
What is flank pain
Flank pain or side pain, is a sensation of discomfort, distress, or agony in the part of the body below the rib and above the ilium, generally beginning posteriorly or in the midaxillary line and resulting from the stimulation of specialized nerve endings upon distention of the ureter or renal capsule. Similar pain is sometimes caused by extraurinary abnormalities. Flank pain can be a sign of a kidney problem. But, since many organs are in this area, other causes are possible. If you have flank pain and fever, chills, blood in the urine, or frequent or urgent urination, then a kidney problem is the likely cause. It could be a sign of kidney stones.
Flank pain is the presenting symptom of many significant diseases of the urinary system. Ureteral obstruction should be recognized promptly, especially when it is associated with infection, in order to prevent kidney damage. Progression of irreversible kidney damage resulting from ureteral obstruction is related to many factors including the duration of obstruction, degree of obstruction, presence or absence of infection above the obstruction, preexisting renal function, status of the opposite kidney, and age of the patient. An obstructed kidney has a greater potential for recovery if the opposite kidney has diminished function; a younger patient has a greater chance of recovery of function than an older patient.
An estimated two million patients present to the emergency room for acute flank pain annually 1. Radiographic evaluation of a patient with flank pain helps to diagnose the cause of the pain. The diagnostic tests available to assess the urinary causes of flank pain are numerous. Some of the tests are intravenous urography (IVP), ultrasonography, computerized tomography (CT scan), retrograde urography, diuretic renography, renal arteriography, and voiding cystourethrography. An efficient and cost-effective evaluation of flank pain can be done by carefully selecting the best diagnostic procedures based on a thorough history of the character of the flank pain and associated aspects of the patient’s history. Currently, computed tomography (CT) scan is the most commonly used imaging test, valued for its excellent sensitivity and specificity for ureteral stone and its ability to detect important alternative diagnoses, such as appendicitis, diverticulitis, and abdominal aortic aneurysm 2.
See your health care provider if you have any of the following:
- Flank pain along with a high fever, chills, nausea, or vomiting
- Blood (red or brown color) in the urine
- Unexplained flank pain that continues
Figure 1. Flank pain area
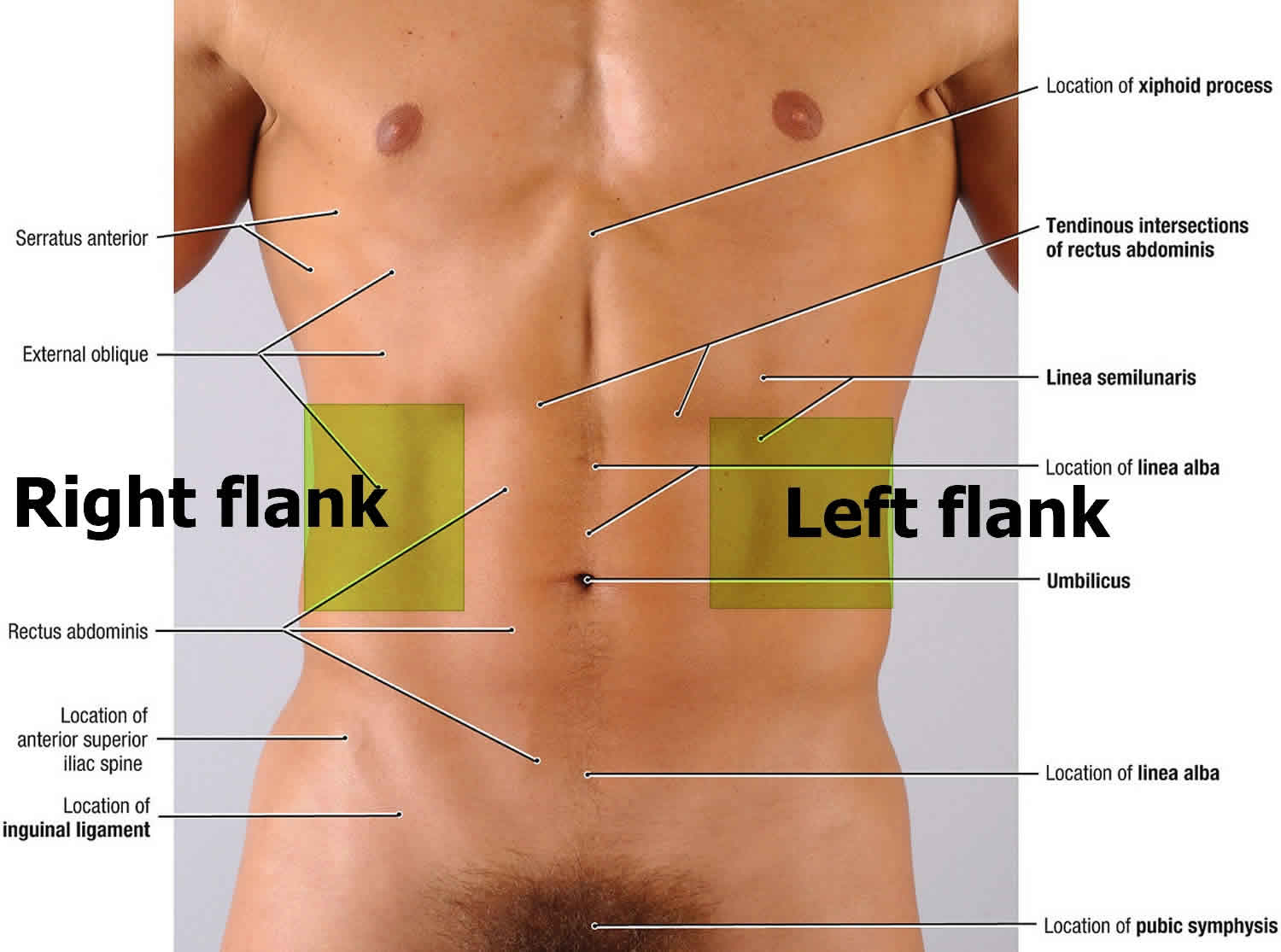
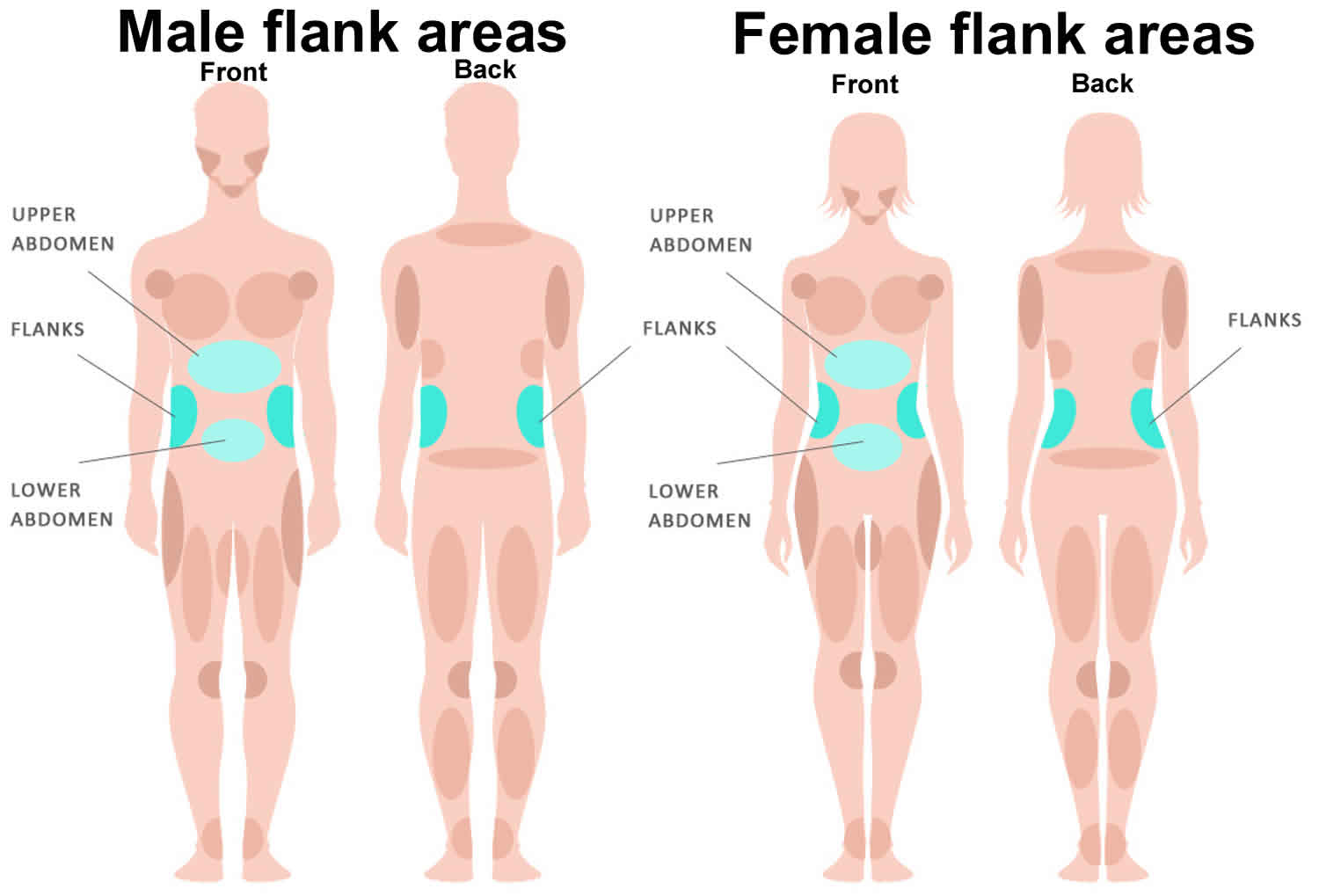
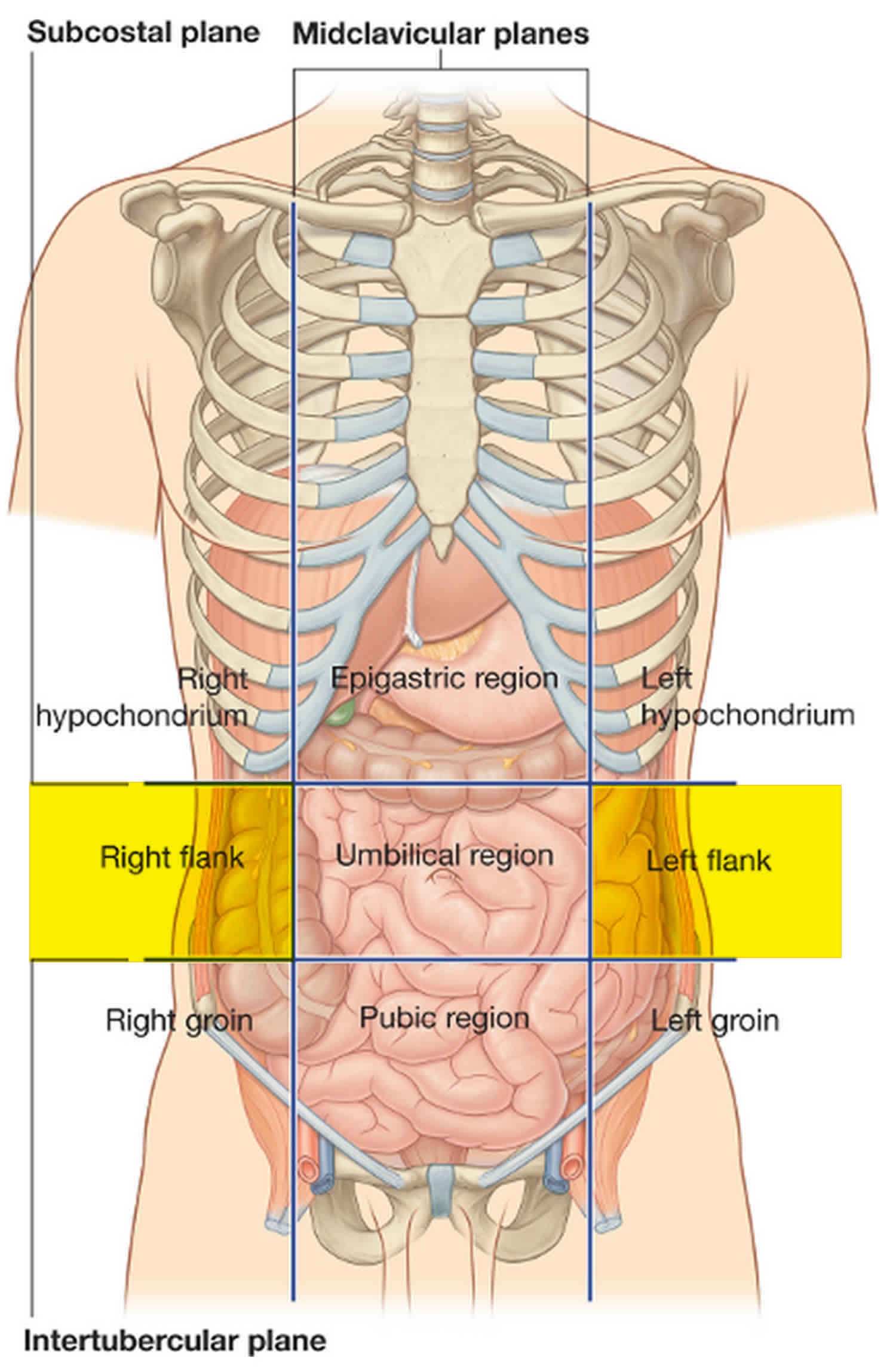
Figure 2. Kidney location
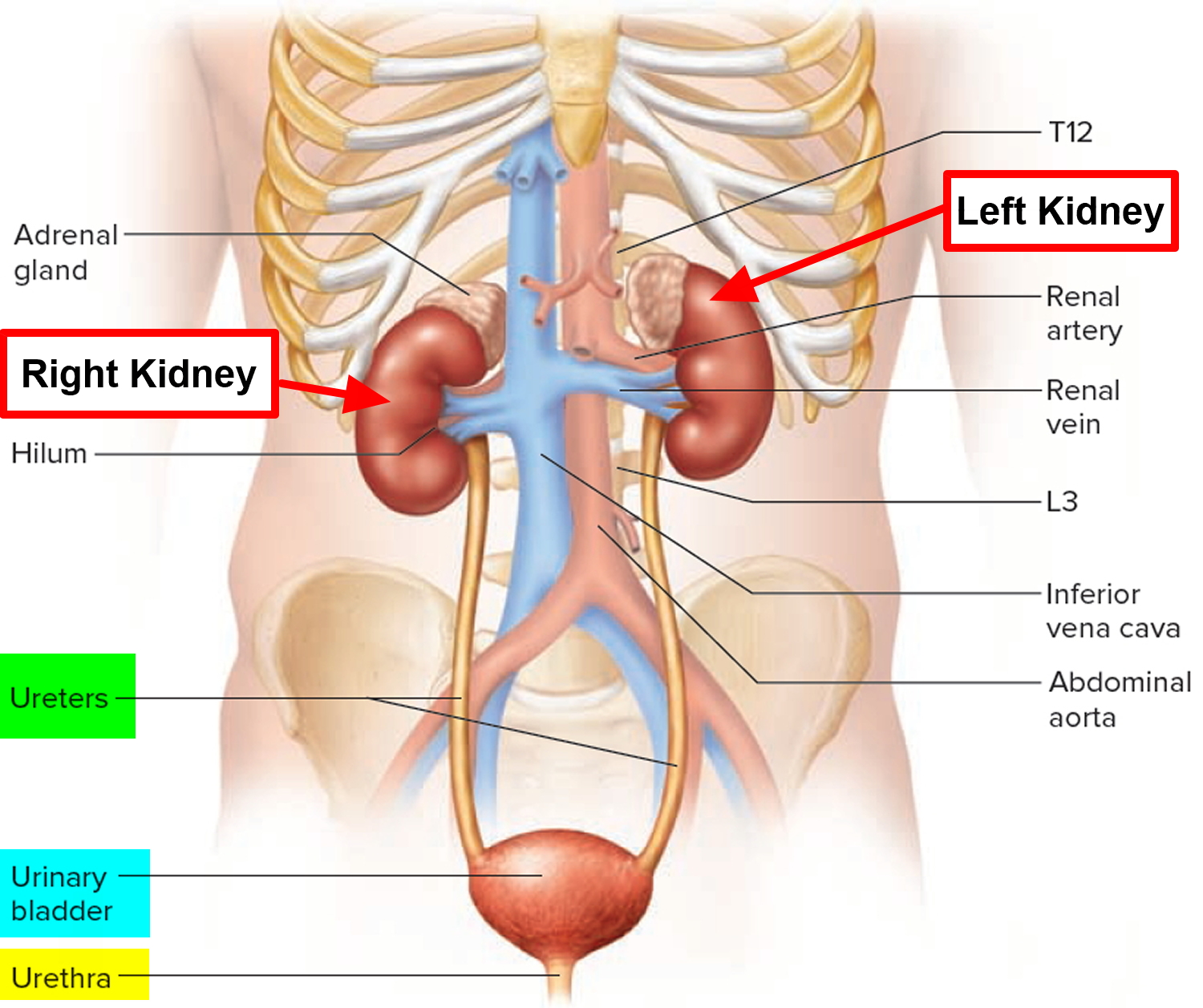
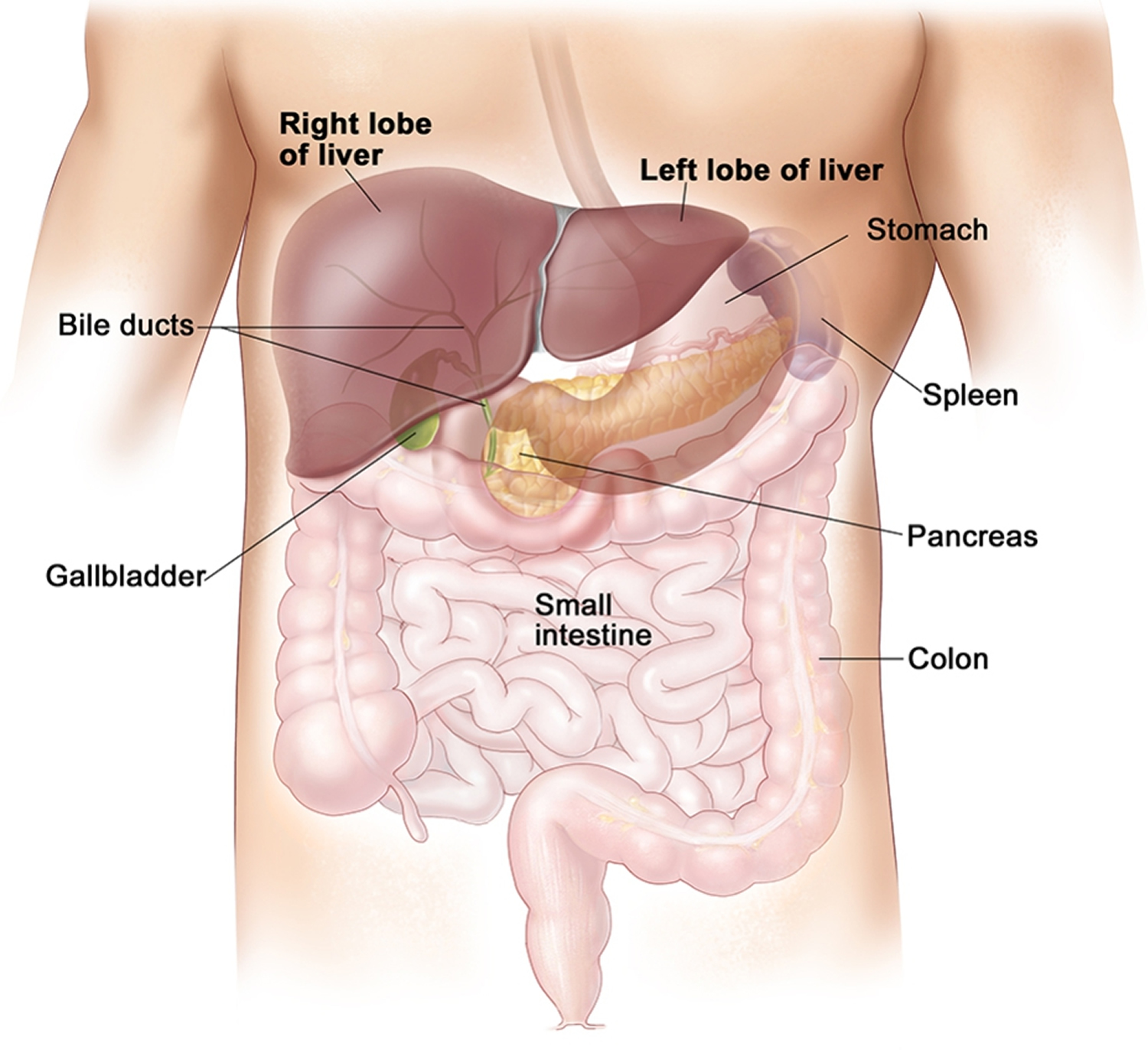
Figure 3. Location of the human liver and gallbladder
Flank pain causes
Flank pain may be caused by any of the following:
Urinary
- Acute ureteral obstruction
- Stone
- Blood clot
- Papillary necrosis
- Chronic ureteral obstruction
- Congenital anomaly
- Tumor
- Stricture of ureter
- Previous surgery
- Radiation therapy
- Retroperitoneal fibrosis
- Stone
- Kidney inflammation
- Acute pyelonephritis (kidney inflammation or infection)
- Perinephric abscess (kidney abscess)
- Kidney tumor
- Renal cell carcinoma
- Transitional cell carcinoma
- Wilms” tumor
- Trauma of kidney
- Renal infarction
- Vesicoureteral reflux
- Genitourinary abnormality (i.e. ureterocele)
Extraurinary
- Gallbladder disease e.g., gallstone, cholelithiasis (gallblader disease blocking the common bile duct), cholecystitis (inflammation of the gallblader)
- Liver disease e.g., hepatitis, portal hypertension, cirrhosis
- Appendicitis
- Diverticulitis or colitis
- Other gastrointestinal disease e.g., celiac disease, constipation, Crohn’s disease, ulcerative colitis, colon cancer, small bowel obstruction
- Intra-abdominal abscess
- Chest disease e.g., pneumonia or pleural effusion
- Salpingitis (inflammation of the fallopian tube) e.g., STD (sexually transmitted disease), PID (pelvic inflammatory disease)
- Arthritis or infection of the spine
- Back problem, such as disk disease
- Muscle spasm or musculoskeletal problems
- Shingles (pain with one-sided rash)
- Spinal fracture
- Non-specific pain
- Pancreatitis
- Cardiovascular
- Peptic ulcer disease or non-specific vomiting
- Testicular or ovarian torsion
- Soft tissue infection
- Hematoma
- Pulmonary embolism, deep vein thrombosis (DVT)
- Diabetic keto-acidosis
The character of flank pain is very helpful in determining the cause of the pain. Important characteristics include local or referred pain, acute or chronic or recurrent pain, degree of severity, and duration. Associated symptoms such as fever, nausea and vomiting, and atrial fibrillation often help in making the correct diagnosis.
Flank pain that radiates to the testicle is usually caused by proximal ureteral or renal pelvic obstruction due to the common innervation of the testicle and the renal pelvis (T11–12). This pain usually originates in the posterior part of the flank and radiates to the testicle of the male or the labia of the female. The pain becomes lower and more anterior in the flank when the obstruction occurs in the middle third of the ureter. The pain is still lower, radiates to the scrotal skin (rather than the testicle), and is associated with voiding symptoms such as urinary frequency and urgency when the obstruction occurs at the level of the ureterovesical junction.
The degree of severity of the pain is directly related to the acuteness of the obstruction rather than the degree of obstruction. Therefore, a kidney stone that passes into the ureter and suddenly becomes lodged in one position usually causes extremely severe pain. But flank pain can be very mild or absent in the presence of very severe but chronic obstruction. Mild and chronic flank pain associated with severe ureteral obstruction can produce irreversible renal damage. A stone passing through the ureter will often cause severe but intermittent pain. The intermittent pain is related to obstruction produced when the stone becomes lodged in the ureter. Therefore, each episode of pain is likely to be associated with a stone becoming lodged in a new and more distal position in the ureter.
Flank pain is often associated with less specific symptoms including fever, nausea and vomiting, and tachycardia. Fever suggests infection proximal to the ureteral obstruction. Flank pain associated with fever requires a prompt diagnosis of ureteral obstruction and relief of the obstruction because infection proximal to the obstruction causes much more rapid renal damage than occurs with obstruction in the absence of infection. Also, the patient is susceptible to septicemia in the presence of infection proximal to a ureteral obstruction.
Gross or microscopic hematuria (blood in urine) helps to confirm a urinary cause of the pain. Hematuria is occasionally absent with acute ureteral obstruction, however, and is often absent with chronic obstruction.
Although ureteral stone is the most common cause of flank pain, many other causes should be considered (see causes of flank pain). Flank pain resulting from acute ureteral obstruction can also be caused by blood clots or sloughed renal papillae passing through the ureter. Blood clots can be produced by many pathologic lesions of the kidney, tumors being the most common cause. Renal papillary necrosis should be considered in patients with a history of analgesic abuse or diabetes mellitus.
Flank pain caused by chronic ureteral obstruction is generally much less severe. Occasionally, congenital anomalies such as ureteropelvic junction obstruction produce flank pain associated with a diuresis after oral intake of a large volume of fluid. Bilateral chronic ureteral obstruction or ureteral obstruction of a solitary kidney can be associated with symptoms of renal failure such as apathy, lethargy, anorexia, muscle twitching, headache, hypertension, and poor growth of a child. A dull or mild flank pain should make the clinician consider many possible causes including congenital ureteral obstruction, ureteral tumor or an extrinsic tumor compressing the ureter, acquired stricture of the ureter due to a previous operation or radiation therapy, retroperitoneal fibrosis, and a ureteral stone.
Flank pain caused by renal inflammation generally is not as sudden in onset or as severe as pain caused by acute ureteral obstruction. Renal inflammation usually produces localized pain and is associated with other manifestations of infection such as fever, leukocytosis, and bacteriuria.
Flank pain can be caused by different types of renal tumors, but pain is not the most common presenting symptom, and when pain is present, it often is associated with other symptoms. Hematuria is the most common symptom seen in tumors presenting in adults; an abdominal mass is the most common presenting symptom of Wilms” tumor in childhood.
Uncommon causes of flank pain include renal trauma, renal infarction, and vesicoureteral reflux even in the absence of infection. Renal infarction should be considered in patients with atrial fibrillation or a recent myocardial infarction. Vesicoureteral reflux occasionally causes mild flank pain due to distention of the ureter and renal pelvis when the reflux occurs while voiding.
A patient should be suspected of being an analgesic abuser when he or she presents with a history of acute severe flank pain, uric acid stones, previous reactions to contrast media, and a residence a great distance away. The physician should not be fooled by hematuria because narcotic addicts find ways to place blood in their urine specimens.
Extraurinary diseases of the abdomen and chest can also cause flank pain. These diseases produce pain less characteristic of the typical “renal colic” seen with acute ureteral obstruction. Nevertheless, this vague, dull, mild flank pain is similar to the pain seen with chronic ureteral obstruction, making the differential diagnosis unclear. The correct diagnosis is made by thinking of all the diseases that have been discussed, considering the associated symptoms, physical examination, urinalysis, and performing carefully selected laboratory tests and radiographic studies.
Flank pain originating in the urinary system is caused by distention of the ureter or renal pelvis or distention of the renal capsule. The severity of the pain is directly related to the rapidity of the distention and not to the degree of distention. Therefore, a patient with acute distention of the ureter will have extremely severe pain. This patient usually has mild dilation of the ureter and no irreversible renal damage. However, a patient with a greatly dilated ureter and irreversible renal damage might have no pain or mild pain because the ureteral dilation has developed over a long period of time.
Distention of the renal capsule causes a milder flank pain. This can be caused by aucte pyelonephritis, ureteral obstruction, or renal subcapsular hematoma.
Kidney and ureteral pain is through visceral afferent fibers that accompany the sympathetic nerves of the lower thoracic and upper lumbar segments.
Flank pain diagnosis
Your doctor will examine you. You will be asked about your medical history and symptoms, including:
- Location of the pain
- When the pain began, if it’s always there or comes and goes, if it’s getting worse
- What the pain feels like, such as dull and aching or sharp
- What other symptoms you have
The following tests may be done:
- Abdominal CT scan
- Blood tests to check kidney and liver function
- Chest x-ray
- Kidney or abdominal ultrasound
- Lumbosacral spine x-ray
- Tests to check the kidneys and bladder, such as urinalysis and urine culture, or cystourethrogram.
- Wang RC, Rodriguez RM, Fahimi J, et al. Derivation of decision rules to predict clinically important outcomes in acute flank pain patients. Am J Emerg Med. 2016;35(4):554-563. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5701802/
- Fwu C-W, Eggers PW, Kimmel PL, Kusek JW, Kirkali Z. Emergency department visits, use of imaging, and drugs for urolithiasis have increased in the United States. Kidney Int. 2013 Apr;83(3):479–86.





{kind=link}