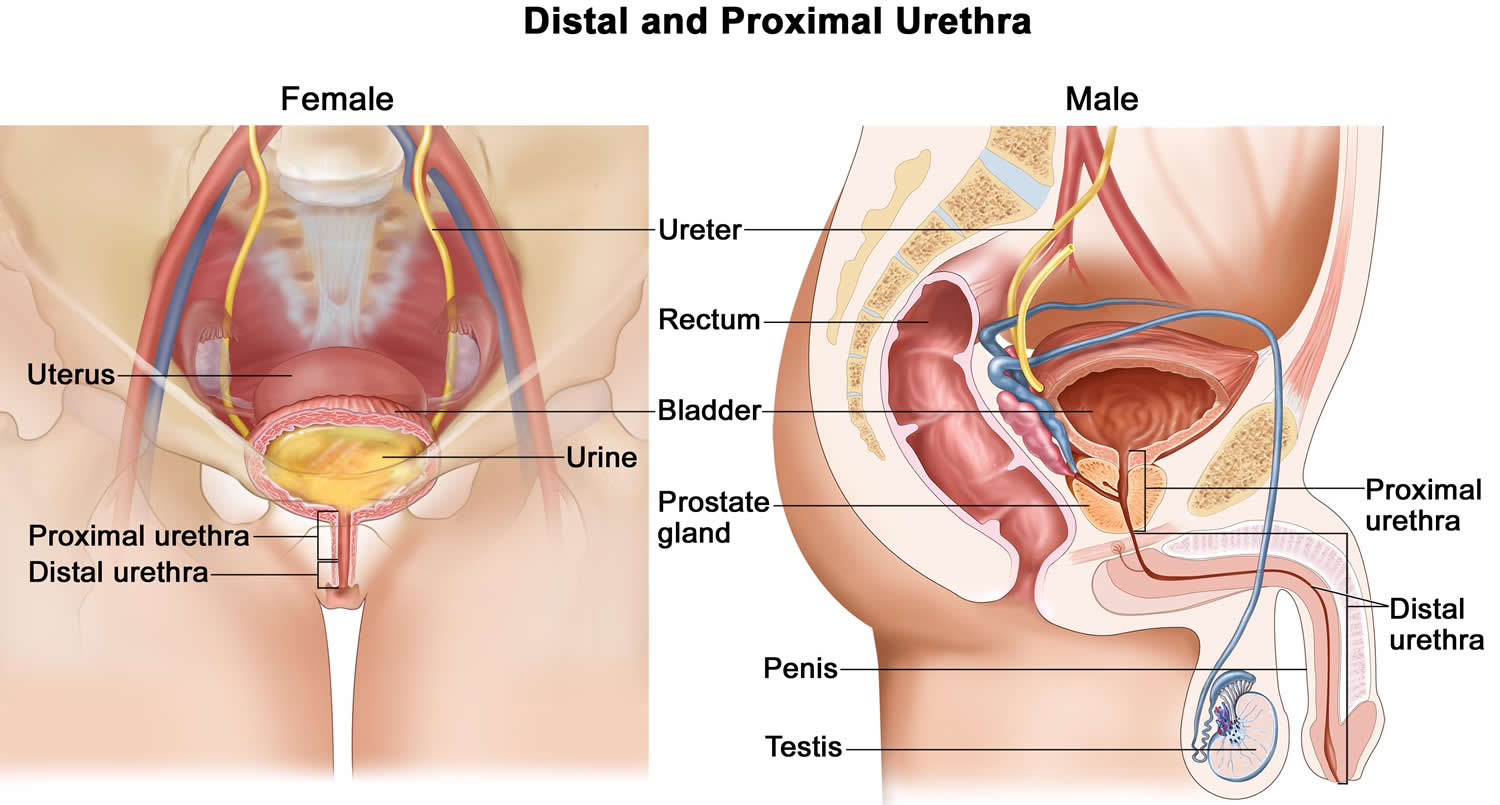
The urethra is a thin-walled tube that drains urine from the bladder. In both males and females, the urethra is the terminal portion of the urinary system and the passageway for discharging urine from the body. In males, it discharges semen (fluid that contains sperm) as well (Figure 1 and 2). This tube consists of smooth muscle and an inner mucosa.
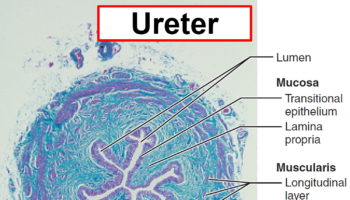
In males, the muscle layer becomes very thin toward the distal end of the urethra. The lining epithelium changes from a transitional epithelium near the bladder to a stratified and pseudostratified columnar epithelium in mid-urethra (sparse in females), and then to a stratified squamous epithelium near the end of the urethra.
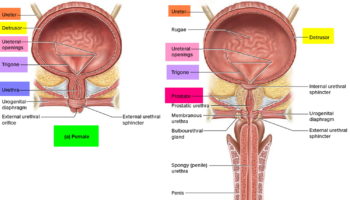
At the bladder-urethra junction, a thickening of the detrusor forms the internal urethral sphincter. This is an involuntary sphincter of smooth muscle that keeps the urethra closed when urine is not being passed and prevents dribbling of urine between voidings. A second sphincter, the external urethral sphincter, surrounds the urethra within the sheet of muscle called the urogenital diaphragm. This external sphincter is a skeletal muscle used to inhibit urination voluntarily until the proper time. The levator ani muscle of the pelvic floor also serves as a voluntary constrictor of the urethra.
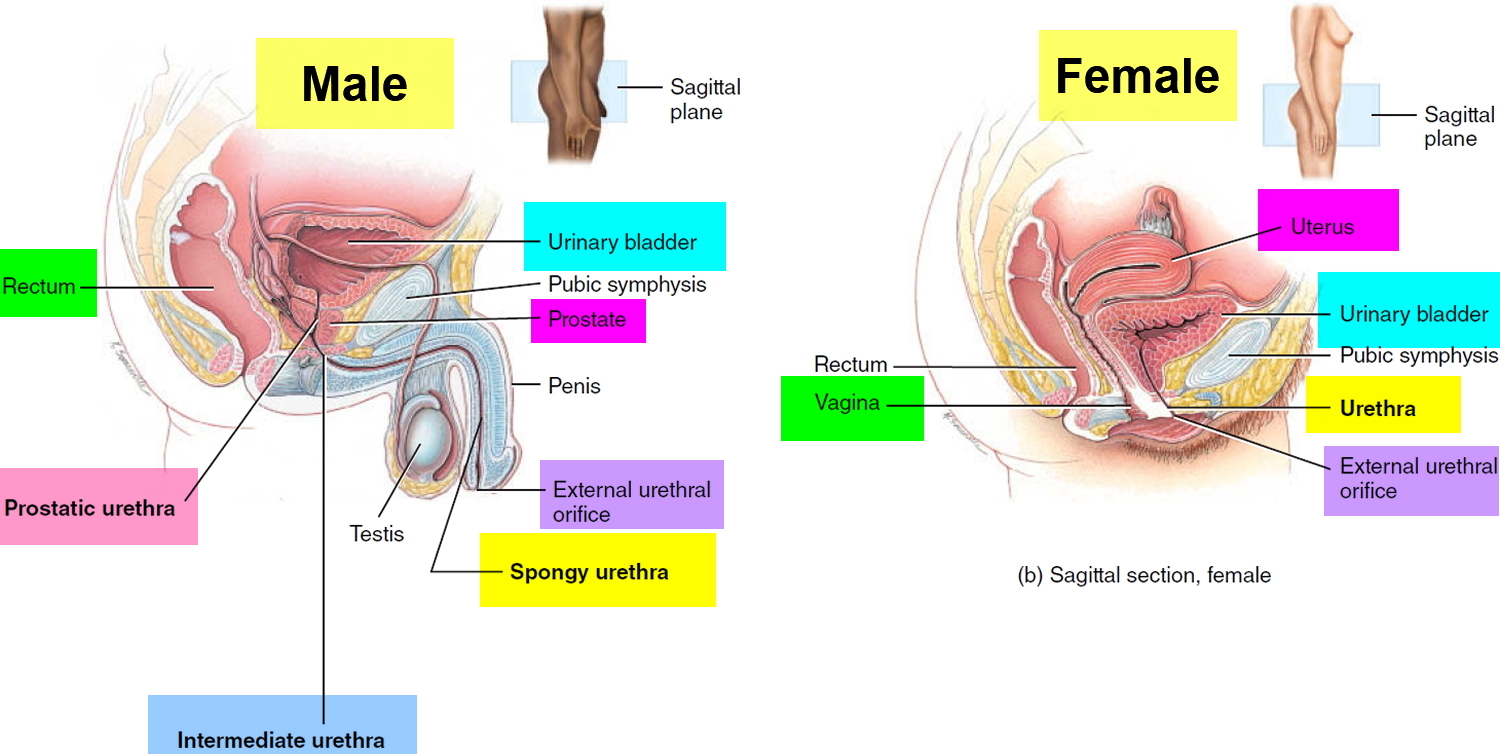
The length and functions of the urethra differ in the two sexes. In females, the urethra is just 3–4 cm (1.5 inches) long and is bound to the anterior wall of the vagina by connective tissue (see Figure 2). It opens to the outside at the external urethral orifice, a small, often difficult-to-locate opening that lies anterior to the vaginal opening and posterior to the clitoris.
Male urethra
In males, the urethra is about 20 cm long (8 inches) and has three named regions: the prostatic urethra, which is about 2.5 cm long and runs in the prostate; the intermediate part of the urethra, or membranous urethra, which runs for about 2.5 cm through the membrane like urogenital diaphragm; and the spongy urethra, which is about 15 cm long, passes through the entire penis, and opens at the tip of the penis via the external urethral orifice. The male urethra carries ejaculating semen as well as urine (although not simultaneously) from the body.
The muscularis of the prostatic urethra is composed of mostly circular smooth muscle fibers superficial to the lamina propria; these circular fibers help form the internal urethral sphincter of the urinary bladder. The muscularis of the intermediate (membranous) urethra consists of circularly arranged skeletal muscle fibers of the deep muscles of the perineum that help form the external urethral sphincter of the urinary bladder.
Several glands and other structures associated with reproduction deliver their contents into the male urethra (see Figure 1). The prostatic urethra contains the openings of (1) ducts that transport secretions from the prostate and (2) the seminal vesicles and ductus (vas) deferens, which deliver sperm into the urethra and provide secretions that both neutralize the acidity of the female reproductive tract and contribute to sperm motility and viability. The openings of the ducts of the bulbourethral glands or Cowper’s glands empty into the spongy urethra. They deliver an alkaline substance prior to ejaculation that neutralizes the acidity of the urethra. The glands also secrete mucus, which lubricates the end of the penis during sexual arousal. Throughout the urethra, but especially in the spongy urethra, the openings of the ducts of urethral glands or Littré glands discharge mucus during sexual arousal and ejaculation.
Female urethra
In females, the urethra lies directly posterior to the pubic symphysis; is directed obliquely, inferiorly, and anteriorly; and has a length of 4 cm (1.5 in.). The opening of the urethra to the exterior, the external urethral orifice, is located between the clitoris and the vaginal opening. The wall of the female urethra consists of a deep mucosa and a superficial muscularis. The mucosa is a mucous membrane composed of epithelium and lamina propria (areolar connective tissue with elastic fibers and a plexus of veins). Near the urinary bladder, the mucosa contains transitional epithelium that is continuous with that of the urinary bladder; near the external urethral orifice, the epithelium is nonkeratinized stratified squamous epithelium. Between these areas, the mucosa contains stratified columnar or pseudostratified columnar epithelium. The muscularis consists of circularly arranged smooth muscle fibers and is continuous with that of the urinary bladder.
Figure 1. Male and Female Urethra
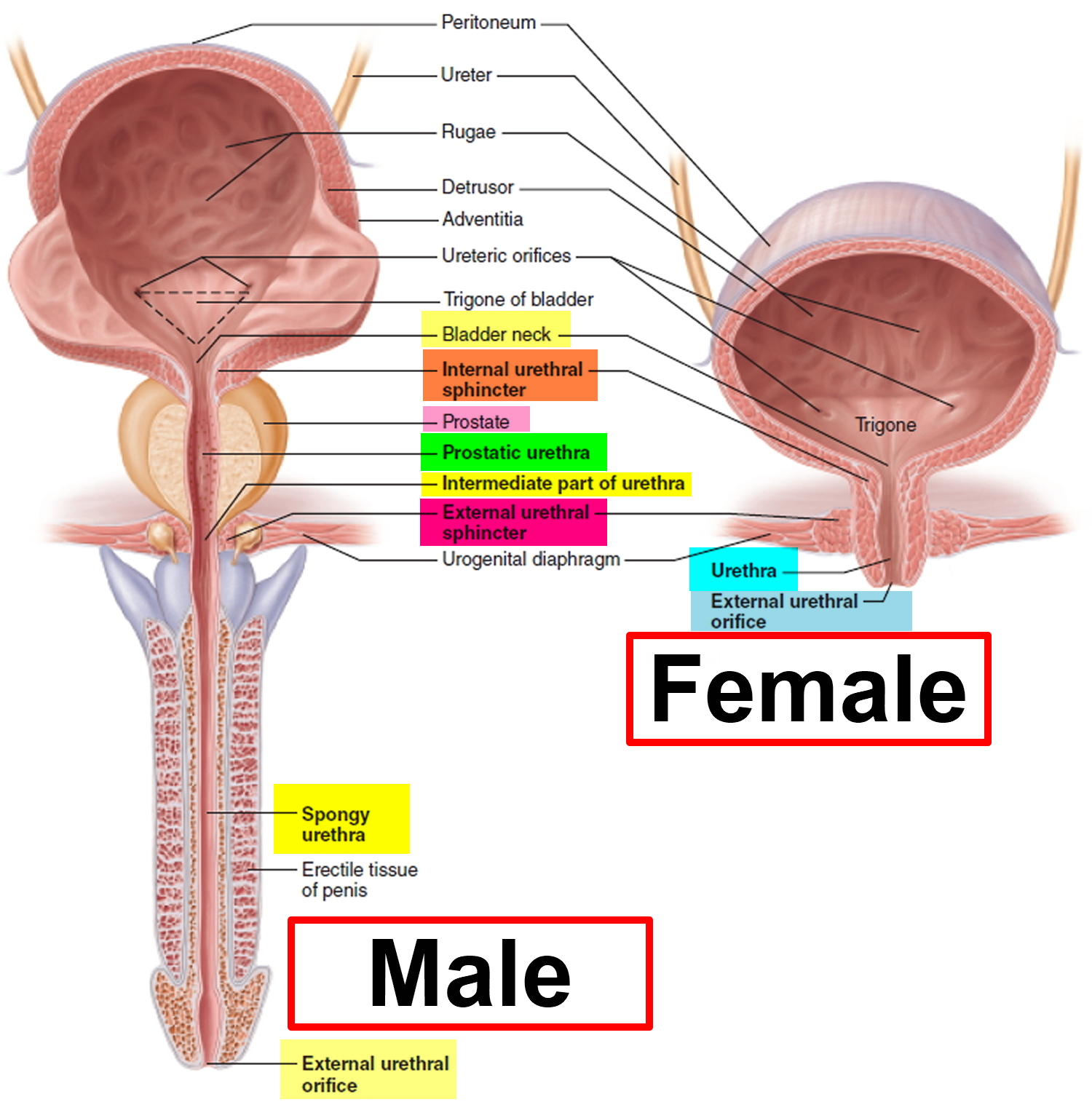
Figure 2. Male and Female Urethra – Location
Urethra function
Drainage tube that transports stored urine from body.
And in men the urethra also carries ejaculating semen as well as urine (although not simultaneously) from the body.
Burning, swollen and itchy urethra
Urethritis is infection (swelling and irritation) of the urethra 1.
Bacteria, including those that are sexually transmitted, are the most common cause of urethritis.
Symptoms include pain while urinating, a frequent or urgent need to urinate, and sometimes a discharge.
Risks for urethritis include 2:
- Being a female
- Being male, ages 20 to 35
- Having many sexual partners
- High-risk sexual behavior (such as anal sex without a condom)
- History of sexually transmitted diseases
Antibiotics are usually given to treat the infection.
Causes of Urethritis
Urethritis may be caused by bacteria, fungi, or viruses (for example, herpes simplex virus).
Sexually transmitted diseases are common causes of urethritis. Organisms—such as Neisseria gonorrhoeae, which causes gonorrhea—can spread to the urethra during sexual intercourse with an infected partner. Chlamydia and the herpes simplex virus are also commonly transmitted sexually and can cause urethritis. When men develop urethritis, the gonorrheal organism is a very common cause. Although this organism may infect the urethra in women, the vagina, cervix, uterus, ovaries, and fallopian tubes are more likely to be infected. Trichomonas, a type of microscopic parasite, also causes urethritis in men. Urethritis may also be caused by the bacteria that commonly cause other urinary tract infections, such as Escherichia coli.
Symptoms of Urethritis
In both men and women, there is usually pain during urination and a frequent, urgent need to urinate. Sometimes people have no symptoms. In men, when gonorrhea or chlamydia is the cause, there is usually a discharge from the urethra. The discharge is often yellowish green and thick when the gonococcal organism is involved and may be clear and thinner when other organisms are involved. In women, discharge is less common.
In men:
- Blood in the urine or semen
- Burning pain while urinating (dysuria)
- Discharge from penis
- Fever (rare)
- Frequent or urgent urination
- Itching, tenderness, or swelling in penis
- Enlarged lymph nodes in the groin area
- Pain with intercourse or ejaculation
In women:
- Abdominal pain
- Burning pain while urinating
- Fever and chills
- Frequent or urgent urination
- Pelvic pain
- Pain with intercourse
- Vaginal discharge
Other disorders that cause pain during urination include bladder infection and vaginitis (inflammation of the vagina).
Complications of Urethritis
Infections of the urethra that are not treated or are inadequately treated may cause a narrowing (stricture) of the urethra. A stricture increases the risk that infections will develop in the bladder or the kidneys. Untreated gonorrhea rarely leads to an accumulation of pus (abscess) around the urethra. An abscess can cause outpouchings from the urethral wall (urethral diverticula), which can also become infected. If the abscess perforates the skin, the vagina, or the rectum, urine may flow through a newly created abnormal connection (urethral fistula).
Diagnosis of Urethritis
The health care provider will examine you.
In men, the exam will include the abdomen, bladder area, penis, and scrotum. The physical exam may show:
- Discharge from the penis
- Tender and enlarged lymph nodes in the groin area
- Tender and swollen penis
A digital rectal exam will also be performed.
Women will have abdominal and pelvic exams. The provider will check for:
- Discharge from the urethra
- Tenderness of the lower abdomen
- Tenderness of the urethra
Your provider may look into your bladder using a tube with a camera on the end. This is called cystoscopy.
The following tests may be done:
- Complete blood count (CBC)
- C-reactive protein test
- Pelvic ultrasound (women only)
- Pregnancy test (women only)
- Urinalysis and urine cultures
- Tests for gonorrhea, chlamydia, and other sexually transmitted illnesses (STI)
- Urethral swab
Doctors can usually make a diagnosis of urethritis based on the symptoms and examination. A sample of the discharge, if present, is collected by inserting a soft-tipped swab into the end of the urethra. The urethral swab is then sent to a laboratory for analysis so that the infecting organism can be identified.
Treatment of Urethritis
The goals of treatment are to 3:
- Get rid of the cause of infection
- Improve symptoms
- Prevent the spread of infection
If you have a bacterial infection, you will be given antibiotics. Antivirals for herpes simplex.
You may take pain relievers, urinary pain reliever along with antibiotics.
People with urethritis who are being treated should avoid sex, or use condoms during sex. Your sexual partner must also be treated if the condition is caused by an infection.
Urethritis caused by trauma or chemical irritants is treated by avoiding the source of injury or irritation.
Urethritis that does not clear up after antibiotic treatment and lasts for at least 6 weeks is called chronic urethritis. Different antibiotics may be used to treat this problem.
For sexually transmitted infections, treatment of partners with antibiotics.
Sexually transmitted diseases that cause urethritis may be prevented by using a condom.
Treatment depends on the cause of the infection. However, identification of the organism causing urethritis can take days. Thus, doctors usually begin treatment with antibiotics that cure the most common causes. For sexually active men, treatment is usually with a ceftriaxone injection for gonorrhea plus oral azithromycin or oral doxycycline for chlamydia 4. If tests exclude the possibility of gonorrhea and chlamydia, trimethoprim/sulfamethoxazole or a fluoroquinolone antibiotic (such as ciprofloxacin) may be used. Women may be treated as if they had cystitis. An antiviral drug, such as acyclovir, may be needed for a herpes simplex infection. If the cause is suspected to be a sexually transmitted disease, the person’s sex partners should be evaluated for treatment. Men who receive a diagnosis of urethritis should be tested for HIV and syphilis.
Prevention of urethritis
Things you can do to help avoid urethritis include:
- Keep the area around the opening of the urethra clean.
- Follow safer sex practices. Have one sexual partner only (monogamy) and use condoms.
Outlook (Prognosis) for urethritis
With the correct diagnosis and treatment, urethritis most often clears up without further problems.
However, urethritis can lead to long-term damage to the urethra and scar tissue called urethral stricture. It can also cause damage to other urinary organs in both men and women. In women, the infection could lead to fertility problems if it spreads to the pelvis.
Possible Complications of urethritis
Men with urethritis are at risk for the following:
- Bladder infection (cystitis)
- Epididymitis
- Infection in the testicles (orchitis)
- Prostate infection (prostatitis)
After a severe infection, the urethra may become scarred and then narrowed.
Women with urethritis are at risk for the following:
- Bladder infection (cystitis)
- Cervicitis
- Pelvic inflammatory disease (PID — an infection of the uterus lining, uterine (fallopian) tubes, or ovaries)
What is Narrow urethra
Narrow urethra also called urethral stricture, involves scarring that narrows the urethra tube that carries urine out of your body 5. A stricture restricts the flow of urine from the bladder and can cause a variety of medical problems in the urinary tract, including inflammation or infection.
Congenital (present at birth) urethral stricture may manifest similarly to urethral valves and may be diagnosed by prenatal ultrasonography, or postnatally by symptoms and signs of outlet obstruction or patent urachus and is confirmed by retrograde urethrography. Initial management is often with endoscopic urethrotomy, although open urethroplasty may be necessary.
Scar tissue, which can narrow the urethra, can be due to:
- A medical procedure that involves inserting an instrument, such as an endoscope, into the urethra
- Intermittent or long-term use of a tube inserted through the urethra to drain the bladder (catheter)
- Trauma or injury to the urethra or pelvis
- An enlarged prostate or previous surgery to remove or reduce an enlarged prostate gland
- Cancer of the urethra or prostate
- Sexually transmitted infections
- Radiation therapy
Urethral stricture is much more common in males than in females. Often the cause is unknown.
Signs and symptoms of urethral stricture include:
- Decreased urine stream
- Incomplete bladder emptying
- Spraying of the urine stream
- Difficulty, straining or pain when urinating
- Increased urge to urinate or more-frequent urination
- Urinary tract infection.
Urethral valves
In boys, folds in the posterior urethra may act as valves impairing urine flow. Urologic sequelae of urethral valves include urinary hesitancy, decreased urinary stream, urinary tract infection (UTI), overflow incontinence, myogenic bladder malfunction, vesicoureteral reflux, upper urinary tract damage, and renal insufficiency. The valves occasionally occur with a patent urachus. Because fetal urine excretion contributes to the amniotic fluid, severe urethral obstruction can cause decreased amniotic fluid (oligohydramnios), which can cause lung hypoplasia and consequent pulmonary hypertension, pulmonary hypoplasia, and/or respiratory failure. Pulmonary hypertension can then cause systemic hypertension. Severe cases may result in perinatal demise.
Diagnosis is often made by findings on routine prenatal ultrasonography, including severe bilateral hydroureteronephrosis or oligohydramnios. Cases suspected postnatally (often because of history of an abnormal urine stream) are confirmed by immediate voiding cystourethrography.
Surgery (usually via endoscopy) is done at time of diagnosis to prevent progressive renal deterioration.
A much less common anomaly, diverticulum of the anterior urethra, may act as a valve (anterior urethral valve) and is also treated endoscopically.
Urethral Dilation
Urethral dilation is used to treat the following:
- Urethral strictures
- Meatal stenosis
Contraindications include untreated infection and bleeding diathesis. Dilation can be done using various techniques, such as by inflating a balloon or by inserting progressively larger instruments called sounds. Usually, lidocaine gel, a local anesthetic, is first introduced into the penis. Typically, after dilation a urethral catheter is left in place temporarily to facilitate healing. Sometimes patients are asked to insert an instrument into their own urethra periodically at home.
Urethra stretching
Urethral dilatation has been advocated as empirical treatment for adult women with lower urinary tract complaints for long time. The discovery of a distal urethral ring by Lyon and associates led to the hypothesis that urethral stenosis was the cause of recurrent urinary tract infections (UTIs) and dysfunctional voiding in girls 6. It was postulated that rupture of this ring by dilatation would relieve the obstruction. Kerr and associates decided on cutting this contraction ring with the otis urethrotome rather than dilating it with sounds 7. At the same time, they extended this procedure to include adult female patients.
Although reviewing the literature reveals little solid evidence regarding the theoretical basis of this practice, several reports suggest that urologists are still practising urethral dilatation as treatment for women with lower urinary tract complaints that are not efficiently managed by other means 8.
Urethral stenosis is the most common chosen indication (97%) for urethral dilatation. Lower urinary tract symptoms with inadequate bladder emptying was the second most common indication (72%). Some 65% of urologists chose to use dilatation for urethral syndrome, 49% for idiopathic acute urinary retention when trail without a catheter fails, while 35% used it for chronic urinary retention. The majority of urologists (69%) indicated that less than 25% of their patients had evidence of stenosis. Of urologists, 55% believed that less than half of their patients experienced long-term improvement, while 45% thought that the improvement was experienced in more than 50% of cases.
Overall, 54% reported that repeated dilatation was required in less than 25%, while one-third of urologists considered repeating the procedure in up to half of the cases. Most urologists perform this procedure only under general anaesthesia (90%), while 7% always use local anaesthesia; 18% perform dilatation under either local or general anaesthesia depending on patient’s condition. Three consultants said that spinal anaesthesia is one of their options, and one consultant used peri-urethral infiltration. Most urologists tend to dilate up to 32 F (45%), while only 9% dilated beyond 36 F. Four consultants used different sizes of Hegar dilators.
There was a lack of uniformity about the size to which urologists dilated the urethra, although it appears that most dilated to 32 Fr. This is consistent with previous studies that showed a surprising dearth of information about the range of urethral calibre that is found in normal healthy women. The tendency to repeat dilatation among some urologists might suggest that urethral dilatation is a small price to pay for a possible relief of symptoms, where there are few, if any, sequelae.
In conclusion, there is little scientific data to support the empirical use of urethral dilatation in women 8. Nonetheless, despite the lack of such data, many urologists continue to find it a useful tool in approaching women with lower urinary tract complaints. Why the perception that urethral dilatation is an effective procedure exists among some urologists and is absent among others is a matter of debate. Obviously, differences in training and personal experience will affect an individual’s practice patterns. Prospective studies with readily definable outcome measures are needed. Until that is done, the presumed beneficial effect of urethral dilatation will remain merely anecdotal 8.
Benign prostatic hyperplasia
Benign prostatic hyperplasia—also called BPH—is a condition in men in which the prostate gland is enlarged and not cancerous. Benign prostatic hyperplasia is also called benign prostatic hypertrophy or benign prostatic obstruction.
Severe benign prostatic hypertrophy can cause serious problems over time, such as urinary tract infections, and bladder or kidney damage. If it is found early, you are less likely to develop these problems.
The complications of benign prostatic hyperplasia may include 9:
- acute urinary retention
- chronic, or long lasting, urinary retention
- blood in the urine
- urinary tract infections (UTIs)
- bladder damage
- kidney damage
- bladder stones
Most men with benign prostatic hyperplasia do not develop these complications. However, kidney damage in particular can be a serious health threat when it occurs.
A health care provider treats benign prostatic hyperplasia based on the severity of symptoms, how much the symptoms affect a man’s daily life, and a man’s preferences.
Men may not need treatment for a mildly enlarged prostate unless their symptoms are bothersome and affecting their quality of life. In these cases, instead of treatment, a urologist may recommend regular checkups. If benign prostatic hyperplasia symptoms become bothersome or present a health risk, a urologist most often recommends treatment.
Prostatic stent insertion. This procedure involves a urologist inserting a small device called a prostatic stent through the urethra to the area narrowed by the enlarged prostate. Once in place, the stent expands like a spring, and it pushes back the prostate tissue, widening the urethra. Prostatic stents may be temporary or permanent. Urologists generally use prostatic stents in men who may not tolerate or be suitable for other procedures.
- Urethritis. Merck Manual. http://www.merckmanuals.com/home/kidney-and-urinary-tract-disorders/urinary-tract-infections-uti/urethritis[↩]
- Urethritis. Medline Plus. https://medlineplus.gov/ency/article/000439.htm[↩]
- Augenbraun MH, McCormack WM. Urethritis. In: Bennett JE, Dolin R, Blaser MJ, eds. Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases, Updated Edition. 8th ed. Philadelphia, PA: Elsevier Saunders; 2015:chap 109.[↩]
- Swygard H, Cohen MS. Approach to the patient with a sexually transmitted disease. In: Goldman L, Schafer AI, eds. Goldman-Cecil Medicine. 25th ed. Philadelphia, PA: Elsevier Saunders; 2016:chap 285.[↩]
- Urethral stricture. Mayo Clinic. https://www.mayoclinic.org/diseases-conditions/urethral-stricture/symptoms-causes/syc-20362330[↩]
- DISTAL URETHRAL STENOSIS IN LITTLE GIRLS. LYON RP, TANAGHO EA. J Urol. 1965 Mar; 93():379-88. https://www.ncbi.nlm.nih.gov/pubmed/14265182/[↩]
- Kerr WS, Leadbetter GW, Donahue J. An evaluation of internal urethrotomy in female patients with urethral or bladder neck obstruction. J Urol. 1966;95:218–20.[↩]
- Masarani M, Willis R. Urethral Dilatation in Women: Urologists’ Practice Patterns in the UK. Annals of The Royal College of Surgeons of England. 2006;88(5):496-498. doi:10.1308/003588406X114884. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1964673/[↩][↩][↩]
- Prostate Enlargement (Benign Prostatic Hyperplasia). National Institute of Diabetes and Digestive and Kidney Diseases. https://www.niddk.nih.gov/health-information/urologic-diseases/prostate-problems/prostate-enlargement-benign-prostatic-hyperplasia[↩]

{kind=link}