
What is fuchs dystrophy
Fuchs’ dystrophy is a disease of the cornea that causes the cells in the corneal innermost layer called the endothelium to die off. These cells normally pump fluid from the cornea to keep it clear. When the corneal endothelium die, fluid builds up and the cornea gets swollen and puffy. Vision becomes cloudy or hazy. Deposits called guttae, which are detectable during an eye exam, form in the middle of the cornea and eventually spread. These guttae contribute to the loss of cells in the cornea, leading to vision problems. Tiny blisters may develop on the cornea, which can burst and cause eye pain.
Fuchs’ dystrophy usually affects both eyes and can cause your vision to gradually worsen over years. People in their 30s and 40s may have Fuchs’ dystrophy but not know it. But most people with Fuchs’ dystrophy don’t develop symptoms until they reach their 50s or 60s. A very rare early-onset variant of this condition starts to affect vision in a person’s twenties. Women are more likely than men to have Fuchs’ dystrophy.
In patients with Fuchs’ corneal dystrophy, the endothelial cells slowly deteriorate as tiny bumps called guttae accumulate on the Descemet’s membrane. When the endothelial cells develop these guttae, the surrounding cells become damagedand cannot work properly. Since the remaining cells cannot keep up with pumping fluid, the cornea begins swelling (known as corneal edema). As a result, the cornea becomes thicker and cloudy, resulting in vision problems. In advanced cases, tiny blisters can form on the surface of your cornea which can be painful, so it is important to seek treatment prior to severe progression.
The term ‘cornea guttata’, as first used by Vogt to refer to these affected corneas of patients with Fuchs’ corneal dystrophy, has its origins in the ‘tropfige’ (German for drop-like) appearance of the endothelium. The singular term ‘gutta’ (plural, ‘guttae’) is the Latin noun for ‘drop’, with ‘guttata’ being the adjective describing the ‘guttate’ cornea. Vogt referred to individual excrescences as ‘dew drops’ in his report 1, suggesting that use of the noun would be appropriate. Nevertheless, it has been pointed out that adapting terminology in the field of ophthalmology is not a historically new development 2, as ‘cornea’ was initially an adjective (tunica cornea) used over 600 years ago to describe the hardness of this unique coat of the eye in similarity to a horn (cornu).
Some medications and self-care steps may help relieve your Fuchs’ dystrophy signs and symptoms. But when the disorder is advanced and you’ve lost vision, the only way to restore vision is with cornea transplant surgery.
Until recently, the most common type of corneal transplant was penetrating keratoplasty. During this procedure, a small round piece of the cornea is removed, leaving an opening in the front of the eye. A matching piece of cornea from a human donor is then sewn into the opening in the front of the eye.
A newer technique called endothelial keratoplasty (DSEK, DSAEK, or DMEK) has become the preferred option for people with Fuchs’ dystrophy. In this procedure, only the inner layers of the cornea are replaced, instead of all the layers. This leads to a faster recovery and fewer complications. Stitches are most often not needed.
The Cornea
The cornea is made up of five distinct layers:
- The Epithelium – the outermost, protective layer of the cornea.
- The Bowman’s membrane – this second layer is extremely tough and difficult to penetrate further protecting the eye
- The Stroma – the thickest layer of the cornea, consisting of water, collagen fibers and other connective tissue components that give the cornea its strength, elasticity and clarity.
- Descemet’s Layer – a thin, strong inner layer that also acts as a protective layer.
- The Endothelium – the innermost layer consisting of specialized cells that pump excess water out of the cornea
The cornea serves two functions; it protects the rest of the eye from dust, germs and other harmful or irritating material, and it acts as the eye’s outermost lens, bending incoming light onto the inner lens, where the light is then directed to the retina (a membranous layer of light-sensing cells in the back of the eye). The retina converts light to images, which are then transmitted to the brain. The cornea must remain clear (transparent) to be able to focus incoming light.
Figure 1. Cornea
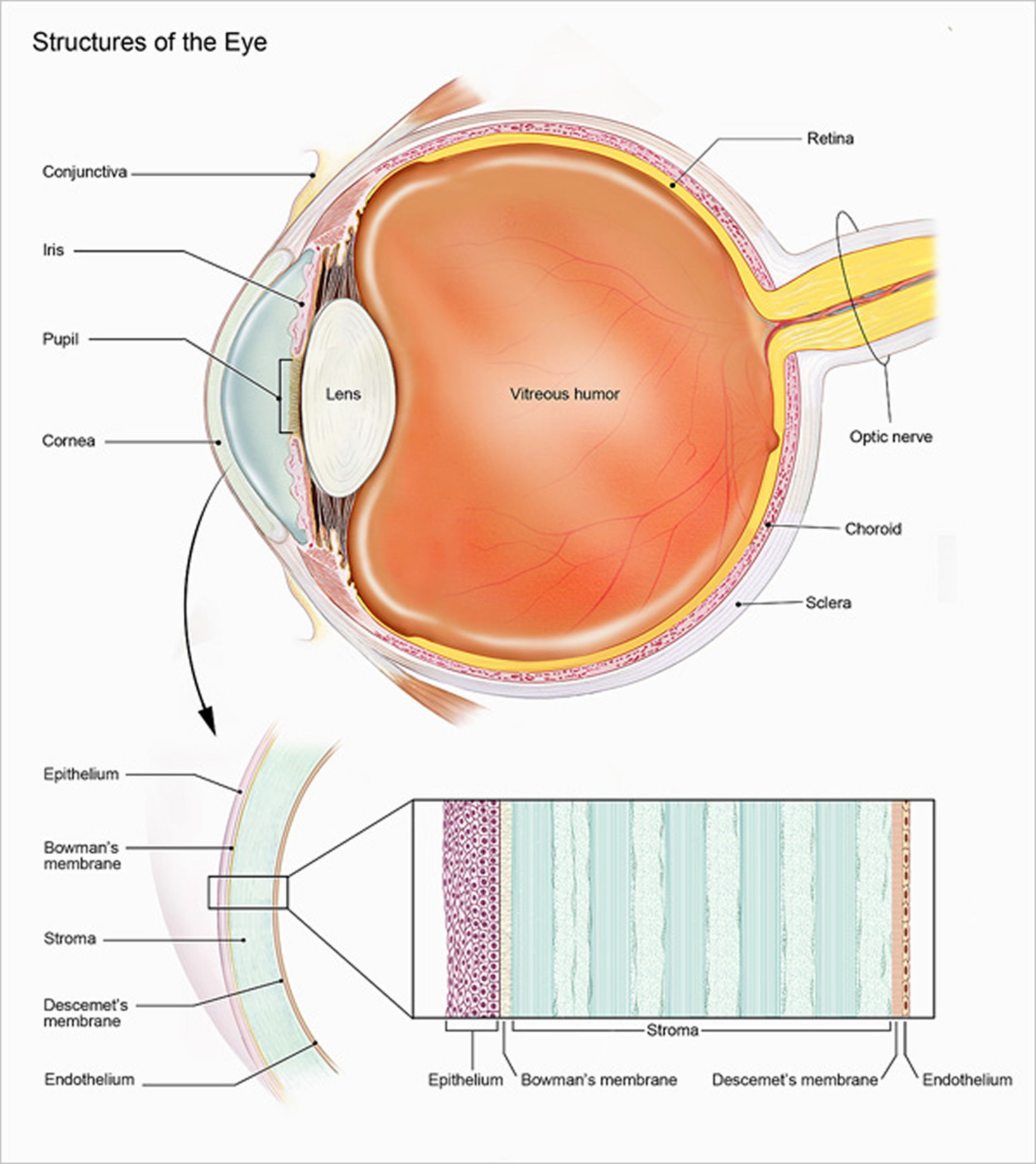
Figure 2. Fuch’s endothelial corneal dystrophy (slit lamp view of corneal guttae or guttata in Fuchs corneal dystrophy)

Fuchs dystrophy stages
Fuchs’ dystrophy has two stages.
- In the early stage (stage 1), you may notice few, if any, problems. Vision is usually hazy in the morning but gets better throughout the day. This is because your eyes normally stay moist when they are closed during sleep. But when you are awake, the fluid dries normally.
- With the later stage 2, vision remains blurry all day. Too much fluid builds up during sleep and not enough dries up during the day. Also, tiny blisters may form in the cornea. The blisters get bigger and eventually break open, causing eye pain.
The late-onset form of Fuchs endothelial dystrophy is a common condition, affecting approximately 4 percent of people over the age of 40. The early-onset variant of Fuchs endothelial dystrophy is rare, although the exact prevalence is unknown.
Vision problems might not appear until age 50 or later. The first symptom of Fuchs’ dystrophy is typically blurred vision in the morning that usually clears during the day. Over time, affected individuals lose the ability to see details (visual acuity). People with Fuchs endothelial dystrophy also become sensitive to bright lights.
Fuchs’ dystrophy prognosis
Fuchs’ dystrophy gets worse over time. Without a corneal transplant, a person with severe Fuchs’ dystrophy may become blind or have severe pain and very reduced vision.
Mild cases of Fuchs’ dystrophy often worsen after cataract surgery. A cataract surgeon will evaluate this risk and may modify the technique or the timing of your cataract surgery.
Fuchs’ dystrophy causes
Normally, the cells lining the inside of the cornea (endothelial cells) help maintain a healthy balance of fluids within the cornea and prevent the cornea from swelling. But with Fuchs’ dystrophy, the endothelial cells gradually die, resulting in fluid buildup (edema) within the cornea. This causes corneal thickening and blurred vision.
The inheritance of Fuchs dystrophy is not straight forward. In some cases, Fuchs dystrophy appears to be inherited in an autosomal dominant pattern, which means one copy of the altered gene in each cell is sufficient to cause the disorder. In autosomal dominant inheritance, if either of your parents has the disease, you have a 50% chance of developing the condition. Or if you have an inherited form of Fuchs’ endothelial dystrophy there is a 50% chance you will pass it on to your children.
When Fuchs dystrophy is caused by a mutation in the COL8A2 gene (which is the early-onset form of Fuchs dystrophy), it is inherited in an autosomal dominant pattern. The genetic basis of the disease is complex — family members can be affected to varying degrees or not at all. In addition, an autosomal dominant inheritance pattern is seen in some situations in which the condition is caused by changes in an unknown gene. However, in many cases, the inheritance pattern is unknown. Spontaneous mutation in the gene for Fuchs’ dystrophy also can cause new Fuchs’ dystrophy in a person with no family history. Due to the complex nature of the inheritance of this condition, doctors strongly recommend you discuss your concerns with a genetics professional.
Currently there are studies underway to try and determine exactly which gene is responsible for the dystrophy, but as of yet scientists still do not know the exact gene. Recent reports suggest that missense mutations in ZEB1 gene may be responsible for at least some cases of late-onset Fuchs endothelial dystrophy. This mutation has also been found in cases of type 3 posterior polymorphous dystrophy suggesting that the two conditions may be allelic.
There are several forms of the disease according to the age of onset of the symptoms and the cause.
The early-onset form is very rare and is known as Fuchs endothelial corneal dystrophy 1 (or early-onset Fuchs endothelial corneal dystrophy) and it is caused by a change (mutation) in the COL8A2 gene.This gene provides instructions for making a protein that is part of type VIII collagen. Type VIII collagen is largely found within the cornea, surrounding the endothelial cells. Specifically, type VIII collagen is a major component of a tissue at the back of the cornea, called Descemet’s membrane. This membrane is a thin, sheet-like structure that separates and supports corneal endothelial cells. COL8A2 gene mutations that cause the early-onset variant of Fuchs endothelial dystrophy lead to an abnormal Descemet’s membrane, which causes the cells to die and leads to the vision problems in people with this condition.
Late-onset Fuchs endothelial corneal dystrophies are common and include:
- Fuchs endothelial corneal dystrophy 2 (caused by a mutation in an unknown gene located in chromosome 13)
- Fuchs endothelial corneal dystrophy 3 (may be caused by TCF4 gene mutations)
- Fuchs endothelial corneal dystrophy 4 (caused by a mutation in the SLC4A11 gene)
- Fuchs endothelial corneal dystrophy 5 (caused by a mutation in an unknown gene located in chromosome 15)
- Fuchs endothelial corneal dystrophy 6 (caused by a mutation in the ZEB1 gene)
- Fuchs endothelial corneal dystrophy 7 (caused by a mutation in an unknown gene located in chromosome 9)
- Fuchs endothelial corneal dystrophy 8 (caused by heterozygous mutation in the AGBL1 gene).
Risk factors for Fuchs’ dystrophy
Factors that increase your risk of developing Fuchs’ dystrophy include:
- Sex. Fuchs’ dystrophy is slightly more common in women than in men.
- Genetics. Having a family history of Fuchs’ dystrophy increases your risk.
- Age. Although there’s a rare early-onset type of Fuch’s dystrophy that begins in childhood, typically the disease starts in the 20s and 30s, with symptoms developing in the 50s and 60s.
Smoking and having diabetes might also put you at higher risk of the disease.
Fuchs dystrophy symptoms
In the early stage (stage 1), you may notice few, if any, symptoms. Your vision may be hazy or blurry when you first wake up in the morning, but improve gradually throughout the day. As the disease progresses, blurred vision either can take longer to improve or doesn’t improve.
In the later stage (stage 2), your blurry or hazy vision will not get better as the day goes on. Here are other symptoms:
- Sandy or gritty feeling in your eyes
- Eye pain from the tiny blisters in the cell layer of the cornea
- Being extra sensitive to bright light
- Eye problems get worse in humid areas
- Very blurry or hazy vision from scarring at the center of the cornea
- Glare, which can decrease your vision in dim and bright light
Other symptoms can include distorted vision, sensitivity to light, difficulty seeing at night and seeing halos around lights.
Fuchs dystrophy diagnosis
Besides testing your vision, your doctor might also have you undergo the following tests to determine whether you have Fuchs’ dystrophy:
- Staging. Your doctor will try to determine the stage of your condition by examining your eye with an optical microscope (slit lamp). He or she will then study the cells lining the back of your cornea (endothelial cells). Irregular bumps (guttae) on the back of the cornea might indicate Fuchs’ dystrophy.
- Corneal pressure test. After numbing your eyes with drops, your doctor will briefly touch your eyes with a special instrument that measures eye pressure. This test can help distinguish between a disease that increases pressure in your eye (glaucoma) and Fuch’s dystrophy.
- Corneal thickness. Your doctor might use a special instrument to measure the thickness of the cornea.
- Corneal cell count. Sometimes your doctor might use another special instrument to record the number, shape and size of the cells that line the back of the cornea.
Fuchs dystrophy treatment
Some nonsurgical treatments and self-care strategies might help relieve the symptoms of Fuchs’ dystrophy. If you have severe disease, your doctor might suggest surgery.
Medications and other therapies:
- Eye medication. Eyedrops or ointments can help reduce the amount of fluid in your cornea. By increasing external osmolality, hypertonic sodium chloride (Muro 128®) drops or ointment can be given to extract water from the cornea. It is typically administered at bedtime and waking.
- Soft contact lenses. These act as a covering to relieve pain.
Fuchs’ dystrophy surgery
People who have surgery for advanced Fuchs’ dystrophy can have much better vision and remain symptom-free for years afterward. Surgical options include 3:
- Replacing the inner layer of the cornea called Descemet’s Stripping Endothelial Keratoplasty (DSEK) or Descemet’s Stripping Automated Endothelial Keratoplasty (DSAEK). In this new keratoplasty procedure, the patient’s diseased endothelium and Descemet’s membrane are replaced with posterior corneal stroma, Descemet’s membrane and endothelium from the donor cornea 4. As a sutureless keratoplasty, Descemet’s stripping endothelial keratoplasty (DSEK )is a more precise treatment and is associated with better overall surgical outcomes than conventional penetrating keratoplasty. The procedure is usually done with local anesthesia in an outpatient setting. Descemet’s stripping endothelial keratoplasty has been rapidly adopted by surgeons worldwide, and it has gradually become the standard surgical treatment for corneal endothelial problems, such as Fuchs corneal dystrophy, pseudophakic bullous keratopathy and iridocorneal endothelial syndrome, because of its short learning curve, good clinical outcomes, easier donor preparation and manipulation, and reproducible results 5. However, the interface opacification, optical irregularities, hyperopic refractive shift and thicker cornea caused by the extra stromal layers transplanted during the Descemet’s stripping endothelial keratoplasty procedure may have a negative impact on postoperative visual quality 6. Therefore, to fully retain the anatomy of the recipient’s cornea, endothelial keratoplasty was used with the introduction by Melles in 2006 of “Descemet’s membrane endothelial keratoplasty” (DMEK), which transplants a lamella of Descemet’s membrane and endothelium without an adherent donor corneal stroma 7. The cornea is the thickness of a credit card, and Descemet’s membrane endothelial keratoplasty (DMEK) replaces less than 1/20th of that thickness. With Descemet’s membrane endothelial keratoplasty (DMEK), only the damaged endothelium of the cornea is replaced. Visual recovery is much faster with Descemet membrane endothelial keratoplasty (DMEK) because the air bubble that holds the tissue in place while it attaches is much less invasive than sutures. In some cases, patients may experience visual acuity as good as 20/20 just a few days after surgery with glasses. Most importantly, the rejection risk is 15 to 20 times lower with DMEK. Such low rejection is unprecedented and essentially eliminates one the main reason that transplants fail. In summary, research has shown that Descemet membrane endothelial keratoplasty (DMEK) is now an excellent treatment option for patients with Fuchs’ dystrophy. Since its introduction, the number of Descemet membrane endothelial keratoplasty (DMEK) cases performed each year in the United States has doubled every year; however, Descemet’s stripping endothelial keratoplasty (DSEK) is still the dominant surgical treatment of choice for endothelial diseases 8.
- In this comprehensive, systematic review 9 of all available and eligible studies, the results showed that Descemet’s membrane endothelial keratoplasty (DMEK) provides better visual rehabilitation than Descemet’s stripping endothelial keratoplasty (DSEK), even when Descemet’s membrane endothelial keratoplasty (DMEK) was performed by a surgeon during the learning curve phase. The extra stroma in Descemet’s stripping endothelial keratoplasty (DSEK) grafts and the rough recipient-donor interface increase the posterior irregular astigmatism and uncorrectable corneal high-order aberrations, which limit the visual outcomes 10. In contrast, Descemet’s membrane endothelial keratoplasty (DMEK) uses an extremely thin graft that consists of only Descemet’s membrane and endothelium without adherent donor stroma 11. This promising new procedure leads to better restorations of the corneal integrity, eliminates recipient-donor interface mismatches, and allows for better visual outcomes; thus, it has become popular among corneal surgeons and patients who suffer from corneal endothelial diseases 12.
- Transplanting the cornea. This surgical procedure, known as full thickness corneal transplant or penetrating keratoplasty (PKP), replaces the full-thickness cornea with a healthy one from a donor. Although not used much anymore for Fuchs’ dystrophy, it might be the best choice in some cases.
Fuchs’ dystrophy surgery complications
Surgical complications include infection, poor wound healing, transplant rejection, and suture related complications can be seen in transplant patients. With a full thickness transplant high refractive error and astigmatism can be seen can also be a problem. Long term use of topical steroids, necessary to prevent rejection, can induce cataract and glaucoma. Unique to Descemet’s stripping endothelial keratoplasty (DSEK) includes early onset detachment of the endothelial cells, which may require a repeat air bubble placement, or rarely replacement of endothelial transplant.
Possible future treatments
New ways of treating Fuchs’ dystrophy are being tested. Ask your doctor if you’re eligible for clinical trials.
Surgical follow up
Follow up is essential after any form of corneal transplantation. Most patients will need to be seen often in the first few weeks after the surgery to ensure surgical success and prevent infection. Routine follow up visits are essential for evaluation of transplant health, wound healing, and visual recovery including removal of sutures minimizing astigmatism. Both full thickness corneal transplant or penetrating keratoplasty (PKP) and partial thickness (DSEK) transplants have the potential for rejection, just as with any organ transplant. Rejection of the corneal transplant has been seen years after the initial surgery. Follow up is essential in order to prevent and treat rejection if seen.
Home remedies
In addition to following your doctor’s instructions for care, you can try these techniques to help reduce glare or soothe your eyes.
- Apply over-the-counter (nonprescription) salt solution (5 percent sodium chloride) eyedrops or ointment.
- Wear wraparound sunglasses with ultraviolet protection.
- Dry your eyes with a hair dryer. Hold it at arm’s length and direct warm — not hot — air across your face two or three times a day. This helps remove excess fluid in the cornea, which decreases swelling.
- Vogt A. Weitere Ergebnisse der Spaltlampenmikroskopie des vordern Bulbusabschnittes. Arch Ophthalmol. 1921:63–113.[↩]
- Lietman T, Lee J, Costanza S. Those excrescences on Descemet’s membrane. Br J Ophthalmol. 2003;87:515–516. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1771580/[↩]
- Posterior lamellar keratoplasty: DLEK to DSEK to DMEK. Melles GR. Cornea. 2006 Sep; 25(8):879-81. https://www.ncbi.nlm.nih.gov/pubmed/17102659/[↩]
- Price FW, Price MO. DSEK: What you need to know about endothelial keratoplasty: SLACK Incorporated; 2009.[↩]
- Endothelial keratoplasty: why aren’t we all doing Descemet membrane endothelial keratoplasty? Terry MA. Cornea. 2012 May; 31(5):469-71. https://www.ncbi.nlm.nih.gov/pubmed/22367047/[↩]
- Uchino Y, Shimmura S, Yamaguchi T, Kawakita T, Matsumoto Y, Negishi K, et al. Comparison of corneal thickness and haze in DSAEK and penetrating keratoplasty. Cornea. 2011;30(3):287–90. doi: 10.1097/ICO.0b013e3181eeafd6 https://www.ncbi.nlm.nih.gov/pubmed/21045661[↩]
- Melles GR, San Ong T, Ververs B, van der Wees J. Descemet membrane endothelial keratoplasty (DMEK). Cornea. 2006;25(8):987–90. doi: 10.1097/01.ico.0000248385.16896.34 https://www.ncbi.nlm.nih.gov/pubmed/17102683[↩]
- Lee JK, Gore PK, Lim CY, Chuck RS. Keratoplasty in the United States: A 10-year review from 2005 through 2014 Park C.Y United States: Elsevier Inc.; 2015 [cited 122 (Park, Lee, Chuck) Department of Ophthalmology and Visual Sciences, Montefiore Medical Center, Albert Einstein College of Medicine, 111 East 210th Street, Bronx, NY 10467, United States]. 12:[2432–42].[↩]
- Li S, Liu L, Wang W, et al. Efficacy and safety of Descemet’s membrane endothelial keratoplasty versus Descemet’s stripping endothelial keratoplasty: A systematic review and meta-analysis. Li W, ed. PLoS ONE. 2017;12(12):e0182275. doi:10.1371/journal.pone.0182275. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5734733/[↩]
- Rudolph M, Laaser K, Bachmann BO, Cursiefen C, Epstein D, Kruse FE. Corneal higher-order aberrations after Descemet’s membrane endothelial keratoplasty. Ophthalmology. 2012;119(3):528–35. Epub 2011/12/27. doi: 10.1016/j.ophtha.2011.08.034 https://www.ncbi.nlm.nih.gov/pubmed/22197439[↩]
- Melles GR. Posterior lamellar keratoplasty: DLEK to DSEK to DMEK. Cornea. 2006;25(8):879–81. doi: 10.1097/01.ico.0000243962.60392.4f https://www.ncbi.nlm.nih.gov/pubmed/17102659[↩]
- Tourtas T, Laaser K, Bachmann BO, Cursiefen C, Kruse FE. Descemet membrane endothelial keratoplasty versus descemet stripping automated endothelial keratoplasty. American journal of ophthalmology. 2012;153(6):1082–90.e2. Epub 2012/03/09. doi: 10.1016/j.ajo.2011.12.012 https://www.ncbi.nlm.nih.gov/pubmed/22397955[↩]





{kind=link}