
What is a gluten allergy
Gluten is a mix of protein (glutenins and gliadins) found in wheat, rye, and barley. Oats are constitutionally gluten free but can be cross-contaminated with wheat during processing 1. The current tests for ‘gluten’ in food can measure the gluten in wheat (gliadin), barley (hordein), and rye (secalin). Gluten is found mainly in foods but may also be in other products like medicines, vitamins, and supplements. Gluten can cause two distinct immunological diseases: Celiac disease and IgE-mediated gluten allergy (also called wheat allergy) [see Figure 1 below]. In gluten allergy (wheat allergy) it is the cross-linking of immunoglobulin IgE by repeat sequences in gluten peptides (for example, serine-glutamine-glutamine -glutamine-(glutamine-)proline-proline-phenylalanine) that triggers the release of chemical mediators, such as histamine, from basophils and mast cells 2. In contrast, Celiac disease is an autoimmune disorder (your immune system attacks healthy cells in your body by mistake), as demonstrated by specific serologic autoantibodies, most notably serum anti-tissue transglutaminase antibodies immunoglobulin A (tTG-IgA) and anti-endomysial antibody immunoglobulin A (EMA-IgA) 3. There are few cases of gluten allergy reported and little is known about its natural history 4.
Besides wheat, foods that contain gluten include:
- Barley
- Bulgur
- Durum
- Farina
- Graham flour
- Malt
- Rye
- Semolina
- Spelt (a form of wheat)
- Triticale
Gluten can be hidden in foods, medications and nonfood products, including:
- Modified food starch, preservatives and food stabilizers
- Prescription and over-the-counter medications
- Vitamin and mineral supplements
- Herbal and nutritional supplements
- Lipstick products
- Toothpaste and mouthwash
- Communion wafers
- Envelope and stamp glue
- Play dough
Figure 1. Gluten related disorders classification (proposed new nomenclature and classification)
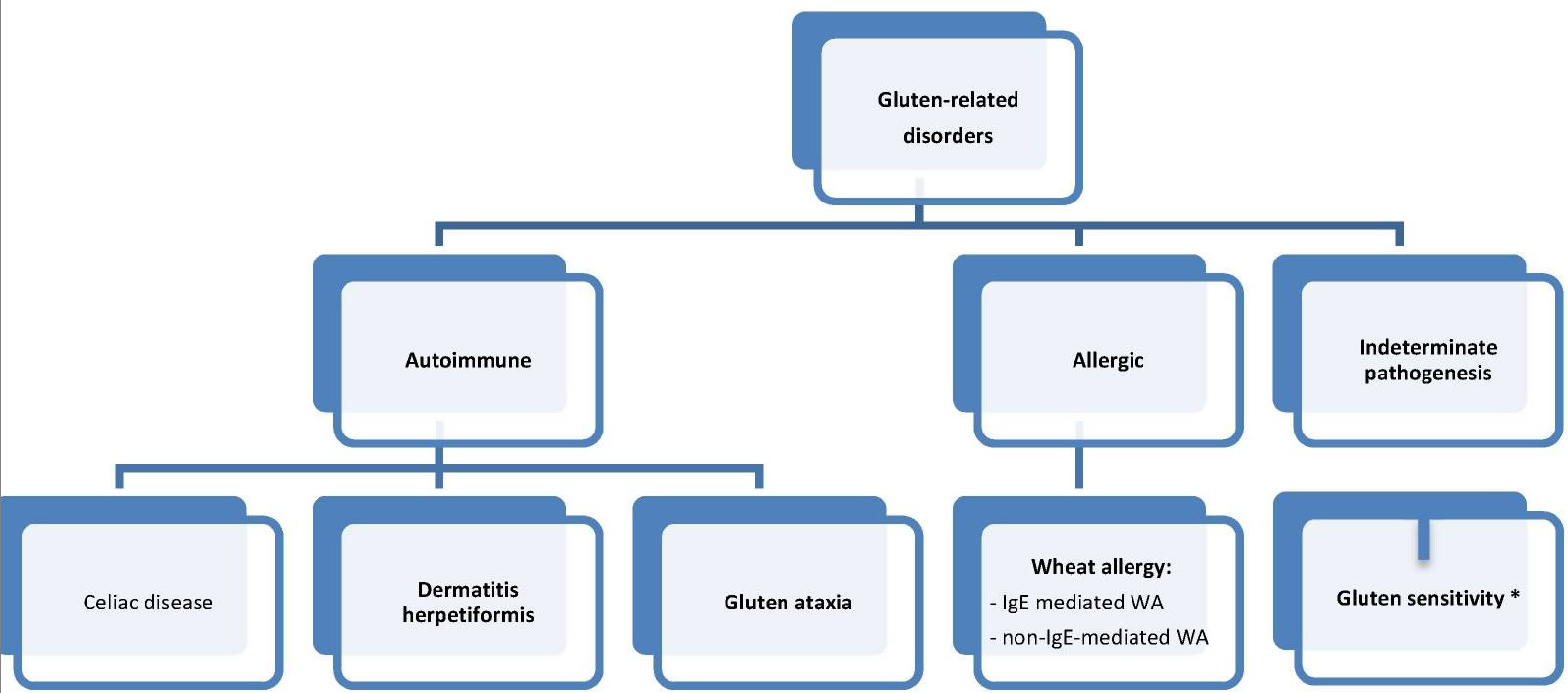
Footnote: Gluten sensitivity (GS) = non-celiac gluten sensitivity (NCGS).
[Source 3]Gluten allergy (wheat allergy) is defined as an adverse immunologic reaction to wheat proteins 3. Depending on the routes of entry, wheat-related allergic disorders are classified into: food allergy affecting the skin, gastrointestinal tract or respiratory tract; wheat-dependent, exercise-induced anaphylaxis; occupational asthma (baker’s asthma) and rhinitis; and contact urticaria (Figure 2) 5. IgE antibodies play a central role in the pathogenesis of these diseases 3.
The allergy classifications also consider Celiac disease as a wheat-related allergic disorder. However, Celiac disease is, rather, an autoimmune disease and in most countries it is treated according to gastroenterological protocols. Food allergies triggered by wheat consumption are divided to IgE-dependent wheat allergy and IgE-non-dependent wheat allergy 5. One of the wheat allergy syndromes is also wheat-dependent exercise-induced anaphylaxis. In the latest European Academy of Allergy and Clinical Immunology classification it has been recognized as an independent form of wheat allergy 5.
Gluten allergy (wheat allergy) is also one of the gluten-related disorders, the classification of which was published in 2012 (see Figure 1 above) 3. It is important to note that although wheat allergy belongs to this group, all of its forms stem solely from the adverse effect of wheat proteins (including gluten proteins). Therefore, the treatment is based on the elimination of wheat grains only. The allergy induced by proteins contained in other gluten grains is less common and has not been included in the classification discussed herein.
Figure 2. Classification of gluten/wheat-related allergic diseases
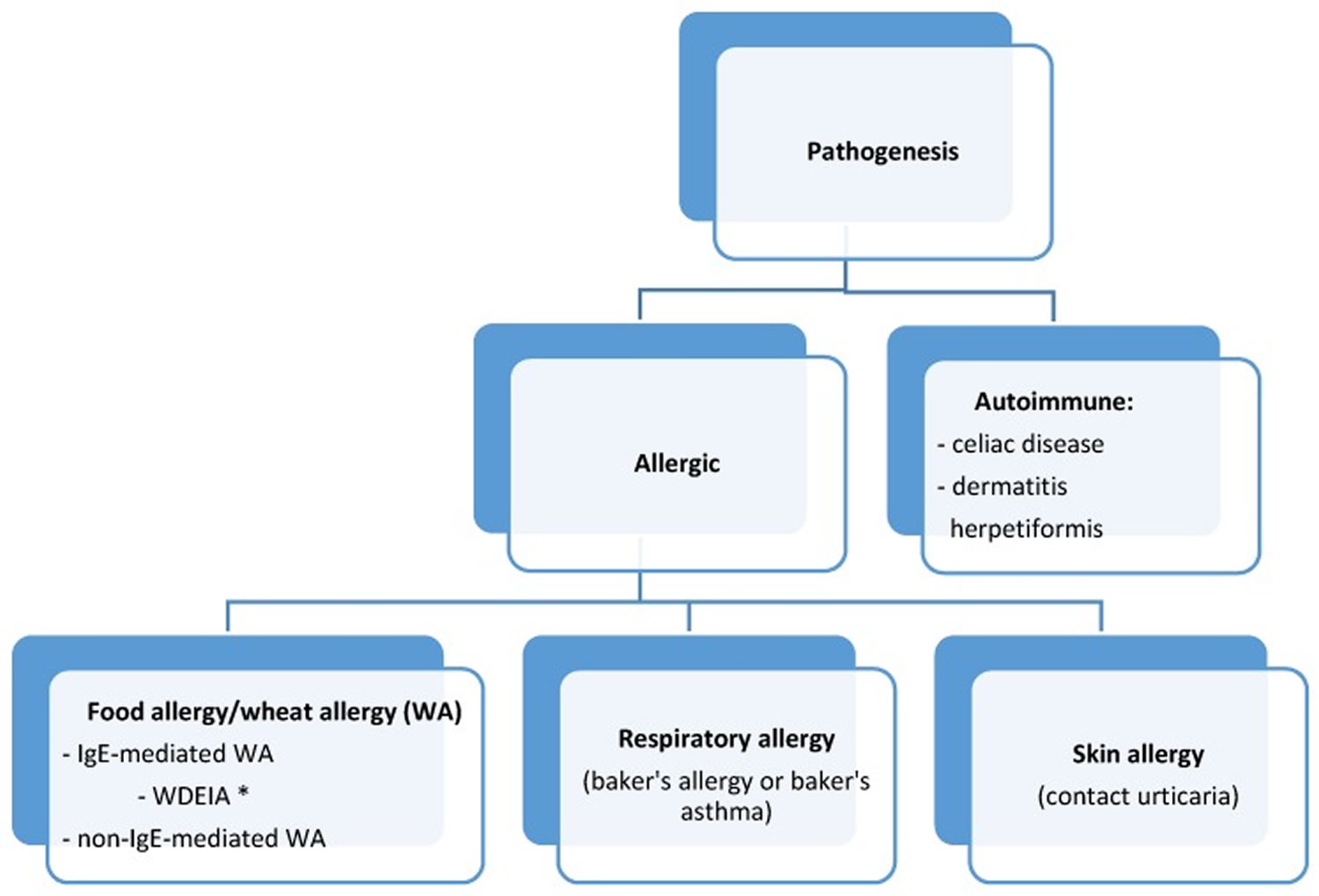
Footnote: WDEIA = wheat-dependent exercise-induced anaphylaxis
[Source 6]Prevalence of IgE-Mediated Gluten (Wheat) Allergy
Wheat is one of the five most common foods that trigger allergic reactions in children. In Germany, Japan, and Finland it has been reported as the third most common allergen, after milk and egg 7. Wheat allergy prevalence, both in children and adults, is usually approximately 1% (0.4%–4%), depending on age and region 7, 8, 9, 10. In people with food allergies, wheat allergy is diagnosed in 11%–20% of children and in 25% of adults 11. Taking into account all gluten-related disorders, it has been estimated that about 3% of the human population suffers from wheat intolerance (1% WA, 1% celiac disease, 1% non-celiac gluten sensitivity) 12.
Figure 3. Gluten allergy rash

What is Celiac disease?
Celiac disease also called celiac sprue or gluten-sensitive enteropathy, is a disorder in which the body’s immune system attacks the lining of the small intestine after a person consumes gluten, a protein found in wheat, barley and rye. Individuals with Celiac disease experience an immune reaction when eating gluten containing products such as wheat, barley, rye and sometimes oats. Oats are constitutionally gluten free but can be cross-contaminated with wheat during processing. Gluten can also be found in medicines, vitamins and lip balms. Untreated celiac disease leads to inflammation that damages the small intestine, which prevents a person from properly absorbing nutrients that the body needs.
Celiac disease is called an autoimmune disorder because a person’s own immune system causes harm to the body. Celiac disease is triggered by the consumption of gluten in genetically susceptible individuals, who are exposed to as-yet-unidentified environmental triggers. Celiac disease has a worldwide distribution that affects ∼1% of the world’s population 13 and has a prevalence of 0.7% in the United States 14.
If you have celiac disease, eating gluten triggers an immune reaction in your small intestine by damaging the villi (tiny, finger-like projections which line the small intestine) and causing abdominal pain, bloating or diarrhea. Over time, this immune reaction damages your small intestine’s lining (villous atrophy) which reduces the surface area of the small intestine available for nutrient absorption and prevents it from absorbing some nutrients from food (malabsorption) and as the condition progresses, malnourishment occurs. The intestinal damage often causes diarrhea, fatigue, weight loss, bloating and anemia, and can lead to serious complications. Left untreated, celiac disease may lead to non-intestinal symptoms including anemia, chronic fatigue, osteoporosis, impaired spleen, infertility, neurologic disorders, skin rashes and cancer.
In children, malabsorption can affect growth and development, besides causing the symptoms seen in adults.
Celiac disease can only develop in those with certain genes called HLA-DQ2 or HLA-DQ8. Either one or both of these genes are present in the majority of people with celiac disease. Thirty percent of the population carries these genes. If you do not have these genes, HLA-DQ2 or HLA-DQ8, celiac disease cannot develop, but only a small percentage of those with the genes (approximately 1 in 40 of these people) develop celiac disease.
A first degree relative (parent, sibling, child) of someone with celiac disease has about a 10% chance of also having Celiac disease. If one identical twin has Celiac disease there is an approximate 70% chance that the other twin will also have celiac disease (but may not necessarily be diagnosed at the same time). Environmental factors play an important role in triggering celiac disease in infancy, childhood or later in life.
Diagnosing Celiac disease involves the measurement of several blood tests and may also require a small intestine biopsy through an endoscopy procedure.
- Serology testing looks for antibodies in your blood. Elevated levels of certain antibody proteins indicate an immune reaction to gluten.
- Genetic testing for human leukocyte antigens (HLA-DQ2 and HLA-DQ8) can be used to rule out celiac disease.
- Endoscopy. This test uses a long tube with a tiny camera that’s put into your mouth and passed down your throat (upper endoscopy). The camera enables your doctor to view your small intestine and take a small tissue sample (biopsy) to analyze for damage to the villi.
It’s important to be tested for celiac disease before trying a gluten-free diet. Eliminating gluten from your diet might make the results of blood tests appear normal.
There’s no cure for celiac disease, because people with celiac disease remain sensitive to gluten throughout their life. For most people, following a strict lifelong gluten-free diet can help manage symptoms and promote intestinal healing. By removing the cause of celiac disease, a gluten free diet allows the small bowel lining to heal and symptoms to resolve. As long as the gluten free diet is strictly adhered to, problems arising from celiac disease should not return. Relapse occurs if gluten is reintroduced into the diet.
What is non-celiac gluten sensitivity?
Nonceliac gluten sensitivity is a syndrome characterized by symptoms disappearing after a gluten-free diet after a diagnosis of celiac disease or wheat allergy (gluten allergy) has been excluded 15. Non-celiac gluten sensitivity is mainly a “diagnosis of exclusion” made after other wheat-related and non-wheat-related disorders have been ruled out. Patients who do not have celiac disease or wheat allergy but who experience intestinal and extraintestinal symptoms related to the ingestion of gluten-containing foods are said to have ‘nonceliac gluten sensitivity’ 16.
Non-celiac gluten sensitivity is a heterogeneous disorder induced by gluten ingestion in which neither allergic nor autoimmune mechanisms seem to be involved 17. The clinical spectrum of non-celiac gluten sensitivity has been reported to range from upper/lower gastrointestinal symptoms to extraintestinal symptoms, including headache, malaise, asthenia, and muscle cramps 18.
Like Celiac disease, the clinical picture of non-celiac gluten sensitivity is variable and diverse and includes intestinal symptoms such as diarrhea, constipation, bloating, and abdominal pain as well as extraintestinal symptoms including anxiety, fatigue, fibromyalgia, foggy mind, and headache 19. However, unlike celiac disease, there are no known serologic markers for nonceliac gluten sensitivity and there is no agreed-upon diagnostic approach. Patients with non-celiac gluten sensitivity do not have duodenal villous atrophy, the histologic hallmark of celiac disease. Although susceptibility to celiac disease is dependent on the human leukocyte antigens (HLAs) DQ2 and DQ8, there is no established genetic marker identified for non celiac gluten sensitivity 15. Although gluten has been shown to induce an adaptive immune response in patients with celiac disease, intestinal tissue of patients with non-celiac gluten sensitivity has been suggested to show reduced numbers of T-regulatory cells, which may indicate that the innate immune system is involved in patients who develop non celiac gluten sensitivity 20. Wheat amylase trypsin inhibitors (ATIs), rather than gluten, have been proposed as major stimulators of these innate immune cells 21.
According to the international expert panel at the Salerno conference on non-celiac gluten sensitivity 16, before an investigation for alternative diagnoses there must first be a proper evaluation for the presence of celiac disease or wheat allergy with the use of serologic markers. Serologic markers for celiac disease will normalize once a gluten free diet is started, with normalization typically preceding recovery of duodenal histology 13. Therefore, some patients who appear to have non-celiac gluten sensitivity may actually have celiac disease that remains undetected because testing was performed after the gluten free diet was already started. A current survey in 147 patients believed to have non-celiac gluten sensitivity found that 62% had inadequate exclusion of celiac disease 22. Of the 75 patients who underwent esophagogastroduodenoscopy with biopsy, only 29% had adequate gluten intake at the time of duodenal biopsy to exclude celiac disease. In 15% of the patients surveyed, no serologic, HLA, or endoscopic testing had been conducted. This study highlights the fact that patients who present with apparent non-celiac gluten sensitivity often have not had an adequate investigation for celiac disease or alternative diagnoses. In addition to undiagnosed celiac disease or wheat allergy, other possible causes of symptoms in patients with suspected non-celiac gluten sensitivity may be innate immunity to amylase trypsin inhibitors (ATIs) 21 or fermentable, poorly absorbed, short-chain carbohydrates (fermentable, oligo-, di-, monosaccharides, and polyols [FODMAPs]) 23 rather than gluten itself. As per the Salerno experts’ 2-step diagnostic protocol, patients with suspected non-celiac gluten sensitivity following a gluten-containing diet in whom celiac disease and wheat allergy have been excluded should first be assessed for clinical responsiveness with a gluten free diet followed by a gluten challenge to measure the effects of the reintroduction of gluten to the diet 16. The gluten that is reintroduced to the diet should have a defined amylase trypsin inhibitor content and be free of FODMAPs (fermentable, oligo-, di-, monosaccharides, and polyols). If the gluten challenge is negative, patients should then be evaluated for other possible diagnoses, such as small intestinal bacterial overgrowth (SIBO), fructose or lactose intolerance, microscopic colitis, gastroparesis, FODMAP intolerance or other food intolerances 15.
For patients with celiac disease, the gluten free diet is a lifelong prescription with both economic and social consequences 13. In contrast, the duration and degree of gluten avoidance necessary for patients with non-celiac gluten sensitivity have not been established 15.
Table 1. Comparison of celiac disease and non celiac gluten sensitivity
| Celiac disease | Nonceliac Gluten Sensitivity | |
|---|---|---|
| Prevalence | 1% | Unknown |
| Symptoms | Variable, diverse | Variable, diverse |
| Genetic markers | HLA-DQ2 or HLA-DQ8 | None known |
| Serologic markers | anti-tissue transglutaminase antibodies immunoglobulin A (tTG-IgA), gliadin antibodies, deamidated gliadin, anti-endomysial antibody immunoglobulin A (EMA-IgA) | None (gliadin antibodies). Anti gliadin IgG positive in 50% of cases |
| Duodenal histology | Villous atrophy | Normal |
| Malignancy risk | Yes | None known |
| Osteoporosis risk | Yes | None known |
| Diagnostic approach | Established | Not established |
| Duration | Lifelong | Unknown |
What is wheat allergy?
Wheat allergy is an allergic reaction to foods containing wheat. Allergic reactions can be caused by eating wheat and also, in some cases, by inhaling wheat flour. Wheat allergy is classified into occupational asthma (baker’s asthma) and rhinitis; food allergy affecting the skin, the gastrointestinal tract or the respiratory tract; wheat-dependent exercise-induced anaphylaxis (WDEIA) and contact urticaria 24. Ingested wheat can cause IgE-mediated wheat allergies in both children and adults 25.
Immediate wheat allergy is mainly seen in children who commonly outgrow it by school-age, the same as with egg or milk allergy 26. The majority of wheat allergic children suffer from moderate-to-severe atopic dermatitis and wheat ingestion may elicit typical IgE mediated reactions, including urticaria, angioedema, bronchial obstruction, nausea and abdominal pain, or in severe cases systemic anaphylaxis 27. In adults food allergy to ingested wheat is infrequent: the most common variant in adults is the wheat-dependent exercise-induced anaphylaxis (WDEIA), where symptoms result from the combination of causative food intake and physical exercise (as well as non-steroidal anti-inflammatory drugs or alcohol). In adults, food allergy gastrointestinal symptoms could be mild and difficult to recognize, the most common are diarrhea and bloating.
Wheat allergy sometimes is confused with celiac disease, but these conditions differ. Wheat allergy occurs when your body produces antibodies to proteins found in wheat. You can develop an allergy to any of the four classes of wheat proteins — albumin, globulin, gliadin and gluten. The latest updated version of the International Union of Immunological Societies Allergen Nomenclature Database describes 21 different well-classified wheat allergens 28, 29. Some allergens seem mainly associated with respiratory symptoms [alpha-amylase/trypsin inhibitor), food allergy (non-specific lipid transfer protein (nsLTP), gliadins], wheat-dependent exercise-induced anaphylaxis (omega-5 gliadin), or contact urticaria (HMW glutenins) 30.
Celiac disease is an autoimmune disorder triggered by exposure to gluten. Celiac disease is not considered to be a food allergy. People with celiac disease have an autoimmune response to gluten that damages the small intestine. This does not occur in people with gluten sensitivity.
The diagnosis of wheat allergy is classically based on skin prick tests, blood test for specific Immunoglobulin E (sIgE) and the food challenge testing.
- Skin prick test. Tiny drops of purified allergen extracts — including extracts for wheat proteins — are pricked onto your skin’s surface, either on your forearm or on your upper back. After 15 minutes, your doctor or nurse looks for signs of allergic reactions. If you develop a red, itchy bump where the wheat protein extract was pricked onto your skin, you may be allergic to wheat. The most common side effect of these skin tests is itching and redness.
- Blood test. If a skin condition or possible interactions with certain medications prevent you from having a skin test, your doctor may order a blood test that screens for specific allergy-causing antibodies to common allergens, including wheat proteins.
- Food challenge testing. You eat food suspected of being the allergy-causing agent while being monitored for allergy symptoms. Under supervision, you begin with a small amount of the food and gradually increase the amount you consume.
- Food diary. Your doctor may ask you to keep a detailed record of what and when you eat and when symptoms develop for a time.
- Elimination diet. Your doctor may recommend that you remove certain foods from your diet, particularly those that are common allergens. Under your doctor’s direction, you will gradually add foods back and note when symptoms return.
Avoiding wheat is the primary treatment for wheat allergy, but that isn’t always as easy as it sounds. Wheat is found in many foods, including some you might not suspect, such as soy sauce, ice cream and hot dogs. Because wheat proteins appear in so many prepared foods, read product labels carefully. If you have wheat allergy, it’s possible you might also be allergic to barley, oats and rye.
Some sources of wheat proteins are obvious, such as bread, but all wheat proteins — and gluten in particular — can be found in many prepared foods and even in some cosmetics, bath products and play dough. Foods that may include wheat proteins include:
- Breads and bread crumbs
- Cakes, muffins and cookies
- Breakfast cereals
- Pasta
- Couscous
- Farina
- Semolina
- Spelt
- Crackers
- Hydrolyzed vegetable protein
- Soy sauce
- Meat products, such as hot dogs
- Dairy products, such as ice cream
- Natural flavorings
- Gelatinized starch
- Modified food starch
- Vegetable gum
Unless you’re allergic to grains other than wheat, the recommended wheat-free diet is less restrictive than a gluten-free diet.
Medications may be necessary to manage allergic reactions if you accidentally eat wheat.
- Antihistamines may reduce signs and symptoms of minor wheat allergy. These drugs can be taken after exposure to wheat to control your reaction and help relieve discomfort. Ask your doctor if a prescription or an over-the-counter allergy drug is appropriate for you.
- Epinephrine is an emergency treatment for anaphylaxis. If you’re at risk of having a severe reaction to wheat, you may need to carry two injectable doses of epinephrine (EpiPen, Adrenaclick, others) with you at all times. A second pen is recommended for people at high risk of life-threatening anaphylaxis in case anaphylactic symptoms return before emergency care is available.
Scientists are working on several types of immunotherapy to treat food allergies. Immunotherapy exposes you to small amounts of the allergic substance and then increases that exposure over time. The hope is that your body will become desensitized to the allergen, and you’ll have fewer or no symptoms. Several small clinical trials have been done on an oral form of immunotherapy for wheat allergy that showed reduced allergy symptoms. More research is needed, however.
Gluten allergy signs and symptoms
Wheat allergy prevails chiefly in children with a family history of atopy. Almost all of the juvenile wheat allergy patients are diagnosed with allergies to other foods and other allergic disorders, most commonly atopic dermatitis (78%–87%). Half of people suffer from asthma (48%–67%) and/or allergic rhinitis (34%–62%) 31. The majority of children are allergic to cow’s milk (80%), chicken egg white (56%–72%), fish (28%), soya (24%–50%), and peanuts (29%–50%) 31.
The wheat allergy clinical picture depends on age 31. Symptoms develop within minutes to 1–2 h after the ingestion of wheat. In young children gastroenterological symptoms prevail, such as vomiting, diarrhea or rarely, abdomen pains. In about 40% of children skin symptoms are observed in a form of urticaria, erythema, angioedema, pruritus, or worsening atopic dermatitis 32. Intestinal symptoms recede with age; therefore, older children suffer mostly from dermatitis, which is accompanied by respiratory disorders (wheeze, stridor, persistent cough, hoarse voice, respiratory distress, nasal congestion) and, in the most severe cases, anaphylaxis. In teenagers and adults the most severe forms of allergy prevail, such as anaphylaxis symptoms (in 45%–50%), which is typical of wheat allergy. Intestinal and skin symptoms are less common in these age groups 31.
Wheat allergy is usually diagnosed in young children, but it is rarely seen in infants, despite the fact that wheat proteins pass into breast milk, which wheat allergys proven by Linn et al. in 1996 33. In another study on 50 children with wheat allergy, the disease was diagnosed in 32% of infants 6. Three of them were fed exclusively on their mother’s milk 31. In 1981, Rudd et al. 34 described a case of an infant with anaphylactic shock after consuming semolina pudding.
Wheat allergy can be accompanied by allergies to other cereals, most often to rye and/or corn 35.
A child or adult with wheat allergy is likely to develop symptoms within minutes to hours after eating something containing wheat. Wheat allergy symptoms include:
- Swelling, itching or irritation of the mouth or throat
- Hives, itchy rash or swelling of the skin
- Nasal congestion
- Headache
- Itchy, watery eyes
- Difficulty breathing
- Cramps, nausea or vomiting
- Diarrhea
- Anaphylaxis
Most young children with wheat allergy outgrow it by ages 3 to 5.
Anaphylaxis
Anaphylaxis is the most severe type of allergic reaction. It can happen after exposure to certain triggers, such as food, bites and stings. Anaphylaxis can be fatal so should always be treated as a medical emergency with adrenaline (epinephrine).
Symptoms of severe allergy (anaphylaxis) may include:
- trouble breathing or noisy breathing
- difficulty talking more than a few words and/or hoarse voice
- wheeze
- cough
- swelling and tightness of the throat
- collapse
- light-headedness or dizziness
- diarrhea
- tingling in the hands, feet, lips or scalp
- swelling of tongue
- pale and floppy (in young children)
Sometimes, other less dangerous symptoms come before anaphylaxis:
- swelling of face, lips and/or eyes
- hives or welts
- abdominal pain or vomiting
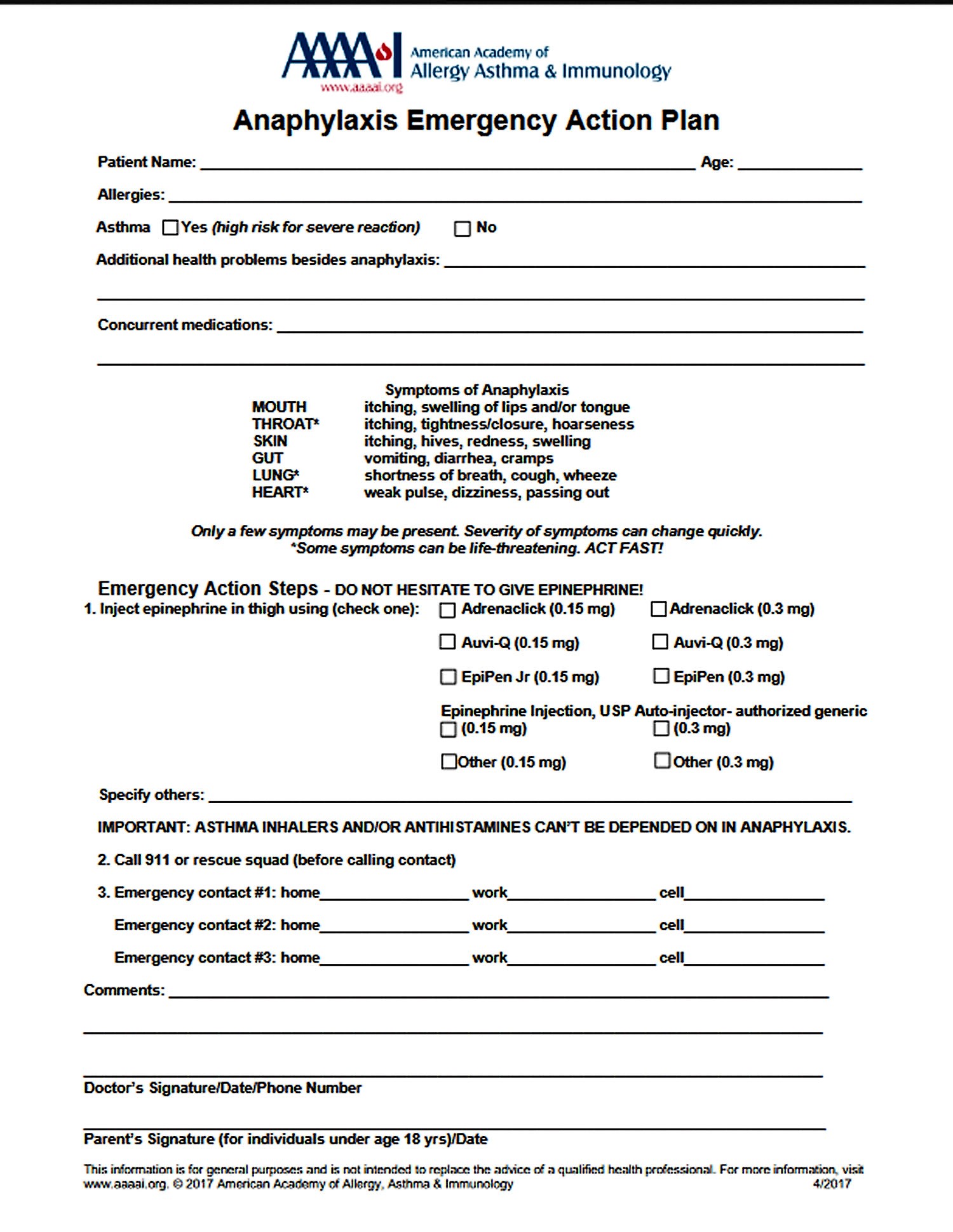
A severe allergic reaction (anaphylaxis) is a medical emergency. Call your local emergency immediately. Lay the person down. If they have an adrenaline injector and you are able to administer it, do so.
Figure 4. Anaphylaxis Emergency Action Plan
Causes of wheat allergy
If you have wheat allergy, exposure to a wheat protein primes your immune system for an allergic reaction. You can develop an allergy to any of the four classes of wheat proteins — albumin, globulin, gliadin and gluten.
Wheat Grain Proteins
All of the wheat-induced diseases are caused by wheat proteins which constitute 10%–18% of the grain mass, depending on the strain. The main component (70%) of the wheat grain is starch.
Depending on their dissolving agent, the wheat grain proteins are categorized into four main fractions: albumins (15%), globulins (7%), gliadins (33%), and glutenins (45%). Albumins are soluble in water; globulins, in salt solutions; gliadins, in alcohol; and while glutenins, in dilute acid and alkali. Albumins and globulins are structural proteins that contain many enzymes. Gliadins and glutenins are prolamins and are referred to as gluten. They are storage proteins.
The wheat proteins that are regarded today as the WA major allergens will be discussed in detail in the next chapter. Wheat proteins triggering CD symptoms belong to gliadins. Wheat proteins responsible for non-celiac-gluten sensitivity have not been identified yet. One of the proteins under the researchers’ examination is a group of amylase-trypsin inhibitors that do not belong to glutens 36.
Sources of wheat proteins
Some sources of wheat proteins are obvious, such as bread, but all wheat proteins — and gluten in particular — can be found in many prepared foods and even in some cosmetics, bath products and play dough. Foods that may include wheat proteins include:
- Breads and bread crumbs
- Cakes and muffins
- Cookies
- Breakfast cereals
- Pasta
- Couscous
- Farina
- Semolina
- Spelt
- Crackers
- Beer
- Hydrolyzed vegetable protein
- Soy sauce
- Some condiments, such as ketchup
- Meat products, such as hot dogs or cold cuts
- Dairy products, such as ice cream
- Natural flavorings
- Gelatinized starch
- Modified food starch
- Vegetable gum
- Licorice
- Jelly beans
- Hard candies
If you have a wheat allergy, you might also be allergic to barley, oats and rye — but the chance is slim. If you’re not allergic to grains other than wheat, a wheat-free diet is less restrictive than a gluten-free diet.
Wheat-dependent, exercise-induced anaphylaxis
Some people with a wheat allergy develop symptoms only if they exercise within a few hours after eating wheat. Exercise-induced changes in your body either trigger an allergic reaction or worsen an immune system response to a wheat protein. This condition usually results in life-threatening anaphylaxis.
Risk factors for wheat allergy
Certain factors may put you at greater risk of developing a wheat allergy:
- Family history. You’re at increased risk of allergy to wheat or other foods if your parents have food allergies or other allergies, such as hay fever.
- Age. Wheat allergy is most common in babies and toddlers, who have immature immune and digestive systems. Most children outgrow wheat allergy, but adults can develop it, often as a cross-sensitivity to grass pollen.
Diagnosis of gluten (wheat) allergy
Gluten allergy test
The wheat allergy diagnosis is difficult because not all of the major wheat grain allergens are recognized. Similarly, to any other allergy, the gold standard of wheat allergy diagnosis remains the oral food challenge. It is usually performed in its open form, as the majority of the observed adverse reactions is of the objective nature. The patient is given whole wheat starting from small doses of wheat-specific protein (1–50 mg) followed by increasingly larger hourly doses (digestion of wheat can be slower than egg or milk), ending with a cumulative dose of up to 0.5–1 g of wheat protein 5. Additionally, double-blind placebo-controlled protocols of wheat allergy have been published both for children 37 and adults 38. Wheat allergy is diagnosed when the challenge test results are positive and the symptoms appear up to two hours after ingestion.
In the next stage, allergological tests should be performed to confirm the elevated levels of wheat allergen-specific IgE. The first are skin tests to wheat flour. Generally, commercial wheat extract is used, the specificity of which is very low 5 Some allergologists prepare an in-house wheat flour solution, but its specificity is also very low. It can be improved by additional testing to ω-5 gliadin or other gliadins, but these solutions are not routinely available and are mainly used in scientific research. In skin test, tiny drops of purified allergen extracts — including extracts for wheat proteins — are pricked onto your skin’s surface, either on your forearm or upper back. After 15 minutes, your doctor or nurse looks for signs of allergic reactions. If you develop a red, itchy bump where the wheat protein extract was pricked onto your skin, you may be allergic to wheat. The most common side effect of these skin tests is itching and redness.
Another step is the determination of serum concentrations of allergen-specific IgE to whole wheat extract. They are commercially available but their specificity is low despite high sensitivity 5.
Solutions used for skin tests to wheat flour and for the assessment of allergen-specific IgE to whole wheat extract consist of the mixture of grain albumins and globulins and, thus, do not contain the insoluble major wheat allergens, i.e., prolamins. This is why the utility of these tests in wheat allergy diagnosis is lower than in allergies to other foods, such as milk, egg, or peanuts 39. Moreover, their concentration is not correlated with the severity of clinical reactions after wheat ingestion.
Gluten-specific IgE can also be assessed. Since the commercial test contains wheat gluten proteins, it is positive only in the case of a wheat allergy and negative in the case of allergies to other gluten-containing cereals. It is not known if it includes major wheat allergens. Gluten-specific IgE assays are positive in two thirds of children with wheat allergy 31.
Currently, there are commercial tests for the IgE specific to two known allergenic molecules of wheat: Tri a 14 non-specific lipid transfer protein and Tri a 19 rω-5-gliadin.
It is characteristic of children who had wheat allergy, and have developed a tolerance to wheat, that in most of them (approximately 80%) skin tests to wheat continue to be positive and IgE specific to whole wheat extract and gluten-specific IgE remain elevated, which is rare in other food allergies 31. For the majority of food allergens, tolerance development is accompanied by negative skin tests and normalized specific IgE levels. In our studies, at the time of tolerance development, the levels of IgE specific to whole wheat extract ranged between 0.35–23.9 kU/L (median: 3.0 kU/L) 31. In that group of people, at the time of wheat allergy diagnosis, the levels of IgE specific to whole wheat extract had been between 2.2 kU/L and 39.3 kU/L (median: 8.42 kU/L). This is why the size of skin test and the levels of IgE specific to whole wheat extract are not useful in differentiating between the periods of allergy and tolerance. It should be stressed, however, that in individual children who have developed tolerance to wheat the skin test values and IgE specific to whole wheat extract and gluten are lower than when wheat allergy was diagnosed.
Gluten allergy management
Avoiding wheat proteins is the best treatment for wheat allergy. Because wheat proteins appear in so many prepared foods, read product labels carefully. It is believed that different species of wheat have the same allergenicity, therefore, it is not recommended for the patients with severe wheat allergy to try different forms of wheat.
The research literature has provided the first report on the oral immunotherapy administered to older children with anaphylaxis triggered by wheat ingestion. After two years, the therapy resulted in the desensitization in 61% of the patients 40. Further studies are necessary to evaluate the effectiveness of this type of wheat allergy treatment.
In the USA the rω-5 gliadin-free variety of wheat has been produced 41.
It is worth emphasizing that even though IgE-mediated wheat allergy belongs to gluten-dependent disorders, it is induced solely by wheat proteins, thus being treated by a wheat-free diet. The remaining gluten cereals, such as rye, barley, and oats are well tolerated by most patients and should not be eliminated from their diet 6. In wheat allergy children, oat allergy is very rare. Rye and barley allergies are slightly more common.
Wheat-free diet
Wheat is found in many foods. To stay away from foods that contain wheat, you must read food labels.
The Food Allergen Labeling and Consumer Protection Act (FALCPA) is a law that requires U.S. packaged foods to state clearly on the label if they contain wheat. Always read the entire ingredient label to look for wheat. Wheat ingredients may be in the ingredient list. Or wheat could be listed in a “contains wheat” statement beneath the ingredient list.
Some foods and products are not covered by the Food Allergen Labeling and Consumer Protection Act (FALCPA). These include:
- Foods that are not regulated by the FDA
- Cosmetics and personal care items
- Prescription and over-the-counter medicines and supplements
- Toys, crafts (Play-Doh), and pet foods
Foods that don’t contain wheat could be contaminated during manufacturing. Advisory statements are not regulated by the FDA. They are voluntary. These include labels such as “processed in a facility that also processed wheat.” Or “made on shared equipment.”
Be sure to stay away from foods that contain any of the following ingredients:
- Bran
- Bread crumbs
- Bulgur
- Cereal extract
- Couscous
- Cracker meal
- Durum
- Einkorn
- Emmer
- Farina
- Flour (enriched, graham, high-gluten, high-protein, whole-wheat)
- Matzoh, matzoh meal
- Pasta
- Seitan
- Semolina
- Spelt
- Vital gluten
- Wheat berries, bran, germ, gluten, grass, malt, sprouted, starch
Ingredients that may contain wheat:
- Gluten
- Gelatinized starch
- Gum
- Hydrolyzed vegetable protein
- Kamut
- Modified food starch
- Modified starch
- Natural flavoring
- Soy sauce
- Starch. Unless otherwise stated on the food label, the single word starch in an ingredient list means cornstarch. Starches from other sources should be noted by some non-misleading term that means the source of the starch, for example: wheat starch.
- Surimi
- Vegetable starch
Gluten free diet
People with a wheat allergy should avoid certain foods containing gluten, but not because of the gluten. Wheat triggers an immune response in their bodies, which can cause symptoms such as a skin rash, headache or sneezing. They can still eat gluten in other grains, including barley and rye.
A gluten-free diet is a diet that excludes foods containing gluten. Gluten is a mix of protein (glutenins and gliadins) found in wheat, rye, and barley. Oats are constitutionally gluten free but can be cross-contaminated with wheat during processing 1. Cross contamination occurs when food allergens come into contact with a food that does not contain that allergen.
If you have medically diagnosed Celiac disease you must follow a strict gluten-free diet for your whole life. This is because your sensitivity to gluten will never disappear. Every time you eat gluten, even in very small amounts, it will cause damage to your small bowel.
Your doctor may advise you to follow a gluten-free diet for other reasons — for example, if you have irritable bowel syndrome or ‘non-celiac gluten sensitivity’. This refers to a range of symptoms attributed to eating gluten, such as dermatitis herpetiformis. Their cause and treatment, however, is not well understood.
On a gluten-free diet you can eat:
- foods that are naturally gluten-free such as fresh fruit and vegetables, fresh meats, eggs, nuts and legumes, milk, fats and oils and gluten-free grains such as rice and corn
- products labelled ‘gluten-free’ irrespective of their country of origin
- products that use the ‘Crossed Grain Logo’. This logo means the food item is suitable for a gluten-free diet wherever you are
- products that are gluten-free according to their ingredients list
Many people think a gluten-free diet is a healthy alternative, but it’s not 42. Gluten-free food products often have higher fat or sugar contents to make the food tastier and give them a better consistency.
A gluten-free diet is essential for people medically diagnosed with Celiac disease. Others need to be very careful because a gluten-free diet can lack essential nutrients if it’s not balanced well 43. Reasons for following a gluten free diet included the belief that the diet would decrease systemic inflammation and improve athletic performance. To further explore this concept, Lis et al. 42 designed a randomized, controlled, double-blind crossover study in 13 nonceliac cyclists. Subjects were randomly assigned to receive either 1 week of a gluten-containing diet or a gluten free diet and then crossed over after a 10-days washout period. Data on gastrointestinal symptoms as well as athletic performance on timed trials were collected at the end of each diet and there were no significant differences found between the short-term gluten free diet compared with the gluten-containing diet 42. Future studies will be needed to further explore if this trend of athletes using a gluten free diet is sustained, and whether this diet makes any significant difference in athletic performance or overall well-being.
Gluten itself doesn’t offer special nutritional benefits but the many whole grains that contain gluten do. They’re rich in an array of vitamins and minerals such as B vitamins, folate and iron, as well as fiber. You may miss out on these nutritional benefits if you follow a gluten-free diet and have not sought professional help from a dietitian to ensure your diet is balanced.
It’s a good idea to seek guidance about following a gluten-free diet from a dietitian, especially if you have other medical conditions or dietary requirements.
A dietitian who works with people with celiac disease can help you plan a healthy gluten-free diet. A dietitian can:
- prepare an individual dietary plan
- show you how to read food labels
- make sure your diet is nutritionally balanced
- determine if you need vitamin supplements.
Some gluten-free foods that people with celiac disease can enjoy include:
- meat products – unprocessed meat, fish, chicken, bacon, ham off the bone and meats that are frozen or canned, but with no sauce
- dairy products – eggs, full-cream milk, low-fat milk, evaporated milk, condensed milk, fresh cream, yogurt, processed or block cheese, and some custards, ice creams and soy milks
- fruits and vegetables – fresh, canned or frozen (but not sauced), fruit juices
- seeds, nuts and nut butters
- gluten-free cereal and baking products – corn (maize) flour, soya flour, lentil flour, rice (all types), rice flour, rice bran, potato flour, sorghum, buckwheat, millet, amaranth, breakfast cereals made from corn and rice (without malt extract from barley), polenta and psyllium
- gluten-free bread, cakes and biscuits – most rice crackers, corn cakes, rice crispbreads, corn tortillas and corn taco shells, packaged breads labelled gluten free, packaged biscuits and cakes labelled gluten free
- gluten-free pasta and noodles – gluten free pasta, rice noodles, rice or bean vermicelli and 100 per cent buckwheat noodles
- condiments – tahini, jam, honey, maple syrup, cocoa, all vinegars (except malt vinegar), tomato pastes, some sauces and some salad dressings
- snacks – plain chips, plain corn chips and unflavored popcorn
- drinks – water, full-cream and low-fat milk, fruit and vegetable juices, tea, coffee, mineral water, wine, spirits and liqueurs.
Naturally gluten-free cereal products and grains that can be enjoyed include:
- amaranth
- arrowroot
- buckwheat (despite its name it is not a type of wheat)
- chestnut flour
- chickpea flour (also known as gram flour and besan)
- coconut flour
- cornflour (from maize) – some cornflours are not made from corn, so always check the label
- cornmeal
- corn tortillas
- lentil flour
- millet meal
- pappadums (most types)
- polenta
- potato flour
- psyllium
- quinoa
- rice (any kind)
- rice bran
- rice flour
- rice vermicelli
- sago
- sorghum
- soy flour
- tapioca
- teff
Are there risks to trying a gluten-free diet if you don’t have celiac disease?
If you cut all gluten out of your diet, there’s a risk that you could miss out on nutritious whole grains, fiber and micronutrients. Getting enough whole grains in your diet is especially important if you’re at risk for heart disease or diabetes. Whole grains can lower cholesterol levels and even help regulate your blood sugar. In addition, some gluten-containing foods are sources of important vitamins and minerals, such as B vitamins, iron and magnesium.
Some processed gluten-free foods contain high amounts of unhealthy ingredients such as sodium, sugar and fat. Consuming these foods can lead to weight gain, blood sugar swings, high blood pressure and other problems. So, a gluten-free label doesn’t necessarily make a food healthy.
If you don’t have celiac disease or gastrointestinal irritation, removing highly processed foods from your diet first before removing gluten. Add in more fruits, vegetables, whole-grain bread or pasta, and lean proteins. Many people find they feel better just by eating better, not by removing gluten.
Can I go gluten-free to lose weight?
People who adopt a gluten-free diet often lose weight, but it’s usually because they also cut out a lot of processed foods and refined carbohydrates that contain gluten. If you stop eating gluten to lose weight, it’s important to watch your portion sizes, get regular exercise and eat plenty of whole foods such as fruits, vegetables and lean proteins.
Drugs
Antihistamines may reduce signs and symptoms of wheat allergies. These drugs can be taken after exposure to wheat to control your reaction and help relieve discomfort. Ask your doctor if a prescription or over-the-counter allergy drug is appropriate for you.
Epinephrine is an emergency treatment for anaphylaxis. If you’re at risk of having a severe reaction to wheat, you may need to carry two injectable doses of epinephrine (EpiPen, Auvi-Q, others) with you at all times. A second pen is recommended for people at high risk of life-threatening anaphylaxis in case anaphylactic symptoms return before emergency care is available.
Home remedies
You can take steps to avoid exposure to wheat proteins and ensure prompt treatment when you’re accidentally exposed to wheat.
- Keep others informed. If your child has wheat allergy, make sure that anyone who takes care of your child, including the principal, teachers and nurse at school, know about the allergy and the signs of wheat exposure. If your child carries epinephrine, make sure school personnel know how to use the pen, if necessary, and that they need to contact emergency care immediately. Inform friends, relatives and co-workers of your own food allergy.
- Wear a bracelet. A medical identification bracelet that describes the allergy and need for emergency care can help if you experience anaphylaxis and can’t communicate.
- Always read labels. Don’t trust that a product is free of what you can’t eat until you read the label. Wheat proteins, especially gluten, are used as food thickeners, and they appear in many unexpected places. Also, don’t assume that once you’ve used a certain brand of a product, that it’s always safe. Ingredients change.
- Shop for gluten-free foods. Some specialty stores and supermarkets offer gluten-free foods, which are safe for people with wheat allergies. However, they may also be free of grains that you can eat, so sticking to gluten-free foods may limit your diet for no reason.
- Consult wheat-free cookbooks. Cookbooks specializing in recipes without wheat can help you cook safely and enable you to enjoy baked goods and other foods made with substitutes for wheat.
- Dine out cautiously. Tell restaurant staff about your allergy and how serious it can be if you eat anything with wheat. Order simple dishes prepared with fresh foods. Avoid foods that may have hidden sources of wheat proteins, such as sauces, or deep-fried foods that may be cooked with other foods containing wheat.
- Mitchell, S., Gomes, A., Zelig, R., & Parker, A. (2019). Not All Grains Are Created Equal: Gluten-Free Products Not Included in Mandatory Folate Fortification. Current developments in nutrition, 3(5), nzz020. https://doi.org/10.1093/cdn/nzz020
- Tanabe S. Analysis of food allergen structures and development of foods for allergic patients. Biosci Biotechnol Biochem. 2008;72:649–659. doi: 10.1271/bbb.70708. https://www.jstage.jst.go.jp/article/bbb/72/3/72_70708/_pdf/-char/en
- Sapone A, Bai JC, Ciacci C, et al. Spectrum of gluten-related disorders: consensus on new nomenclature and classification. BMC Medicine. 2012;10:13. doi:10.1186/1741-7015-10-13. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3292448/
- Barrosa Maia E, Chaves LC, Lemos S, Pinheiro JA. P98 – Gluten allergy. Clinical and Translational Allergy. 2014;4(Suppl 1):P153. doi:10.1186/2045-7022-4-S1-P153. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4082129/
- Mäkelä M. Wheat allergy. In: Matricardi P.M., Kleine-Tebbe J., Hoffmann H., Rudolf V., Ollert M., editors. EAACI Molecular Allergology User’s Guide. 1st ed. European Academy of Allergy and Clinical Immunology; Viena, Austria: 2016. pp. 213–223.
- Czaja-Bulsa G, Bulsa M. What Do We Know Now about IgE-Mediated Wheat Allergy in Children? Nutrients. 2017;9(1):35. doi:10.3390/nu9010035. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5295079/
- Longo G., Berti I., Burks A.W., Krauss B., Brabie E. IgE-mediated food allergy in children. Lancet. 2013;382:1656–1664. doi: 10.1016/S0140-6736(13)60309-8. https://www.ncbi.nlm.nih.gov/pubmed/23845860
- Nwaru B.I., Hickstein L., Panesar S.S., Roberts G., Muraro A., Sheikh A. on behalf of The EAACI Food Allergy and Anaphyllaxis Guidelines Group. Prevelence of common food allergies in Europe. In: Muraro A., Roberts G., editors. Food Allergy and Anaphylaxis Guidelines. 1st ed. European Academy of Allergy and Clinical Immunology (EAACI); Zurich, Switzerland: 2014. pp. 23–45. https://www.ncbi.nlm.nih.gov/pubmed/24816523
- Zuidmeer L., Goldhahn K., Rona R.J., Gislason D., Madsen C., Summers C., Sodergren E., Dahlstrom J., Lindner T., Sigurdardottir S.T., et al. The prevalence of plant food allergies: A systematic review. J. Allergy Clin. Immunol. 2008;121:1210–1218. doi: 10.1016/j.jaci.2008.02.019. https://www.ncbi.nlm.nih.gov/pubmed/18378288
- Ostblom E., Lilja G., Pershagen G., van Hage M., Wickman M. Phenotypes of food hypersensitivity and development of allergic diseases during the first 8 years of life. Clin. Exp. Allergy. 2008;38:1325–1332. doi: 10.1111/j.1365-2222.2008.03010.x. https://www.ncbi.nlm.nih.gov/pubmed/18477012
- Sicherer S.H., Morrow E.H., Sampson H.A. Dose-response in double-blind, placebo-controlled oral food challenges in children with atopic dermatitis. J. Allergy Clin. Immunol. 2004;114:144–149. doi: 10.1067/mai.2000.104941. https://www.ncbi.nlm.nih.gov/pubmed/10719311
- Catassi C., Gatti S., Fasano A. The new epidemiology of celiac disease. J. Pediatr. Gastroenterol. Nutr. 2014;59:S7–S9. doi: 10.1097/01.mpg.0000450393.23156.59. https://www.ncbi.nlm.nih.gov/pubmed/24979197
- Lebwohl, B., Ludvigsson, J. F., & Green, P. H. (2015). Celiac disease and non-celiac gluten sensitivity. BMJ (Clinical research ed.), 351, h4347. https://doi.org/10.1136/bmj.h4347
- Rubio-Tapia A, Ludvigsson JF, Brantner TL, Murray JA, Everhart JE. The prevalence of celiac disease in the United States. Am J Gastroenterol. 2012 Oct;107(10):1538-44; quiz 1537, 1545. doi: 10.1038/ajg.2012.219
- Krigel, A., & Lebwohl, B. (2016). Nonceliac Gluten Sensitivity. Advances in nutrition (Bethesda, Md.), 7(6), 1105–1110. https://doi.org/10.3945/an.116.012849
- Catassi, C., Elli, L., Bonaz, B., Bouma, G., Carroccio, A., Castillejo, G., Cellier, C., Cristofori, F., de Magistris, L., Dolinsek, J., Dieterich, W., Francavilla, R., Hadjivassiliou, M., Holtmeier, W., Körner, U., Leffler, D. A., Lundin, K. E., Mazzarella, G., Mulder, C. J., Pellegrini, N., … Fasano, A. (2015). Diagnosis of Non-Celiac Gluten Sensitivity (NCGS): The Salerno Experts’ Criteria. Nutrients, 7(6), 4966–4977. https://doi.org/10.3390/nu7064966
- Elli, L., Roncoroni, L., & Bardella, M. T. (2015). Non-celiac gluten sensitivity: Time for sifting the grain. World journal of gastroenterology, 21(27), 8221–8226. https://doi.org/10.3748/wjg.v21.i27.8221
- Volta, U., Bardella, M. T., Calabrò, A., Troncone, R., Corazza, G. R., & Study Group for Non-Celiac Gluten Sensitivity (2014). An Italian prospective multicenter survey on patients suspected of having non-celiac gluten sensitivity. BMC medicine, 12, 85. https://doi.org/10.1186/1741-7015-12-85
- Elli L, Tomba C, Branchi F, Roncoroni L, Lombardo V, Bardella MT, Ferretti F, Conte D, Valiante F, Fini L, et al. . Evidence for the presence of non-celiac gluten sensitivity in patients with functional gastrointestinal symptoms: r esults from a multicenter randomized double-blind placebo-controlled gluten challenge. Nutrients 2016;8:84
- Fasano A, Sapone A, Zevallos V, Schuppan D. Nonceliac gluten sensitivity. Gastroenterology. 2015 May;148(6):1195-204. doi: 10.1053/j.gastro.2014.12.049
- Schuppan D, Zevallos V. Wheat amylase trypsin inhibitors as nutritional activators of innate immunity. Dig Dis. 2015;33(2):260-263. doi: 10.1159/000371476
- Biesiekierski JR, Newnham ED, Shepherd SJ, Muir JG, Gibson PR. Characterization of Adults With a Self-Diagnosis of Nonceliac Gluten Sensitivity. Nutr Clin Pract. 2014 Aug;29(4):504-509. doi: 10.1177/0884533614529163
- Biesiekierski JR, Peters SL, Newnham ED, Rosella O, Muir JG, Gibson PR. No effects of gluten in patients with self-reported non-celiac gluten sensitivity after dietary reduction of fermentable, poorly absorbed, short-chain carbohydrates. Gastroenterology. 2013 Aug;145(2):320-8.e1-3. doi: 10.1053/j.gastro.2013.04.051
- Elli, L., Branchi, F., Tomba, C., Villalta, D., Norsa, L., Ferretti, F., Roncoroni, L., & Bardella, M. T. (2015). Diagnosis of gluten related disorders: Celiac disease, wheat allergy and non-celiac gluten sensitivity. World journal of gastroenterology, 21(23), 7110–7119. https://doi.org/10.3748/wjg.v21.i23.7110
- Matricardi PM, Bockelbrink A, Beyer K, Keil T, Niggemann B, Grüber C, Wahn U, Lau S. Primary versus secondary immunoglobulin E sensitization to soy and wheat in the Multi-Centre Allergy Study cohort. Clin Exp Allergy. 2008 Mar;38(3):493-500. doi: 10.1111/j.1365-2222.2007.02912.x
- Keet CA, Matsui EC, Dhillon G, Lenehan P, Paterakis M, Wood RA. The natural history of wheat allergy. Ann Allergy Asthma Immunol. 2009 May;102(5):410-5. doi: 10.1016/S1081-1206(10)60513-3
- Ramesh S. Food allergy overview in children. Clin Rev Allergy Immunol. 2008 Apr;34(2):217-30. doi: 10.1007/s12016-007-8034-1
- Salcedo G, Quirce S, Diaz-Perales A. Wheat allergens associated with Baker’s asthma. J Investig Allergol Clin Immunol. 2011;21(2):81-92; quiz 94.
- Tatham AS, Shewry PR. Allergens to wheat and related cereals. Clin Exp Allergy. 2008 Nov;38(11):1712-26. doi: 10.1111/j.1365-2222.2008.03101.x
- Inomata N. Wheat allergy. Curr Opin Allergy Clin Immunol. 2009 Jun;9(3):238-43. doi: 10.1097/ACI.0b013e32832aa5bc
- Czaja-Bulsa G., Bulsa M. The natural history of IgE mediated wheat allergy in children with dominant gastrointestinal symptoms. Allergy Asthma Clin. Immunol. 2014;10:12. doi: 10.1186/1710-1492-10-12. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3939402/
- Christensen M.J., Eller E., Mortz C.H., Bindslev-Jensen C. Patterns of suspected wheat-related allergy: A retrospective single-centre case note review in 156 patients. Clin. Transl. Allergy. 2014;4:39. doi: 10.1186/2045-7022-4-39. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4405838/
- Linna O. Specific IgE antibodies to uningested cereals. Allergy. 1996;51:849–850. doi: 10.1111/j.1398-9995.1996.tb00034.x. https://www.ncbi.nlm.nih.gov/pubmed/8947346
- Rudd P., Manuel P., Walker-Smith J. Anaphylactic shock in an infant after feeding with a wheat rusk. A transient phenomenon. Postgrad Med. J. 1981;57:794–795. doi: 10.1136/pgmj.57.674.794. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2426275/pdf/postmedj00228-0054.pdf
- Mansouri M., Pourpak Z., Mozafari H., Abdollah Gorji F., Shokouhi Shoormasti R. Follow-up of the wheat allergy in children; consequences and outgrowing the allergy. Iran. J. Allergy Asthma Immunol. 2012;11:157–163. https://www.ncbi.nlm.nih.gov/pubmed/22761189
- Junker Y., Zeissinq S., Kim S.J., Barisani D., Wieser H., Leffler D.A., Zevallos V., Libermann T.A., Dillon S., Freitaq T.L., et al. Wheat amylase trypsin inhibitors drive intestinal inflammation via activation of toll-like receptor 4. J. Exp. Med. 2012;209:2395–2408. doi: 10.1084/jem.20102660. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3526354/
- Ito K., Futamura M., Borres M.P., Takaoka Y., Dahlstrom J., Sakamoto T., Tanaka A., Kohno K., Matsuo H., Morita E. IgE antibodies to ω-5 gliadin associate with immediate symptoms on oral wheat challenge in Japanese children. Allergy. 2008;63:1536–1542. doi: 10.1111/j.1398-9995.2008.01753.x. https://www.ncbi.nlm.nih.gov/pubmed/18925890
- Scibilia J., Pastorello E.A., Zisa G., Ottolenghi A., Bindslev-Jensen C., Pravettoni V., Scovena E., Robino A., Ortolani C. Wheat allergy: A double-blind, placebo-controlled study in adults. J. Allergy Clin. Immunol. 2006;117:433–439. doi: 10.1016/j.jaci.2005.10.014. https://www.ncbi.nlm.nih.gov/pubmed/16461145
- Sampson H.A. Utility of food-specific IgE concentrations in predicting symptomatic food allergy. J. Allergy Clin. Immunol. 2001;107:891–896. doi: 10.1067/mai.2001.114708. https://www.ncbi.nlm.nih.gov/pubmed/11344358
- Sato S., Utsunomiya T., Imai T., Yanagida N. Wheat oral immunotherapy for wheat-induced anaphylaxis. J. Allergy Clin. Immunol. 2015;4:1131–1133. doi: 10.1016/j.jaci.2015.07.019. https://www.ncbi.nlm.nih.gov/pubmed/26319801
- Altenbach S.B., Allen P.V. Transformation of the US bread wheat ‘Butte 86’ and silencing of omega-5 gliadin genes. GM Crops. 2011;2:66–73. doi: 10.4161/gmcr.2.1.15884. https://www.ncbi.nlm.nih.gov/pubmed/21844700
- Lis D, Stellingwerff T, Kitic CM, Ahuja KD, Fell J. No Effects of a Short-Term Gluten-free Diet on Performance in Nonceliac Athletes. Med Sci Sports Exerc. 2015 Dec;47(12):2563-70. doi: 10.1249/MSS.0000000000000699
- Shepherd SJ, Gibson PR. Nutritional inadequacies of the gluten-free diet in both recently-diagnosed and long-term patients with coeliac disease. J Hum Nutr Diet. 2013 Aug;26(4):349-58. doi: 10.1111/jhn.12018





{kind=link}