What is C peptide
C-peptide is short for connecting-peptide, connects alpha and beta chains of proinsulin, which are formed in the endoplasmic reticulum following removal of the signal peptide of pre-proinsulin 1. C-peptide is released into the blood as a byproduct of the formation of insulin by the pancreas. In the pancreas, within specialized cells called beta cells of the endocrine islets of Langerhans of the pancreas, proinsulin, a biologically inactive molecule, splits apart to form one molecule of C-peptide and one molecule of insulin. C-peptide plays an important role in the correct folding of insulin and the formation of disulfide bridges. C-peptide is removed in the Golgi apparatus from proinsulin resulting in the formation of the mature insulin molecule with both alpha and beta chains bound together by disulfide bonds 2. Both insulin and C-peptide are stored in secretory vesicles and released in equimolar concentrations upon stimulation of beta cells by glucose and other secretagogues 3. Insulin is vital for the transport of glucose into your body’s cells and is required on a daily basis. When insulin is required and released from the beta cells into the blood in response to increased levels of glucose, equal amounts of C-peptide are also released. Since C-peptide is produced at the same rate as insulin, it is useful as a marker of insulin production. The most important indications for measurement of C-peptide levels include the differential diagnosis of fasting hypoglycemia with hyperinsulinism and as a measure of insulin secretory reserve.
Once secreted, both insulin and C-peptide are routed through the liver 1. In the liver, insulin binds to its receptors and initiates glucose uptake, inhibits gluconeogenesis, glycogenolysis, and ketogenesis and is degraded within 5 to 10 minutes. C-peptide, on the other hand, has limited degradation in the liver and is degraded by the kidneys. Hence, the half-life of C-peptide is around 30 to 35 minutes. As a result, although both insulin and C-peptide are secreted in equimolar concentrations, the molar ratio of circulating insulin to C-peptide is less than 1. Several studies have shown that C-peptide can bind to the cell membranes and could exert biological effects; however, a specific receptor has not been identified, and this is described later.
Even though they are produced at the same rate, C-peptide and insulin leave the body by different routes. Insulin is processed and eliminated mostly by the liver, while C-peptide is removed by the kidneys. Since the half-life of C-peptide is about 30 minutes compared to insulin’s 5 minutes, normally there will be about 5 times as much C-peptide in the blood as insulin. C-peptide is catabolized in the kidneys, and only a small fraction is excreted in urine. Modern ultrasensitive C-peptide immunoassays can detect plasma levels as low as 0.0045 to 0.0075 ng/ml.
The normal physiological C-peptide plasma concentration in a fasted state is 0.9 to 1.8 ng/ml 2. A high level could indicate insulin resistance, insulinoma, or kidney disease. A low C-peptide is usually present in patients with type 1, or sometimes, type 2 diabetes.
Researchers are starting to better understand the role of C-peptide in the body. Some studies have been conducted to evaluate the use of C-peptide as a therapy for those with diabetes. Results have been promising, showing decreased diabetic complications with improvements in kidney function, blood flow, and nerve function. However, further studies are needed.
C-peptide is a 31-amino acid polypeptide and is negatively charged. In mammals, the 8 residues (position 1, 3, 6, 11, 12, 21, 27, and 31) are conserved, and the C-terminal pentapeptide has been shown to interact with the cell membrane and elicit signaling pathways 4. Although the exact mechanism of binding is not known, the binding characteristics and the intracellular effects could be modified by pertussis toxin, suggesting that the G-protein coupled receptors might be involved 5. The binding of C-peptide was shown to elevate the intracellular calcium levels. It also can induce phospholipase C, protein kinase C isoforms, Rho A, and p38 MAPK in renal tubular cells and fibroblasts 6. Activation of the PI3 kinase, Akt, and PPAR-gamma is also observed in fibroblasts, myoblasts, renal tubular cells, and lymphocytes 7. In endothelial cells, C-peptide was shown to induce the nitric oxide release by enhancing the expression of eNOS mRNA and protein in aortic endothelial cells. It was also shown to stimulate Na, K-ATPase in renal tubular cells in vitro 6.
C-peptide was also shown to possess several anti-inflammatory, cytoprotective, and anti-apoptotic effects in various cell types. Under physiological conditions, C-peptide was shown to inhibit the formation of reactive oxygen species (ROS) via RAC1-mediated inhibition of NAD(P)H oxidase in endothelial cells of streptozotocin (STZ)-diabetic mice 8. C-peptide could inhibit ROS-mediated activation of transglutaminase 2, thereby inhibiting apoptosis. It also exerted the anti-apoptotic effect by inhibiting caspase 3 activation and enhancing the anti-apoptotic protein, BCL-2 in endothelial cells and neuroblastoma cells. C-peptide was also shown to inhibit the inflammatory pathway by the downregulation of NF-kB. It was also shown that C-peptide could decrease the expression of high glucose-induced ICAM, VCAM, and P-selectin 9. High glucose-induced, vascular, smooth muscle cell proliferation and migration may be inhibited by the presence of C-peptide, thereby causing the inhibition of atherosclerotic lesion formation 10. There is considerable interest in the biology of C-peptide, its elusive receptor, and biological effects in humans. However, this body of data is largely experimental, and needs much further research in the clinical area to gain mainstream support.
Figure 1. Islets of Langerhans of the pancreas
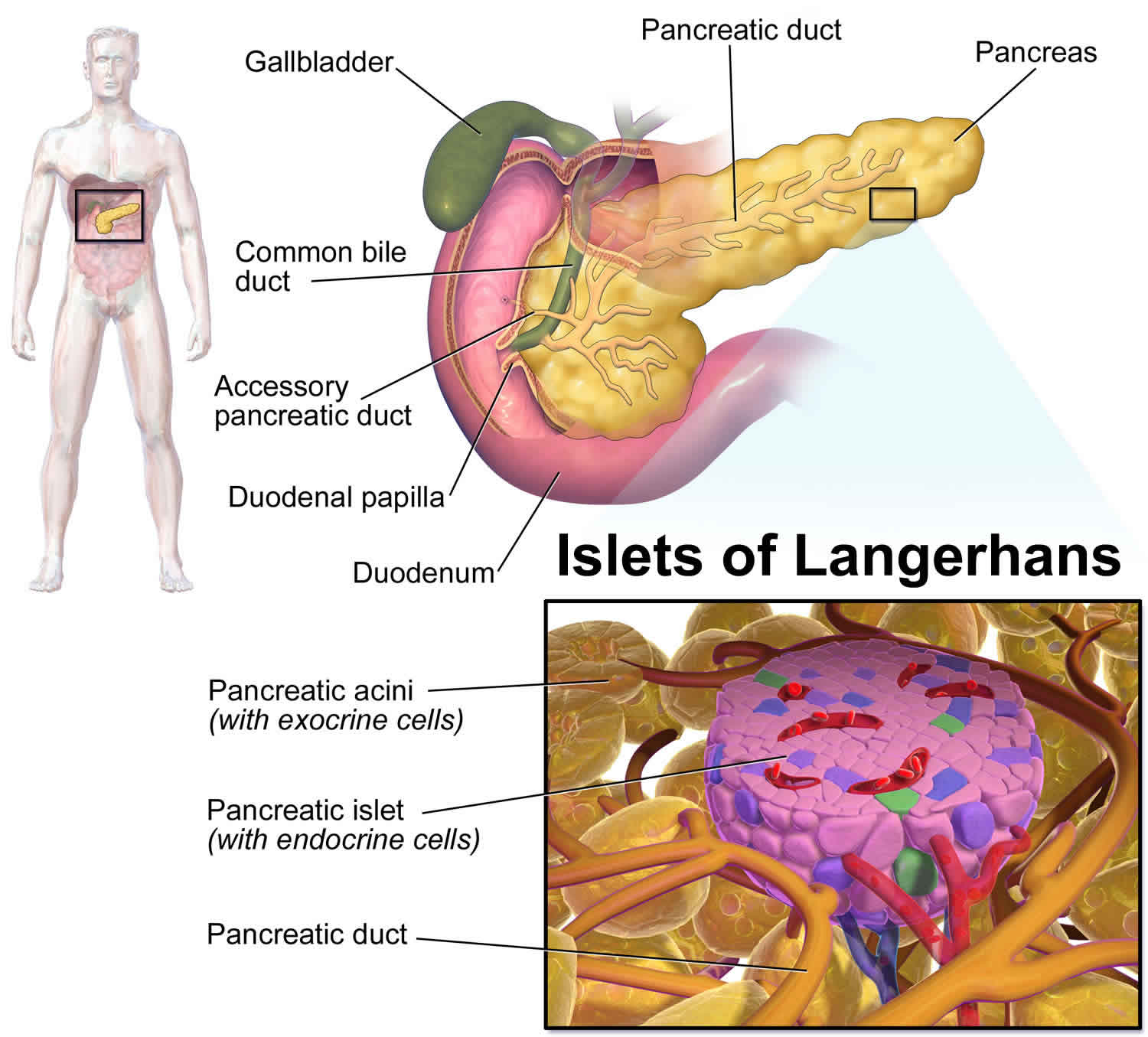 Figure 2. C-peptide
Figure 2. C-peptide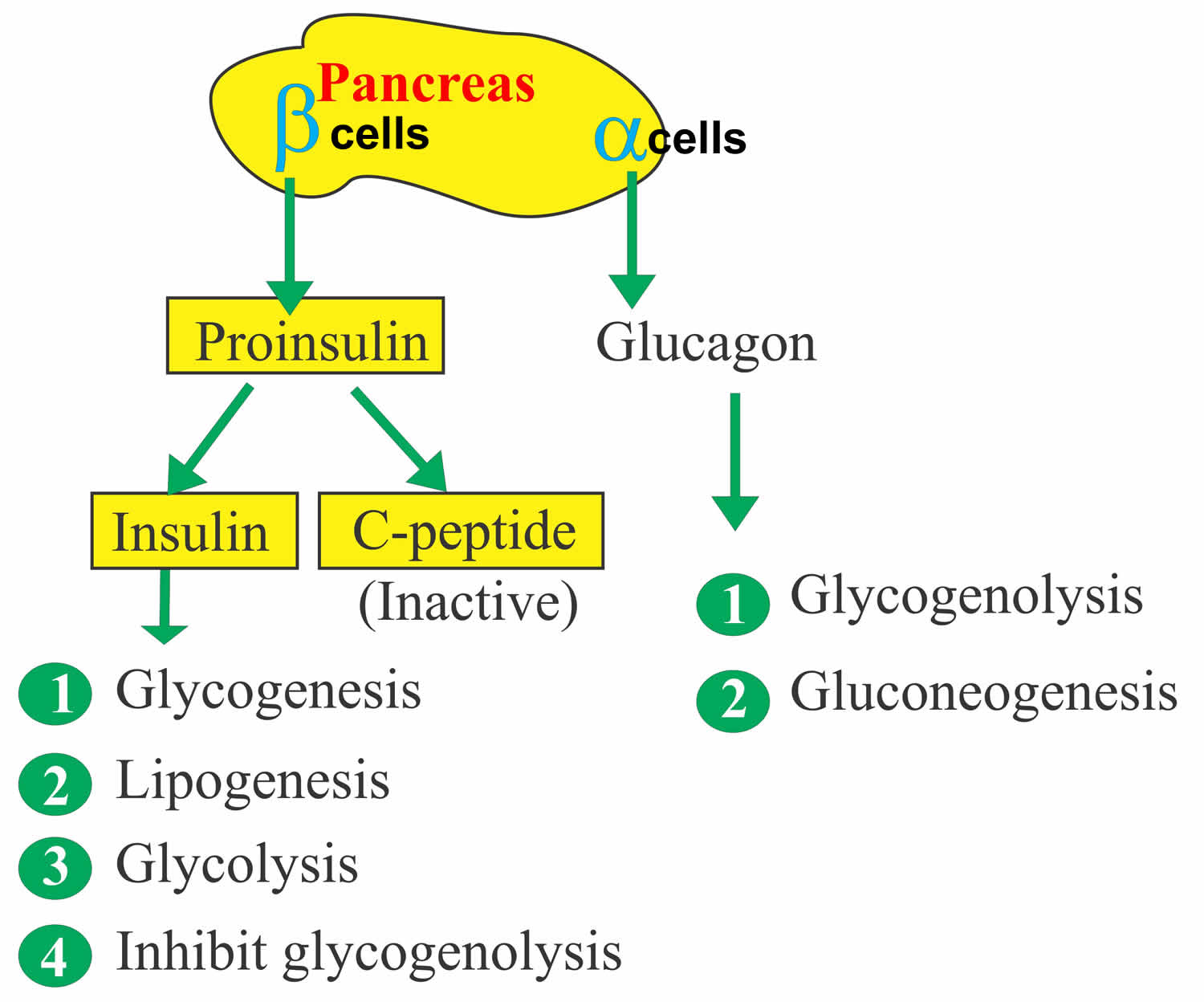
C peptide test
C-peptide test measures the amount of C-peptide in a blood or urine sample. Since C-peptide is produced at the same rate as insulin, it is useful as a marker of insulin production. In particular, C-peptide testing can be used to help evaluate the production of insulin made by the body (endogenous) and to help differentiate it from insulin that is not produced by the body but is taken in as diabetic medication (exogenous) and so does not generate C-peptide. C-peptide test may be done in conjunction with an insulin test.
For the C-peptide test, a blood sample is obtained by inserting a needle into a vein in the arm. Fasting for 8 to 10 hours before blood testing is usually required. If a 24-hour urine sample is required, all urine produced over a 24-hour time period will be collected. Urinary C-peptide measurement is a non-invasive test, and the urine can be collected in boric acid, where urinary C-peptide is stable at room temperature for up to 3 days. With normal urinary function, the urinary C-peptide excretion is reflective of 5% to 10% of total C-peptide secreted by the pancreas 11.
C-peptide testing is not widely used and may not be available in every laboratory. If a series of C-peptide tests are going to be performed, they should be done at the same laboratory using the same method.
Can I do a C-peptide test at home like I can when I check my blood glucose?
No. The C-peptide test requires special equipment and training to perform.
C-peptide test uses
The 2 major indications for measuring C-peptide levels include fasting hypoglycemia and assessment of insulin secretory reserve in patients with diabetes. In patients with fasting hypoglycemia with concomitant hyperinsulinism, one needs to entertain a differential diagnosis comprising insulinoma, exogenous insulin administration (factitious), sulfonylurea therapy (factitious), insulin autoimmune syndrome due to endogenous anti-insulin antibodies (Hirata disease).[15] All of these conditions can result in hypoglycemia with elevated insulin levels. A C-peptide level is very useful in the differential diagnosis since it is only elevated with a beta cell tumor, insulinoma, and sulfonylurea therapy. A sulfonylurea drug screen can exclude the latter. C-peptide is not elevated with Hirata disease, which is confirmed by positive anti-insulin antibodies and is decreased with factious, exogenous insulin therapy. Hence, it is a very important test in the workup of fasting hypoglycemia with hyperinsulinism.
The other major indication is the assessment of insulin secretory reserve in patients with diabetes. Diabetes mellitus is characterized by hyperglycemia due to the lack of insulin secretion and/or insulin action. Insulin deficiency is associated with C-peptide-deficiency in type 1 diabetes due to beta cell demise. A fasting C-peptide level of less than 0.6 ng/ml is consistent with beta cell failure and predicts requirement for insulin therapy. Although the origins of type 2 diabetes are insulin resistance, it only manifests clinically when there is beta cell failure resulting in impaired insulin and C-peptide secretion culminating in fasting and post-prandial hyperglycemia. Much more research is needed to define the biology of C-peptide and potential role in the pathogenesis of diabetic microvascular complications or as a novel therapeutic agent.
Also, Medicare uses C-peptide assessment of insulin reserve as a criterion for continuous subcutaneous insulin infusion therapy (insulin pump therapy).
The following are some purposes of C-peptide testing:
- A C-peptide test is not ordered to help diagnose diabetes, but when a person has been newly diagnosed with diabetes, it may be ordered by itself or along with an insulin level to help determine how much insulin a person’s pancreas is still producing (endogenous insulin).
- In type 2 diabetes, the body is resistant to the effects of insulin (insulin resistance) and it compensates by producing and releasing more insulin, which can also lead to beta cell damage. Type 2 diabetics usually are treated with oral drugs to stimulate their body to make more insulin and/or to cause their cells to be more sensitive to the insulin that is already being made. Eventually, because of the beta cell damage, type 2 diabetics may make very little insulin and require injections. Any insulin that the body does make will be reflected in the C-peptide level; therefore, the C-peptide test can be used to monitor beta cell activity and capability over time and to help a health practitioner determine when to begin insulin treatment.
- People who are on insulin therapy, regardless of the source of the insulin, may develop antibodies to insulin. These typically interfere with tests for insulin, making it nearly impossible to directly evaluate endogenous insulin production. In these cases, C-peptide measurement is a useful alternative to testing for insulin.
- C-peptide measurements can also be used in conjunction with insulin and glucose levels to help diagnose the cause of documented hypoglycemia and to monitor its treatment. Symptoms of hypoglycemia may be caused by excessive supplementation of insulin, alcohol consumption, inherited liver enzyme deficiencies, liver or kidney disease, or by insulinomas.
- The C-peptide test may be used to help diagnose Insulinomas. These are tumors of the islet cells in the pancreas that can produce uncontrolled amounts of insulin and C-peptide and can cause acute episodes of hypoglycemia. C-peptide tests may be used to monitor the effectiveness of insulinoma treatment and to detect recurrence.
- Sometimes a C-peptide test may be used to help evaluate a person diagnosed with metabolic syndrome, a set of risk factors that includes abdominal obesity, increased blood glucose and/or insulin resistance, unhealthy blood lipid levels, and high blood pressure (hypertension).
Rarely, when someone has had his pancreas removed or has had pancreas islet cell transplants, intended to restore the ability to make insulin, C-peptide levels may be used to verify the effectiveness of treatment and continued success of the procedure.
If I need to go on the insulin pump, will I need a C-peptide test?
You may. Insulin pumps are usually recommended for those who are not producing sufficient insulin. Sometimes a C-peptide test will be ordered during an initial evaluation to check the status of your beta cells and to see if you are still producing insulin.
When is C-peptide test ordered?
C-peptide levels may be ordered when a person has been newly diagnosed with type 1 diabetes as part of an evaluation of the person’s “residual beta cell function.”
With type 2 diabetes, the test may be ordered on a regular basis when a health practitioner wants to monitor the status of a person’s beta cells and insulin production over time and to determine if/when insulin injections may be required.
C-peptide levels may be done when there is documented acute or recurring low blood glucose (hypoglycemia) and/or excess insulin is suspected. Symptoms of hypoglycemia include:
- Sweating
- Palpitations
- Hunger
- Confusion
- Blurred vision
- Fainting
- In severe cases, seizures and loss of consciousness
However, many of these symptoms can occur with other conditions as well.
When a person has been diagnosed with an insulinoma, a C-peptide test may be ordered periodically to monitor the effectiveness of treatment and to detect tumor recurrence.
Rarely, C-peptide levels may be monitored over time when someone has had his pancreas removed or has had pancreas islet cell transplants.
High C-peptide
The plasma concentration of C-peptide in a fasted state is 0.9 to 1.8 ng/ml, and the postprandial levels are 3 to 9 ng/m in healthy individuals 12. The higher levels are observed in the overweight individuals. The presence of increased titers of anti-insulin antibodies that bind to both proinsulin and C-peptide could give false positive results.
A high level of C-peptide generally indicates a high level of endogenous insulin production. This may be in response to a high blood glucose caused by glucose intake and/or insulin resistance. A high level of C-peptide is also seen with insulinomas and may be seen with low blood potassium, Cushing syndrome, and renal failure.
When used for monitoring, decreasing levels of C-peptide in someone with an insulinoma indicate a response to treatment; levels that are increasing may indicate a tumor recurrence.
Low C-peptide
A low level of C-peptide is associated with a low level of insulin production. This can occur when insufficient insulin is being produced by the beta cells, with diabetes for example, or when production is suppressed by treatment with exogenous insulin.
References- Venugopal SK, Jialal I. C Peptide. [Updated 2018 Oct 27]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK526026
- Yosten GL, Maric-Bilkan C, Luppi P, Wahren J. Physiological effects and therapeutic potential of proinsulin C-peptide. Am. J. Physiol. Endocrinol. Metab. 2014 Dec 01;307(11):E955-68
- Steiner DF, Cunningham D, Spigelman L, Aten B. Insulin biosynthesis: evidence for a precursor. Science. 1967 Aug 11;157(3789):697-700
- Rigler R, Pramanik A, Jonasson P, Kratz G, Jansson OT, Nygren P, Stâhl S, Ekberg K, Johansson B, Uhlén S, Uhlén M, Jörnvall H, Wahren J. Specific binding of proinsulin C-peptide to human cell membranes. Proc. Natl. Acad. Sci. U.S.A. 1999 Nov 09;96(23):13318-23
- Al-Rasheed NM, Willars GB, Brunskill NJ. C-peptide signals via Galpha i to protect against TNF-alpha-mediated apoptosis of opossum kidney proximal tubular cells. J. Am. Soc. Nephrol. 2006 Apr;17(4):986-95
- Zhong Z, Kotova O, Davidescu A, Ehrén I, Ekberg K, Jörnvall H, Wahren J, Chibalin AV. C-peptide stimulates Na+, K+-ATPase via activation of ERK1/2 MAP kinases in human renal tubular cells. Cell. Mol. Life Sci. 2004 Nov;61(21):2782-90
- Kitamura T, Kimura K, Jung BD, Makondo K, Okamoto S, Cañas X, Sakane N, Yoshida T, Saito M. Proinsulin C-peptide rapidly stimulates mitogen-activated protein kinases in Swiss 3T3 fibroblasts: requirement of protein kinase C, phosphoinositide 3-kinase and pertussis toxin-sensitive G-protein. Biochem. J. 2001 Apr 01;355(Pt 1):123-9
- Bhatt MP, Lim YC, Kim YM, Ha KS. C-peptide activates AMPKα and prevents ROS-mediated mitochondrial fission and endothelial apoptosis in diabetes. Diabetes. 2013 Nov;62(11):3851-62
- Luppi P, Cifarelli V, Tse H, Piganelli J, Trucco M. Human C-peptide antagonises high glucose-induced endothelial dysfunction through the nuclear factor-kappaB pathway. Diabetologia. 2008 Aug;51(8):1534-43
- Wahren J, Larsson C. C-peptide: new findings and therapeutic possibilities. Diabetes Res. Clin. Pract. 2015 Mar;107(3):309-19
- Bowman P, McDonald TJ, Shields BM, Knight BA, Hattersley AT. Validation of a single-sample urinary C-peptide creatinine ratio as a reproducible alternative to serum C-peptide in patients with Type 2 diabetes. Diabet. Med. 2012 Jan;29(1):90-3
- Yosten GL, Maric-Bilkan C, Luppi P, Wahren J. Physiological effects and therapeutic potential of proinsulin C-peptide. Am. J. Physiol. Endocrinol. Metab. 2014 Dec 01;307(11):E955-68.





{kind=link}