
What is Familial Mediterranean fever
Familial Mediterranean fever is an autosomal recessive inherited autoinflammatory disease characterized by self-limited bouts of fever and recurrent episodes of painful inflammation of the abdominal lining (peritonitis), inflammation of the lining surrounding the lungs (pleurisy), painful, swollen joints (arthralgia and occasionally arthritis), and a characteristic ankle rash. These episodes are often accompanied by fever and sometimes a rash or headache. Occasionally inflammation may occur in other parts of the body, such as inflammation of the lining surrounding the heart (pericarditis); benign, recurrent inflammation of the membrane that surrounds the brain and spinal chord (meningitis); and in males, inflammation of the testis (orchitis). In about half of affected individuals, attacks are preceded by mild signs and symptoms known as a prodrome. Prodromal symptoms include mildly uncomfortable sensations in the area that will later become inflamed, or more general feelings of discomfort. Young children sometimes present with recurrent fevers alone. The frequency of Familial Mediterranean fever attacks is highly variable, both among groups of patients or for any individual patient, with the interval between attacks ranging from days to years. Moreover, the type of attack – whether abdominal, pleural or arthritic – may also vary over time.
The first episode of illness in Familial Mediterranean fever usually occurs in childhood or the teenage years, but in some cases, the initial attack occurs much later in life. 80 to 90 percent of patients experience their first episode by age 20. Typically, episodes last 12 to 72 hours and can vary in severity. The length of time between attacks is also variable and can range from days to years. During these periods, affected individuals usually have no signs or symptoms related to the condition. However, without treatment to help prevent attacks and complications, a buildup of amyloid protein deposits (amyloidosis) in the body’s organs and tissues may occur, especially in the kidneys. Potentially, amyloid protein deposits (amyloidosis) is the most serious complication of Familial Mediterranean fever, causing kidney failure. In some cases the amyloidosis can develop even without overt attacks of Familial Mediterranean fever.
As for other autoinflammatory syndromes, the skin is an important target tissue for inflammation. In Familial Mediterranean fever, the appearance of an erysipeloid erythema, typically monolateral and localized to the lower leg and on the dorsal surface of the foot, is pathognomonic in the context of systemic inflammation, including fever, serositis, and synovitis. However, the clinical significance of such a cutaneous feature is difficult to define in patients without a disease-associated history or in the absence of a positive genetic test finding.
Familial Mediterranean fever primarily affects populations originating in the Mediterranean region, particularly people of Armenian, Arab, Turkish, or Sephardic (non-Ashkenazi) Jewish ancestry. Among people with these backgrounds, about 1 in 200 has Familial Mediterranean fever. The availability of genetic testing has helped identify numerous cases among several additional populations with Mediterranean roots, including: Ashkenazi Jews, Italians, Greeks, Spaniards, and Cypriots, and occasional cases in a broad range of other ethnicities (Northern Europeans and Japanese). It is less common in other populations.
Familial Mediterranean fever is typically diagnosed during childhood. While there’s no cure for this disorder, you may be able to relieve signs and symptoms of Familial Mediterranean fever — or even prevent them altogether — by sticking to your treatment plan.
Untreated individuals with Familial Mediterranean fever have a risk of infertility. Individuals with severe Familial Mediterranean fever characterized by multiple frequent episodes and/or amyloidosis are particularly at risk if untreated. In males, inflammation of the testes (orchitis) may also occur. Orchitis is characterized by pain, redness and swelling.
Enlargement of the spleen can also occur (splenomegaly) and is quite frequent in children.
According to the medical literature, some individuals with Familial Mediterranean fever have an increased risk of developing additional inflammatory disorders, especially those characterized by inflammation of the blood vessels (vasculitides), including Bechet’s disease, polyarteritis nodosa, and Henoch-Schonlein purpura. Affected individuals may also have at greater risk of developing ulcerative colitis, Crohn’s disease and rheumatoid arthritis.
A common therapy for Familial Mediterranean fever is daily use of the drug colchicine, a medicine that reduces inflammation. This therapy has been successful in preventing attacks of fever in 75 percent of patients who take the drug regularly, and over 90 percent of patients demonstrate a marked improvement. Even if colchicine does not prevent the fever attacks, it does prevent the amyloidosis. However, compliance in taking colchicine every day is very important. If a patient stops taking the drug, an attack can occur within a couple of days.
Other names for Familial Mediterranean fever
- benign paroxysmal peritonitis
- familial paroxysmal polyserositis
- FMF
- MEF
- recurrent polyserositis
- Reimann periodic disease
- Siegal-Cattan-Mamou disease
- Wolff periodic disease
Figure 1. Familial Mediterranean fever rash
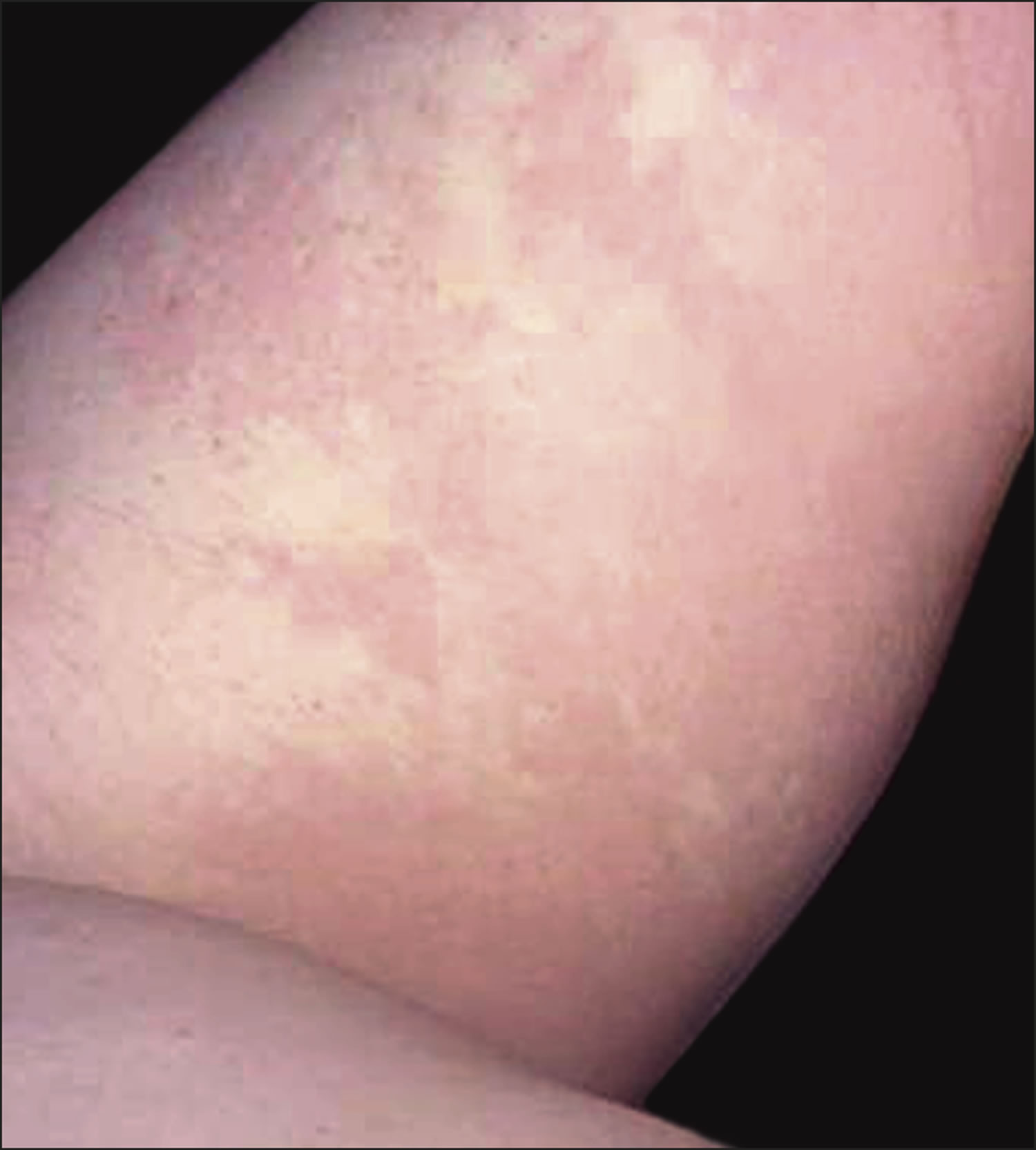
Figure 2. Familial Mediterranean fever ankle rash

Familial Mediterranean fever complications
Complications can occur if familial Mediterranean fever isn’t treated. Complications can include:
- Abnormal protein in the blood. During attacks of familial Mediterranean fever, your body may produce an abnormal protein (amyloid A). The protein can accumulate in your body and cause organ damage (amyloidosis).
- Kidney damage. Amyloidosis can damage the kidneys, causing nephrotic syndrome. Nephrotic syndrome occurs when your kidneys’ filtering systems (glomeruli) are damaged. People with this condition may lose large amounts of protein in their urine (proteinuria). Nephrotic syndrome can lead to blood clots in your kidneys (renal vein thrombosis) or kidney failure.
- Infertility in women. Inflammation caused by familial Mediterranean fever may also affect the female reproductive organs, causing infertility.
- Joint pain. Arthritis is common in people with familial Mediterranean fever. The most commonly affected joints are the knees, ankles, hips and elbows.
Familial Mediterranean fever and Amyloid A amyloidosis
A serious complication of Familial Mediterranean fever is development of amyloid A amyloidosis, which may lead to kidney failure. As well as preventing Familial Mediterranean fever attacks, regular colchicine treatment is effective in preventing development of amyloid A amyloidosis in most patients with Familial Mediterranean fever.
Some Familial Mediterranean fever patients taking colchicine may have on-going auto-inflammation despite experiencing few attacks. Serum amyloid A protein is a very sensitive marker of inflammation, so we monitor the serum amyloid A protein levels regularly in all our Familial Mediterranean fever patients. This is the best way to ensure that they are receiving sufficient doses of colchicine to suppress inflammation and prevent development of amyloid A amyloidosis.
Colchicine is usually effective in treatment of Familial Mediterranean fever patients who have already developed amyloid A amyloidosis. It can lead to regression of amyloid A amyloid deposits and improved kidney function.
Familial Mediterranean fever prognosis
There is no known cure for Familial Mediterranean fever. Most people continue to have attacks, but the number and severity of attacks is different from person to person.
Familial Mediterranean fever life expectancy
Compliant patients with daily colchicine can expect to have a normal lifespan if colchicine is started before proteinuria develops (signs of amyloidosis of kidneys). Even with amyloidosis, the use of colchicine, dialysis and renal transplantation should extend a patient’s life beyond age 50 years.
Familial Mediterranean fever causes
Familial Mediterranean fever is the commonest inherited fever syndrome. Located on the short (p) arm of chromosome 16, MEFV (MEditerranean FeVer) is the gene that, when mutated, causes Familial Mediterranean fever. The MEFV gene provides the instructions (codes) for creating a protein, called pyrin (also known as marenostrin), which is found in the white blood cells (granulocytes), which are important in the immune response, and myeloid bone marrow precursors. The pyrin protein (marenostrin) is involved in the immune system, helping to regulate the process of inflammation. Inflammation occurs when the immune system sends signaling molecules and white blood cells to a site of injury or disease to fight microbial invaders and facilitate tissue repair. When this process is complete, the body stops the inflammatory response to prevent damage to its own cells and tissues.
Mutations in the MEFV gene reduce the activity of the pyrin protein, which disrupts control of the inflammation process. An inappropriate or prolonged inflammatory response can result, leading to fever and pain in the abdomen, chest, or joints. There are more than 30 mutations in the MEFV gene known to cause FFamilial Mediterranean fever, but four of them are very common in the patients of Middle Eastern ancestry.
Normal variations in the SAA1 gene may modify the course of familial Mediterranean fever. Some evidence suggests that a particular version of the SAA1 gene (called the alpha variant) increases the risk of amyloidosis among people with familial Mediterranean fever.
Inheritance Pattern
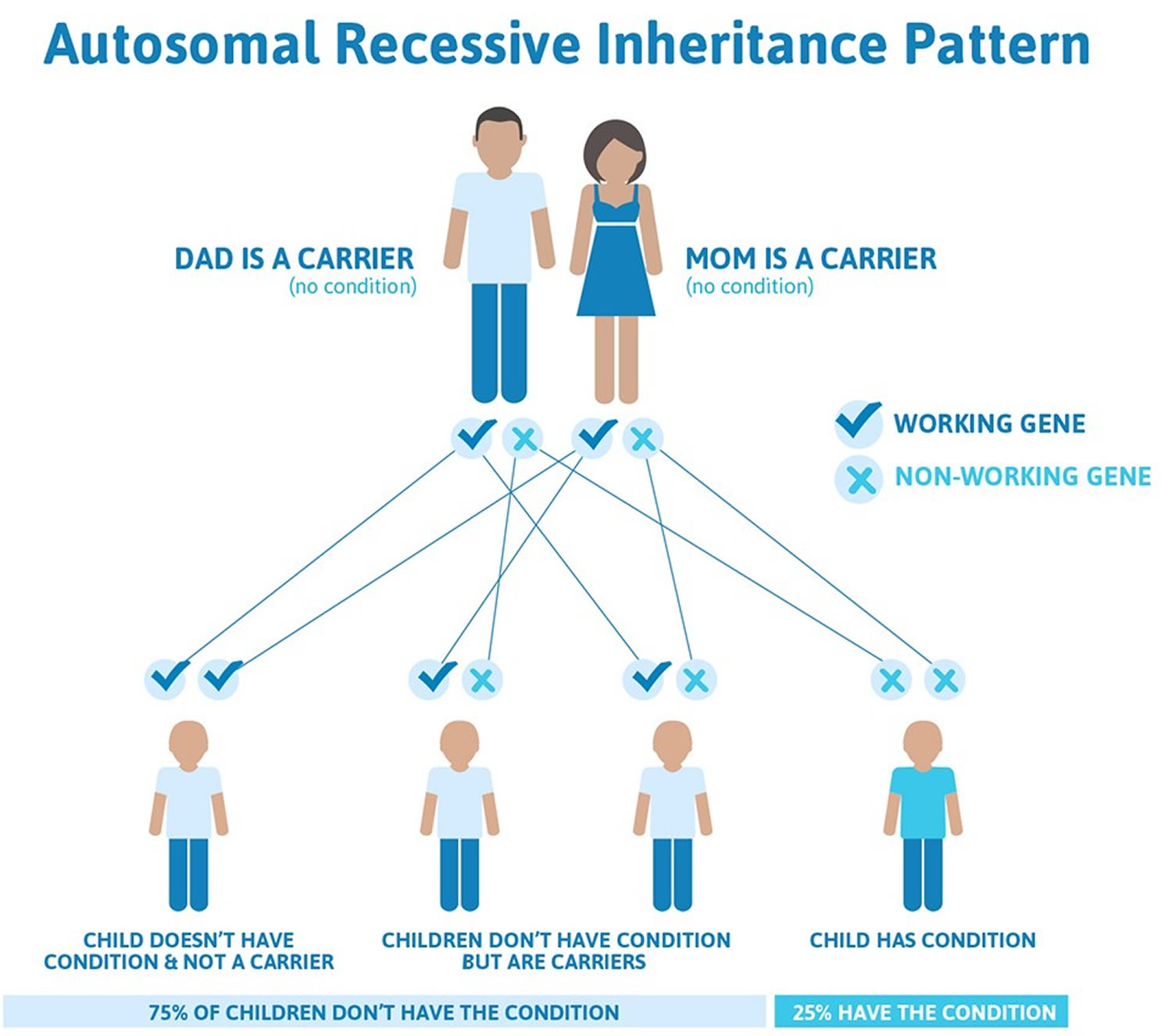
Familial Mediterranean fever is almost always inherited in an autosomal recessive pattern, which means both copies of the MEFV gene in each cell have mutations. The parents of an individual with an autosomal recessive condition each carry one copy of the mutated gene, but they typically do not show signs and symptoms of the condition. As many as 1 in 5 people of Sephardic (non-Ashkenazi) Jewish, Armenian, Arab and Turkish heritage have one mutant copy of the gene and are therefore carriers of Familial Mediterranean fever, which means they carry the mutant gene but do not suffer from Familial Mediterranean fever themselves.
More rarely, (when the deletion of M694 mutation is present), Familial Mediterranean fever may be inherited by autosomal dominant inheritance. This means that one abnormal copy of the gene can cause the disease, and people with Familial Mediterranean fever may have one affected parent. An autosomal dominant inheritance pattern describes cases in which one copy of the altered gene in each cell is sufficient to cause the disorder. In autosomal dominant inheritance, affected individuals often inherit the mutation from one affected parent.
However, another mechanism is believed to account for some cases of familial Mediterranean fever that were originally thought to be inherited in an autosomal dominant pattern. A gene mutation that occurs frequently in a population may result in a disorder with autosomal recessive inheritance appearing in multiple generations in a family, a pattern that mimics autosomal dominant inheritance. If one parent has familial Mediterranean fever (with mutations in both copies of the MEFV gene in each cell) and the other parent is an unaffected carrier (with a mutation in one copy of the MEFV gene in each cell), it may appear as if the affected child inherited the disorder only from the affected parent. This appearance of autosomal dominant inheritance when the pattern is actually autosomal recessive is called pseudodominance.
Figure 3. Familial Mediterranean fever autosomal recessive inheritance pattern
Risk factors for Familial Mediterranean fever
Factors that may increase the risk of familial Mediterranean fever include:
- Having a family history of the disease. If you have a family history of familial Mediterranean fever, your risk of the disease is increased.
- Being of Mediterranean ancestry. If your family can trace its history to the Mediterranean region, your risk of the disease may be increased. Familial Mediterranean fever can affect any ethnic group, but it may be more likely in Sephardic Jews, Arabs, Italians, Armenians and Turks.
Familial Mediterranean fever symptoms
Signs and symptoms of familial Mediterranean fever usually begin during childhood. They occur in bouts called attacks that last one to three days. Arthritic attacks may last for weeks or months.
Signs and symptoms of familial Mediterranean fever include:
- Fever
- Abdominal pain
- Chest pain
- Achy, swollen joints
- Constipation followed by diarrhea
- A red rash on your legs, especially below your knees
- Muscle aches
- Rarely (less than 5%), testicular pain and swelling, in children
The pain may be so severe that the first attack is thought to be appendicitis. Between attacks, you’ll likely feel normal and grow and develop normally. Symptom-free periods may be as short as a few days or as long as several years.
Some patients experience muscle pain on exertion between attacks, usually affecting the calves.
The frequency of the attacks varies from once every week to several times a year. The symptoms and severity vary between different patients, sometimes even amongst members of the same family.
The frequency of episodes is variable, ranging from weekly to every few years. Attacks may be triggered by:
- Exercise
- Infection
- Menstruation
- Stress.
Acute attacks settle spontaneously. Between episodes, health is normal.
The characteristics of the recurrent acute episodes of familial Mediterranean fever are described in the table below.
Table 1. Clinical features of Familial Mediterranean fever
| Symptom | Features |
|---|---|
| Fever |
|
| Abdominal pain |
|
| Chest pain |
|
| Joint pain and swelling (arthralgia, arthritis) |
|
| Skin rashes |
|
| Scrotal pain (orchitis) |
|
| Spleen enlargement (splenomegaly) |
|
| Muscle pain (myalgia) |
|
| Neurologic symptoms |
|
| Amyloidosis |
|
Familial Mediterranean fever diagnosis
Tests and procedures used to diagnose familial Mediterranean fever include:
- Physical exam. Your doctor may ask you about your signs and symptoms and conduct a physical exam to gather more information.
- Review of your family medical history. A family history of familial Mediterranean fever increases your likelihood of developing the condition because this genetic mutation is passed from parents to their children.
- Blood tests. During an attack, blood tests may show elevated levels of certain markers that indicate an inflammatory condition in your body. An elevated level of white blood cells, which fight infections, is one such marker.
- Genetic testing. Genetic testing may determine if your MEFV gene contains a mutation that is associated with familial Mediterranean fever. Genetic tests aren’t advanced enough to test for every gene mutation that’s linked to familial Mediterranean fever, so there is a possibility of false-negative results. For this reason, doctors typically don’t use genetic tests as the sole method of diagnosing familial Mediterranean fever.
- There are a few labs in the United States and Canada and a few more in Europe and the Middle East that are offering molecular or DNA testing for Familial Mediterranean Fever (Familial Mediterranean fever). Most centers, however, only test for a subset of the mutations that cause Familial Mediterranean fever, particularly those common in Familial Mediterranean fever patients.
In making a diagnosis of Familial Mediterranean Fever, doctors take all of these factors into account:
- Whether or not the patient has the clinical symptoms common for the disease and whether the symptoms are recurrent.
- How he or she responds to colchicine treatment.
- Usually a positive family history in people of Middle Eastern ancestry.
- The results of genetic testing.
Also helpful in establishing a correct diagnosis of Familial Mediterranean Fever is the patient’s ancestry. Testing for the following can also be helpful:
- Elevated white blood cell count, which is an indication of an immune response.
- Elevated erythrocyte sedimentation rate (ESR), which is an indication of an inflammatory response.
- Elevated plasma fibrinogen, which helps stop bleeding. An elevated amount would indicate that something might be wrong with this mechanism.
- Elevated serum haptoglobin, which would indicate that red blood cells are being destroyed, a common occurrence in rheumatic diseases, such as Familial Mediterranean Fever.
- Elevated C-reactive protein, which is a special type of protein, produced by the liver, that is only present during episodes of acute inflammation.
- Elevated albumin in the urine, which is demonstrated by urinalysis. The presence of the protein albumin in the urine can be a symptom of kidney disease, along with microscopic hematuria (very small – microscopic – amounts of blood or blood cells in the urine), during attacks.
Diagnosis of familial Mediterranean fever is made using the Tel-Hashomer criteria:
The diagnosis if definite if 2 major or 1 major + 2 minor criteria are met.
The diagnosis is probable if 1 major + 1 minor criteria are met.
Major criteria
- Recurrent febrile episodes associated with peritonitis, pleuritis or synovitis
- Amyloidosis of AA (amyloid A amyloidosis)-type without a predisposing disease
- Favorable response to daily colchicine
Minor criteria
- Recurrent febrile episodes
- Erysipelas-like erythema
- Positive history of familial Mediterranean fever in a first degree relative
Familial Mediterranean fever treatment
There’s no cure for familial Mediterranean fever. However, treatment can help prevent signs and symptoms.
Medications used to control signs and symptoms of familial Mediterranean fever include:
- Colchicine. Colchicine has been used successfully to treat Familial Mediterranean fever since 1972. This drug, taken in pill form, reduces inflammation in your body and helps prevent attacks. Work with your doctor to determine the best dosing strategy for you. Some people take one dose a day, while others need smaller, more-frequent doses. Colchicine is effective at preventing attacks in the vast majority of patients, so long as sufficient doses are taken. Colchicine has been very widely used and more than 30 years of experience in Familial Mediterranean fever has shown it to be very safe at the usual doses of 0.5 to 2mg per day. It may be safely given to children with Familial Mediterranean fever even before the age of 1 year. Children taking colchicine grow and develop completely normally. It is also safe during pregnancy. Common side effects include bloating, abdominal cramps and diarrhea. This can usually be avoided by increasing the dose slowly and in some individuals cutting out milk products for a period. Colchicine is dangerous if taken as an overdose and should always be kept out of reach of children. During acute attacks, other pain suppressing drugs may be helpful.
- The most common reason for failure to respond to colchicine is poor compliance due to gastrointestinal upset. However 5-10% do not respond to colchicine and this may be due to ABCB1 gene polymorphisms affecting colchicine uptake by mononuclear cells. Thalidomide and biologic agents, such as daily subcutaneous anakinra (an interleukin-1 receptor antagonist) or etanercept, may then be considered to prevent attacks and the development of amyloidosis. To reduce the severity of an attack, single dose methylprednisolone or anakinra at the start of episodes have been reported to relieve symptoms.
- Other drugs to prevent inflammation. For people whose signs and symptoms aren’t controlled with colchicine, other medications that control inflammation may be options, though these treatments are considered experimental. Other medications include rilonacept (Arcalyst) and anakinra (Kineret).
- Acute attacks are treated with non-steroidal anti-inflammatory drugs (NSAID) and pain relief.
Colchicine in pregnancy
It is very important for all patients with Familial Mediterranean fever to take colchicine regularly at all times. This treatment:
- controls auto-inflammation very effectively
- prevents development of amyloidosis
Most Familial Mediterranean fever patients are diagnosed in childhood or young adulthood.
Many patients are concerned about the effect on child-bearing potential both of Familial Mediterranean fever itself and of Familial Mediterranean fever treatment.
Some women with Familial Mediterranean fever enjoy a period free from attacks while pregnant. Others actually experience severe attacks during pregnancy that are worse than their usual attacks. These attacks may endanger the pregnancy itself, by causing miscarriage, if the Familial Mediterranean fever is not treated.
Colchicine use during the reproductive years has been studied extensively, and the results of all studies are clear:
- Colchicine is safe in pregnancy and breastfeeding.
- Colchicine has no effect on fertility in women or in men.
- Women should continue taking colchicine regularly, in the dose prescribed throughout the period when they are trying to conceive, and throughout pregnancy and breastfeeding.
- Men who are trying to conceive should continue taking colchicine regularly, in the dose prescribed.
In contrast, untreated Familial Mediterranean fever has been associated with:
- increased risk of miscarriage and infertility in women
- impaired functioning of the testicles, which may affect sperm production
- increased risk of premature birth and low weight babies
The chances of successful pregnancy outcome are actually better in patients who are careful to take their colchicine.
For many patients this information provides sufficient reassurance.
For those who wish to understand more, the evidence on which this advice is based is summarized below:
Review of the medical literature on colchicine in pregnancy
Colchicine has been used as standard treatment for Familial Mediterranean fever since 1972. Since then, 40 years have passed and hundreds of pregnant women with Familial Mediterranean fever have taken colchicine throughout pregnancy and given birth to healthy children. Several major research studies on colchicine in pregnancy have been published during this period of time. The results of these studies are extremely reassuring for women with Familial Mediterranean fever and are summarized below.
This comprehensive review of the medical literature is up to date as of December 2012:
- Fertility and obstetric history in patients with familial Mediterranean fever on long-term colchicine therapy 3.
- Colchicine Prophylaxis in Familial Mediterranean fever: reappraisal after 15 years 4
- Colchicine treatment in conception and pregnancy: two hundred thirty-one pregnancies in patients with familial Mediterranean fever 5
- Familial Mediterranean fever in the colchicine era: the fate of one family 6
- Familial Mediterranean fever and its implications for fertility and pregnancy 7
- Reproductive system in familial Mediterranean fever: an overview 8
- Safety of colchicine therapy during pregnancy 9
- Familial Mediterranean fever during pregnancy: an independent risk factor for preterm delivery 10
- Pregnancy outcomes in women with familial Mediterranean fever receiving colchicine: is amniocentesis justified? 11
- Pregnancy outcome after in utero exposure to colchicine 12
- The impact of familial Mediterranean fever on women’s health 13
- Pregnancy outcome in women with familial Mediterranean fever 14
Coping and support
Learning that you or your child has a chronic illness, such as familial Mediterranean fever, can be upsetting and frustrating. Here are some tips that may help you cope:
- Learn about Familial Mediterranean fever. Find out enough about familial Mediterranean fever so that you feel comfortable making decisions about your child’s care. Ask your doctor for good sources of information to get you started.
- Find someone to talk with. Talking to a family member, trusted friend, or a counselor or therapist can allow you to express your fears and frustrations. Some people also find support groups helpful because members truly understand what you’re going through. Ask your doctor if there is a support group for people affected by Familial Mediterranean fever in your area.
- Late-Onset Familial Mediterranean Fever: An Atypical Presentation of Dermatologic Interest. Arch Dermatol. 2007;143(8):1073–1087. doi:10.1001/archderm.143.8.1080[↩]
- Erysipelas-like Erythema in a Patient with Familial Mediterranean Fever. The Journal of Rheumatology November 2014, 41 (11) 2271-2272; DOI: https://doi.org/10.3899/jrheum.140324 http://www.jrheum.org/content/41/11/2271[↩]
- Ehrenfeld M et al. Br J Obstet Gynaecol. 1987 Dec;94(12):1186-91[↩]
- Ben-Chetrit E and Levy M. Semin Arthritis Rheum. 1991 Feb;20(4):241-6.[↩]
- Rabinovitch O et al. Am J Reprod Immunol. 1992 Oct-Dec;28(3-4):245-6.[↩]
- Zemer D et al. Am J Med Genet 1993;45:340-4.[↩]
- Mijatovic Vet al. Eur J Obstet Gynecol Reprod Biol. 2003 Jun 10;108(2):171-6.[↩]
- Ben-Chetrit E. and Levy M. Ann Rheum Dis. 2003 October; 62(10): 916–919.[↩]
- Ong M et al. Can Fam Physician. 2003 August; 49: 967–969.[↩]
- Ofir D et al. Eur J Obstet Gynecol Reprod Biol. 2008 Dec;141(2):115-8. Epub 2008 Sep 3.[↩]
- Ben-Chetrit E. et al. Arthritis Care Res (Hoboken). 2010 Feb;62(2):143-8.[↩]
- Diav-Citrin O et al. Am J Obstet Gynecol. 2010 Aug;203(2):144.e1-6. Epub 2010 Jul 1.[↩]
- Dotters-Katz S et al. Obstet Gynecol Surv. 2012 Jun;67(6):357-6.[↩]
- Nabil H et al. J Obstet Gynaecol. 2012 Nov;32(8):756-9.[↩]





{kind=link}