
What is babesia
Babesiosis refers to a condition caused by microscopic apicomplexan parasites of the genus, Babesia that infect red blood cells and are spread by certain ticks. In the United States, tickborne transmission is most common in particular regions and seasons: it mainly occurs in parts of the Northeast and upper Midwest and usually peaks during the warm months. While more than 100 species of Babesia parasites have been reported, only a few have been identified as causing human infections, including Babesia microti, Babesia divergens, Babesia duncani, and a currently un-named strain designated MO-1. Babesia microti—which usually infects white-footed mice and other small mammals—is the main species that has been found in people in the United States 1. Occasional cases caused by other Babesia species have been detected.
Although many people who are infected with Babesia do not have symptoms, for those who do effective treatment is available. When present, signs and symptoms may include flu-like symptoms such as fever, chills, headache, body aches, nausea and fatigue. In severe cases, babesiosis can be associated with hemolytic anemia. Babesia parasites are primarily spread by infected ticks. Treatment is generally only required in people who develop symptoms of the condition. When necessary, affected people are often prescribed a combination of antimicrobial medications along with supportive care to manage symptoms.
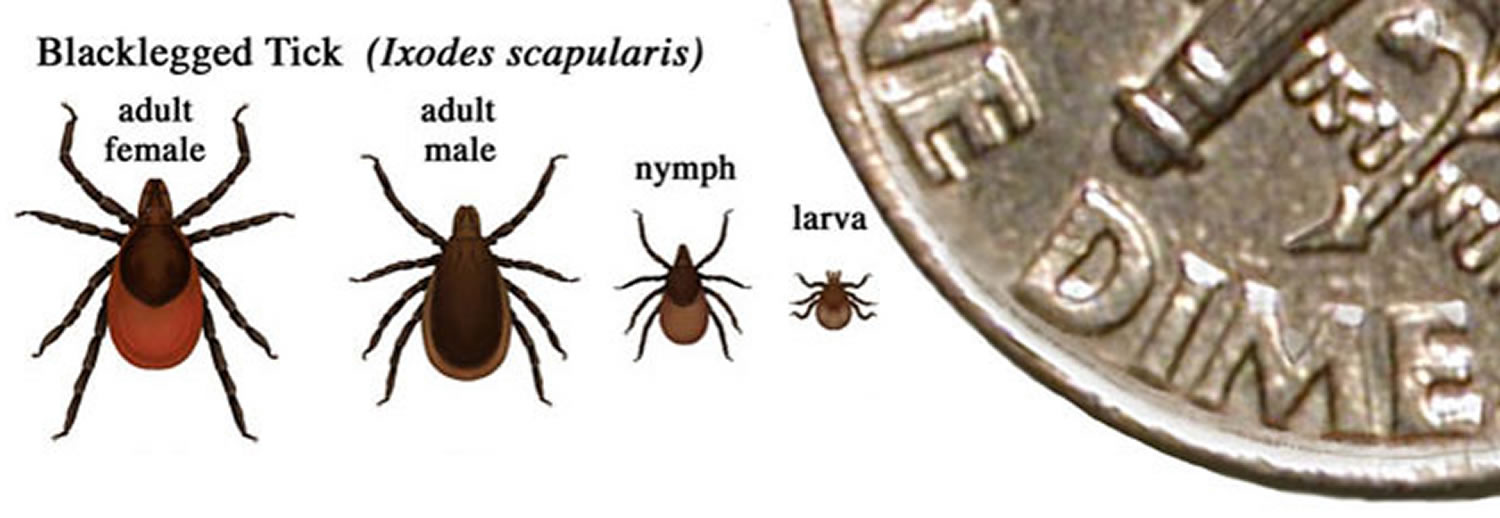
Babesiosis is preventable, if simple steps are taken to reduce exposure to ticks. Babesia microti is transmitted by the bite of infected Ixodes scapularis ticks—typically, by the nymph stage of the tick, which is about the size of a poppy seed. An Ixodes scapularis nymph is shown on Figure 1. Typically Babesia microti is transmitted by the nymphal stage of Ixodes scapularis ticks (about the size of a poppy seed).
Figure 1. Ixodes scapularis tick that can transmit Babesia

How do people get infected with Babesia?
People can get infected with Babesia parasites in several ways:
- The main way is through the bite of an infected tick—during outdoor activities in areas where babesiosis is found (see below).
- A less common way is by getting a transfusion from a blood donor who has a Babesia infection but does not have any symptoms. (No tests have been licensed yet for screening blood donors for Babesia.)
- Rare cases of congenital transmission—from an infected mother to her baby (during pregnancy or delivery)—have been reported.
Babesia parasites are not transmitted from person-to-person like the flu or the common cold.
Many different species (types) of Babesia parasites have been found in animals, only a few of which have been found in people. Babesia microti—which usually infects white-footed mice and other small mammals—is the main species that has been found in people in the United States. Occasional (sporadic) cases of babesiosis caused by other Babesia species have been detected.
The main way is through the bite of an infected tick.
- Babesia microti is spread by Ixodes scapularis ticks, which are commonly called blacklegged ticks or deer ticks. (Although white-tailed deer are the most important food source for the adult stage of the tick, deer are not infected with Babesia microti.)
- Babesia parasite typically is spread by the young nymph stage of the tick. Nymphs are mostly found during warm months (spring and summer) in areas with woods, brush, or grass.
- Infected people might not recall a tick bite because I. scapularis nymphs are very small (about the size of a poppy seed).
Other possible ways of becoming infected with Babesia include:
- Receipt of a contaminated blood transfusion (no tests have been licensed yet for donor screening); or
- Transmission from an infected mother to her baby during pregnancy or delivery.
Where do most of the cases of babesiosis occur in the United States?
Most cases occur in the Northeast and upper Midwest, particularly in parts of New England, New York state, New Jersey, Wisconsin, and Minnesota. In the Northeast, babesiosis occurs in both inland and coastal areas, including off-shore islands, such as Nantucket and Martha’s Vineyard (Massachusetts); Block Island (Rhode Island); and Shelter Island, Fire Island, and eastern Long Island (New York state).
Can babesiosis be prevented?
Yes. People can take steps to prevent babesiosis and other tickborne infections. The use of prevention measures is particularly important for people at increased risk for severe babesiosis (for example, people who do not have a spleen). If possible, areas infested with ticks should be avoided, especially during warm months. If such areas cannot be avoided, use protective measures during outdoor activities. The tiny Ixodes scapularis ticks that spread Babesia microti usually must stay attached to a person for more than 36–48 hours to be able to transmit the parasite. Daily tick checks can prevent transmission of the parasite.
Before giving blood, potential blood donors are asked if they have ever been diagnosed with babesiosis. If the answer is “yes,” they are indefinitely deferred from donating blood. In March 2018, FDA approved the first Babesia microti screening tests for U.S. blood donors, who can feel fine despite being infected.
No vaccine is available to protect people against babesiosis.
Prevention and Control
Steps can be taken to reduce the risk for babesiosis and other tickborne infections. The use of prevention measures is especially important for people at increased risk for severe babesiosis (for example, people who do not have a spleen). Avoiding exposure to tick habitats is the best defense.
Babesia microti is spread by Ixodes scapularis ticks, which are mostly found in wooded, brushy, or grassy areas, in certain regions and seasons. No vaccine is available to protect people against babesiosis. However, people who live, work, or travel in tick-infested areas can take simple steps to help protect themselves against tick bites and tickborne infections.
During outdoor activities in tick habitats, take precautions to keep ticks off the skin.
- Walk on cleared trails and stay in the center of the trail, to minimize contact with leaf litter, brush, and overgrown grasses, where ticks are most likely to be found.
- Minimize the amount of exposed skin, by wearing socks, long pants, and a long-sleeved shirt. Tuck the pant legs into the socks, so ticks cannot crawl up the inside of the pants. Wear light-colored clothing, to make it easier to see and remove ticks before they attach to skin.
- Apply repellents to skin and clothing. Follow the instructions on the product label.
- Products that contain DEET (N,N-diethylmetatoluamide) can be directly applied to exposed skin and to clothing, to help keep ticks away (by repelling them). The product label includes details about how and where to apply the repellent, how often to reapply it, and how to use it safely on children.
- Permethrin products can be applied to clothing/boots (not to skin), actually kill ticks that come in contact with the treated clothing, and usually stay effective through several washings.
After outdoor activities, conduct daily tick checks and promptly remove any ticks that are found. Thorough, daily tick checks are very important. The Ixodes scapularis nymphs that typically spread Babesia microti are so small (about the size of a poppy seed) that they are easily overlooked. But they usually must stay attached to a person for more than 36-48 hours to be able to transmit the parasite.
- Remove ticks from clothing and pets before going indoors.
- Conduct a full-body exam for ticks. Use a hand-held or full-length mirror to view all parts of the body. Be sure to check behind the knees, between the legs (groin/thighs), between the toes, under the arms (armpits), around the waist, inside the belly button, the back of the neck, behind and in the ears, as well as in and around the scalp, hairline, and hair. Remember to check children and pets, too.
Remove ticks that are attached to the skin as soon as possible, preferably by using pointed (fine-tipped) tweezers. Grab the tick’s mouth parts close to the skin, and slowly pull the tick straight out (with steady outward pressure), until the tick lets go.
Babesia parasite life cycle
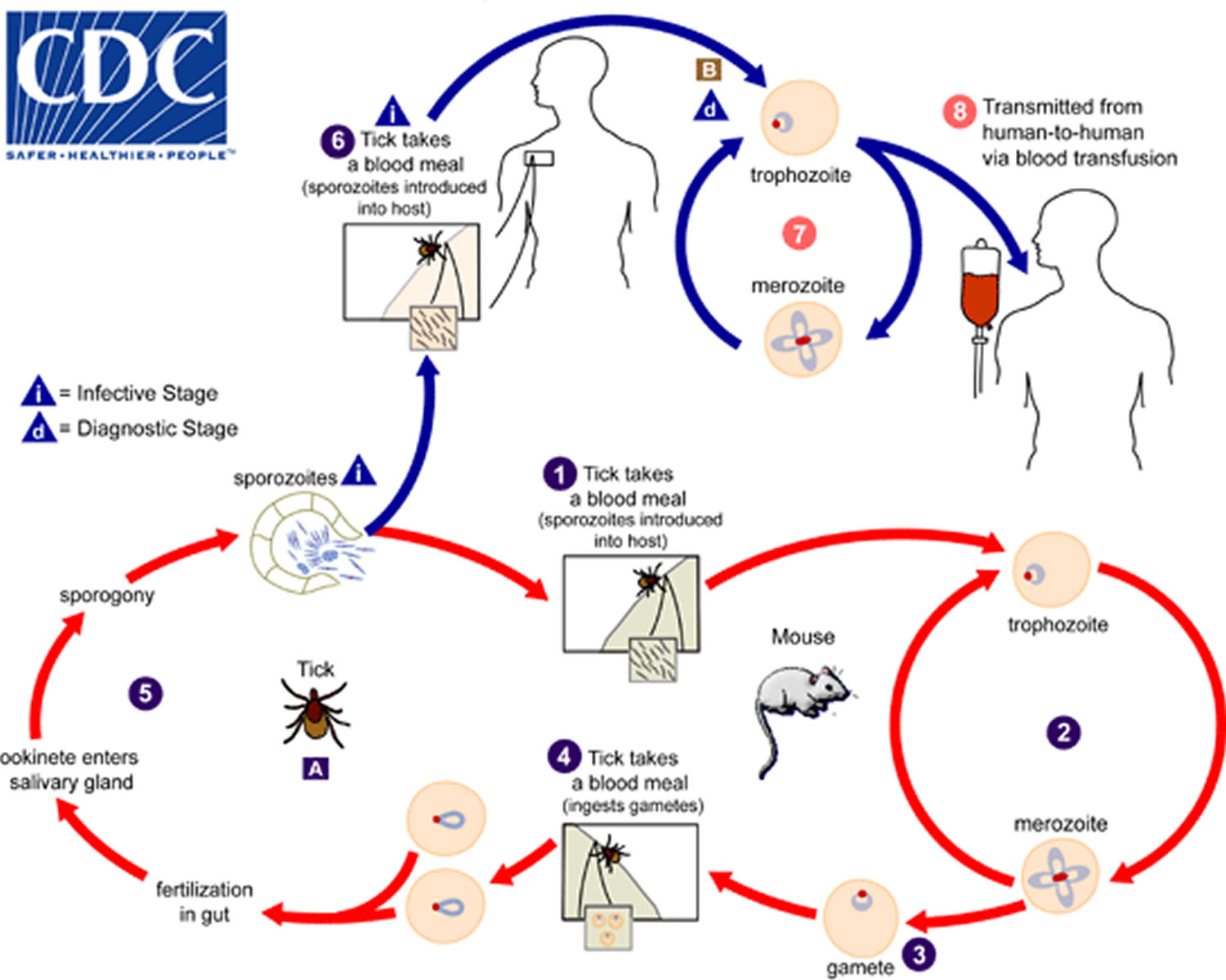
The Babesia microti life cycle involves two hosts, which includes a rodent, primarily the white-footed mouse, Peromyscus leucopus, and a tick in the genus, Ixodes. (1) During a blood meal, a Babesia-infected tick introduces sporozoites into the mouse host. (2) Sporozoites enter erythrocytes and undergo asexual reproduction (budding). (3) In the blood, some parasites differentiate into male and female gametes although these cannot be distinguished at the light microscope level. (4) The definitive host is the tick. (5) Once ingested by an appropriate tick, gametes unite and undergo a sporogonic cycle resulting in sporozoites. (A) Transovarial transmission (also known as vertical, or hereditary, transmission) has been documented for “large” Babesia spp. but not for the “small” babesiae, such as Babesia microti.
Humans enter the cycle when bitten by infected ticks. (6) During a blood meal, a Babesia-infected tick introduces sporozoites into the human host. (B) Sporozoites enter erythrocytes and undergo asexual replication (budding) (7). Multiplication of the blood stage parasites is responsible for the clinical manifestations of the disease. Humans are, for all practical purposes, dead-end hosts and there is probably little, if any, subsequent transmission that occurs from ticks feeding on infected persons. (8) However, human to human transmission is well recognized to occur through blood transfusions.
Figure 2. Babesia microti life cycle
Babesia symptoms
Many people who are infected with Babesia microti feel fine and do not have any symptoms. Some people develop nonspecific flu-like symptoms, such as fever, chills, sweats, headache, body aches, loss of appetite, nausea, or fatigue.
Because Babesia parasites infect and destroy red blood cells, babesiosis can cause a special type of anemia called hemolytic anemia. This type of anemia can lead to jaundice (yellowing of the skin) and dark urine.
Babesiosis can be a severe, life-threatening disease, particularly in people who:
- Do not have a spleen (asplenia);
- Have a weak immune system for other reasons (such as cancer, lymphoma, corticosteroid therapy or AIDS);
- Have other serious health conditions (such as liver or kidney disease); or
- Are elderly.
Complications of babesiosis can include:
- A low and unstable blood pressure;
- Severe hemolytic anemia (hemolysis);
- A very low platelet count (thrombocytopenia);
- Disseminated intravascular coagulation (also known as “DIC” or consumptive coagulopathy), which can lead to blood clots and bleeding;
- Malfunction of vital organs (such as the kidneys, lungs, and liver); or
- Death.
Some immunosuppressive therapies or conditions may affect the clinical manifestations (e.g., the patient might be afebrile). Severe cases can be associated with marked thrombocytopenia, disseminated intravascular coagulation (DIC), hemodynamic instability, acute respiratory distress syndrome (ARDS), myocardial infarction (heart attack), renal failure, hepatic compromise, altered mental status, and death.
How soon after the exposure do symptoms develop?
Symptoms, if any, can start within a week or so. They usually develop within a few weeks or months, sometimes longer.
Babesiosis diagnosis
Diagnosis of babesiosis requires a high index of suspicion, in part because the clinical manifestations are nonspecific. For acutely ill patients, the findings on routine laboratory testing frequently include hemolytic anemia and thrombocytopenia. Additional findings may include proteinuria, hemoglobinuria, and elevated levels of liver enzymes, blood urea nitrogen, and creatinine.
In symptomatic people, babesiosis usually is diagnosed by examining blood under a microscope and seeing Babesia parasites inside red blood cells. To be sure the diagnosis is correct, your health care provider might have specimens of your blood tested by a specialized reference laboratory (such as at CDC or a health department). In addition, your health care provider might decide to have your blood tested for other possible causes of your symptoms, including other tickborne infections, such as Lyme disease and anaplasmosis.
Sometimes it can be difficult to distinguish between Babesia and Plasmodium (especially Plasmodium falciparum) parasites and even between parasites and artifacts (such as stain or platelet debris). Consider having a reference laboratory confirm the diagnosis—by blood-smear examination and, if indicated, by other means, such as molecular and/or serologic methods tailored to the setting/species.
Diagnosis can be made by microscopic examination of thick and thin blood smears stained with Giemsa. Repeated smears may be needed.
Figure 3. Babesia parasites inside red blood cells stained with Giemsa – Babesia parasites resemble Plasmodium falciparum (malaria), however Babesia has several distinguishing features: the parasites are pleomorphic (vary in shape and size), can be vacuolated, and do not produce pigment.

Antibody Detection
Diagnosis of Babesia infection should be made by detection of parasites in patients’ blood smears. However, antibody detection tests are useful for detecting infected individuals with very low levels of parasitemia (such as asymptomatic blood donors in transfusion-associated cases), for diagnosis after infection is cleared by therapy, and for discrimination between Plasmodium falciparum and Babesia infection in patients whose blood smear examinations are inconclusive and whose travel histories cannot exclude either parasite.
The indirect fluorescent antibody test (IFA) using Babesia microti parasites as antigen detects antibodies in 88-96% of patients with Babesia microti infection. Indirect fluorescent antibody test (IFA) antigen slides are prepared using washed, parasitized erythrocytes produced in hamsters. Patients’ titers generally rise to ≥1:1024 during the first weeks of illness and decline gradually over 6 months to titers of 1:16 to 1:256 but may remain detectable at low levels for a year or more. Specificity is 100% in patients with other tick-borne diseases or persons not exposed to the parasite. Cross-reactions may occur in serum specimens from patients with malaria infections, but generally titers are highest with the homologous antigen.
The extent of cross-reactivity between Babesia species is variable. A negative result with Babesia microti antigen for a patient exposed on the West Coast may be a false-negative reaction for Babesia infection. Individuals whose exposure could have occurred on the West Coast should be tested also for antibodies to the Babesia duncani, because of the lack of cross-reactivity with Babesia microti.
Molecular diagnosis
In some infections with intraerythrocytic parasites, the morphologic characteristics observed on microscopic examination of blood smears do not allow an unambiguous differentiation between Babesia and Plasmodium. Moreover, potential blood donors may have subclinical symptoms and very low parasitemia, undetectable in blood smears. In such cases, the diagnosis can be derived from molecular techniques, such as polymerase chain reaction (PCR). In addition, molecular approaches are very valuable in investigations of new Babesia variants (or species) observed in recent human infections in the United States and in Europe.
Babesia treatment
Most asymptomatic persons do not require treatment. Health care providers may consult CDC staff about whether to treat someone who has babesiosis, what type(s) of therapy to use, how to monitor the status of the infection, and how long to treat. The first step is to make sure the diagnosis is correct. Treatment decisions should be individualized, especially for patients who have (or are at risk for) severe or relapsing infection.
For ill patients, babesiosis usually is treated for at least 7-10 days with a combination of two prescription medications — typically either:
- Atovaquone PLUS azithromycin; OR
- Clindamycin PLUS quinine (this combination is the standard of care for severely ill patients).
The typical daily doses for adults are provided in the table below.
| Drug | Adult dosage (usually treat for at least 7–10 days) |
|---|---|
| Atovaquone | 750 mg orally twice a day |
| along with | |
| Azithromycin | On the first day, give a total dose in the range of 500–1000 mg orally; on subsequent days, give a total daily dose in the range of 250–1000 mg |
| or | |
| Clindamycin | 600 mg orally 3 times a day or 300–600 mg intravenously 4 times a day |
| along with | |
| Quinine | 650 mg orally 3 times a day |
Some patients—including those with severe illness—might require or benefit from supportive care, such as:
- Antipyretics;
- Vasopressors (if the blood pressure is low and unstable);
- Blood transfusions;
- Exchange transfusions (in which portions of a patient’s blood or blood cells are replaced with transfused blood components);
- Mechanical ventilation; or
- Dialysis





{kind=link}