
Ankylosing spondylitis
Ankylosing spondylitis known as spondylitis, bamboo spine or radiographic axial spondyloarthritis, is a kind of arthritis that primarily affects the joints and ligaments of your spine (vertebrae) and sacroiliac joints. ‘Ankylosing’ means stiff and ‘spondylo’ means vertebra. In more advanced cases this inflammation can lead to ankylosis — new bone formation in the spine — causing sections of the spine to fuse in a fixed, immobile position. The hallmark feature of ankylosing spondylitis is the involvement of the sacroiliac joints during the progression of the disease. The sacroiliac joints are located at the base of the spine, where the spine joins the pelvis.
Ankylosing spondylitis can also affect other large joints – such as the shoulders, hips, ribs, heels, and small joints of the hands and feet and may also cause problems in your eyes (known as iritis or uveitis), skin, bowel, lungs and heart.
Ankylosing spondylitis affects 1 in 2,000 births. Males tend to be affected more severely and at an earlier age. Usual onset is between 15 and 25 years of age. Ankylosing spondylitis often runs in families. Relatives may have the disease, or another disease that is associated, for instance Reiter’s disease, psoriatic arthritis or enteropathic arthritis. The cause is unknown, but it is likely that both genes and factors in the environment play a role.
The hallmark feature of ankylosing spondylitis is the involvement of the sacroiliac (SI) joints during the progression of the disease in the late teens or early 20’s. The sacroiliac joints are located at the base of the spine, where the spine joins the pelvis. These problems often start in late adolescence or early adulthood. Early symptoms of ankylosing spondylitis include back pain and stiffness. Pain in one or both buttocks and lower back pain and stiffness are typically worse in the morning, and relieved by exercise. Over time, ankylosing spondylitis can fuse your vertebrae together, limiting movement. Some people have symptoms that come and go. Others have severe, chronic pain and discomfort.
Inflammation can also occur in other parts of the body. Other symptoms may include:
- Pain, stiffness, and inflammation in other joints.
- Difficulty taking deep breaths if the joints connecting the ribs are affected (costochondritis).
- Vision changes and eye pain (iritis or anterior uveitis).
- Feeling very tired or fatigue.
- Loss of appetite and weight loss.
- Skin rashes.
- Abdominal pain and loose bowel movements.
Most people with ankylosing spondylitis are young men in their late teens or early 20s who complain of persistent back pain and early morning stiffness. A smaller number experience pain in their hands or feet. Pronounced stiffness of the spine is the most typical sign, with diminished movements in all directions.
In severe cases the entire backbone may be fixed in a rigid position (‘poker back’), and chest expansion on breathing is reduced. Sometimes the hip joints are involved and become completely fused with resulting loss of movement. Some people may also develop eye, heart and breathing complications.
The exact cause of ankylosing spondylitis is currently unknown but a strong hereditary component has been observed. In particular, people who have a gene called human leukocyte antigen (HLA)-B27 are at a greatly increased risk of developing ankylosing spondylitis 1. However, only some people with the HLA-B27 gene develop the condition. Studies show that about 75 percent of children who inherit HLA-B27 from a parent with ankylosing spondylitis do not develop the disorder 2, 3. Generally speaking, no more than 2 percent of people born with HLA-B27 gene will eventually develop spondylitis. Ankylosing spondylitis cause is thought to be a combination of genetic predisposition and an environmental trigger.
Ankylosing spondylitis is diagnosed with a combination of blood tests and X-Rays. In addition to getting X-Rays of your lower back, your doctor may request X-Rays of your upper spine and neck. If you have symptoms affecting other joints in your body, like your hips or shoulders, you may also need X-Rays of these joints.
There is no cure for ankylosing spondylitis, but treatments can lessen symptoms and possibly slow progression of spondylitis and reduce the impact it has on quality of life. The goals of treatment of ankylosing spondylitis are to reduce symptoms, maintain spinal flexibility and normal posture, reduce functional limitations, maintain work ability, and decrease disease complications 4. The mainstays of treatment have been nonsteroidal antiinflammatory drugs (NSAIDs) and exercise, with the additional use of slow-acting antirheumatic drugs (SAARDs) in patients with peripheral arthritis. Over the past 15 years, the availability of tumor necrosis factor (TNF) inhibitors (e.g., infliximab, etanercept, adalimumab, certolizumab, golimumab, and their biosimilars) have greatly altered the approach to the treatment of ankylosing spondylitis. More recently, additional biologic agents (e.g., abatacept, rituximab, sarilumab, tocilizumab, ustekinumab) have been developed.
Figure 1. Vertebral column
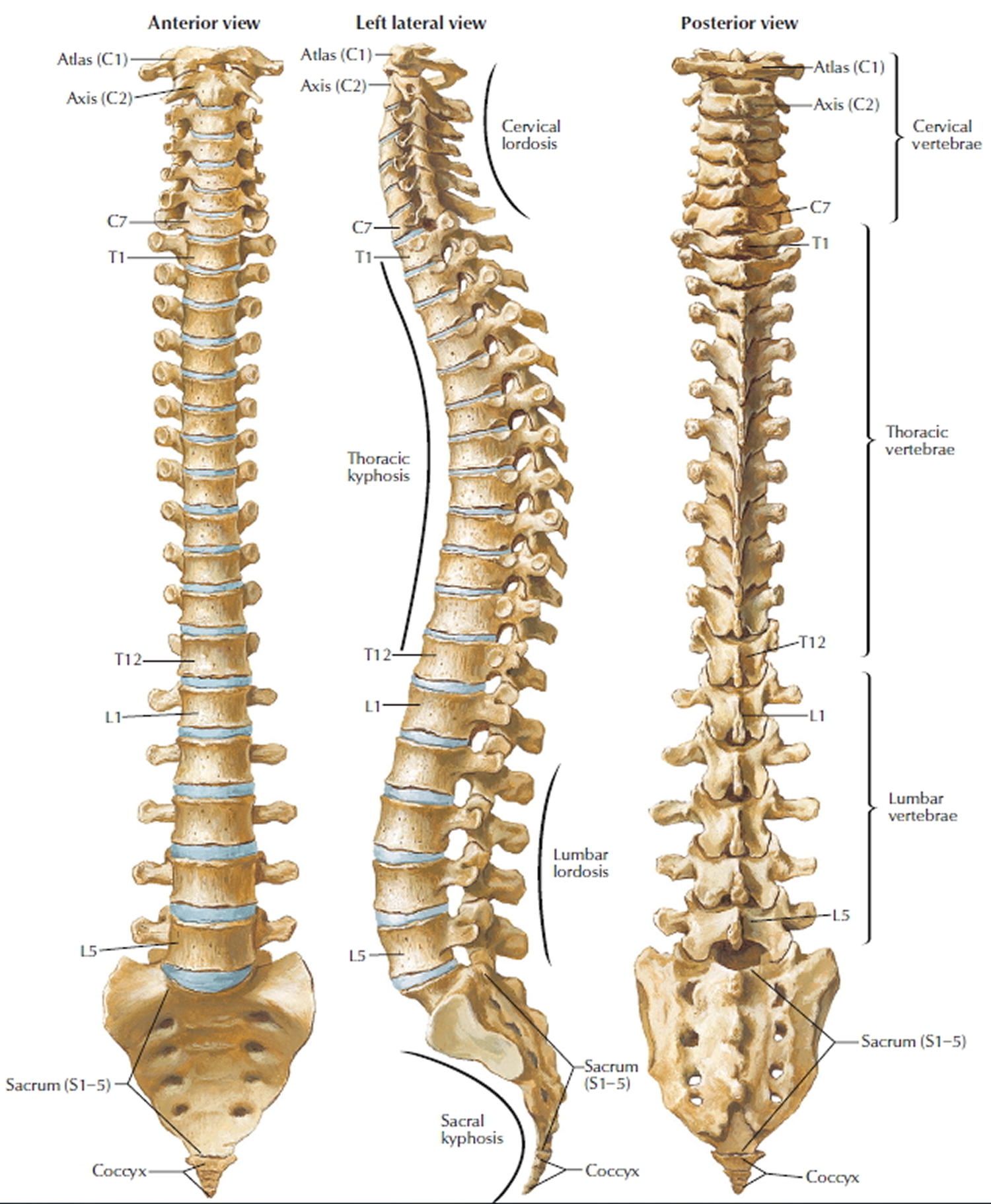
Figure 2. Ankylosing spondylitis areas of body involvement and inflammation
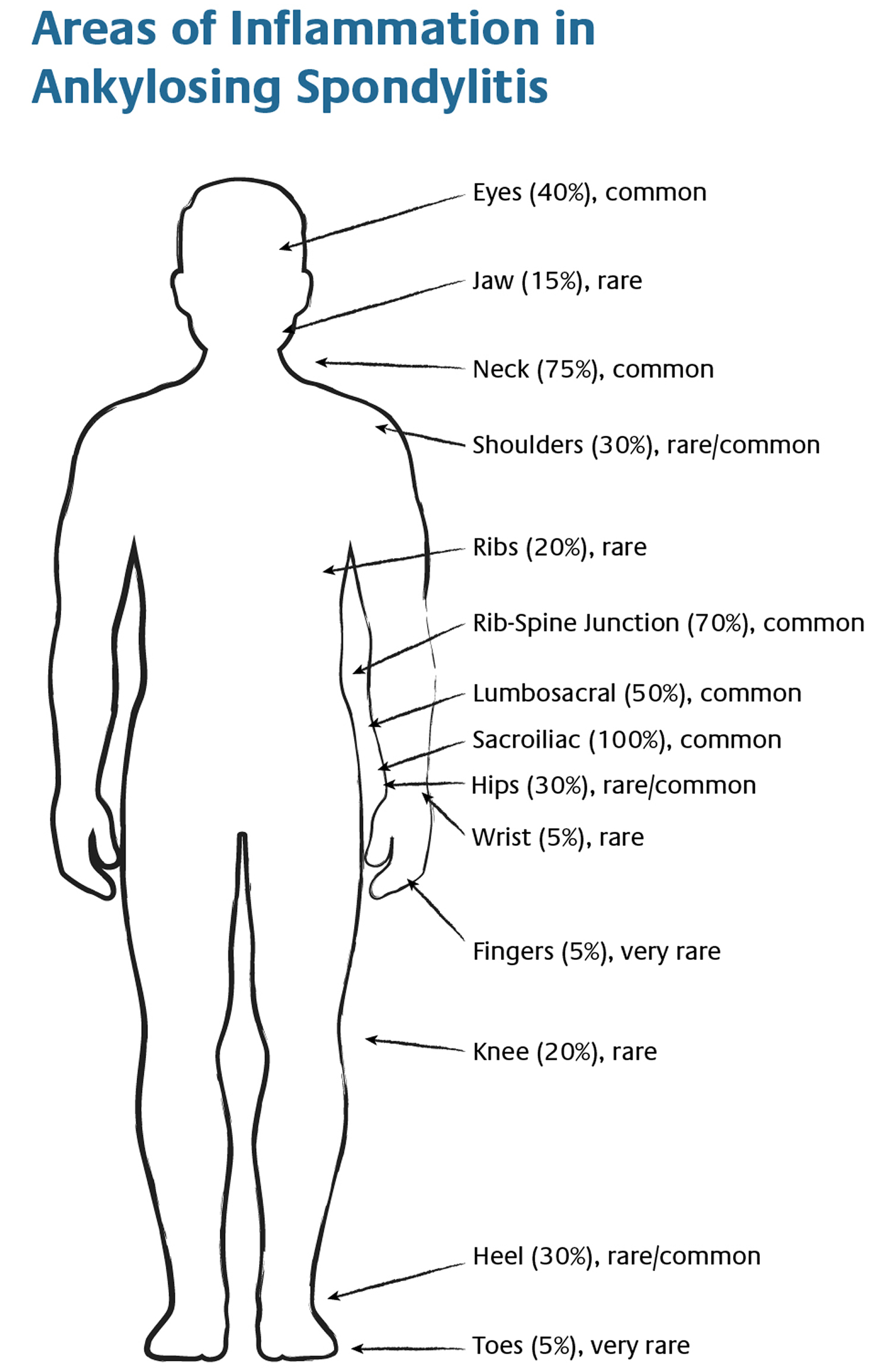
Figure 3. Ankylosing spondylitis in a 30 y.o male patient with chronic low back pain. HLA B27+ with active sacroiliitis

Figure 4. Ankylosing spondylitis sacroiliac joint inflammation (bone scan) – note high bone metabolic turnover at both sacroiliac joint indicating active inflammation.
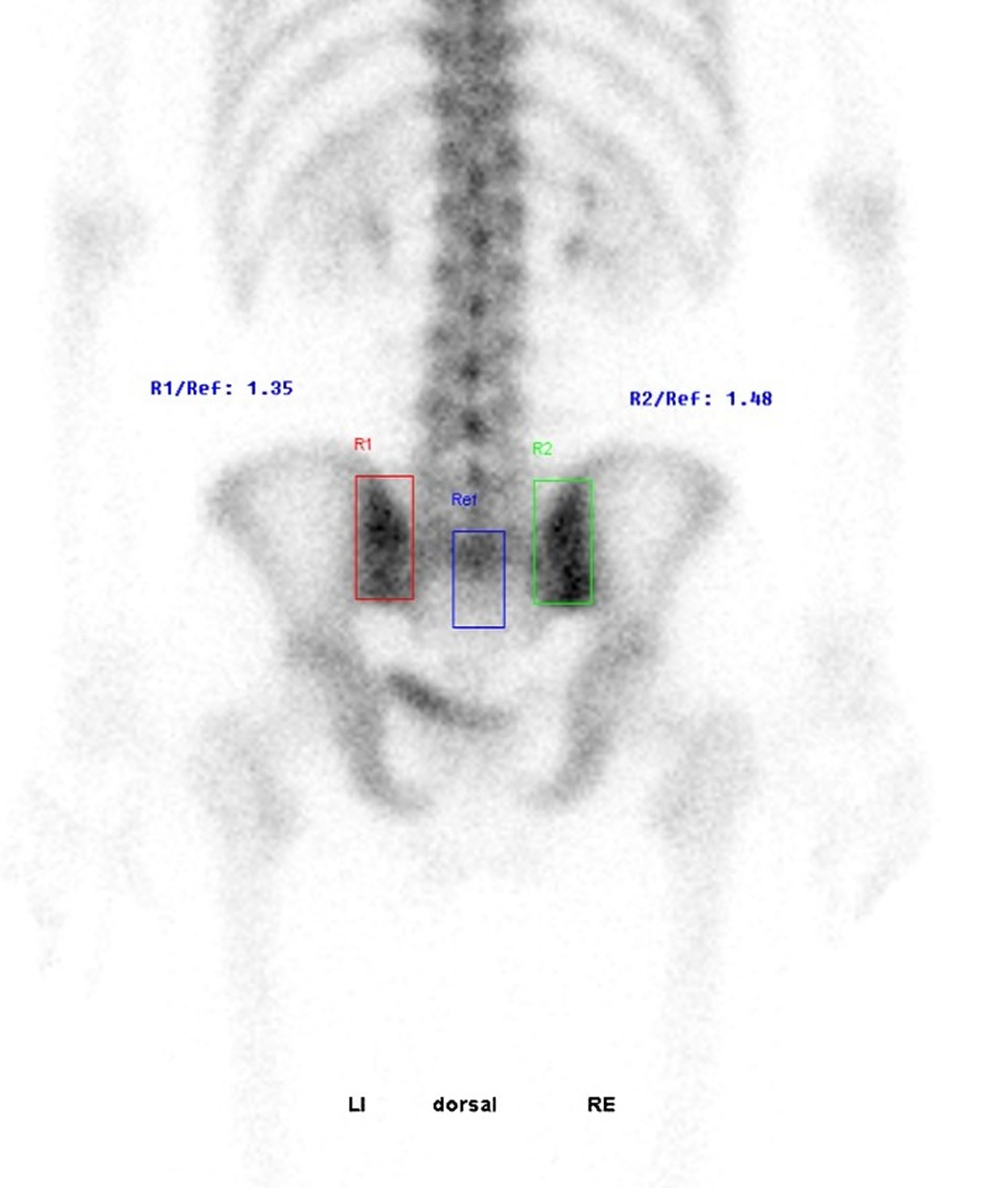
Figure 5. Bamboo spine

Footnote: Bamboo spine is a pathognomonic radiographic feature seen in ankylosing spondylitis that occurs as a result of vertebral body fusion by marginal syndesmophytes. It is often accompanied by fusion of the posterior vertebral elements as well. There is also a single central radiodense line related to ossification of supraspinous and interspinous ligaments which is called dagger sign. Additionally bilateral sacroiliac ankylosis is evident. Several hyperdense stones are present at bilateral renal lodges.
[Source 5 ]What is spondylosis?
Spondylosis also known as osteoarthritis of the spine, is used as a broad descriptive term referring to a common progressive degenerative (wear and tear) disorder of the human spine from any cause; it is usually further qualified by the part of the spine affected, e.g. cervical spondylosis (neck), thoracic spondylosis (middle back) and lumbar spondylosis (lower back). The lumbar region the most affected, because of the exposure to mechanical stress. Spondylosis is usually caused by wear and tear to the facet joints (zygapophysial joints), intervertebral discs, muscles and bones in your spine resulting in pain and stiffness in your neck (cervical spondylosis), middle back (thoracic spondylosis) and lower back (lumbar spondylosis). Like the rest of your body, the intervertebral disks and facet joints in your spine slowly degenerate as you age. Intervertebral discs consist of three major components: an outer fibrous ring called the anulus fibrosus, which surrounds an inner gel-like center, the nucleus pulposus and the cartilaginous endplates that anchor the discs to adjacent vertebrae (Figure 6) 6. The intervertebral disc (intervertebral disk) is the connecting medium between the vertebrae for the transmission of external force in a physiological environment and is important in the normal functioning of the spine. The intervertebral disc is a cushion of fibrocartilage and the principal joint between two vertebrae in the spinal column. There are 23 discs in the human spine: 6 in the cervical region (neck), 12 in the thoracic region (middle back), and 5 in the lumbar region (lower back). From a biomechanical point of view, the intervertebral discs facilitates spinal mobility by allowing your spine to be flexible without sacrificing a great deal of strength 7. They also provide a shock-absorbing effect within the spine and prevent the vertebrae from grinding together. The intervertebral disc is innervated in the outer few millimeters of the annulus fibrosus 8. Only the outer third of the anulus fibrosus is vascular and innervated in a non-pathologic state. In ageing and states of inflammation, both nerve growth and granulation tissue growth are stimulated. Additionally, the granulation tissue secretes inflammatory cytokines, which further increases sensitivity to pain sensations 6. Spondylosis changes can also result in spinal stenosis (narrowing of the spinal canal) and foraminal stenosis (a condition that results when the spinal nerve roots are compressed at the small openings at every level of the spinal column called foramina).
Patients with facet joint pain may present with symptoms of neck pain, back pain, and pain worsened with hyperextension, bending laterally, and rotation 9.
Many people with spondylosis that is seen on X-rays do not present any symptoms. In fact, lumbar spondylosis is present in 27%-37% of people without symptoms.
Approximately 90% of men ages 50 and older — and 90% of women ages 60 and older — have evidence of degenerative changes in the spine.
Some of the risk factors for spondylosis include:
- Repeated strains and sprains
- Occupation – such as jobs that require repetitive motions involving the neck or back
- Previous injuries
- Genetics
- Smoking
Symptoms of spondylosis may include:
- Tingling, numbness and weakness in the arms, hands, legs or feet
- Lack of coordination and difficulty walking
- Sciatica
- Radiculopathy
- Radiculitis
- Pinched nerves
- Localized pain and regional tenderness
- Muscle spasms
- Pain that worsens with prolonged standing, sitting and forward bending
- Numbness and tingling
- Weakness in one or more limbs
- Loss of bladder or bowel control
Seek immediate medical attention if you notice a sudden onset of numbness or weakness, or loss of bladder or bowel control.
As many people with spondylosis do not present symptoms, specific testing may be needed to get a medical diagnosis. If positive, a physician may use more specific terminology regarding your condition such as cervical degenerative disc disease, cervical spinal stenosis, or lumbar spinal stenosis as they describe the pain more effectively.
A doctor will begin with a physical examination to check your range of motion, reflexes, muscle strength and walk to observe if there are changes in your gait.
Imaging studies, such as an x-ray, MRI scan or CT myelography can provide detailed views of your spine. Electromyography (EMG) may also be performed to measure the electrical activity from your nerves to muscles.
The severity of your symptoms and diagnostic imaging results will determine the spondylosis treatment plan that is best for you. Often, conservative treatments will be suggested to relieve pain and help you get back to everyday life.
In severe cases or when non-surgical treatments for spondylosis fail to provide relief, surgical treatment may be recommended.
Non-surgical treatment
In mild to moderate cases of spondylosis, non-surgical treatment options can be effective. These options include:
- Lifestyle changes
- Rest
- Over-the-counter anti-inflammatory drugs
- Physical therapy
- Cortisone shots
- Chiropractic adjustments
- Prescription pain medication
Surgical treatment
Whether you have cervical (neck), lumbar (lower back), or thoracic (mid-back) spondylosis, surgery is NOT commonly recommended for spondylosis unless your doctor determines that:
- A spinal nerve is being pinched by a herniated disk or bone (cervical radiculopathy), or
- Your spinal cord is being compressed (cervical spondylotic myelopathy)
Patients who have progressive neurologic symptoms, such as arm weakness, numbness, unsteadiness while walking, or falling, are more likely to be helped by surgery.
Sometimes, surgery may be recommended if you have severe neck pain (without nerve compression) that has not been relieved by nonsurgical treatment. However, some patients with severe neck pain will not be candidates for surgery. This may be due to the widespread nature of their arthritis, other medical problems, or other causes for their pain, such as fibromyalgia.
What is spondyloarthritis?
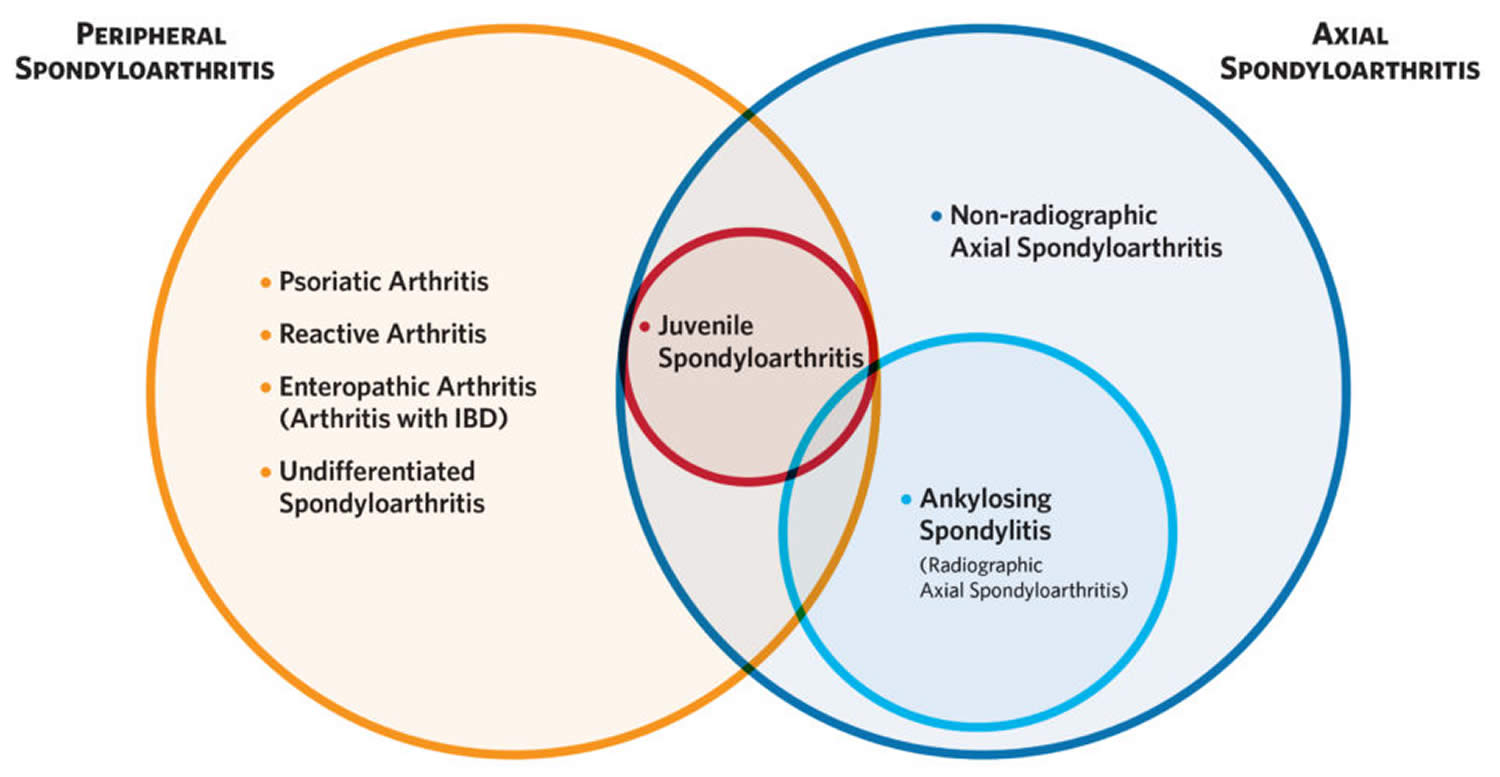
Spondyloarthritis refers to a family of closely related diseases that share common features – chief among them being inflammatory arthritis in the spine and other joints. These conditions are currently grouped into two overlapping categories:
- Axial spondyloarthritis, which is characterized by inflammatory pain and arthritis in the spine and hips. A hallmark symptom of axial spondyloarthritis is inflammatory back pain, frequently characterized by a dull ache felt deep in the lower back, or buttocks. It is associated with inflammation of the sacroiliac (SI) joints, which are the joints linking the lowest part of the spine to the pelvis. Axial spondyloarthritis is a broad category that includes people with and without characteristic bone changes or fusion in the spine. Doctors further classify adults as having one of two types of axial spondyloarthritis:
- Radiographic axial spondyloarthritis more commonly called ankylosing spondylitis, in which bone changes or fusing in the spine can be seen on x-ray; or
- Non-radiographic axial spondyloarthritis, without characteristic bone changes or fusing seen on x-ray. When other signs and symptoms of axial spondyloarthritis are present, but spinal changes are not visible on x-ray, the diagnosis is non-radiographic axial spondyloarthritis. Ankylosing spondylitis and non-radiographic axial spondyloarthritis are thus part of the same axial spondyloarthritis disease spectrum and present with many of the same symptoms. The main difference is that those with non-radiographic axial spondyloarthritis don’t show bone changes on x-rays, although inflammation can be spotted with the help of MRI. Some people with non-radiographic axial spondyloarthritis progress to developing ankylosing spondylitis, although many do not.
- Peripheral spondyloarthritis, characterized by inflammatory pain and arthritis in peripheral joints and tendons other than the spine. Commonly involved sites include joints in the hands, wrists, elbows, shoulders, knees, ankles, and feet. Inflammation of the tendons can occur in the fingers or toes (dactylitis) or where tendons and ligaments attach to bone (enthesitis). Other organs can also become involved, including the eyes (iritis), gut (inflammatory bowel disease), and skin (psoriasis). Peripheral spondyloarthritis encompasses a number of distinct, though closely related conditions, including psoriatic arthritis, enteropathic arthritis, reactive arthritis, and undifferentiated arthritis.
A person may have both axial and peripheral symptoms. The predominant symptoms (whether they are axial or peripheral) will determine the category, and the specific diagnosis.
Spondyloarthritis often begins in young people, with symptoms usually starting before age 45.
Figure 6. Spondyloarthritis
Who gets ankylosing spondylitis?
Anyone can get ankylosing spondylitis; however, certain factors may increase your risk for developing the disease, such as:
- Family history and genetics. If you have a family history of ankylosing spondylitis, you are more likely to develop the disease.
- Age. Most people develop symptoms of ankylosing spondylitis before age 45.
- Sex. Men are more likely to have ankylosing spondylitis than women.
- Other conditions. People who have Crohn’s disease, ulcerative colitis, or psoriasis may be more likely to develop the disease.
Does pregnancy in an individual with ankylosing spondylitis cause any complication to the mother or her baby?
It does not involve any problem for mother or baby , however some medications taken by the mother can be harmful to the baby. Consult and discuss with your doctor.
Is anemia, an indication for ankylosing spondylitis?
No, anemia is a disease where there is a deficiency of hemoglobin in the blood. It can be treated either by medication or blood transfusion (if necessary). In ankylosing spondylitis, anemia is an associated symptom, as the general constitution of the body is affected.
Ankylosing spondylitis prognosis
The outlook for ankylosing spondylitis is highly variable. For some people the condition improves after an initial period of inflammation, whereas for others it can get progressively worse over time. With special exercises and pain relief, most patients are able to lead independent lives and be fully employed.
Around 70-90% of people with ankylosing spondylitis remain fully independent or minimally disabled in the long term.
Most patients never require hospitalization. However, some people eventually become severely disabled as a result of the bones in their spine fusing in a fixed position and damage to other joints, such as the hips or knees.
With modern treatments, ankylosing spondylitis doesn’t normally affect life expectancy significantly, although the condition is associated with an increased risk of other potentially life-threatening problems.
What Happens over Time
Back and Spine
It is the process of healing and repair following inflammation of the entheses (inflammation where the ligaments attach to the bone) that eventually can lead to scarring of the tissues, which subsequently can lead to extra bone formation. Thus, in someone with very severe disease, the process of inflammation can lead, over many years, to a bony fusion of the ligaments in the spine and sometimes in other joints as well, which is called ankylosis. This can cause an increased risk of spinal fracture because of the restricted range of movement and the fact that the bone formed during fusion is inherently weak. Not everyone will go on to this stage of spondylitis.
Fusion of the spine can sometimes lead to a forward curvature of the spine, called kyphosis, causing a forward-stooped posture. Although this can happen in the most severe cases of ankylosing spondylitis, it is now far less common given the advances in treatment.
It is important to follow your doctor’s instructions, take your medicine on schedule and maintain a daily exercise regimen, which, over time, will make you feel better and lead to better outcomes. It is also important to pay particular attention to your posture in order to avoid kyphosis. With the advent of the newer classes of medications, specifically the biologics anti-tumor necrosis factor-alpha agents), there is reason to believe that the natural course of spondylitis may be slowed or halted. More studies are needed to confirm this.
Figure 7. Ankylosing spondylitis spine

Hips and shoulders
The hips and shoulders are affected in about one-third of people with ankylosing spondylitis. Hip involvement usually comes on gradually, and although the pain often is felt in the groin area, it can sometimes be felt in other areas of the body, such as the knees or the front of the thigh. When this happens, it is called “referred pain,” which can be very misleading to both a doctor and affected person. Hip involvement typically is more common in younger people when symptoms first begin. It often carries with it a more severe prognosis or course of disease. Generally speaking, shoulder involvement is mild.
Chest
Adults with spondylitis often have chest pain caused by costochondritis (a benign inflammation of the cartilage connecting the ribs to the breastbone) that mimics the heavy chest pain of unstable angina (acute heart attack) or pleurisy (the pain with deep breathing that occurs when the outer lining of the lung is inflamed). Anyone experiencing symptoms should seek medical attention to rule out a more serious condition. Over time, long-term inflammation of the joints between the ribs and spine (a condition called costochondritis), and where the ribs meet the breastbone in front of the chest, and scarring of tissue results in decreased chest expansion. Costochondritis pain can often be excruciating, especially after exercise or coughing. The pain usually goes away on its own; however, in certain cases, it can last for several months or longer. If the pain is found to be spondylitis-related and you find yourself unable to practice critical deep-breathing exercises, which help maintain chest expansion, there are things that you can do to help yourself:
- Use ice packs on the affected areas for short periods
- Try gentle massage of the neck and shoulder area
- Try deep breathing exercises after a hot shower or warm bath
- Talk to your doctor about trying different medications. Treatment focuses on pain relief, with prescription nonsteroidal antiinflammatory drugs (NSAIDs) like ibuprofen or naproxen or narcotics (Vicodin, Percocet) if the pain is severe. In addition, antidepressants (amitriptyline) and the epilepsy drug gabapentin (Neurontin) have proven successful in treating chronic pain.
Once your doctor has ruled out more serious problems, it might be helpful to take a few sessions with a physical therapist or respiratory therapist, who can provide instructions on how to maximize air intake by learning a technique called “diaphragm breathing.”
The Jaw
About 15 percent of people with spondylitis experience inflammation of the jaw. This can be particularly debilitating, causing difficulty in fully opening the mouth to eat.
Ankylosing spondylitis complications
In severe ankylosing spondylitis, new bone forms as part of the body’s attempt to heal. This new bone gradually bridges the gap between vertebrae and eventually fuses sections of vertebrae. Those parts of your spine become stiff and inflexible. Fusion can also stiffen your rib cage, restricting your lung capacity and function.
Other complications might include:
- Eye inflammation (iritis or anterior uveitis). Up to 50 percent of people with spondylitis will experience inflammation of the eye (iritis or uveitis) at least once. One of the most common complications of ankylosing spondylitis, iritis or anterior uveitis, can cause rapid-onset eye pain, redness, sensitivity to light and blurred vision. See your doctor right away if you develop these symptoms. Iritis is inflammation of the iris (the colored part of the eye). White blood cells can be seen in the front part of the eye (anterior chamber) by an ophthalmologist using a microscope known as a slit lamp. Iritis is a medical emergency and needs immediate attention as untreated eye inflammation may lead to permanent damage and even blindness. Iritis that is associated with spondylitis is typically treated with topical corticosteroid eye drops along with a dilating eye drop to prevent the iris from sticking to other ocular tissues, most notably the lens. In severe or unresponsive cases, corticosteroid injections around the eye may be used. Certain TNF inhibitors are also highly effective at reducing occurrences of iritis. Medications for glaucoma are sometimes required. The overall goal of treatment is to eliminate inflammation and minimize the amount and duration of steroid required 11. Other systemic medications utilized include methotrexate, infliximab (Remicade) and adalimumab (Humira).
- Osteoporosis and compression spinal fractures. Some people’s bones thin during the early stages of ankylosing spondylitis. Weakened vertebrae (osteoporosis) can crumble, increasing the severity of your stooped posture. Vertebral fractures can put pressure on and possibly injure the spinal cord and the nerves that pass through the spine. Osteoporosis is where the bones become weak and brittle. In AS osteoporosis can develop in the spine and increase your risk of fracturing the bones in your backbone. The longer you have the condition, the more this risk increases. If you do develop osteoporosis, you’ll usually need to take medication to help strengthen your bones. There are a number of medications that can be used to treat osteoporosis, which can be taken by mouth (orally) as tablets or given by injection.
- Reduced flexibility. Although most people with ankylosing spondylitis remain fully independent or minimally disabled in the long term, some people with the condition eventually have severely restricted movement in their spine. This usually only affects the lower back and is the result of the bones in the spine joining up (fusing). Fusing of the spine can make it difficult to move your back and can mean your posture becomes fixed in one position, although it doesn’t lead to severe disability in most cases. In rare cases surgery may be recommended to correct severe bends in the spine.
- Heart problems. In addition to well-known extra-articular manifestations, ankylosing spondylitis has been reported to be associated with a number of cardiovascular diseases, including aortitis (inflammation of the aorta), aortic valve disease, conduction disturbances, cardiomyopathy, and ischemic heart disease. Cardiac issues are found in an estimated two to 10 percent of people with ankylosing spondylitis. In the 1930s, a study found aortitis in a group of patients with ankylosing spondylitis. Since then, a number of cardiovascular diseases have been linked to ankylosing spondylitis, many of which begin prior to the onset of clinical symptoms. In 2011, Canadian researchers found that ankylosing spondylitis increases the risk of heart disease and stroke by as much as 25 percent to 60 percent. The increase was greatest for people with ankylosing spondylitis between the ages of 20 and 39. Compared to the non-ankylosing spondylitis population, the study found that ankylosing spondylitis patients had a 58 percent higher risk of valvular heart disease, a 37 percent higher risk of ischemic heart disease, and a 25 percent higher risk of stroke. The researchers say the link between ankylosing spondylitis and heart disease exists for a number of reasons, including the chronic inflammation associated with ankylosing spondylitis, the use of NSAIDs, and a tendency to exercise less than the general population due to pain. Spondylitis patients should be screened with a physical exam, and an echocardiogram (a diagnostic test that may show abnormalities such as valve dysfunction or damage to heart tissue) annually to rule out any issues affecting the heart.
- Aortitis. Aortitis is the inflammation of the aorta, the large artery that takes blood from the heart and distributes it to the rest of the body. Aortitis can result in aortic insufficiency, or the inability of the aorta to carry sufficient amounts of blood to the body, and hypertension (high blood pressure). A number of people with AS have chronic inflammation at the base of the heart, around the aortic valve, and at the origin of the aorta. Years of chronic inflammation can lead to valve leakage, which sometimes requires surgical intervention. Management of aortitis includes controlling the inflammation with medications, treating complications, and preventing its recurrence. Aortic valve disease – a condition in which the valve between the heart’s main pumping chamber (left ventricle) and the aorta does not work properly. There are two main types of aortic valve disease – aortic stenosis (narrowing of the aortic valve opening) and aortic regurgitation, in which the aortic valve does not close properly, causing blood to flow backward into the left ventricle. This condition, which can cause shortness of breath, chest pain (angina), and dizziness, is often treated with surgery to repair or replace the faulty valve.
- Conduction disturbances. Conduction disturbances are arrhythmias that cause the heart to beat too fast (tachycardia) or too slow (bradycardia), and to pump blood less efficiently. The disturbances are caused either by a disruption of the heart’s normal electrical conduction system or by heart disease. People with conduction disturbances often feel a palpitation or skipped heart beat and a fluttering sensation the chest and neck, as well as fatigue, dizziness, lightheadedness, shortness of breath, and chest pain. In extreme cases, conduction disturbances can cause sudden cardiac arrest. Arrhythmias are treated with medication, ablation (radiofrequency energy delivered at the site of the electrical disturbance), defibrillation (an electronic shock to the heart), or with an implantable cardioverter defibrillator (a pacemaker-like device that delivers a shock to the heart to restore normal rhythm).
- Cardiomyopathy. Cardiomyopathy is a disease that enlarges and weakens the heart muscle, making it harder for the heart to pump blood to the rest of the body. Left untreated, cardiomyopathy can lead to heart failure, blood clots, valve problems, and cardiac arrest. The symptoms of cardiomyopathy include shortness of breath with exertion or even at rest, swelling of the legs, ankles and feet, abdominal bloating, fatigue, and an irregular heartbeat. Most often, cardiomyopathy is treated by managing symptoms, preventing the condition from worsening, and reducing the risk for complications. Medications like ACE inhibitors (a type of blood pressure medication) can help improve the heart’s pumping capabilities, and beta blockers can help improve heart function, as well. Some patients receive a pacemaker to coordinate contractions between the left and right ventricles or a ventricular assist device to keep blood circulating through the heart.
- Ischemic hearts disease. Ischemic hearts disease is characterized by reduced blood supply to the heart muscle, usually due to coronary artery disease. People with ischemic heart disease, also called atherosclerosis, often have angina, chest pressure, decreased tolerance for exercise, and difficulty breathing; many people mistake these symptoms for heartburn. Treatment includes anti-angina medications (nitroglycerin), medications to lower blood pressure and blood cholesterol, angioplasty with stent placement, and coronary bypass surgery.
- Cauda equina syndrome. Cauda equina syndrome is a very rare complication of ankylosing spondylitis that occurs when nerves at the bottom of your spine become compressed (compacted). Cauda equina syndrome causes:
- pain or numbness in your lower back and buttocks
- weakness in your legs – which can affect your ability to walk
- urinary incontinence or bowel incontinence – when you cannot control your bladder or bowels
- See your doctor as soon as possible if you have ankylosing spondylitis and you develop any of these symptoms.
- Chest infections
- Joint damage. Ankylosing spondylitis can cause joints such as the hips and knees to become inflamed. This can damage the affected joints over time, making them painful and difficult to move. If a joint becomes particularly damaged, you may need surgery to replace it with an artificial one.
- The effect of medications.
- Steroids (prednisolone). Although not always used to treat ankylosing spondylitis, they may be used from time to time. Common side effects include thinning of the bones, gaining weight and mood disturbance.
- Specialist medications (tumor necrosis factor (TNF) inhibitors) – these have a number of side effects, including nausea, vomiting and drowsiness. More seriously, they can increase the risk of serious infection, and mildly increase the risk of developing some rare cancers.
- Fatigue is a common complaint in spondyloarthritis, and one that doesn’t often receive the attention it deserves. Different from feeling “tired,” fatigue doesn’t just go away after a good night’s sleep, and can affect many aspects of life. Fatigue, sometimes appearing with brain fog, can negatively impact one’s work, social life, relationships, ability to focus, and even emotional state. Studies show that uncontrolled systemic inflammation is the factor most closely associated with fatigue in spondyloarthritis. If inflammation is extensive, then the body must use energy to deal with it. The release of certain cell messengers (cytokines) during the inflammatory process can produce the sensation of fatigue, as well as mild to moderate anemia in some cases – which can also contribute to fatigue. When inflammation is well controlled, and disease activity properly managed, fatigue can lessen and energy can improve. Uncontrolled pain and stiffness can disturb sleep and make it difficult to get rest. This of course contributes to fatigue. Besides causing fatigue, not sleeping well can also increase pain, creating a feedback loop of pain causing sleeplessness, which then causes more pain and fatigue, and so on. When symptoms such as pain and stiffness are appropriately treated, sleep often improves, and fatigue diminishes. Other things to help bring about better sleep include slowly increasing physical activity – which can help by tiring the body, helping with stiffness and pain, as well as reducing inflammation. Practicing good sleep hygiene is also important. This includes avoiding caffeine and other sleep disruptive foods or drinks late in the evening, establishing a regular and relaxing bedtime routine, creating a comfortable and calming sleep environment, and considering the use of items to block out light and disruptive noises if needed. Depression also causes fatigue directly by lowering energy levels, as well as indirectly by interfering with sleep. Depression lowers serotonin levels, which, among other things, helps regulate our circadian rhythm – the internal body clock controlling sleepiness and wakefulness. As such, depression is often linked with insomnia, while lack of sleep can worsen depression. Those with chronic pain are more likely than the general population to suffer from depression. There is also a feedback loop between pain and depression, with each making the other worse, and of course further impacting fatigue. Other causes of fatigue may include untreated anemia, and thyroid diseases, among other things. Speaking with your rheumatologist about fatigue is the first step. Only after your particular causes of fatigue have been identified, can those causes be addressed, and appropriate changes made to help lessen it.
- Rarely, kidney disease
- Amyloidosis. In very rare cases it’s possible to develop a condition called amyloidosis as a complication of ankylosing spondylitis 12, 13. Amyloid is a protein produced by cells in your bone marrow, the spongy material found in the centres of some hollow bones. Amyloidosis is a condition where amyloid builds up in organs such as your heart, kidneys and liver. It can cause a wide range of symptoms, including:
- fatigue
- weight loss
- fluid retention (edema)
- shortness of breath
- numbness or tingling in the hands and feet
Ankylosing spondylitis causes
The causes of ankylosing spondylitis are not yet understood. However, doctors believe genetics may play a role, because ankylosing spondylitis tends to run in families. Also, most people with ankylosing spondylitis share the same gene (called HLA B27). However, only some people with the gene develop the condition. Studies show that about 75 percent of children who inherit HLA-B27 from a parent with ankylosing spondylitis do not develop the disorder 2, 3. It is not fully known how HLA-B27 increases the risk of developing ankylosing spondylitis. Multiple genetic and environmental factors likely play a part in determining the risk of developing ankylosing spondylitis.
Among people who are HLA-B27 positive, the prevalence of ankylosing spondylitis is approximately 5% to 6%. In the United States, the prevalence of HLA-B27 varies among ethnic groups. According to a 2009 survey, prevalence rates of HLA-B27 were 7.5% among non-Hispanic Whites, 4.6% among Mexican-Americans, and 1.1% among non-Hispanic Blacks 14, 15.
HLA-B27 gene
Research has shown more than 9 out of 10 people with ankylosing spondylitis carry a particular gene known as human leukocyte antigen B27 (HLA-B27).
Having the HLA-B27 gene doesn’t necessarily mean you’ll develop ankylosing spondylitis. It’s estimated 8 in every 100 people in theCaucasian population have the HLA-B27 gene, but most don’t have ankylosing spondylitis. Generally speaking, no more than 2 percent of people born with HLA-B27 gene will eventually develop spondylitis.
It is important to note that the HLA-B27 test is not a diagnostic test for ankylosing spondylitis. Also, the association between ankylosing spondylitis and HLA-B27 varies among different ethnic and racial groups. It can be a very strong indicator in that more than 95 percent of people in the Caucasian population who have ankylosing spondylitis test positive for HLA-B27. However, close to 80 percent of ankylosing spondylitis patients from Mediterranean countries and only 50 percent of African American patients with ankylosing spondylitis are HLA-B27 positive.
It’s thought having this gene may make you more vulnerable to developing ankylosing spondylitis. The condition may be triggered by one or more environmental factors, although it’s not known what these are.
Testing for this gene may be carried out if ankylosing spondylitis is suspected. However, this test isn’t a very reliable method of diagnosing the condition because some people can have the HLA-B27 gene but not have ankylosing spondylitis.
Ankylosing spondylitis can run in families, and the HLA-B27 gene can be inherited from another family member.
- If you have ankylosing spondylitis and tests have shown you carry the HLA-B27 gene, the chance of any children you have developing the condition is less than 20%.
- If you have ankylosing spondylitis but don’t carry the HLA-B27 gene, the chance of any children you have developing the condition is less than 10%.
- If you have a close relative who has ankylosing spondylitis, such as a parent or a brother or sister, you’re three times more likely to develop the condition compared with someone who doesn’t have a relative with the condition.
Risk factors for developing ankylosing spondylitis
Men are more likely to develop ankylosing spondylitis than are women. Onset generally occurs in late adolescence or early adulthood. Most people who have ankylosing spondylitis have the HLA-B27 gene. But many people who have this gene never develop ankylosing spondylitis.
Variations in several additional genes, including ERAP1, IL1A, and IL23R, have also been associated with ankylosing spondylitis 16. Although many of these genes play critical roles in the immune system, it is not fully known how variations in these genes affect a person’s risk of developing ankylosing spondylitis. Changes in genes that have not yet been identified also likely affect the chances of developing ankylosing spondylitis and influence the progression of the disorder. Researchers are working to identify these genes and clarify their role in ankylosing spondylitis.
Ankylosing spondylitis symptoms
Inflammation of the entheses, where joint capsules, ligaments, or tendons attach to bone, is a hallmark of ankylosing spondylitis. This can be felt in multiple areas of the body, where doctor can check for pain and tenderness. The sites are sometimes referred to as “hot spots.” They can lead to swelling and tenderness along the back, pelvic bones, sacroiliac joints, the chest, and the heel. The heel can be significantly affected, and the pain and tenderness can have a serious impact on a person’s mobility. The two areas of the foot that can be affected are the Achilles tendon, at the back of the heel and the plantar fascia, at the base of the heel.
It is important to note that the course of ankylosing spondylitis varies greatly from person to person. So too can the onset of symptoms. Although symptoms usually start to appear in late adolescence or early adulthood (ages 17 to 45), symptoms can occur in children or much later in life.
The areas most commonly affected by ankylosing spondylitis are:
- The joint between the base of the spine and the pelvis
- The vertebrae in the lower back
- The places where tendons and ligaments attach to bones, mainly in the spine, but sometimes along the back of the heel
- The cartilage between the breastbone and the ribs
- The hip and shoulder joints
The symptoms of ankylosing spondylitis tend to come and go. The more common symptoms include:
- back pain or buttock pain, that may be worse in bed at night
- stiffness in the morning, or after long periods of rest
- other joint pain
- pain in tendons and ligaments, such as in the chest wall, soles of the feet, or heels
- problems with your heart, lungs, bowel, skin or eyes.
Ankylosing spondylitis additional symptoms that you may or may not experience include:
- Lethargy, general unwellness, recurrent bouts of mild fever.
- Pain and swelling in other joints eg. hip, shoulder, kneecap, below the heel.
- Red and sore eyes and problems with vision due to inflammation in the eye (iritis). Damage will become permanent if left untreated.
- Diarrhea and bloating caused by inflammation of the stomach lining (inflammatory bowel disease).
- Focal pain on the chest due to inflammation of the rib-ligament joints (enthesitis).
- White-scaly rashes (psoriasis) on the skin around your elbow and/or knees.
Many of these symptoms can be a sign of other conditions, so it’s best to seek medical advice to make a diagnosis.
The most common early symptoms of ankylosing spondylitis are frequent pain and stiffness in the lower back and buttocks, which comes on gradually over the course of a few weeks or months. At first, discomfort may only be felt on one side, or alternate sides. The pain is usually dull and diffuse, rather than localized. This pain and stiffness is usually worse in the mornings and during the night, but may be improved by a warm shower or light exercise. Also, in the early stages of ankylosing spondylitis, there may be mild fever, loss of appetite, and general discomfort. It is important to note that back pain from ankylosing spondylitis is inflammatory in nature and not mechanical.
The pain typically becomes persistent (chronic) and is felt on both sides, usually lasting for at least three months. Over the course of months or years, the stiffness and pain can spread up the spine and into the neck. Pain and tenderness spreading to the ribs, shoulder blades, hips, thighs, and heels is possible as well.
Note that ankylosing spondylitis can present differently at onset in some people. This tends to be the case in women more than men. For example, anecdotally from some women with ankylosing spondylitis that their symptoms started in the neck rather than in the lower back.
Varying levels of fatigue may also result from the inflammation caused by ankylosing spondylitis. The body must expend energy to deal with the inflammation, thus causing fatigue. Also, mild to moderate anemia, which may also result from the inflammation, can contribute to an overall feeling of tiredness.
In a minority of individuals, pain does not start in the lower back, or even the neck, but in a peripheral joint such as the hip, ankle, elbow, knee, heel, or shoulder. This pain is commonly caused by enthesitis, inflammation of the site where a ligament or tendon attaches to bone. Inflammation and pain in peripheral joints is more common in juveniles with ankylosing spondylitis. This can be confusing since, without the immediate presence of back pain, ankylosing spondylitis may look like some other form of arthritis.
Many people with ankylosing spondylitis also experience bowel inflammation, which may be associated with Crohn’s disease or ulcerative colitis.
Ankylosing spondylitis is often accompanied by iritis or uveitis (inflammation of the eyes). About one-third of people with ankylosing spondylitis will experience inflammation of the eye at least once. Signs of iritis or uveitis are: Eye(s) becoming painful, watery, and red, blurred vision, and sensitivity to bright light.
Ankylosing spondylitis prevention
If you are very concerned about developing this disease there are genetic tests that confirm if you have a gene strongly related to ankylosing spondylitis.
If you have a diagnosis of ankylosing spondylitis and wish to prevent complications, you should:
- Stay active, exercising regularly and when appropriate using physical therapy to maintain your posture. Exercise is an integral part of treating ankylosing spondylitis. In fact, in no other type of arthritis is the role of exercise more important. Exercise can counteract some of the impacts of spondyloarthritis, helping you maintain more of your mobility and flexibility. According to doctors and patients alike, exercise is effective in controlling pain. Exercise has been shown to optimize physical and mental health in everybody. In addition to directly increasing strength, endurance, balance, and flexibility, some of the other physical benefits of exercise include improving cardiovascular endurance, reducing high blood pressure, increasing good cholesterol (HDL), maximizing bone density, helping weight management and possibly even enhancing response to medications.
- Stop smoking – the importance of preserving lung function cannot be overemphasised in ankylosing spondylitis. Talk to your doctor about Quit programs and medications if you are struggling to stop smoking.
- Take medications and anti-inflammatories as prescribed by your doctor.
- Wear spine braces early in the disease. These can be worn at night.
Ankylosing spondylitis diagnosis
A rheumatologist is commonly the physician who will diagnose ankylosing spondylitis, since they are doctors who are specially trained in diagnosing and treating disorders that affect the joints, muscles, tendons, ligaments, connective tissue, and bones. A thorough physical exam, including X-rays, individual medical history, and a family history of ankylosing spondylitis, as well as blood work (including a test for HLA-B27) are factors in making a diagnosis.
Note that ankylosing spondylitis can present differently at onset in some people. This tends to be the case in women more than men.
The following clinical features are taken into account when making an ankylosing spondylitis diagnosis:
- Onset is usually under 45 years of age.
- Pain persists for more than three months (i.e., it is chronic).
- Back pain and stiffness worsen with immobility, especially at night and early morning.
- Back pain and stiffness tend to ease with physical activity and exercise.
Varying levels of fatigue may also result from the inflammation caused by ankylosing spondylitis. The body must expend energy to deal with the inflammation, thus causing fatigue. Also, mild to moderate anemia, which may also result from the inflammation, can contribute to an overall feeling of tiredness.
The hallmark of ankylosing spondylitis is involvement of the sacroiliac (SI) joints. Some physicians still rely on X-ray to show erosion typical of sacroiliitis, which is inflammation of the sacroiliac joints. Using conventional X-rays to detect this involvement can be problematic because it can take seven to 10 years of disease progression for the changes in the sacroiliac joints to be serious enough to show up on conventional X-rays.
Another option is to use MRI to check for SI involvement, but MRI can be cost prohibitive in some cases.
Ankylosing spondylitis test
There are no specific lab tests to identify ankylosing spondylitis. Certain blood tests can check for markers of inflammation, but inflammation can be caused by many different health problems. Laboratory findings in ankylosing spondylitis are generally nonspecific but may help assist with diagnosis. About 50% to 70% of patients with active ankylosing spondylitis have elevated acute phase reactants, such as erythrocyte sedimentation rate (ESR) and elevated C-reactive protein (CRP). A normal ESR and CRP, however, should not exclude the disease 17, 18.
Your blood can be tested for the HLA-B27 gene, but most people who have that gene don’t have ankylosing spondylitis, and fewer black people with the disease have the gene than do white people. HLA-B27 is a perfectly normal gene found in 8 percent of the Caucasian population. Generally speaking, no more than 2 percent of people born with this gene will eventually develop ankylosing spondylitis.
It is important to note that the HLA-B27 test is not a diagnostic test for ankylosing spondylitis. Also, the association between ankylosing spondylitis and HLA-B27 varies among different ethnic and racial groups. It can be a very strong indicator in that more than 95 percent of people in the Caucasian population who have ankylosing spondylitis test positive for HLA-B27. However, close to 80 percent of ankylosing spondylitis patients from Mediterranean countries and only 50 percent of African American patients with ankylosing spondylitis are HLA-B27 positive.
Since there is no single blood test for ankylosing spondylitis, laboratory work may, or may not, be of help. Elevated erythrocyte sedimentation rate (ESR), also known as SED rate, and C-reactive protein (CRP) are common indicators of inflammation. Elevated levels of these markers, however, are not present in all ankylosing spondylitis patients and, when they are, it can be from other causes such as anemia, infection, or cancer. For example, it is estimated that less than 70 percent of people with ankylosing spondylitis have a raised ESR level.
Finally, there is no association between ankylosing spondylitis and rheumatoid factor (associated with rheumatoid arthritis) and antinuclear antibodies (associated with lupus).
Imaging tests
A number of imaging abnormalities, especially those affecting the spine and sacroiliac joints, are characteristic of ankylosing spondylitis.
X-rays allow doctors to check for changes in joints and bones, though the visible signs of ankylosing spondylitis might not be evident early in the disease. Bamboo spine is a pathognomonic radiographic feature seen in ankylosing spondylitis that occurs as a result of vertebral body fusion by marginal syndesmophytes. It is often accompanied by fusion of the posterior vertebral elements as well. In a bamboo spine, the outer fibers of the annulus fibrosus of the intervertebral discs ossify, which results in the formation of marginal syndesmophytes between adjoining vertebral bodies 19. The resulting radiographic appearance, therefore, is that of thin, curved, radiopaque spicules that completely bridge adjoining vertebral bodies. There is also accompanying squaring of the anterior vertebral body margins with associated reactive sclerosis of the vertebral body margins (shiny corner sign) 19. Together these give the impression of undulating continuous lateral spinal borders on AP spinal radiographs and resemble a bamboo stem; hence the term bamboo spine.
The hallmark of ankylosing spondylitis is involvement of the sacroiliac (SI) joints. Some physicians still rely on X-ray to show erosion typical of sacroiliitis, which is inflammation of the sacroiliac joints. Using conventional X-rays to detect this involvement can be problematic because it can take seven to 10 years of disease progression for the changes in the SI joints to be serious enough to show up on conventional X-rays.
Another option is to use MRI to check for sacroiliac (SI) involvement. An MRI uses radio waves and a strong magnetic field to provide more-detailed images of bones and soft tissues. MRI scans can reveal evidence of ankylosing spondylitis earlier in the disease process, but are much more expensive.
Although scans can sometimes show spinal inflammation and fusing of the spine (ankylosis), damage to the spine can’t always be picked up in the early stages of ankylosing spondylitis.
This is why diagnosis is often difficult. In many cases confirming a diagnosis is a long process that can take years.
A diagnosis of ankylosing spondylitis can usually be confirmed if an X-ray shows inflammation of the sacroiliac joints (sacroiliitis) and you have at least one of the following:
- at least three months of lower back pain that gets better with exercise and doesn’t improve with rest
- limited movement in your lower back (lumbar spine)
- limited chest expansion compared with what is expected for your age and sex
If you have all three of these features but don’t have sacroiliitis – or if you only have sacroiliitis – you’ll be diagnosed with probable ankylosing spondylitis.
According to the Assessment of SpondyloArthritis international Society (ASAS) 2009 axial spondyloarthritis criteria, evidence of sacroiliitis on imaging (radiographic or MRI) is a major inclusion criterion for ankylosing spondylitis 20. A standardized plain radiographic grading scale exists for sacroiliitis, which ranges from normal (0) to most severe (4), as detailed below.
- 0: Normal SI joint width, sharp joint margins
- 1: Suspicious
- 2: Sclerosis, some erosions
- 3: Severe erosions, pseudo dilation of the joint space, partial ankylosis
- 4: Complete ankylosis (fusion)
In the first few years of ankylosing spondylitis, plain radiographic changes in the sacroiliac (SI) joints can be very subtle, but within the first decade will usually become more obvious 21. Subchondral erosions, sclerosis, and joint fusion are the most obvious abnormalities, and these radiographic changes are typically symmetric.
A series of plain radiographic changes characteristic of ankylosing spondylitis can progressively develop over the course of the disease. An early sign is “squaring” of the vertebral bodies, best seen on lateral x-ray. This is seen as a loss of normal concavity of the anterior and posterior borders of the vertebral body due to inflammation and bone deposition. Romanus lesions, or the “shiny corner sign,” can also be seen on this radiographic view in the early stages. These lesions are characterized by small erosions and reactive sclerosis at the corners of the vertebral bodies. Late-stage findings include ankylosis (fusion) of the facet joints of the spine, syndesmophytes, and calcification of the anterior longitudinal ligament, supraspinous ligaments, and interspinous ligaments. This calcification may be seen on imaging as the “dagger sign,” which is represented as a single radiodense line running vertically down the spine on frontal radiographs. The classic radiographic finding in late-stage ankylosing spondylitis is the “bamboo spine sign,” which refers to the vertebral body fusion by syndesmophytes. A bamboo spine typically involves the thoracolumbar or lumbosacral junctions. It is this fusion of the spine that predisposes the patient to progressive back stiffness.
While plain radiography is the first-line imaging modality in ankylosing spondylitis, MRI may be needed to reveal more subtle abnormalities such as fatty changes or inflammatory changes. Active SI joint inflammatory lesions appear as bone marrow edema (BME) on short tau inversion recovery (STIR) and T2-weighted images with fat suppression. It should be noted that the presence of bone marrow edema on MRI can also be seen in up to 23% of patients with mechanical back pain and 7% of healthy people 22.
Ankylosing spondylitis treatment
The aim of treatment is to reduce pain and stiffness, and prevent or delay spinal deformity or other complications. If you have ankylosing spondylitis, your doctor may suggest that you try physiotherapy, including different types of exercise to strengthen your back, encourage movement in the spine and reduce pain.
You may also be prescribed anti-inflammatories or other types of medications to relieve inflammation, pain and stiffness. Surgery may be recommended to replace or remove joints or thickened bone. However, most people with ankylosing spondylitis don’t need surgery.
The course of your condition can change over time, and you might have painful episodes (relapses) and periods of less pain (remissions) throughout your life. But most people are able to live productive lives despite a diagnosis of ankylosing spondylitis.
You might want to join an online or in-person support group of people with this condition, to share experiences and support.
Medications
Nonsteroidal anti-inflammatory drugs (NSAIDs) — such as naproxen (Aleve, Naprosyn, others) and ibuprofen (Advil, Motrin IB, others) — are the medications doctors most commonly use to treat ankylosing spondylitis. Nonsteroidal anti-inflammatory drugs (NSAIDs) can relieve inflammation, pain and stiffness, but they can damage the lining of the gut and cause gastrointestinal bleeding. Adding a cup of active-culture yogurt and a banana each day to your diet can help protect your digestive tract. Yogurt’s bacteria helps maintain a healthy mix of microorganisms, while bananas have a type of starch that is digested by organisms in the gut to form a substance that helps protect the lining of the gut wall. Easily reap the benefits by combining the banana, yogurt, and a cup of orange juice for a quick and delicious smoothie.
Sometimes, high doses of NSAIDs are needed to maintain relief from the symptoms of ankylosing spondylitis and related diseases. This can pose a problem because NSAIDs can cause significant side effects, especially in the gastrointestinal tract (stomach, intestines, etc.). NSAIDs can cause reduced amounts of protective mucus in the stomach, which can result in stomach irritation. Over time, this can lead to heartburn, gastritis, and possibly ulcers and even bleeding. People can take other medications (such as antacids) to neutralize or prevent the production of excess stomach acid, help coat and protect the stomach (such as Carafate), or restore the lost mucus (such as Cytotec). NSAIDs may also be an increased risk of heart attack or stroke associated with NSAIDs, especially in people with a history of heart diseases.
If NSAIDs aren’t helpful, your doctor might suggest starting sulfasalazine, methotrexate, corticosteroid, tumor necrosis factor (TNF) blocker (also called tumor necrosis factor alpha (TNF-α) inhibitor) or an interleukin-17 (IL-17) inhibitor.
Sulfasalazine is one medication that can be helpful to some people with severe disease. It is known to effectively control not only pain and joint swelling from arthritis of the small joints, but also the intestinal lesions in inflammatory bowel disease. It comes in tablet form and is taken orally. Sulfasalazine is generally not utilized for spinal arthritis. Side effects are relatively infrequent, but can include headaches, abdominal bloating, nausea, and oral ulcers. Rarely, someone being prescribed this medication can develop bone marrow suppression, which is why it is important for your doctor to regularly monitor your blood count.
Methotrexate was originally developed to treat cancer, this chemotherapy drug is widely used and often very effective for the treatment of rheumatoid arthritis. When prescribed for treating symptoms of spondyloarthritis, it is given in smaller doses and is generally not utilized for spinal arthritis. Methotrexate can either be taken via a self-injectable shot or orally in tablet form. When taking methotrexate, it is also necessary to take the vitamin folic acid in order to help suppress some of the possible side effects, including oral ulcers and nausea. Because of other potential serious side effects, frequent monitoring of blood counts and liver function are required. Methotrexate is strongly contraindicated in pregnant women, as it has caused birth defects and death in unborn babies.
Tumor necrosis factor blocker (TNF inhibitor) or an interleukin-17 (IL-17) inhibitor are injected under the skin or through an intravenous line. A serious and well known complication of the TNF inhibitors is an increased frequency of infections, along with a reduced ability to fight infections, including tuberculosis (TB). Thus, a TB test is required before starting any of the TNF therapies. There is also a slightly increased risk of certain cancers associated with TNF inhibitors, such as lymphoma (most notably in children and teens) and skin cancers.
Examples of tumor necrosis factor (TNF) inhibitors include:
- Adalimumab (Humira)
- Certolizumab pegol (Cimzia)
- Etanercept (Enbrel)
- Golimumab (Simponi)
- Infliximab (Remicade)
IL-17 inhibitors used to treat ankylosing spondylitis include secukinumab (Cosentyx) and ixekizumab (Taltz). IL-17 inhibitors carry similar risks of infections, and reduced ability to fight infections as the TNF inhibitors. They have also shown in clinical trials to exacerbate inflammatory bowel disease in patients who have it, as well as bring on new cases of inflammatory bowel disease.
Both interleukin-17 (IL-17) and tumor necrosis factor alpha (TNF-α) are inflammatory cytokines (cell signaling molecules) that, as the name implies, signal to activate inflammation throughout the body, modulating or altering the immune system response. Inflammatory cytokines play an important role; however, when there is an overabundance of these, as has been described in inflammatory disease, they can cause harm to the body if left unchecked.
IL-17 and TNF-α cytokines signal to specific immune cells directing them to activate inflammation, with each cytokine being responsible for signaling to a different set of cells. IL-17 and TNF inhibitor medications work by targeting their respective cytokines, obstructing their signaling pathways, and by this mechanism seek to reduce inflammation. Since IL-17 inhibitors target different cytokines than the TNF inhibitors, the hope is that this newer class of biologic medications will help those who haven’t responded well to the TNF inhibitors, or are not able to tolerate them.
Janus kinase (JAK) inhibitors also known as JAKi, are the latest class of synthetic (non-biologic) disease-modifying anti-rheumatic drugs (DMARDs) that have been proven effective in the treatment of multiple forms of arthritis, including psoriatic arthritis and ankylosing spondylitis 23. Two janus kinase (JAK) inhibitors are FDA-approved for ankylosing spondylitis and for psoriatic arthritis: tofacitinib (Xeljanz or Xeljanz XR) and upadacitinib (Rinvoq). These medications are taken orally as pills, as opposed to biologics, which are injectable.
JAK inhibitors specifically target the JAK family of enzymes, namely JAK1, JAK2, JAK3, and tyrosine kinase 2 (TYK2), each of which are involved in the initiation of the signal for a cell to make more than 60 different cytokines and growth factors.
Unlike biologics, which inhibit the effects of one single cytokine, JAKi can block the effects of multiple cytokines that are implicated in the pathogenesis (development) of many immune-mediated rheumatic diseases, including ankylosing spondylitis. They have a shorter half-life compared to biologics, meaning they are active in the body for less time, which means if they are discontinued, any side effects will disappear in a quicker fashion.
Figure 8. Summary of the main recommendations for the treatment of patients with ankylosing spondylitis
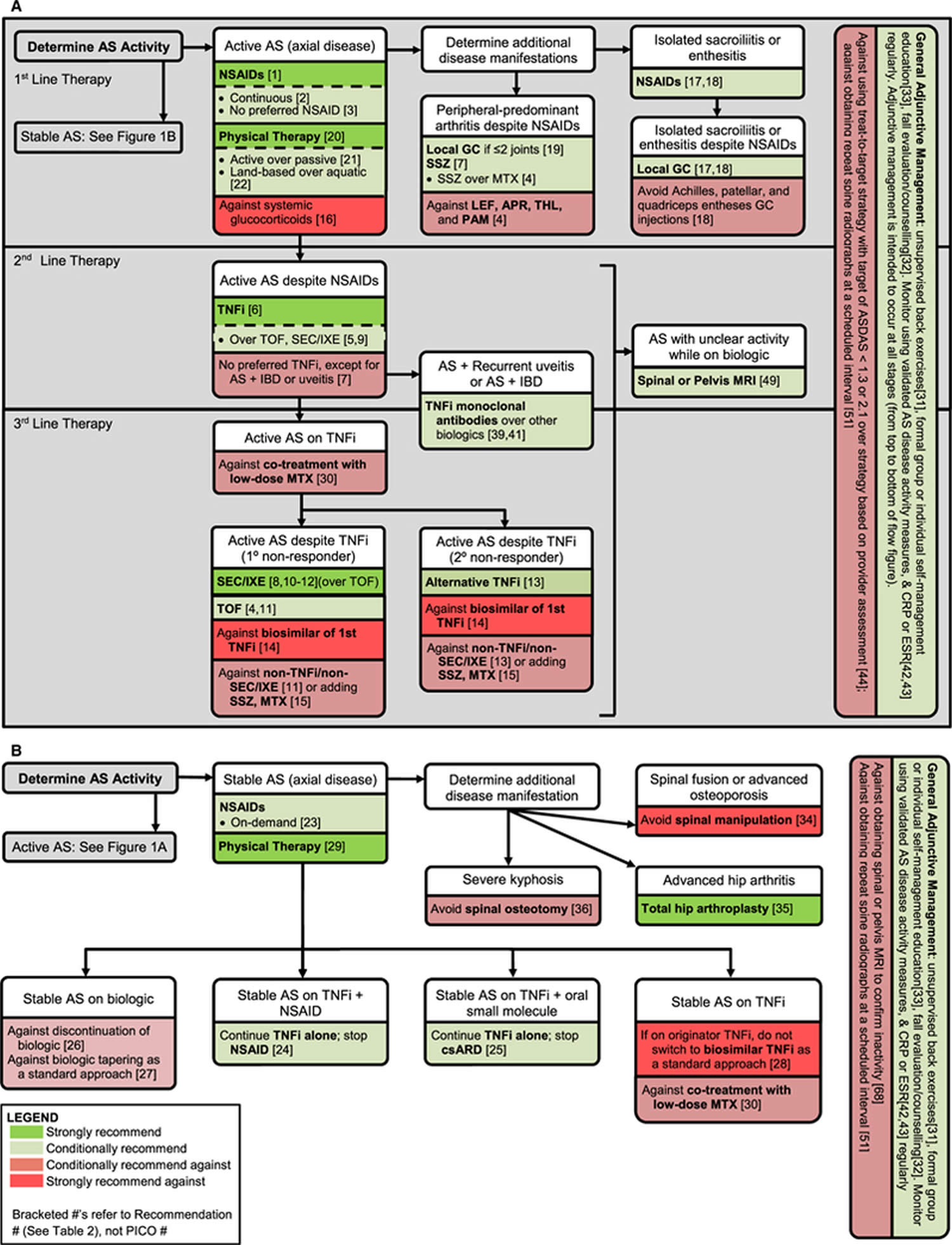
Footnotes: Summary of the main recommendations for the treatment of patients with (A) active ankylosing spondylitis and (B) stable ankylosing spondylitis.
Abbreviations: AS = ankylosing spondylitis; NSAIDs = nonsteroidal antiinflammatory drugs; GC = glucocorticoid; SSZ = sulfasalazine; MTX = methotrexate; LEF = leflunomide; APR = apremilast; THL = thalidomide; PAM = pamidronate; TNFi = tumor necrosis factor inhibitor; TOF = tofacitinib; SEC = secukinumab; IXE = ixekizumab; IBD = inflammatory bowel disease; csARD = conventional synthetic antirheumatic drugs; ESR = erythrocyte sedimentation rate; CRP = C-reactive protein level; ASDAS = Ankylosing Spondylitis Disease Activity Score; MRI = magnetic resonance imaging; PICO = population, intervention, comparison, and outcomes.
[Source 24 ]Active ankylosing spondylitis treatment recommendations
In 2019, the American College of Rheumatology (ACR), Spondylitis Association of America (SAA), and Spondyloarthritis Research and Treatment Network (SPARTAN) published updated recommendations for the treatment of adults with ankylosing spondylitis and those with nonradiographic axial spondyloarthritis 24. Recommendations were provided for pharmacologic treatment, rehabilitation, use of surgery, management of selected comorbidities, disease monitoring, patient education, and preventive care. The recommendations were tailored to patients with either active or stable ankylosing spondylitis disease and focused on the most common decisions confronting clinicians when treating these patients 4. But you are unique, and there is no replacement for working with your doctor to design the best plan for you.
In adults with active ankylosing spondylitis, the expert committee conditionally recommend continuous treatment with nonsteroidal anti-inflammatory drugs (NSAIDs) over on-demand treatment with NSAIDs 24. The efficacy of NSAIDs for symptom improvement in active ankylosing spondylitis has been established in many controlled trials. Evidence that continuous NSAID use results in less spinal fusion on radiographs over 2 years compared to on-demand NSAID use is inconsistent, with results of one trial of celecoxib suggesting less progression with continuous use, and one trial of diclofenac indicating no difference in progression 25. Despite the uncertainty regarding potential disease-modifying effects, the committee conditionally favored continuous use of NSAIDs in patients with active ankylosing spondylitis, primarily for controlling disease activity 24. The decision to use NSAIDs continuously may vary depending on the severity of symptoms, patient preferences, and comorbidities, particularly gastrointestinal and kidney comorbidities, and cardiovascular disease 24.
In adults with active ankylosing spondylitis despite treatment with NSAIDs, the expert committee conditionally recommend treatment with sulfasalazine, methotrexate, or tofacitinib over no treatment with these medications 24. Sulfasalazine or methotrexate should be considered only in patients with prominent peripheral arthritis or when tumor necrosis factor (TNF) inhibitors are not available.
Treatment with sulfasalazine is recommended primarily for patients with prominent peripheral arthritis and few or no axial skeleton symptoms. However, TNF inhibitors may provide a better option for these patients. Evidence for the efficacy of sulfasalazine is based on 8 older controlled trials that showed benefit for peripheral arthritis 24. Although a recent placebo-controlled trial of sulfasalazine demonstrated improvement in spine skeleton symptoms, and modest clinical and imaging responses were seen in a second trial, the preponderance of evidence indicates that sulfasalazine has little benefit for axial skeleton symptoms 26, 27. Sulfasalazine may have a role in treating patients who have contraindications to TNF inhibitor, those who decline treatment with TNF inhibitor or those with limited access to TNF inhibitor.
Three negative trials of methotrexate tested doses of 10 mg or less weekly, and the lack of benefit may reflect the low doses used 28, 29, 30. One uncontrolled study of methotrexate 20 mg weekly showed no improvement in axial skeleton symptoms, but a decrease in swollen joint count 31. Treatment with methotrexate may be considered for patients with predominately peripheral arthritis, although among non-biologics, there is more evidence supporting the use of sulfasalazine.
A phase 2 study of tofacitinib showed benefit in both clinical and imaging outcomes of axial skeleton disease over 12 weeks 32. Use of tofacitinib could be another option, although the results of phase 3 trials are not available. Leflunomide, apremilast, thalidomide, and pamidronate are not recommended 24.
In adults with active ankylosing spondylitis despite treatment with NSAIDs, the expert committee strongly recommend treatment with TNF inhibitor over no treatment with TNF inhibitor.
In adults with active ankylosing spondylitis despite treatment with NSAIDs, the expert committee do not recommend any particular TNF inhibitor as the preferred choice 24.
The efficacy of TNF inhibitor in patients with active ankylosing spondylitis has been demonstrated in 24 randomized controlled trials, most of which were short-term (6 months or shorter) placebo-controlled studies 24. Improvements were shown in patient-reported outcomes, composite response criteria, and spine and sacroiliac inflammation on magnetic resonance imaging (MRI). The expert panel judged that the evidence justified a strong recommendation for use of TNF inhibitor, in patients whose ankylosing spondylitis remained active despite treatment with NSAIDs. The panel recommended that lack of response (or intolerance) to at least 2 different NSAIDs at maximal doses over 1 month, or incomplete responses to at least 2 different NSAIDs over 2 months, would be adequate trials with which to judge NSAID responsiveness prior to escalating to treatment with TNF inhibitor.
Indirect comparisons in network meta-analyses of clinical trials have not showed clinically meaningful differences in short-term efficacy among TNF inhibitor in the treatment of active ankylosing spondylitis 33. Direct comparisons among these medications are limited to a trial of infliximab versus its biosimilar, and a very small open-label trial of infliximab versus etanercept 34. The expert panel judged that the evidence did not support preference of 1 TNF inhibitor over any other for the typical patient. Important exceptions apply to patients with recurrent uveitis or coexistent inflammatory bowel disease (IBD) 24. Patients treated with infliximab may have increased risks of tuberculosis and of infections generally 35. TNF inhibitor other than infliximab should be considered for patients at higher risk of tuberculosis exposure (either through travel or household contacts) or with a history of recurrent infections. Patient preferences regarding the frequency of dosing and route of administration should be weighed when selecting a specific TNF inhibitor.
In adults with active ankylosing spondylitis despite treatment with NSAIDs, the expert committee strongly recommend treatment with secukinumab or ixekizumab over no treatment with secukinumab or ixekizumab 24.
In adults with active ankylosing spondylitis despite treatment with NSAIDs, the expert committee conditionally recommend treatment with TNF inhibitor over treatment with secukinumab or ixekizumab 24.
In adults with active ankylosing spondylitis despite treatment with NSAIDs, the expert committee conditionally recommend treatment with TNF inhibitor over treatment with tofacitinib 24.
In adults with active ankylosing spondylitis despite treatment with NSAIDs, the expert committee conditionally recommend treatment with secukinumab or ixekizumab over treatment with tofacitinib 24.
The use of secukinumab and ixekizumab in patients with active ankylosing spondylitis is supported by data from large placebo-controlled trials 24. The expert panel recommended use of TNF inhibitor over secukinumab or ixekizumab based on greater experience with TNF inhibitor and familiarity with their long-term safety and toxicity. Similarly, the panel judged that TNF inhibitor, secukinumab or ixekizumab should be used over tofacitinib, given their larger evidence base. In patients with coexisting ulcerative colitis, if treatment with TNF inhibitor is not an option, tofacitinib should be considered over secukinumab or ixekizumab. Interleukin-17 (IL-17) inhibitors have not been shown to be efficacious in inflammatory bowel disease (IBD), although tofacitinib is an approved treatment for ulcerative colitis 36.
In adults with active ankylosing spondylitis despite treatment with NSAIDs and who have contraindications to TNF inhibitor, the expert committee conditionally recommend treatment with secukinumab or ixekizumab over treatment with sulfasalazine, methotrexate, or tofacitinib 24.
No studies have directly compared the risks and benefits of treatment alternatives in patients who have contraindications to treatment with TNF inhibitor. The expert panel favored treatment with secukinumab or ixekizumab over treatment with sulfasalazine or methotrexate based on a higher likelihood of benefit, but this recommendation was conditional on the specific contraindication. If the contraindication to TNF inhibitor use was the presence of congestive heart failure or demyelinating disease, secukinumab or ixekizumab was preferred, since these medications have not been shown to worsen these conditions. If the contraindication to TNF inhibitor use was tuberculosis, other chronic infection, or a high risk of recurrent infections, sulfasalazine was preferred over secukinumab, izekizumab, and tofacitinib. In these cases, efforts to mitigate the infectious contraindications should be undertaken so that TNF inhibitor might safely be used. Treatment with rituximab, abatacept, ustekinumab, or interleukin-6 inhibitors is not recommended, even in patients with contraindications to TNF inhibitor, due to lack of effectiveness.
In adults with active ankylosing spondylitis despite treatment with the first TNF inhibitor used, the expert committee conditionally recommend treatment with secukinumab or ixekizumab over treatment with a different TNF inhibitor in patients with primary non-response to TNF inhibitor 24.
In adults with active ankylosing spondylitis despite treatment with the first TNF inhibitor used, the expert committee conditionally recommend treatment with a different TNF inhibitor over treatment with a non-TNFi biologic in patients with secondary non-response to TNF inhibitor 24.
In adults with active ankylosing spondylitis despite treatment with the first TNF inhibitor used, the expert committee strongly recommend against switching to treatment with a biosimilar of the first TNF inhibitor 24.
In adults with active ankylosing spondylitis despite treatment with the first TNF inhibitor used, the expert committee conditionally recommend against the addition of sulfasalazine or methotrexate in favor of switching to a new biologic 24.
Direct comparisons of treatment strategies for patients who do not have or sustain adequate responses to their first TNF inhibitor have not been reported, and the recommendations are based on the panel’s consideration of indirect comparisons among the available treatment options 24. Data from observational studies suggest that 25–40% of patients who switch from one TNF inhibitor to another will have a meaningful response (e.g., 50% improvement in Bath Ankylosing Spondylitis Disease Activity Index) to the second TNF inhibitor 37. However, not all patients in these studies switched TNF inhibitor because of ineffectiveness.
The panel judged that treatment should differ for patients who had a primary non-response to TNF inhibitor and those with secondary non-response to TNF inhibitor. Switching to secukinumab or ixekizumab was recommended in most patients who had a primary non-response to the first TNF inhibitor, under the assumption that TNF was not the key inflammatory mediator in these patients. Continuing treatment with the first TNF inhibitor could be considered if additional time was believed important to assess the response fully, or if a higher dose or shorter dosing interval was thought to be beneficial.
In patients who relapse after an initial response (i.e., secondary non-response), the expert panel judged that treatment with a different TNF inhibitor held a reasonable prospect of benefit and should be used in most patients, rather than immediately switching to a different class of biologics. Although ixekizumab is efficacious among TNF inhibitor non-responders, trials have not directly compared responses to ixekizumab (or secukinumab) to responses to a second TNF inhibitor in patients with a secondary non-response to the first TNF inhibitor 38. Given that options for biologics are limited, treatment with a second TNF inhibitor was recommended in these patients.
In cases of non-response (primary or secondary), the panel recommended against switching to the biosimilar of the first TNF inhibitor (e.g., switching from originator infliximab to infliximab-dyyb), as the clinical response would not be expected to be different. The expert panel also recommended against the addition of sulfasalazine or methotrexate to TNF inhibitor in cases of non-response to TNF inhibitor, judging any benefit would likely be marginal. The addition of sulfasalazine could be considered in the rare patient whose axial skeleton symptoms are well-controlled on TNF inhibitor but who has active peripheral arthritis.
In adults with either active or stable ankylosing spondylitis on treatment with TNF inhibitor, the expert committee conditionally recommend against co-treatment with low-dose methotrexate 24.
In rheumatoid arthritis, the likelihood of TNF inhibitor discontinuation is lower among patients who receive co-treatment with methotrexate, perhaps by reducing the development of antidrug antibodies 39. In ankylosing spondylitis, it is less clear whether the duration of TNF inhibitor use, and by inference their effectiveness, is similarly prolonged 40. Data from observational studies are conflicting, although some studies, primarily of infliximab, showed longer TNF inhibitor treatment when methotrexate was co-administered. Clinical responses were not greater among patients who received co-treatment with methotrexate. In the absence of convincing evidence of benefit, and due to greater burden for patients, the panel recommended against routine co-administration of methotrexate with TNF inhibitor, although its use could be considered in patients treated with infliximab.
Stable ankylosing spondylitis treatment recommendations
In adults with stable ankylosing spondylitis the expert committee conditionally recommend on-demand treatment with NSAIDs over continuous treatment with NSAIDs 24. This recommendation applies to patients who have been stable while not receiving any pharmacologic treatment. In this group, the expert panel considered that the potential toxicities of continuous NSAID treatment outweighed the uncertain benefit of less radiographic progression. On-demand treatment should be considered for short-term symptom recurrences (flares).
In adults with stable ankylosing spondylitis receiving treatment with TNF inhibitor and NSAIDs, the expert committee conditionally recommend continuing treatment with TNF inhibitor alone over continuing both medications 24.
In adults with stable ankylosing spondylitis receiving treatment with TNF inhibitor and a conventional synthetic antirheumatic drug, the expert committee conditionally recommend continuing treatment with TNF inhibitor alone over continuing both medications 24.
No new studies have directly compared outcomes between patients who continued combination treatment and those who discontinued either NSAIDs or a conventional synthetic antirheumatic drug. The NSAID-sparing potential of etanercept was demonstrated in a recent trial 41. The expert panel judged these recommendations primarily based on symptom control, rather than on any potential effect of combination therapy on future spinal fusion. In stable patients, a trial of withdrawing either the NSAIDs or the conventional synthetic antirheumatic drug should be considered, due to the likelihood of greater toxicity with the long-term use of more than one medication. However, on-demand NSAID treatment for control of intermittent symptoms is recommended for patients with good responses to previous courses of NSAIDs.
In adults with stable ankylosing spondylitis receiving treatment with a biologic, the expert committee conditionally recommend against discontinuation of the biologic 24.
In adults with stable ankylosing spondylitis receiving treatment with a biologic, the expert committee conditionally recommend against tapering of the biologic dose as a standard approach 24.
Data from several observational studies suggest that discontinuation of TNF inhibitor after achieving either remission or low disease activity results in relapses in 60–74% of patients, occasionally within a few weeks to months of discontinuation 24. Although the data only concerned TNF inhibitor discontinuation, the expert panel judged that a similar recommendation would also apply to other biologics. In general, treatment with a biologic should be planned to be continued long-term, barring toxicities. Discontinuation might be considered in patients in sustained remission (i.e., several years), with the anticipation that only one-third of patients would not relapse. Patient preferences should help guide this decision.
Tapering of TNF inhibitor could entail a change in either the dose or frequency of administration. Two controlled unblinded trials of tapering etanercept to 25 mg weekly versus maintaining the dose at 50 mg weekly in patients with stable ankylosing spondylitis showed that remission or partial remission was somewhat less likely among those in whom etanercept was tapered 42, 43. In small observational studies, 53–70% of patients were still receiving their reduced dose at 2 years, but there is little evidence regarding maintenance of long-term remission after tapering of TNF inhibitor 24. Therefore, the expert panel recommended against tapering of biologics as a standard approach. One condition in which tapering could be considered would be in patients with prolonged stable ankylosing spondylitis, if the patient and provider engage in shared decision-making.
In adults with stable ankylosing spondylitis receiving an originator TNF inhibitor, the expert committee strongly recommend continuing treatment with the originator TNF inhibitor over mandated switching to its biosimilar 24.
While the efficacy of originator and biosimilar TNF inhibitor is comparable, and although either could be chosen to initiate new courses of TNF inhibitor treatment, it was the opinion of the expert panel to recommend against mandated switching to a biosimilar during the course of treatment, in the absence of evidence of interchangability. Medication changes can increase the risk of destabilizing a patient, and the panel judged that additional data were needed to understand the frequency of potential problems and concerns associated with switching patients who were stable on an originator TNF inhibitor to its biosimilar. Given these concerns, the expert panel judged that there should be a compelling rationale for switching medications, particularly in light of the marginal cost savings apparent for US patients 44.
In adults with ankylosing spondylitis and recurrent uveitis, the expert committee conditionally recommend treatment with TNF inhibitor monoclonal antibodies over treatment with other biologics 24.
Evidence for this recommendation is limited to indirect comparisons of the rates of acute uveitis episodes in clinical trials or observational studies, rather from direct comparisons 24. Many studies showed overall rates of uveitis without separately showing recurrences as opposed to incident episodes 45. The rates were generally lower for adalimumab and infliximab compared to etanercept. For example, a large observational study reported rates of uveitis (per 100 patient-years) in patients receiving adalimumab, infliximab, and etanercept of 13.6, 27.5, and 60.3, respectively, compared to pre-treatment rates of 36.8, 45.5, and 41.6, respectively 46. Adalimumab or infliximab are preferred over etanercept for the treatment of ankylosing spondylitis in patients with recurrent uveitis. Certolizumab or golimumab may also be considered, although supporting data are less substantial 47. Data from clinical trials suggest that rates of uveitis flares were not different between patients with ankylosing spondylitis treated with secukinumab and those treated with placebo, but more evidence is needed. Secukinumab was not efficacious in the treatment of panuveitis or posterior uveitis 48. Rates of uveitis flares among patients treated with ixekizumab have not been well-defined.
In adults with ankylosing spondylitis and inflammatory bowel disease (IBD), the expert committee conditionally recommend treatment with TNF inhibitor monoclonal antibodies over treatment with other biologics 24.
This recommendation was based on limited indirect evidence on the risks of flares or new onset of inflammatory bowel disease (IBD) among patients with ankylosing spondylitis during treatment with biologics, and the much larger literature on the treatment of IBD in general. Patients with ankylosing spondylitis treated with infliximab or adalimumab have lower risks of IBD exacerbations than those treated with etanercept 24. Infliximab, adalimumab, and certolizumab are approved for the treatment of Crohn’s disease, and infliximab, adalimumab, and golimumab are approved for the treatment of ulcerative colitis, while etanercept is not approved for either condition 49. This evidence is the basis for the recommendation favoring TNF inhibitor monoclonal antibody use in patients with ankylosing spondylitis and coexisting IBD. The choice of the particular TNF inhibitor monoclonal antibody should be made in consultation with the patient’s gastroenterologist. Secukinumab has been associated with the new onset, or exacerbation, of Crohn’s disease 50. Increased risks of IBD exacerbation appear to also occur with ixekizumab 51.
Ankylosing spondylitis exercise
Physical therapy is an important part of treatment and can provide a number of benefits, from pain relief to improved strength and flexibility. A physical therapist can design specific exercises for your needs. Taking regular exercise – 150 minutes of exercise a week can greatly increase your health.
Range-of-motion and stretching exercises can help maintain flexibility in your joints and preserve good posture. Proper sleep and walking positions and abdominal and back exercises can help maintain your upright posture.
Mobility exercises
The mobility section consists of exercises that slowly move the different parts of the spine to the limit of their movement. This is the most important section for keeping the spine mobile. Physical therapist recommend that you do these exercises every day.
Flexibility exercises
These exercises stretch the large muscle groups such as the hamstrings and quadriceps that are anchored around the spine. It is important that these muscles do not shorten or the spine be pulled into wrong positions. We recommend that you do these exercises every day.
Breathing exercises
These exercises are designed to maximize the volume of the chest and lungs. We recommend that you do these every day.
Physical therapy
At all stages of ankylosing spondylitis, physical therapy and exercise can be very beneficial in reducing symptoms and maintaining the flexibility in the spine. Physical therapy can provide a number of benefits, from pain relief to improved strength and flexibility. A physical therapist can design specific exercises for your needs. To help preserve good posture, you may be taught:
- Range-of-motion and stretching exercises
- Strengthening exercises for abdominal and back muscles
- Proper sleeping and walking positions
Lifestyle and home remedies
Lifestyle choices can also help manage ankylosing spondylitis.
- Stay active. Exercise can help ease pain, maintain flexibility and improve your posture. For those with ankylosing spondylitis, regular exercise can help improve posture, stiffness, pain, fatigue, breathing capacity, and therefore overall function. Remember that it is your doctor’s job to help control the pain, inflammation and stiffness so that you can maintain a healthy exercise program. It is often difficult to exercise or participate in physical activity if pain persists due to active inflammation. A good treatment plan must include exercise/physical activity. A physical therapist can help you craft an individualized stretching and strengthening program to fit specific needs.
- There are 4 main types of exercises recommended:
- Range of motion or stretching exercises. These exercises are done without weights to move the muscles and joints through their full range of motion. Range of motion exercises improve flexibility and reduce stiffness, swelling, and pain, as well as minimize the risk of fusion. These are often done as warm up exercises before sports. Range of motion or stretching exercises are critical in spondyloarthritis because people tend to limit movement and use of an area when there is pain, swelling, and/or stiffness around a joint, such as when there is active inflammation. Lack of movement can lead to loss of mobility and increase the risk of fusion of the joints. In addition, when a joint is inflamed, surrounding muscles tighten to control motion, resulting in even more stiffness and pain. Therefore, it is recommended that range of motion or stretching exercises be done daily for all joints that are stiff or that have the potential for becoming stiff.
- Aerobic or cardiovascular exercise. This exercise consists of activities performed for a sustained period of time that increase blood flow through the heart. Aerobic exercise improves heart and lung function and overall health. Studies show that people with spondyloarthritis who do aerobic exercise have better breathing function, endurance, and mood, and less disease activity, pain and fatigue than people who do not exercise. The current aerobic exercise recommendations include performing aerobic exercise between 3 to 5 times per week for a total of 75 to 150 minutes per week.
- Strengthening exercises. These exercises use your muscles to move or hold against a weight or resistance. Strengthening exercises improve the performance of muscles that help you move efficiently and safely and support good posture. Some of the most important muscles to strengthen in spondyloarthritis are the “core muscles,” which are the abdominal and back muscles that act like a “corset” to support the spine. Having strong core muscles has been shown to reduce stress in the spine and therefore can minimize back pain. It is common for a person who has back pain from spondyloarthritis to change their posture to ease the pain. Over time, these postural changes may lead to stiffness and weakness of the muscles and joints, and more pain. As such, “core strengthening” is key to managing back pain in spondyloarthritis. Strengthening exercises should be performed 2 to 4 times per week for best results.
- Balance exercises. Focus on improving your stability when you are still and moving. These exercises are especially important for people who are less active and as we age. Balance exercises can help reduce the chances of falling, which is especially important for people with lower bone density, and thus at greater risk for fracture during a fall. Balance exercises should be performed 3 to 5 times per week for best results.
- An ideal exercise program will incorporate each of the types of exercise noted above. Consistently performing a program that addresses flexibility, aerobic conditioning, strength and balance for 20 minutes a day has been shown to significantly improve pain, stiffness, fatigue, function, and mood. By working with your physician and physical therapist, you can set realistic goals for yourself, choose exercises/physical activities that are safe and enjoyable, and stay with the program that optimizes your health.
- There are 4 main types of exercises recommended:
- Maintaining a healthy weight. Besides the well-known medical problems individuals can develop as a result of weight gain (high blood pressure, diabetes, cancer, stroke, and heart disease), extra weight puts additional stress on joints and bones. For example, the corticosteroid prednisone causes weight gain to some degree in nearly all patients who take the medication and can lead to redistribution of body fat to places like the face, back of the neck, and abdomen. On the other hand, underweight people can suffer from medical problems, ranging from chronic fatigue and anemia to lowered resistance to infection and clinical depression. Inflammation, certain medications, and depression associated with a chronic illness may lessen your appetite or upset your stomach, making it difficult for some people with spondylitis to maintain a healthy weight. This is especially true for those who have spondylitis with inflammatory bowel disease or Crohn’s disease who experience gastrointestinal problems on top of arthritis symptoms. Any severe weight loss to should be reported to your doctor.
- Don’t smoke. If you smoke, quit. Smoking is generally bad for your health, but it creates additional problems for people with ankylosing spondylitis, including further hampering breathing.
- Practice good posture. Practicing standing straight in front of a mirror can help you avoid some of the problems associated with ankylosing spondylitis.
Complementary and alternative medicine
Although there has been no rigorous scientific evidence to support the use of complementary and alternative medicine (CAM) by people with ankylosing spondylitis and its related diseases, some patients have benefited from such treatments.
- Chiropractic treatment. Some people with spondylitis swear by regular chiropractic sessions.
- Acupuncture. The exact way in which acupuncture works on the body remains unclear, but stimulation of acupuncture points by puncturing the skin with hair-thin needles may lead to release by the brain and spinal cord of opium-like molecules that help relieve pain. Some research suggests that acupuncture relieves pain in some people, and is safe if performed by a trained professional using sterile or disposable needles. More scientific studies are underway to help determine its effect on various forms of arthritis.
- Yoga. Yoga has been practiced for more than 5,000 years and can greatly benefit people with spondylitis under the instruction of a knowledgeable instructor who can tailor the program to the individual.
- Massage. Many people with spondylitis find therapeutic massage very helpful. If done carefully, it can be a beneficial tool for pain relief and stress reduction. If a massage therapist is aware of a person’s spondylitis and understands the disease and any potential manipulation issues, gentle massage can help promote well-being. It may provide temporary relief of pain or stiffness and, in some cases, improve flexibility because of increased blood circulation. However, some people with spondylitis, however, cannot tolerate the procedure due to increased pain as a result of the massage. Others attribute massage as a trigger for disease flare-ups.
Be sure to talk to your doctor about whether the medications you take affect your diet and if a vitamin supplement would be useful in your situation.
Researchers have found that patients who take folic acid or folinic acid supplements along with the arthritis drug methotrexate are less likely to have a malfunctioning liver than those taking just methotrexate. As a result, patients taking folate supplements are able to continue their drug therapy for longer periods.
Surgery
Most people with ankylosing spondylitis don’t need surgery. Surgery may be recommended if you have severe pain or if a hip joint is so damaged that it needs to be replaced.
When ankylosing spondylitis has been present for some time and the spine has already begun to fuse, braces and physical therapy will do little if anything to reverse the deformity of the spine.
Surgery may be considered when the deformity is:
- Significantly affecting quality of life, for example impacting the ability to work or perform simple tasks like eating.
- Putting you at serious risk, for example, the development of tingling and numbness in the lower limbs may suggest the deformity is now impinging on the spinal cord.
Alternatively, surgery may be necessary when there is a fracture in the spine.
In all the above situations, the aim of surgery is to stabilise the spine in a functional position – not to make it flexible again. The standard surgical option for ankylosing spondylitis is osteotomy or reshaping and trimming of bones. This is usually combined with fusion (lumbar spinal fusion and cervical spinal fusion).
After these operations, you may need to keep your back / neck still for some time as the bones heal over the screws.
Ankylosing spondylitis and other joints
Other joints may be seriously affected by ankylosing spondylitis. The symptoms in joints like the hip and shoulder, feet and knees should also be controlled by medications. When these joints are seriously affected, surgery may be considered. Surgical options may include:
- Hip replacement or hip fusion.
- Shoulder replacement or fusion.
- Arthroscopy and debridement of joints in the feet.
Ankylosing spondylitis diet
Today, magazine articles and web pages bombard us with claims about special diets, foods, or supplements that can cause or cure arthritis. It is appealing to think that there are simple answers to a complicated disease like ankylosing spondylitis, but unfortunately, most claims for cure-all diets or nutritional supplements have not been scientifically tested to determine if they work and if they are safe. Some are outright frauds, while others have undergone scientific studies that are often incomplete and show that they may be harmful instead of beneficial.
In recent years, many specialized diets have gained popularity among some people with arthritis. To date, few of these claims have been substantiated by rigorously controlled studies. That said, some people find that certain foods trigger changes in symptoms, either for the better or the worse. If you find yourself noticing this type of pattern, try keeping a food diary for a few weeks to test if indeed what you eat makes a difference or if you have food sensitivities.
There is, in fact, evidence that certain foods tend to be inflammatory in nature, while others can help manage inflammation.
Whether a person is affected by a chronic illness or not, there are some straightforward guidelines that, if followed, would lead to improved health and well-being for almost everyone:
- Both calcium and alcohol can affect the strength of your bones, and it is a well-known fact that people with spondylitis are already at higher risk for osteoporosis, a dangerous thinning of the bones that can lead to fractures. Following a diet with adequate amounts of calcium and vitamin D will help reduce the risk of osteoporosis. Consuming more than two alcoholic drinks per day increases a person’s chances of developing weakened bones. In addition, alcohol mixed with certain medications can cause serious side effects to the gastrointestinal tract and major organs such as the liver and the kidneys. Since the liver detoxifies (or metabolizes) alcohol, continued and excessive use of alcohol may damage the liver in various ways, including the eventual development of a potentially fatal condition of the liver called cirrhosis. To further complicate things, the presence of alcohol impairs the absorption of essential nutrients because it can damage the lining of the small intestine and the stomach, where most nutrients are digested. Alcohol also requires some vitamins in its metabolism, and it interferes with the absorption and storage of some specific vitamins.
- It is important to find out from your doctor whether any medications that you take affect how your body uses what you eat. For instance, some medications cause a person to retain sodium, while others cause potassium loss. Methotrexate can lower folic acid levels, causing a variety of adverse symptoms that can be offset by taking additional supplements.
Experts agree that there are basic guidelines to good nutrition, which are:
- Eat a variety of healthy foods rich in antioxidants, such as colorful vegetables and fruits.
- Eat foods rich in omega 3 fatty acids, such as salmon, flax seeds, and certain nuts.
- Use fat (especially saturated fat found in animal products), cholesterol, sugar, and salt in moderation.
- Minimized processed foods, fried foods, and other products high in artificial ingredients and preservatives.
- Drink 8 to 10 glasses of water a day.
- Most people receive daily requirements of vitamins and minerals by eating a well-balanced diet, but others need to take vitamin supplements.
Avoid alcohol or foods that can interact with your medication. Talk with your doctor and/or pharmacist about potential interactions.
Maintaining a Healthy Weight
Besides the well-known medical problems individuals can develop as a result of weight gain (high blood pressure, diabetes, cancer, stroke, and heart disease), extra weight puts additional stress on joints and bones. For example, the corticosteroid prednisone causes weight gain to some degree in nearly all patients who take the medication and can lead to redistribution of body fat to places like the face, back of the neck, and abdomen.
On the other hand, underweight people can suffer from medical problems, ranging from chronic fatigue and anemia to lowered resistance to infection and clinical depression. Inflammation, certain medications, and depression associated with a chronic illness may lessen your appetite or upset your stomach, making it difficult for some people with spondylitis to maintain a healthy weight. This is especially true for those who have spondylitis with inflammatory bowel disease or Crohn’s disease who experience gastrointestinal problems on top of arthritis symptoms. Any severe weight loss to should be reported to your doctor.
References- van der Linden S, Valkenburg HA, Cats A. Evaluation of diagnostic criteria for ankylosing spondylitis. A proposal for modification of the New York criteria. Arthritis Rheum. 1984 Apr;27(4):361-8. doi: 10.1002/art.1780270401
- Akkoç N, Yarkan H, Kenar G, Khan MA. Ankylosing Spondylitis: HLA-B*27-Positive Versus HLA-B*27-Negative Disease. Curr Rheumatol Rep. 2017 May;19(5):26. doi: 10.1007/s11926-017-0654-8
- Bittar M, Yong WC, Magrey M, Khan MA. Worldwide Differences in Clinical Phenotype of Axial Spondyloarthritis. Curr Rheumatol Rep. 2021 Sep 29;23(10):76. doi: 10.1007/s11926-021-01043-5
- Ward MM, Deodhar A, Akl EA, Lui A, Ermann J, Gensler LS, Smith JA, Borenstein D, Hiratzka J, Weiss PF, Inman RD, Majithia V, Haroon N, Maksymowych WP, Joyce J, Clark BM, Colbert RA, Figgie MP, Hallegua DS, Prete PE, Rosenbaum JT, Stebulis JA, Van Den Bosch F, Yu DT, Miller ankylosing spondylitis, Reveille JD, Caplan L. American College of Rheumatology/Spondylitis Association of America/Spondyloarthritis Research and Treatment Network 2015 Recommendations for the Treatment of Ankylosing Spondylitis and Nonradiographic Axial Spondyloarthritis. Arthritis Care Res (Hoboken). 2016 Feb;68(2):151-66. doi: 10.1002/acr.22708
- Ankylosing spondylitis. https://radiopaedia.org/cases/ankylosing-spondylitis-67
- Waxenbaum JA, Reddy V, Futterman B. Anatomy, Back, Intervertebral Discs. [Updated 2021 Aug 10]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470583
- Patwardhan A, Havey R, Meade K, Lee B, Dunlap B. A follower load increases the load-carrying capacity of the lumbar spine in compression. Spine 1999;4( 10): 1003-9.
- Roberts S, Evans H, Trivedi J, Menage J. Histology and pathology of the human intervertebral disc. J Bone Joint Surg Am. 2006 Apr;88 Suppl 2:10-4. doi: 10.2106/JBJS.F.00019
- Le DT, Alem N. Facet Joint Injection. [Updated 2022 Jun 27]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK572125
- Raychaudhuri SP, Deodhar A. The classification and diagnostic criteria of ankylosing spondylitis. J Autoimmun. 2014 Feb-Mar;48-49:128-33. doi: 10.1016/j.jaut.2014.01.015
- Iritis. https://www.aapos.org/glossary/iritis
- Levy AR, Szabo SM, Rao SR, Cifaldi M, Maksymowych WP. Estimating the occurrence of renal complications among persons with ankylosing spondylitis. Arthritis Care Res (Hoboken). 2014 Mar;66(3):440-5. https://onlinelibrary.wiley.com/doi/epdf/10.1002/acr.22176
- Dönmez S, Pamuk ÖN, Pamuk GE, Aydoğdu E, Inman R. Secondary amyloidosis in ankylosing spondylitis. Rheumatol Int. 2013 Jul;33(7):1725-9. doi: 10.1007/s00296-012-2646-3
- Mahmoudi M, Garshasbi M, Ashraf-Ganjouei A, Javinani A, Vojdanian M, Saafi M, Ahmadzadeh N, Jamshidi A. Association between rs6759298 and Ankylosing Spondylitis in Iranian Population. Avicenna J Med Biotechnol. 2018 Jul-Sep;10(3):178-182. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6064007
- van den Berg R, Jongbloed EM, de Schepper EIT, Bierma-Zeinstra SMA, Koes BW, Luijsterburg PAJ. The association between pro-inflammatory biomarkers and nonspecific low back pain: a systematic review. Spine J. 2018 Nov;18(11):2140-2151. doi: 10.1016/j.spinee.2018.06.349
- Ankylosing spondylitis. https://medlineplus.gov/genetics/condition/ankylosing-spondylitis
- Aloush V, Dotan I, Ablin JN, Elkayam O. Evaluating IBD-specific antiglycan antibodies in serum of patients with spondyloarthritis and rheumatoid arthritis: are they really specific? Clin Exp Rheumatol. 2019 Jan-Feb;37(1):32-36.
- Rahbar MH, Lee M, Hessabi M, Tahanan A, Brown MA, Learch TJ, Diekman LA, Weisman MH, Reveille JD. Harmonization, data management, and statistical issues related to prospective multicenter studies in Ankylosing spondylitis (AS): Experience from the Prospective Study Of Ankylosing Spondylitis (PSOAS) cohort. Contemp Clin Trials Commun. 2018 Jul 25;11:127-135. doi: 10.1016/j.conctc.2018.07.004
- Reinders A, van Wyk M. Bamboo spine – X-ray findings of ankylosing spondylitis revisited. (2012) South African Journal of Radiology. 16 (3): 111. https://doi.org/10.4102/sajr.v16i3.294
- Sieper J, Rudwaleit M, Baraliakos X, et al. The Assessment of SpondyloArthritis international Society (ASAS) handbook: a guide to assess spondyloarthritis. Annals of the Rheumatic Diseases 2009;68:ii1-ii44. http://dx.doi.org/10.1136/ard.2008.104018
- Wenker KJ, Quint JM. Ankylosing Spondylitis. [Updated 2022 Apr 9]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470173
- Kucybała I, Urbanik A, Wojciechowski W. Radiologic approach to axial spondyloarthritis: where are we now and where are we heading? Rheumatol Int. 2018 Oct;38(10):1753-1762. doi: 10.1007/s00296-018-4130-1
- Medications Used to Treat Ankylosing Spondylitis and Related Diseases. https://spondylitis.org/about-spondylitis/treatment-information/medications
- Ward MM, Deodhar A, Gensler LS, Dubreuil M, Yu D, Khan MA, Haroon N, Borenstein D, Wang R, Biehl A, Fang MA, Louie G, Majithia V, Ng B, Bigham R, Pianin M, Shah AA, Sullivan N, Turgunbaev M, Oristaglio J, Turner A, Maksymowych WP, Caplan L. 2019 Update of the American College of Rheumatology/Spondylitis Association of America/Spondyloarthritis Research and Treatment Network Recommendations for the Treatment of Ankylosing Spondylitis and Nonradiographic Axial Spondyloarthritis. Arthritis Rheumatol. 2019 Oct;71(10):1599-1613. doi: 10.1002/art.41042
- Sieper J, Listing J, Poddubnyy D, Song IH, Hermann KG, Callhoff J, Syrbe U, Braun J, Rudwaleit M. Effect of continuous versus on-demand treatment of ankylosing spondylitis with diclofenac over 2 years on radiographic progression of the spine: results from a randomised multicentre trial (ENRADAS). Ann Rheum Dis. 2016 Aug;75(8):1438-43. doi: 10.1136/annrheumdis-2015-207897
- Khanna Sharma S, Kadiyala V, Naidu G, Dhir V. A randomized controlled trial to study the efficacy of sulfasalazine for axial disease in ankylosing spondylitis. Int J Rheum Dis. 2018 Jan;21(1):308-314. doi: 10.1111/1756-185X.13124
- Song IH, Hermann K, Haibel H, Althoff CE, Listing J, Burmester G, Krause A, Bohl-Bühler M, Freundlich B, Rudwaleit M, Sieper J. Effects of etanercept versus sulfasalazine in early axial spondyloarthritis on active inflammatory lesions as detected by whole-body MRI (ESTHER): a 48-week randomised controlled trial. Ann Rheum Dis. 2011 Apr;70(4):590-6. doi: 10.1136/ard.2010.139667. Erratum in: Ann Rheum Dis. 2011 Jul;70(7):1350. Althoff, Ce [corrected to Althoff, C E].
- Altan L, Bingöl U, Karakoç Y, Aydiner S, Yurtkuran M, Yurtkuran M. Clinical investigation of methotrexate in the treatment of ankylosing spondylitis. Scand J Rheumatol. 2001;30(5):255-9. doi: 10.1080/030097401753180318. Erratum in: Scand J Rheumatol. 2003;32(6):380.
- Roychowdhury B, Bintley-Bagot S, Bulgen DY, Thompson RN, Tunn EJ, Moots RJ. Is methotrexate effective in ankylosing spondylitis? Rheumatology (Oxford). 2002 Nov;41(11):1330-2. doi: 10.1093/rheumatology/41.11.1330
- Gonzalez-Lopez L, Garcia-Gonzalez A, Vazquez-Del-Mercado M, Muñoz-Valle JF, Gamez-Nava JI. Efficacy of methotrexate in ankylosing spondylitis: a randomized, double blind, placebo controlled trial. J Rheumatol. 2004 Aug;31(8):1568-74.
- Haibel H, Brandt HC, Song IH, Brandt A, Listing J, Rudwaleit M, Sieper J. No efficacy of subcutaneous methotrexate in active ankylosing spondylitis: a 16-week open-label trial. Ann Rheum Dis. 2007 Mar;66(3):419-21. doi: 10.1136/ard.2006.054098
- van der Heijde D, Deodhar A, Wei JC, Drescher E, Fleishaker D, Hendrikx T, Li D, Menon S, Kanik KS. Tofacitinib in patients with ankylosing spondylitis: a phase II, 16-week, randomised, placebo-controlled, dose-ranging study. Ann Rheum Dis. 2017 Aug;76(8):1340-1347. doi: 10.1136/annrheumdis-2016-210322
- Wang R, Dasgupta A, Ward MM. Comparative Efficacy of Tumor Necrosis Factor-α Inhibitors in Ankylosing Spondylitis: A Systematic Review and Bayesian Network Metaanalysis. J Rheumatol. 2018 Apr;45(4):481-490. doi: 10.3899/jrheum.170224
- Park W, Hrycaj P, Jeka S, Kovalenko V, Lysenko G, Miranda P, Mikazane H, Gutierrez-Ureña S, Lim M, Lee YA, Lee SJ, Kim H, Yoo DH, Braun J. A randomised, double-blind, multicentre, parallel-group, prospective study comparing the pharmacokinetics, safety, and efficacy of CT-P13 and innovator infliximab in patients with ankylosing spondylitis: the PLANETAS study. Ann Rheum Dis. 2013 Oct;72(10):1605-12. doi: 10.1136/annrheumdis-2012-203091
- Yun H, Xie F, Delzell E, Chen L, Levitan EB, Lewis JD, Saag KG, Beukelman T, Winthrop K, Baddley JW, Curtis JR. Risk of hospitalised infection in rheumatoid arthritis patients receiving biologics following a previous infection while on treatment with anti-TNF therapy. Ann Rheum Dis. 2015 Jun;74(6):1065-71. doi: 10.1136/annrheumdis-2013-204011
- Sandborn WJ, Su C, Sands BE, D’Haens GR, Vermeire S, Schreiber S, Danese S, Feagan BG, Reinisch W, Niezychowski W, Friedman G, Lawendy N, Yu D, Woodworth D, Mukherjee A, Zhang H, Healey P, Panés J; OCTAVE Induction 1, OCTAVE Induction 2, and OCTAVE Sustain Investigators. Tofacitinib as Induction and Maintenance Therapy for Ulcerative Colitis. N Engl J Med. 2017 May 4;376(18):1723-1736. doi: 10.1056/NEJMoa1606910
- Ciurea A, Exer P, Weber U, Tamborrini G, Steininger B, Kissling RO, Bernhard J, Scherer A; Rheumatologists of Swiss Clinical Quality Management Program for Axial Spondyloarthritis. Does the reason for discontinuation of a first TNF inhibitor influence the effectiveness of a second TNF inhibitor in axial spondyloarthritis? Results from the Swiss Clinical Quality Management Cohort. Arthritis Res Ther. 2016 Mar 22;18:71. doi: 10.1186/s13075-016-0969-2
- Deodhar A, Poddubnyy D, Pacheco-Tena C, Salvarani C, Lespessailles E, Rahman P, Järvinen P, Sanchez-Burson J, Gaffney K, Lee EB, Krishnan E, Santisteban S, Li X, Zhao F, Carlier H, Reveille JD; COAST-W Study Group. Efficacy and Safety of Ixekizumab in the Treatment of Radiographic Axial Spondyloarthritis: Sixteen-Week Results From a Phase III Randomized, Double-Blind, Placebo-Controlled Trial in Patients With Prior Inadequate Response to or Intolerance of Tumor Necrosis Factor Inhibitors. Arthritis Rheumatol. 2019 Apr;71(4):599-611. doi: 10.1002/art.40753
- Souto A, Maneiro JR, Gómez-Reino JJ. Rate of discontinuation and drug survival of biologic therapies in rheumatoid arthritis: a systematic review and meta-analysis of drug registries and health care databases. Rheumatology (Oxford). 2016 Mar;55(3):523-34. doi: 10.1093/rheumatology/kev374
- Heiberg MS, Koldingsnes W, Mikkelsen K, Rødevand E, Kaufmann C, Mowinckel P, Kvien TK. The comparative one-year performance of anti-tumor necrosis factor alpha drugs in patients with rheumatoid arthritis, psoriatic arthritis, and ankylosing spondylitis: results from a longitudinal, observational, multicenter study. Arthritis Rheum. 2008 Feb 15;59(2):234-40. doi: 10.1002/art.23333
- Dougados M, Wood E, Combe B, Schaeverbeke T, Miceli-Richard C, Berenbaum F, Koppiker N, Dubanchet A, Logeart I. Evaluation of the nonsteroidal anti-inflammatory drug-sparing effect of etanercept in axial spondyloarthritis: results of the multicenter, randomized, double-blind, placebo-controlled SPARSE study. Arthritis Res Ther. 2014 Nov 27;16(6):481. doi: 10.1186/s13075-014-0481-5
- Yates M, Hamilton LE, Elender F, Dean L, Doll H, MacGregor AJ, Thomas J, Gaffney K. Is Etanercept 25 mg Once Weekly as Effective as 50 mg at Maintaining Response in Patients with Ankylosing Spondylitis? A Randomized Control Trial. J Rheumatol. 2015 Jul;42(7):1177-85. doi: 10.3899/jrheum.141335
- Cantini F, Niccoli L, Cassarà E, Kaloudi O, Nannini C. Duration of remission after halving of the etanercept dose in patients with ankylosing spondylitis: a randomized, prospective, long-term, follow-up study. Biologics. 2013;7:1-6. doi: 10.2147/BTT.S31474
- Yazdany J, Dudley RA, Lin GA, Chen R, Tseng CW. Out-of-Pocket Costs for Infliximab and Its Biosimilar for Rheumatoid Arthritis Under Medicare Part D. JAMA. 2018 Sep 4;320(9):931-933. doi: 10.1001/jama.2018.7316
- Rudwaleit M, Rødevand E, Holck P, Vanhoof J, Kron M, Kary S, Kupper H. Adalimumab effectively reduces the rate of anterior uveitis flares in patients with active ankylosing spondylitis: results of a prospective open-label study. Ann Rheum Dis. 2009 May;68(5):696-701. doi: 10.1136/ard.2008.092585
- Lie E, Lindström U, Zverkova-Sandström T, Olsen IC, Forsblad-d’Elia H, Askling J, Kapetanovic MC, Kristensen LE, Jacobsson LTH. Tumour necrosis factor inhibitor treatment and occurrence of anterior uveitis in ankylosing spondylitis: results from the Swedish biologics register. Ann Rheum Dis. 2017 Sep;76(9):1515-1521. doi: 10.1136/annrheumdis-2016-210931
- Calvo-Río V, Blanco R, Santos-Gómez M, Rubio-Romero E, Cordero-Coma M, Gallego-Flores A, Veroz R, Torre I, Hernández FF, Atanes A, Loricera J, González-Vela MC, Palmou N, Hernández JL, González-Gay MA. Golimumab in refractory uveitis related to spondyloarthritis. Multicenter study of 15 patients. Semin Arthritis Rheum. 2016 Aug;46(1):95-101. doi: 10.1016/j.semarthrit.2016.03.002
- Dick AD, Tugal-Tutkun I, Foster S, Zierhut M, Melissa Liew SH, Bezlyak V, Androudi S. Secukinumab in the treatment of noninfectious uveitis: results of three randomized, controlled clinical trials. Ophthalmology. 2013 Apr;120(4):777-87. doi: 10.1016/j.ophtha.2012.09.040
- Lichtenstein GR, Loftus EV, Isaacs KL, Regueiro MD, Gerson LB, Sands BE. ACG Clinical Guideline: Management of Crohn’s Disease in Adults. Am J Gastroenterol. 2018 Apr;113(4):481-517. doi: 10.1038/ajg.2018.27. Epub 2018 Mar 27. Erratum in: Am J Gastroenterol. 2018 Jul;113(7):1101.
- Reich K, Leonardi C, Langley RG, Warren RB, Bachelez H, Romiti R, Ohtsuki M, Xu W, Acharya N, Solotkin K, Colombel JF, Hardin DS. Inflammatory bowel disease among patients with psoriasis treated with ixekizumab: A presentation of adjudicated data from an integrated database of 7 randomized controlled and uncontrolled trials. J Am Acad Dermatol. 2017 Mar;76(3):441-448.e2. doi: 10.1016/j.jaad.2016.10.027. Epub 2016 Dec 24. Erratum in: J Am Acad Dermatol. 2017 Aug;77(2):390-390.e1.
- Atar D, Birkeland KI, Uhlig T. ‘Treat to target’: moving targets from hypertension, hyperlipidaemia and diabetes to rheumatoid arthritis. Ann Rheum Dis. 2010 Apr;69(4):629-30. doi: 10.1136/ard.2010.128462





{kind=link}