
What is cesarean section
A cesarean section, or C-section, is an operation to deliver your baby through a cut made in your abdomen and womb (uterus). The cut is usually made across your abdomen, just below your bikini line. A cesarean is a major operation that carries a number of risks, so it’s usually only done if it’s the safest option for you and your baby. After the baby is removed from the womb, the uterus and abdomen are closed with stitches that later dissolve 1.
In the United States, almost one in three women has their babies this way. Cesarean section is now the most common surgery performed in the United States, with over 1 million women delivered by cesarean every year 2. The cesarean delivery rate rose from 5% in 1970 to 31.9% in 2016 3. Though there are continuing efforts to reduce the rate of cesarean sections, experts do not anticipate a significant drop for at least a decade or two 4. While it confers risks of both immediate and long-term complications, for some women, cesarean delivery can be the safest or even the only way to deliver a healthy newborn.
Some C-sections are planned, but many are done when unexpected problems happen during delivery. Reasons for a C-section may include:
- Health problems in the mother
- The mother carrying more than one baby
- The size or position of the baby
- The baby’s health is in danger
- Labor is not moving along as it should
The cesarean section surgery is relatively safe for mother and baby. Still, it is major surgery and carries risks. It also takes longer to recover from a C-section than from vaginal birth. It can raise the risk of having difficulties with future pregnancies. Some women may have problems attempting a vaginal birth later. Still, many women are able to have a vaginal birth after cesarean section.
Most cesareans are carried out under spinal or epidural anaesthetic. This mean you’ll be awake, but the lower part of your body is numbed so you won’t feel any pain.
During the cesarean section procedure:
- a screen is placed across your body so you can’t see what’s being done – the doctors and nurses will let you know what’s happening
a cut about 10-20cm long will usually be made across your lower tummy and womb so your baby can be delivered - you may feel some tugging and pulling during the procedure
- you and your birth partner will be able to see and hold your baby as soon as they’ve been delivered
The whole operation normally takes about 40-50 minutes.
Occasionally a general anaesthetic, where you’re asleep, may be used, particularly if the baby needs to be delivered more quickly.
Figure 1. Cesarean section scar
C-section recovery time
Recovering from a cesarean usually takes longer than recovering from a vaginal delivery. You might need to stay in hospital for three or four days, compared with one or two days for a vaginal birth.
You may experience some discomfort in your tummy for the first few days, and you’ll be offered painkillers to help with this.
When you go home, you’ll need to take things easy at first. You may need to avoid some activities such as driving for six weeks or so.
The wound in your tummy will eventually form a scar. This may be red and obvious at first, but it should fade with time and will often be hidden in your pubic hair.
Future pregnancies after a cesarean section
If you have a baby by cesarean section, it doesn’t necessarily mean that any babies you have in the future will also have to be delivered this way.
Most women who have had a cesarean section can safely have a vaginal delivery for their next baby, known as vaginal birth after cesarean section.
However, you may need some extra monitoring during labor just to make sure everything is progressing well.
Some women may be advised to have another cesarean section if they have another baby. This depends on whether a cesarean section is still the safest option for them and their baby.
Reasons for cesarean section
A cesarean section may be recommended as a planned (elective) procedure or done in an emergency if it’s thought a vaginal birth is too risky. For example, a cesarean delivery is often the recommended approach if a woman has had a prior classical cesarean scar or previous uterine rupture. However, due to the potential complications of cesarean birth, much study has been done looking for ways to reduce the cesarean rate.
Planned cesareans aren’t usually done before the 39th week of pregnancy.
There has been an emphasis decreasing the number of first-time cesarean births, as many women who have one cesarean birth will ultimately have the remainder of their children via cesarean section. She may choose another cesarean birth for various reasons or she may not be a candidate for a subsequent vaginal birth. For example, if a woman has an unfavorable cervix at term, cervical ripening with medications such as misoprostol is not recommended due to an increased risk of uterine rupture with those agents. In the 2011 article “Safe Prevention of the Primary Cesarean Delivery” 5, the authors addressed the most commonly documented indications for first-time cesarean deliveries (labor dystocia, abnormal fetal heart rate pattern, malpresentation of the fetus, multiple gestations, and suspected fetal macrosomia), and mitigation of how these factors.
One study in 2007 6 looked at what level of additional fetal risk a woman or her caregiver considered to be acceptable to achieve a vaginal delivery and to avoid a cesarean section. They concluded that both the pregnant patients and those taking care of them had a low tolerance for risk. It is understandable and justifiable for a woman to have high expectations for the outcome of her delivery. The goal of reducing cesarean rates may be difficult to achieve, considering this hesitance to expose the fetus to risk.
A cesarean may be carried out because:
- Breech presentation: your baby is in the breech position (feet first) and your doctor has been unable to turn them by applying gentle pressure to your tummy, or you would prefer they didn’t try this
- You have a low-lying placenta (placenta previa)
- You have pregnancy-related high blood pressure (pre-eclampsia)
- You have certain infections, such as a first genital herpes infection occurring late in pregnancy or untreated HIV
- Your baby isn’t getting enough oxygen and nutrients – sometimes this may mean the baby needs to be delivered immediately
- Your labor isn’t progressing or there’s excessive vaginal bleeding
- Failure of labor to progress—contractions may not open the cervix enough for the baby to move into the vagina.
- Concern for the baby—For instance, the umbilical cord may become pinched or compressed or fetal monitoring may detect an abnormal heart rate.
- Multiple pregnancy—you’re pregnant with twins, a cesarean birth may be necessary if the babies are being born too early, are not in good positions in the uterus, or if there are other problems. The likelihood of having a cesarean birth increases with the number of babies a woman is carrying.
- A very large baby. Larger infants are at risk for complications during delivery. These include shoulder dystocia, when the infant’s head is delivered through the vagina but the shoulders are stuck 7. Women with gestational diabetes, especially if their blood sugar levels are not well controlled, are at increased risk for having large babies.
- Maternal infections, such as human immunodeficiency virus (HIV) or herpes, that could be passed to the baby during vaginal birth. Cesarean delivery could help prevent transmission of the virus to the infant.
- Sometimes the placenta is not formed or working correctly, is in the wrong place in the uterus, or is implanted too deeply or firmly in the uterine wall. These issues can cause problems, such as preventing needed oxygen and nutrients from reaching the fetus or causing vaginal bleeding 8.
- Maternal medical conditions, such as diabetes mellitus or high blood pressure
Maternal indications for Cesarean section 9:
- Prior cesarean delivery
- Maternal request
- Pelvic deformity or cephalopelvic disproportion
- Previous perineal trauma
- Prior pelvic or anal/rectal reconstructive surgery
- Herpes simplex or HIV infection
- Cardiac or pulmonary disease
- Cerebral aneurysm or arteriovenous malformation
- Pathology requiring concurrent intraabdominal surgery
- Perimortem cesarean
Uterine and anatomic indications for Cesarean birth 9:
- Abnormal placentation (such as placenta previa, placenta accreta)
- Placental abruption
- Prior classical hysterotomy
- Prior full-thickness myomectomy
- History of uterine incision dehiscence
- Invasive cervical cancer
- Prior trachelectomy
- Genital tract obstructive mass
- Permanent cerclage
Fetal indications for Cesarean birth 10:
- Nonreassuring fetal status (such as abnormal umbilical cord Doppler study) or abnormal fetal heart tracing
- Umbilical cord prolapse
- Failed operative vaginal delivery
- Malpresentation
- Macrosomia
- Congenital anomaly
- Thrombocytopenia
- Prior neonatal birth trauma
If there’s time to plan the procedure, your midwife or doctor will discuss the benefits and risks of a cesarean compared with a vaginal birth.
Is a cesarean birth necessary if I have had a previous cesarean birth?
Women who have had a cesarean birth before may be able to give birth vaginally. The decision depends on the type of incision used in the previous cesarean delivery, the number of previous cesarean deliveries, whether you have any conditions that make a vaginal delivery risky, and the type of hospital in which you have your baby, as well as other factors. Talk to your obstetrician–gynecologist (ob-gyn) or other health care professional about your options.
Can I request cesarean birth?
Some women choose to have a cesarean for non-medical reasons. If you ask your midwife or doctor for a cesarean when there aren’t medical reasons, they will explain the overall benefits and risks of a cesarean compared with a vaginal birth.
Regardless of the type of delivery, unless there is a medical necessity, delivery should not occur before 39 weeks of pregnancy (called “full term”).
If you’re anxious about giving birth, you should be offered the chance to discuss your anxiety with a healthcare professional who can offer support during your pregnancy and labor.
If after discussion and support you still feel that a vaginal birth isn’t an acceptable option, you’re entitled to have a planned cesarean.
Cesarean section procedure
Cesarean sections are carried out in hospital. You may be asked to come in for an appointment a few days beforehand, and you might need to stay in hospital for a few days afterwards.
Preoperative appointment
If there’s time to plan your cesarean, you’ll be given an approximate date for it to be carried out.
You’ll also be asked to attend an appointment at the hospital in the week before the procedure is due to be performed.
During this appointment:
- you can ask any questions you have about the procedure
- a blood test will be carried out to check for a lack of red blood cells (anemia)
- you’ll be given some medication to take before the procedure – this may include antibiotics, anti-sickness medication (anti-emetics) and medication to reduce the acidity of your stomach acid (antacids)
- you’ll be asked to sign a consent form
You’ll need to stop eating and drinking a few hours before the procedure – your doctor or midwife will tell you when.
Cesarean section preparation
You’ll be asked to change into a hospital gown when you arrive at the hospital on the day of the procedure.
Before you have a cesarean delivery, a nurse will prepare you for the operation. An intravenous line (IV) will be put in a vein in your arm or hand. This allows you to get fluids and medications during the surgery. Your abdomen will be washed, and your pubic hair may be clipped or trimmed. You will be given medication to prevent infection.
A thin, flexible tube called a catheter will be inserted into your bladder to empty it while you’re under the anaesthetic, and a small area of pubic hair will be trimmed if necessary. Keeping the bladder empty decreases the chance of injuring it during surgery.
You’ll be given the anaesthetic in the operating room. You will be given either general anesthesia, an epidural block, or a spinal block. If general anesthesia is used, you will not be awake during the delivery. An epidural block numbs the lower half of the body. An injection is made into a space in your spine in your lower back. A small tube may be inserted into this space so that more of the drug can be given through the tube later, if needed. A spinal block also numbs the lower half of your body. You receive it the same way as an epidural block, but the drug is injected directly into the spinal fluid. This means you’ll be awake during the delivery and can see and hold your baby straight away.
It also means your birth partner can be with you.
General anaesthetic – where you’re asleep – is used in some cases if you can’t have a spinal or epidural anaesthetic.
What happens during cesarean surgery
During the cesarean section procedure:
- you lie down on an operating table, which may be slightly tilted to begin with
- a screen is placed across your tummy so you can’t see the operation being done
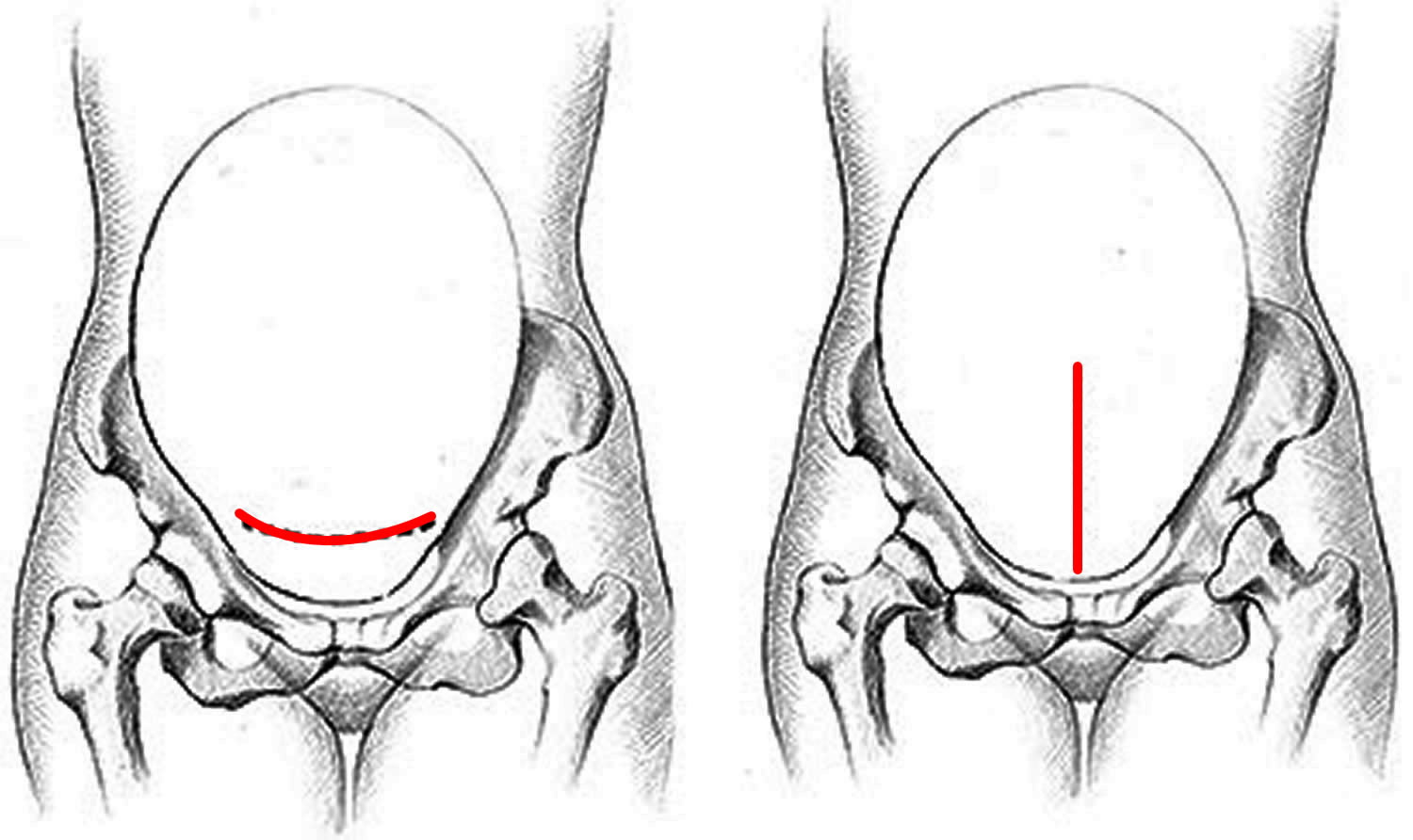
- a 10-20cm cut is made in your tummy and womb – the skin incision may be transverse (horizontal or “bikini”) cut just below your bikini line although sometimes a vertical cut below your bellybutton may be made
- the muscles in your abdomen are separated and may not need to be cut. Another incision will be made in the wall of the uterus. The incision in the wall of the uterus also will be either transverse or vertical.
- your baby is delivered through the opening, the umbilical cord will be cut, and then the placenta will be removed– this usually takes 5-10 minutes and you may feel some tugging at this point
- your baby will be lifted up for you to see as soon as they’ve been delivered, and they’ll be brought over to you
- you’re given an injection of the hormone oxytocin once your baby is born to encourage your womb to contract and reduce blood loss
- your womb is closed with dissolvable stitches, and the cut in your tummy is closed either with dissolvable stitches, or stitches or staples that need to be removed after a few days
The whole procedure usually takes around 40-50 minutes.
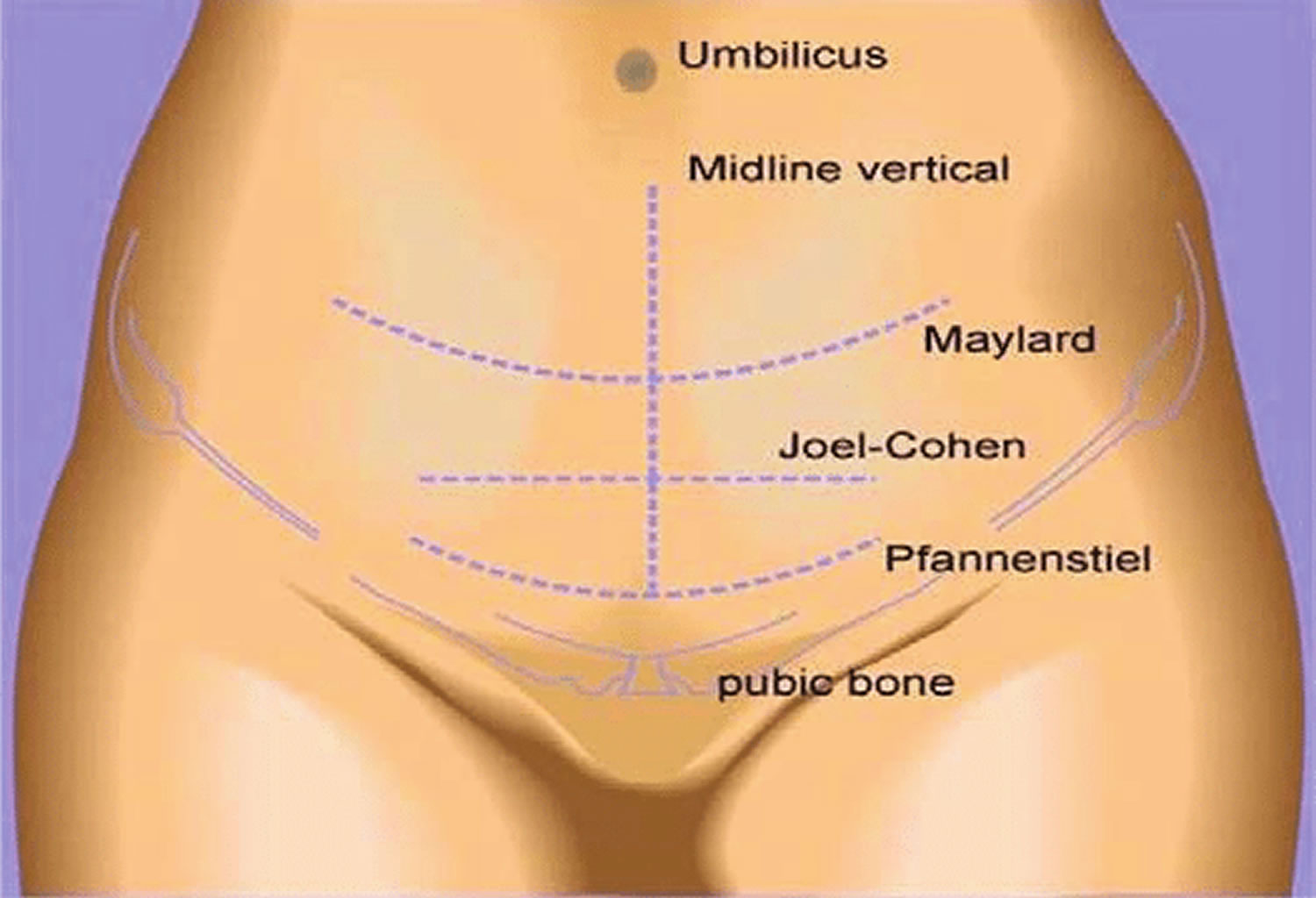
Cesarean section techniques
The four main cesarean section techniques are:
- Pfannenstiel-Kerr method
- Joel-Cohen method
- Misgav-Ladach method
- Modified Misgav-Ladach method
The cesarean section is a complicated procedure.During the surgery itself, several techniques are utilizable at each step or tissue layer. Many factors contribute to a surgeon’s decisions on technique. As with any aspect of medical practice, basing those decisions on evidence is recommended.
The following is a summary of the four general operative methods 11:
Figure 2. Cesarean section techniques
Pfannenstiel-Kerr method
- Pfannenstiel skin incision
- Sharp dissection of the subcutaneous layer
- Sharp extension of the fascial opening
- Sharp entry into the peritoneum
- Sharp superficial then blunt entry into the uterus
- Manual removal of the placenta
- Single-layer interrupted closure of the uterus
- Closure of the peritoneum
- Interrupted closure of the fascia
- Continuous suture of the skin
Joel-Cohen method
- Joel-Cohen skin incision
- Blunt dissection of the subcutaneous layer
- Blunt extension of the fascial opening
- Blunt entry into the peritoneum
- Sharp superficial then blunt entry into the uterus
- Spontaneous removal of the placenta
- Single-layer interrupted closure of the uterus
- Non-closure of the peritoneum
- Interrupted closure of the fascia
- Continuous suture of the skin
Misgav-Ladach method
- Joel-Cohen skin incision
- Blunt dissection of the subcutaneous layer
- Blunt extension of the fascial opening
- Blunt entry into the peritoneum
- Sharp superficial then blunt entry into the uterus
- Manual removal of the placenta
- Single-layer running closure of the uterus
- Non-closure of the peritoneum
- Continuous closure of the fascia
- Mattress suture closure of the skin
Modified Misgav-Ladach method
- Pfannenstiel skin incision
- Blunt dissection of the subcutaneous layer
- Blunt extension of the fascial opening
- Blunt entry into the peritoneum
- Sharp superficial then blunt entry into the uterus
- Spontaneous removal of the placenta
- Single-layer running closure of the uterus
- Closure of the peritoneum
- Continuous closure of the fascia
- Continuous suture of the skin
Cesarean section recovery
You’ll usually be moved from the operating room to a recovery room straight after the cesarean section procedure. If you are awake for the surgery, you can probably hold your baby right away.
Once you’ve started to recover from the anaesthetic, the medical staff will make sure you’re well and continue to observe you every few hours. Your blood pressure, pulse rate, breathing rate, amount of bleeding, and abdomen will be checked regularly.
If you are planning on breastfeeding, be sure to let your doctor know.
Having a cesarean delivery does not mean you will not be able to breastfeed your baby. You should be able to begin breastfeeding right away.
You’ll be offered:
- painkillers to relieve any discomfort
- treatment to reduce the risk of blood clots – this may include compression stockings or injections of blood-thinning medication, or both
- food and water as soon you as you feel hungry or thirsty
- help with breastfeeding your baby if you want it – read more about the first few days of breastfeeding
The catheter will usually be removed from your bladder around 12-18 hours after the procedure, once you’re able to walk around.
You may be in hospital for a few days after a cesarean section, and may need to take things easy for several weeks.
Recovering in hospital
The average stay in hospital after a cesarean is around three or four days. You may be able to go home sooner than this if both you and your baby are well.
While in hospital:
- you’ll be given painkillers to reduce any discomfort
- you’ll have regular close contact with your baby and can start breastfeeding
- you’ll be encouraged to get out of bed and move around as soon as possible. The first few times you get out of bed, a nurse or other adult should help you.
- you can eat and drink as soon as you feel hungry or thirsty
- a thin, flexible tube called a catheter will remain in your bladder for at least 12 hours
- your wound will be covered with a dressing for at least 24 hours
A hospital stay after a cesarean birth usually is 2–4 days. The length of your stay depends on the reason for the cesarean birth and on how long it takes for your body to recover.
When you’re well enough to go home, you’ll need to arrange for someone to give you a lift as you won’t be able to drive for a few weeks.
When you go home, you may need to take special care of yourself and limit your activities.
Looking after your wound
The abdominal incision will be sore for the first few days. Your midwife should also advise you on how to look after your wound.
Your doctor can prescribe pain medication for you to take after the anesthesia wears off. A heating pad may be helpful. There are many different ways to control pain. Talk with your ob-gyn or other health care professional about your options.
You’ll usually be advised to:
- gently clean and dry the wound every day
- wear loose, comfortable clothes and cotton underwear
- take painkillers if the wound is sore – see controlling pain
- watch out for signs of infection – see when to get medical advice
Non-dissolvable stitches or staples will usually be taken out by your midwife after five to seven days.
Your cesarean section scar
The wound in your tummy will eventually form a scar.
This will usually be a horizontal scar about 10-20cm long, just below your bikini line.
In rare cases, you may have a vertical scar just below your belly button.
The cesarean section scar will probably be red and obvious at first, but it should fade with time and will often be hidden in your pubic hair.
Controlling pain and bleeding
Most women experience some discomfort for the first few days after a cesarean, and for some women the pain can last several weeks.
You should be given regular painkillers to take at home, for as long as you need them.
Paracetamol is usually recommended for mild pain, co-codamol for moderate pain, and a combination of co-codamol and ibuprofen for more severe pain.
You may also have some vaginal bleeding. Use sanitary pads rather than tampons to reduce the risk of spreading infection into the vagina, and get medical advice if the bleeding is heavy.
What should I expect during recovery?
While you recover, the following things may happen:
- Mild cramping, especially if you are breastfeeding
- Bleeding or discharge for about 4–6 weeks
- Bleeding with clots and cramps
- Pain in the incision
To prevent infection, for a few weeks after the cesarean birth you should not place anything in your vagina or have sex. Allow time to heal before doing any strenuous activity. Call your Obstetrician–Gynecologist or other health care professional if you have a fever, heavy bleeding, or the pain gets worse.
If you experience severe mood swings, loss of appetite, overwhelming fatigue and lack of joy in life shortly after childbirth, you might have postpartum depression. Contact your health care provider if you think you might be depressed, especially if your signs and symptoms don’t fade on their own, you have trouble caring for your baby or completing daily tasks, or you have thoughts of harming yourself or your baby.
The American College of Obstetricians and Gynecologists recommends that postpartum care be an ongoing process rather than just a single visit after your delivery. Have contact with your health care provider within the first three weeks after delivery. Within 12 weeks after delivery, see your health care provider for a comprehensive postpartum evaluation. During this appointment your health care provider will check your mood and emotional well-being, discuss contraception and birth spacing, review information about infant care and feeding, talk about your sleep habits and issues related to fatigue and do a physical exam. This might include a check of your abdomen, vagina, cervix and uterus to make sure you’re healing well. In some cases, you might have the checkup earlier so that your health care provider can examine your C-section incision. Use this visit to ask questions about your recovery and caring for your baby.
Returning to your normal activities
Try to stay mobile and do gentle activities, such as going for a daily walk, while you’re recovering to reduce the risk of blood clots. Be careful not to overexert yourself.
You should be able to hold and carry your baby once you get home. But you may not be able to do some activities straight away, such as:
- driving
- exercising
- carrying anything heavier than your baby
- having sex
Only start to do these things again when you feel able to do so and don’t find them uncomfortable. This may not be for six weeks or so.
Ask your midwife for advice if you’re unsure when it’s safe to start returning to your normal activities. You can also ask your doctor at your six-week postnatal check.
When to get medical advice
Contact your midwife or Obstetrician–Gynecologist straight away if you have any of the following symptoms after a cesarean:
- severe pain
- leaking urine
- pain when peeing
- heavy vaginal bleeding
- your wound becomes more red, painful and swollen
- a discharge of pus or foul-smelling fluid from your wound
- a cough or shortness of breath
- swelling or pain in your lower leg
These symptoms may be the sign of an infection or blood clot, which should be treated as soon as possible.
Cesarean section complications
A cesarean section is generally a very safe procedure, but like any type of surgery it carries a certain amount of risk of complications. The maternal mortality rate in the USA is approximately 2.2 per 100,000 cesarean deliveries 12. Though this is overall low, it is significantly greater than for vaginal delivery. The maternal mortality for a vaginal birth is approximately 0.2 per 100,000 12.
It’s important to be aware of the possible complications, particularly if you’re considering having a cesarean for non-medical reasons.
The level of risk will depend on things such as whether cesarean section procedure is planned or carried out as an emergency, and your general health.
If there’s time to plan your cesarean section, your doctor or midwife will talk to you about the potential risks and benefits of the procedure.
Possible complications include:
- infection of the wound or womb lining
- blood clots in the legs, pelvic organs, or lungs
- excessive bleeding
- damage to nearby areas, such as the bowel or the bladder or the tubes that connect the kidneys and bladder (ureter)
- temporary breathing difficulties in your baby
- accidentally cutting your baby when your womb is opened.
As with any delivery and with surgery in general, there is a risk of excessive bleeding during and after a cesarean section. Bleeding (hemorrhage) is the leading cause in the United States of serious maternal morbidity 13. Certain conditions preceding a cesarean, such as prolonged labor or fetal macrosomia or polyhydramnios, may increase the risk of uterine atony and subsequent hemorrhage. Intraoperative conditions such as the need for significant adhesiolysis or extension of the hysterotomy laterally into the uterine vessels could also lead to excessive blood loss. Hemorrhage during delivery may then lead to the need for blood product transfusion, which itself has risks of complications. Sheehan syndrome is a known complication of hemorrhage at delivery 13. Approximately ten percent of maternal mortality in the United States is secondary to obstetric hemorrhage 13.
As previously discussed, there is a significant risk of infection after cesarean delivery. In addition to postpartum hemorrhage, wound infection and endometritis are the other most common complications that occur after a cesarean section. In a study 14 examining the efficacy of vaginal cleansing, postoperative endometritis was reduced from 8.7% to 3.8% with cleansing. A study 15 investigating adjunctive azithromycin saw a decrease in wound infection from 6.6% to 2.4% with the additional antibiotic, and serious adverse events decreased from 2.9% to 1.5%. However, given that over a million women have a cesarean every year, these percentages still represent a significant number of women suffering from infectious complications.
In data reported in 2010, the overall risk of infectious morbidity was 3.2% in elective repeat cesarean deliveries as compared to 4.6% in women undergoing a trial of labor 3. This same data reported elective repeat cesareans to have a blood transfusion rate of 0.46%, a surgical injury rate of 0.3 to 0.6%, and a hysterectomy rate of 0.16% 3. Thromboembolism and anesthetic complications can also occur.
While the cesarean section often has the perception of being safer for the fetus, there are risks to fetal delivery in this fashion. The risk of fetal trauma during cesarean is approximately 1%, including skin laceration, fracture of the clavicle or skull, facial or brachial plexus nerve damage, and cephalohematoma 16. Overall, these risks are lower than in vaginal deliveries. With regards to the neonate, there are risks of respiratory complications as well as higher rates of asthma and allergy in those born via cesarean compared to vaginal delivery 3. In 2010 transient tachypnea of the newborn was reported in 4.2% of elected repeat cesareans, and the need for bag-and-mask ventilation was 2.5% 3.
In addition to short-term and surgical risks, cesarean delivery also confers long-term risk, both to the patient and to her subsequent pregnancies. As stated previously, the presence of a vertical scar on the uterus requires a woman to delivery subsequent pregnancies via cesarean. As the number of cesarean sections increases, so too do the surgical risks. Adhesion formation can make each subsequent cesarean more difficult and increase the risk of inadvertent injury. The risks of abnormal placentation also increase with each subsequent surgery. For a woman who has had one cesarean section, the risk of placenta accreta is 0.3%, while the risk increases to 6.74% with five or more cesarean deliveries 17. A morbidly adherent placenta carries with it a risk of significant hemorrhage and possible loss of fertility if a hysterectomy becomes necessary.
Risks to you
Some of the main risks to you of having a cesarean section include:
- infection of the wound (common) – causing redness, swelling, increasing pain and discharge from the wound
- infection of the womb lining (common) – symptoms include a fever, tummy pain, abnormal vaginal discharge and heavy vaginal bleeding
- excessive bleeding (uncommon) – this may require a blood transfusion in severe cases or possibly further surgery to stop the bleeding
- deep vein thrombosis (DVT) (rare) – a blood clot in your leg, which can cause pain and swelling and could be very dangerous if it travels to the lungs (pulmonary embolism)
- damage to your bladder or the tubes that connect the kidneys and bladder (rare) – this may require further surgery
- reaction to medications or to the anesthesia that is used
Women are now given antibiotics before having a cesarean, which should mean infections become much less common.
Risks to your baby
A cesarean doesn’t affect the risk of some of the rarest and most serious birth complications, such as an injury to the nerves in the neck and arms, bleeding inside the skull, or death.
But a cesarean section can sometimes cause the following problems in babies:
- a cut in the skin (common) – this may happen accidentally as your womb is opened, but it’s usually minor and heals without any problems
- breathing difficulties (common) – this most often affects babies born before 39 weeks of pregnancy; it will usually improve after a few days and your baby will be closely monitored in hospital
If you think your baby is experiencing breathing difficulties after you’ve left hospital, contact your doctor straight away.
Risks to future pregnancies
Women who have a cesarean will usually have no problems with future pregnancies.
Most women who have had a cesarean section can safely have a vaginal delivery for their next baby – known as vaginal birth after cesarean. But sometimes another cesarean may be necessary.
Although uncommon, having a cesarean can increase the risk of certain problems in future pregnancies, including:
- the scar in your womb opening up
- the placenta being abnormally attached to the wall of the womb, leading to difficulties delivering the placenta
- stillbirth
Speak to your doctor or midwife if you have any concerns.
Vaginal birth after cesarean section
If you’ve delivered a baby by C-section and you’re pregnant again, you might be able to choose between scheduling a repeat C-section or attempting vaginal birth after C-section (vaginal birth after cesarean section).
For many women, vaginal birth after cesarean section is an option. In fact, research on women who attempt a trial of labor after cesarean shows that about 60 to 80 percent have a successful vaginal delivery.
Vaginal birth after cesarean section isn’t right for everyone, though. Certain factors, such as a high-risk uterine scar, can make vaginal birth after cesarean section inappropriate. Some hospitals don’t offer vaginal birth after cesarean section because they don’t have the staff or resources to handle emergency C-sections. If you’re considering vaginal birth after cesarean section, your health care provider can help you understand if you’re a candidate and what’s involved.
Why vaginal birth after cesarean section is done?
Women consider vaginal birth after cesarean section for various reasons, including:
- Shorter recovery time. You’ll have a shorter hospital stay after a vaginal birth after cesarean section than you would after a repeat C-section. Avoiding surgery will help your energy and stamina return more quickly, as well as reduce the expense of childbirth.
- More participation in the birth. For some women, it’s important to experience a vaginal delivery. Your labor coach and others also may be able to play a greater role.
- Impact on future pregnancies. If you’re planning a larger family, vaginal birth after cesarean section might help you avoid the risks of multiple cesarean deliveries.
The chances of a successful vaginal birth after cesarean section are higher if:
- You’ve had only one prior low transverse uterine incision — the most common type for a C-section
- You and your baby are healthy and your pregnancy is progressing normally
- The reason you had your prior C-section isn’t a factor this time
- Your labor begins naturally on or before your due date
- You’ve had a previous successful vaginal delivery
The chances of a successful vaginal birth after cesarean section are lower if:
- Your pregnancy continues beyond your due date
- You have an unusually large baby — suspected fetal macrosomia
- You’ve had two or more cesarean sections
You’re not a candidate for vaginal birth after cesarean section if you had a uterine rupture during a previous pregnancy. Similarly, vaginal birth after cesarean section isn’t recommended if you have had a vertical incision in the upper part of your uterus (classical incision) due to the risk of uterine rupture.
Vaginal birth after cesarean section risks
Vaginal birth after cesarean section poses potentially serious risks, including:
- Failed attempt at labor. Labor can results in a repeat C-section.
- Uterine rupture. Rarely, the uterus might tear open along the scar line from a prior C-section. If your uterus ruptures, an emergency C-section is needed to prevent life-threatening complications, including heavy bleeding and infection for the mother and brain damage for the baby. In some cases, the uterus might need to be removed (hysterectomy) to stop the bleeding. If your uterus is removed, you won’t be able to get pregnant again.
How you prepare for vaginal birth after cesarean section
If you choose vaginal birth after cesarean section, boost your odds of a positive experience:
- Learn about vaginal birth after cesarean section. Take a childbirth class on vaginal birth after cesarean section. Include your partner or another loved one, if possible. Also discuss your concerns and expectations with your health care provider. Make sure he or she has your complete medical history, including records of your previous cesarean section and any other uterine procedures.
- Plan to deliver the baby at a well-equipped hospital. Close monitoring can decrease the risk of complications. Look for a facility that’s equipped to handle an emergency cesarean section.
- Allow labor to begin naturally, if you can. Drugs to induce labor can make contractions stronger and more frequent, which might contribute to the risk of uterine rupture — especially if the cervix is tightly closed and not ready for labor.
- Be prepared for a cesarean section. Some complications of pregnancy or delivery might require a cesarean section. For example, you might need a cesarean section if there’s a problem with the placenta or umbilical cord, your baby is in an abnormal position or your labor fails to progress.
What you can expect
If you choose vaginal birth after cesarean section, your prenatal care will be just like the care you’d receive during any other healthy pregnancy.
When you go into labor, you’ll follow the same process as any woman expecting to deliver vaginally — although you and your baby will be more closely monitored during labor. Your health care provider will be prepared to do a repeat cesarean section if needed.
- Cesarean Birth (C-section). https://www.acog.org/Patients/FAQs/Cesarean-Birth-C-Section[↩]
- Sung S, Mahdy H. Cesarean Section. [Updated 2019 Nov 10]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK546707[↩]
- ACOG Practice Bulletin No. 205: Vaginal Birth After Cesarean Delivery. Obstet Gynecol. 2019 Feb;133(2):e110-e127[↩][↩][↩][↩][↩]
- Clapp MA, Barth WH. The Future of Cesarean Delivery Rates in the United States. Clin Obstet Gynecol. 2017 Dec;60(4):829-839.[↩]
- American College of Obstetricians and Gynecologists (College). Society for Maternal-Fetal Medicine. Caughey AB, Cahill AG, Guise JM, Rouse DJ. Safe prevention of the primary cesarean delivery. Am. J. Obstet. Gynecol. 2014 Mar;210(3):179-93.[↩]
- Walker SP, McCarthy EA, Ugoni A, Lee A, Lim S, Permezel M. Cesarean delivery or vaginal birth: a survey of patient and clinician thresholds. Obstet Gynecol. 2007 Jan;109(1):67-72.[↩]
- Chatfield, J. (2001). ACOG issues guidelines on fetal macrosomia. American Family Physician, 64(1), 169–170.[↩]
- American College of Obstetricians and Gynecologists. (2016). FAQ: Bleeding during pregnancy. https://www.acog.org/Patients/FAQs/Bleeding-During-Pregnancy[↩]
- Boyle A, Reddy UM, Landy HJ, Huang CC, Driggers RW, Laughon SK. Primary cesarean delivery in the United States. Obstet Gynecol. 2013 Jul;122(1):33-40.[↩][↩]
- Barber EL, Lundsberg LS, Belanger K, Pettker CM, Funai EF, Illuzzi JL. Indications contributing to the increasing cesarean delivery rate. Obstet Gynecol. 2011 Jul;118(1):29-38.[↩]
- Dahlke JD, Mendez-Figueroa H, Rouse DJ, Berghella V, Baxter JK, Chauhan SP. Evidence-based surgery for cesarean delivery: an updated systematic review. Am. J. Obstet. Gynecol. 2013 Oct;209(4):294-306.[↩]
- Clark SL, Belfort MA, Dildy GA, Herbst MA, Meyers JA, Hankins GD. Maternal death in the 21st century: causes, prevention, and relationship to cesarean delivery. Am. J. Obstet. Gynecol. 2008 Jul;199(1):36.e1-5; discussion 91-2. e7-11.[↩][↩]
- Committee on Practice Bulletins-Obstetrics. Practice Bulletin No. 183: Postpartum Hemorrhage. Obstet Gynecol. 2017 Oct;130(4):e168-e186.[↩][↩][↩]
- Haas DM, Morgan S, Contreras K, Enders S. Vaginal preparation with antiseptic solution before cesarean section for preventing postoperative infections. Cochrane Database Syst Rev. 2018 Jul 17;7:CD007892[↩]
- Tita ATN, Boggess K, Saade G. Adjunctive Azithromycin Prophylaxis for Cesarean Delivery. N. Engl. J. Med. 2017 Jan 12;376(2):182.[↩]
- Alexander JM, Leveno KJ, Hauth J, Landon MB, Thom E, Spong CY, Varner MW, Moawad AH, Caritis SN, Harper M, Wapner RJ, Sorokin Y, Miodovnik M, O’Sullivan MJ, Sibai BM, Langer O, Gabbe SG., National Institute of Child Health and Human Development Maternal-Fetal Medicine Units Network. Fetal injury associated with cesarean delivery. Obstet Gynecol. 2006 Oct;108(4):885-90.[↩]
- Marshall NE, Fu R, Guise JM. Impact of multiple cesarean deliveries on maternal morbidity: a systematic review. Am. J. Obstet. Gynecol. 2011 Sep;205(3):262.e1-8.[↩]

{kind=link}