
What is a goiter
Goiter is an enlargement of the thyroid gland that causes a lump to form in the front of the neck (see Figure 4). The lump will move up and down when you swallow. Although goiters are usually painless, the resulting lump on the neck may become extremely large, but most simple goiters are brought under control before this happens. Occasionally a simple goiter may cause some difficulty in breathing and swallowing.
The most common cause of goiters worldwide is a lack of iodine in the diet. In the United States, where the use of iodized salt is common, a goiter is more often due to the over- or underproduction of thyroid hormones or to nodules that develop in the gland itself.
Goiters are more common in women than men, and may be either physiological or pathological. They are present on examination in up to 9% of the population.
The size of a goiter can vary from person to person. In most cases, the swelling is small and doesn’t cause any symptoms.
In more severe cases, the symptoms may include:
- coughing
- a tight feeling in your throat
- changes to your voice, such as hoarseness
- difficulty swallowing (dysphagia)
- difficulty breathing – there may be a high-pitched sound when you breathe (stridor)
As the goiter develops the entire neck looks swollen because of the large thyroid. This mass will compress the trachea and esophagus, leading to goiter symptoms such as coughing, waking up from sleep feeling like you can’t breath, and the sensation that food is getting stuck in the upper throat.
Treatment depends on the size of the goiter, your symptoms and the underlying cause. Small goiters that aren’t noticeable and don’t cause problems usually don’t need treatment.
The Thyroid Gland
Your thyroid is a small butterfly-shaped gland found at the base of your neck, just below your Adam’s apple. This gland makes thyroid hormone that travels in your blood to all parts of your body. The thyroid hormone controls your body’s metabolism in many ways, including how fast you burn calories and how fast your heart beats.
Figure 1. Thyroid gland location
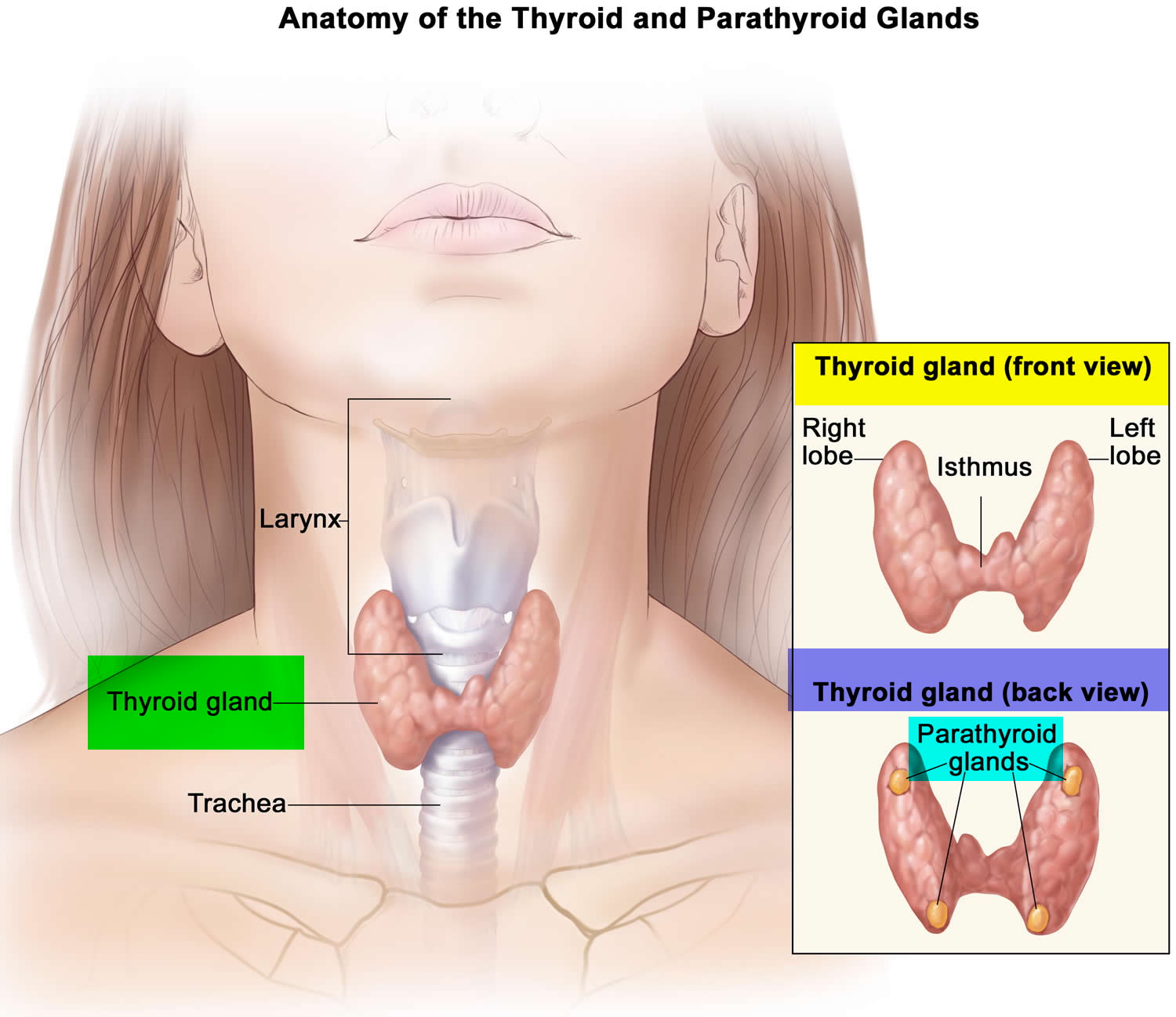
Figure 2. Thyroid gland location
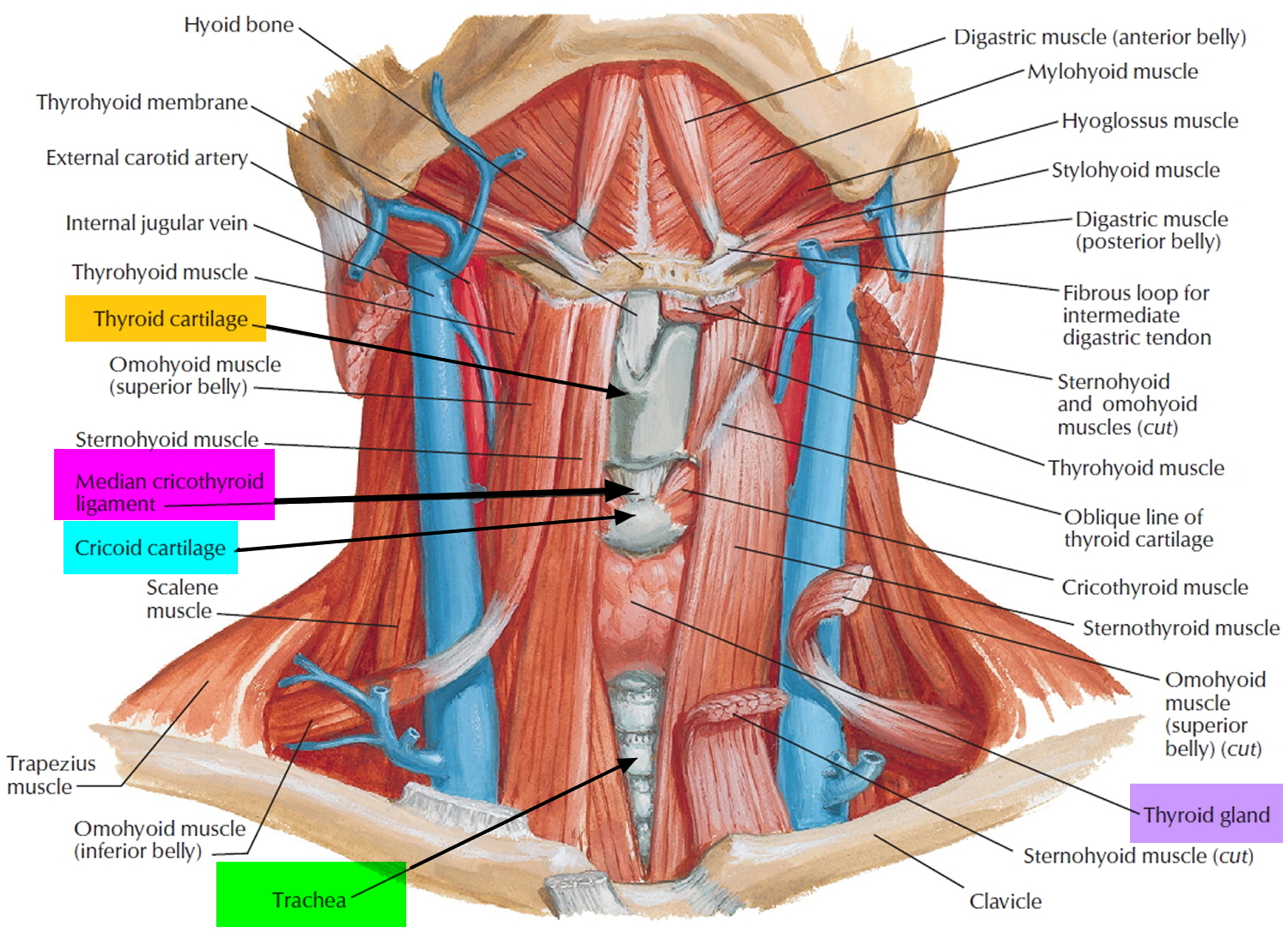
Figure 3. Thyroid gland
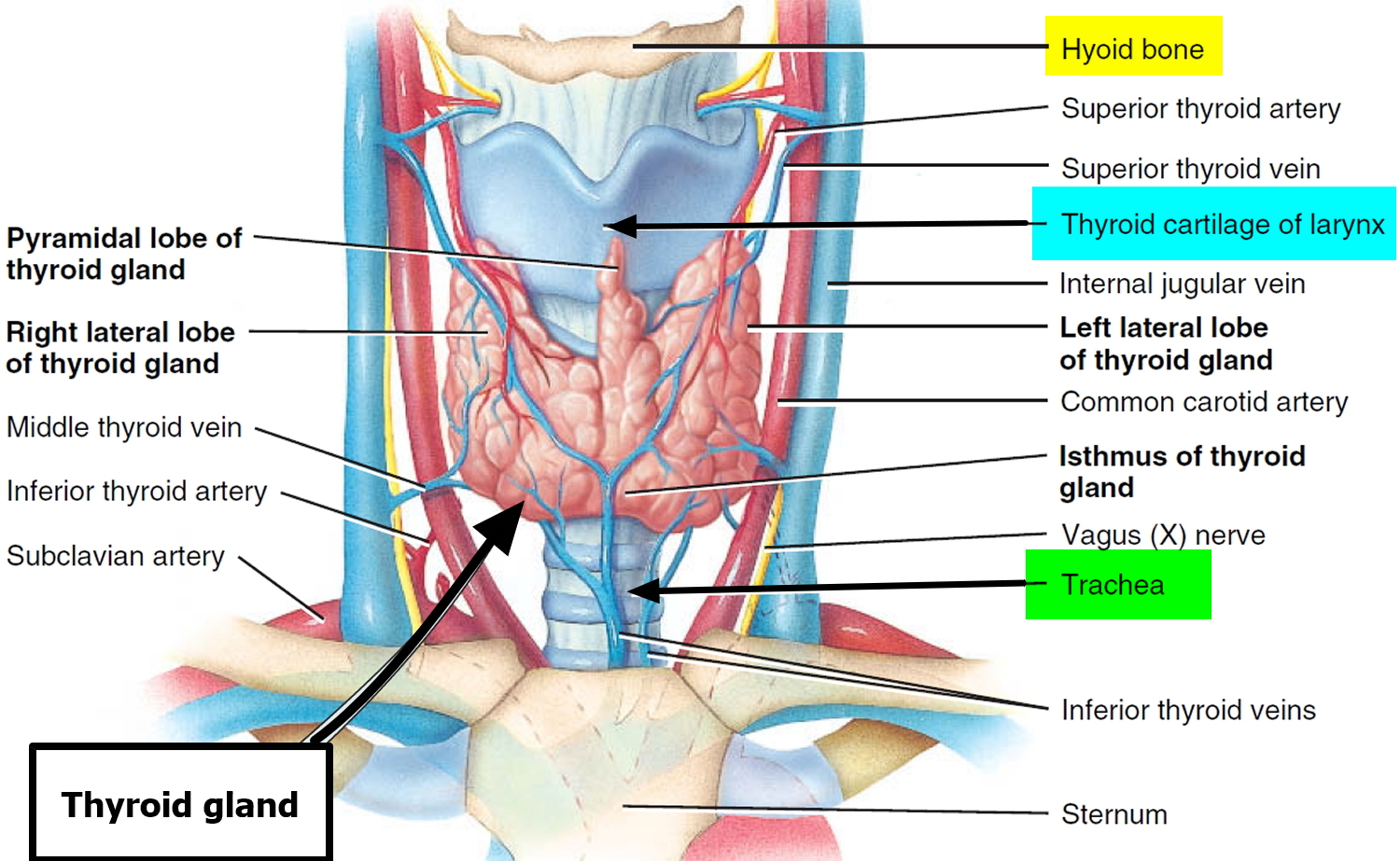
Figure 4. Thyroid goiter

Types of goiter
There are two main types of goiter:
- Diffuse goiter – where the entire thyroid gland swells and feels smooth to the touch
- Nodular goiter – where solid or fluid-filled lumps called nodules develop within the thyroid and make the thyroid gland feel lumpy to touch; the nodules can be single or multiple and may contain fluid (cysts).
Toxic nodular goiter
Toxic nodular goiter involves an enlarged thyroid gland. The gland contains areas that have increased in size and formed nodules. One or more of these nodules produce too much thyroid hormone.
Causes of toxic nodular goiter
Toxic nodular goiter starts from an existing simple goiter. It occurs most often in older adults. Risk factors include being female and over 55 years old. This disorder is rare in children. Most people who develop it have had a goiter with nodules for many years.
Sometimes, people with toxic multinodular goiter will develop high thyroid levels for the first time. This mostly occurs after they take in a large amount of iodine through a vein (intravenously) or by mouth. The iodine may be used as contrast for a CT scan or heart catheterization. Taking medicines that contain iodine, such as amiodarone, may also lead to the disorder.
Toxic nodular goiter possible complications
Heart complications:
- Heart failure
- Irregular heartbeat (atrial fibrillation)
- Rapid heart rate
Other complications:
Bone loss leading to osteoporosis
Thyroid crisis or storm is an acute worsening of hyperthyroidism symptoms. It may occur with infection or stress. Thyroid crisis may cause:
- Abdominal pain
- Decreased mental alertness
- Fever
People with this condition need to go to the hospital right away.
Complications of having a very large goiter may include difficulty breathing or swallowing. These complications are due to pressure on the airway passage (trachea) or esophagus, which lies behind the thyroid.
Toxic nodular goiter symptoms
Symptoms are the same as those of an overactive thyroid gland (hyperthyroidism). However, the bulging eyeballs seen in Graves disease do not occur.
Symptoms may include any of the following:
- Fatigue
- Frequent bowel movements
- Heat intolerance
- Increased appetite
- Increased sweating
- Irregular menstrual period (in women)
- Muscle cramps
- Nervousness
- Restlessness
- Weight loss
Toxic nodular goiter diagnosis
A physical examination will show 1 or many nodules in the thyroid. There may be a rapid heart rate.
Other tests that may be done include:
- Serum thyroid hormone levels (T3, T4)
- Serum TSH (thyroid stimulating hormone)
- Thyroid uptake and scan or radioactive iodine uptake
- Thyroid ultrasound
Toxic nodular goiter treatment
Beta-blockers (propranolol) can control some of the symptoms of hyperthyroidism until thyroid hormone levels in the body are under control.
Certain drugs can block or change how the thyroid gland uses iodine. These drugs may be used to control the overactive thyroid gland in any of the following cases:
- Before surgery or radioiodine therapy occurs
- As a long term treatment
Radioiodine therapy may be used. Radioactive iodine is given by mouth. It then concentrates in the overactive thyroid tissue and causes damage. Some people, but not all, may need to take thyroid replacement afterwards.
Surgery to remove the thyroid may be done when:
- Very large goiter or a goiter is causing symptoms by blocking the airway
- Thyroid cancer is present
- Rapid treatment is needed.
Toxic nodular goiter outlook (prognosis)
Toxic nodular goiter is mainly a disease of older adults, so other chronic health problems may affect the outcome of this condition. An older adult may be less able to tolerate the effect of the disease on the heart. However, the condition is often treatable with medicines.
Nontoxic multinodular goiter
Both diffuse and nodular goiters are usually caused by an imbalance in certain hormones. For example, not getting enough iodine in the diet can cause changes in hormone levels and lead to a goiter.
Lumps or bumps in the thyroid gland are called thyroid nodules. Most thyroid nodules are benign, but about 2 or 3 in 20 are cancerous. Sometimes these nodules make too much thyroid hormone and cause hyperthyroidism. Nodules that produce increased thyroid hormone are almost always benign.
People can develop thyroid nodules at any age, but they occur most commonly in older adults. Fewer than 1 in 10 adults have thyroid nodules that can be felt by a doctor. But when the thyroid is looked at with ultrasound, many more people are found to have nodules that are too small to feel. Most evidence suggests that they are benign.
Most nodules are cysts filled with fluid or with a stored form of thyroid hormone called colloid. Solid nodules have little fluid or colloid. These nodules are more likely to be cancerous than are fluid-filled nodules. Still, most solid nodules are not cancer. Some types of solid nodules, such as hyperplastic nodules and adenomas, have too many cells, but the cells are not cancer cells.
Benign thyroid nodules sometimes can be left alone (not treated) as long as they’re not growing or causing symptoms. Others may require some form of treatment.
Radioiodine scans can be used to help determine if someone with a lump in the neck might have thyroid cancer. They are also often used in people who have already been diagnosed with differentiated (papillary, follicular, or Hürthle cell) thyroid cancer to help show if it has spread. Because medullary thyroid cancer cells do not absorb iodine, radioiodine scans are not used for this cancer.
For this test, a small amount of radioactive iodine (called I-131) is swallowed (usually as a pill) or injected into a vein. Over time, the iodine is absorbed by the thyroid gland (or thyroid cells anywhere in the body). A special camera is used several hours later to see where the radioactivity is.
For a thyroid scan, the camera is placed in front of your neck to measure the amount of radiation in the gland. Abnormal areas of the thyroid that have less radioactivity than the surrounding tissue are called cold nodules, and areas that take up more radiation are called hot nodules. Hot nodules usually are not cancerous, but cold nodules can be benign or cancerous. Because both benign and cancerous nodules can appear cold, this test by itself can’t diagnose thyroid cancer.
Ultrasound uses sound waves to create images of parts of your body. For this test, a small, wand-like instrument called a transducer is placed on the skin in front of your thyroid gland. It gives off sound waves and picks up the echoes as they bounce off the thyroid. The echoes are converted by a computer into a black and white image on a computer screen. You are not exposed to radiation during this test.
This test can help determine if a thyroid nodule is solid or filled with fluid. (Solid nodules are more likely to be cancerous.) It can also be used to check the number and size of thyroid nodules. How a nodule looks on ultrasound can sometimes suggest if it is likely to be a cancer, but ultrasound can’t tell for sure.
The actual diagnosis of thyroid cancer is made with a biopsy, in which cells from the suspicious area are removed and looked at under a microscope. However, this might not be the first test done if you have a suspicious lump in your neck. The doctor might order other tests first, such as blood tests, an ultrasound exam, or a radioiodine scan to get a better sense of whether you might have thyroid cancer. If your doctor thinks a biopsy is needed, the simplest way to find out if a thyroid lump or nodule is cancerous is with a fine needle aspiration (FNA) of the thyroid nodule. This type of biopsy can usually be done in your doctor’s office or clinic.
This test is generally done on all thyroid nodules that are big enough to be felt. This means that they are larger than about 1 centimeter (about 1/2 inch) across. Doctors often use ultrasound to see the thyroid during the biopsy, which helps make sure they are getting samples from the right areas. This is especially helpful for smaller nodules. FNA biopsies can also be used to get samples of swollen lymph nodes in the neck to see if they contain cancer.
Sometimes an FNA biopsy will need to be repeated because the samples didn’t contain enough cells. Most FNA biopsies will show that the thyroid nodule is benign. Rarely, the biopsy may come back as benign even though cancer is present. Cancer is clearly diagnosed in only about 1 of every 20 FNA biopsies.
Sometimes the test results first come back as “suspicious” or “of undetermined significance” if FNA findings don’t show for sure if the nodule is either benign or malignant. If this happens, the doctor may order tests on the sample to see if the BRAF or RET/PTC genes are mutated (changed). Finding these changes makes thyroid cancer much more likely, and may also play a role in determining the best treatment for the cancer.
If the diagnosis is not clear after an FNA biopsy, you might need a more involved biopsy to get a better sample, particularly if the doctor has reason to think the nodule may be cancerous. This might include a core biopsy using a larger needle, a surgical “open” biopsy to remove the nodule, or a lobectomy (removal of half of the thyroid gland). Surgical biopsies and lobectomies are done in an operating room while you are under general anesthesia (in a deep sleep). A lobectomy can also be the main treatment for some early cancers, although for many cancers the rest of the thyroid will need to be removed as well (during an operation called a completion thyroidectomy).
Goiter prognosis (outlook)
A goiter is a benign disease. Simple goiter may disappear spontaneously, or may become enlarged. Over time, hypothyroidism may develop due to destruction of the normal thyroid tissue. This can be treated with medications to replace the thyroid hormones.
On the odd occasion, a goiter may progress to a toxic state when a nodule is making thyroid hormones on its own. This can cause hyperthyroidism. It can be treated with radioactive iodine to destroy the nodule.
Goiter causes
Having a goiter doesn’t necessarily mean that your thyroid gland isn’t working normally. Even when it’s enlarged, your thyroid may produce normal amounts of hormones. It might also, however, produce too much or too little thyroxine (T4) and T3.
A number of factors can cause your thyroid gland to enlarge. Among the most common are:
- Iodine deficiency. Iodine, which is essential for the production of thyroid hormones, is found primarily in seawater and in the soil in coastal areas. In the developing world, people who live inland or at high elevations are often iodine deficient and can develop goiters when the thyroid enlarges in an effort to obtain more iodine. The initial iodine deficiency may be made even worse by a diet high in hormone-inhibiting foods, such as cabbage, broccoli and cauliflower. Although a lack of dietary iodine is the main cause of goiters in many parts of the world, this is not often the case in countries where iodine is routinely added to table salt and other foods.
- Graves’ disease. A goiter can sometimes occur when your thyroid gland produces too much thyroid hormone (hyperthyroidism). In Graves’ disease, antibodies produced by your immune system mistakenly attack your thyroid gland, causing it to produce excess thyroxine. This overstimulation causes the thyroid to swell.
- Hashimoto’s disease. A goiter can also result from an underactive thyroid (hypothyroidism). Like Graves’ disease, Hashimoto’s disease is an autoimmune disorder. But instead of causing your thyroid to produce too much hormone, Hashimoto’s damages your thyroid so that it produces too little. Sensing a low hormone level, your pituitary gland produces more TSH to stimulate the thyroid, which then causes the gland to enlarge.
- Multinodular goiter. In this condition, several solid or fluid-filled lumps called nodules develop in both sides of your thyroid, resulting in overall enlargement of the gland.
- Solitary thyroid nodules. In this case, a single nodule develops in one part of your thyroid gland. Most nodules are noncancerous (benign) and don’t lead to cancer.
- Thyroid cancer. Thyroid cancer is far less common than benign thyroid nodules. A biopsy of a thyroid nodule is very accurate in determining if it’s cancerous.
- Pregnancy. A hormone produced during pregnancy, human chorionic gonadotropin (HCG), may cause your thyroid gland to enlarge slightly.
- Inflammation. Thyroiditis is an inflammatory condition that can cause pain and swelling in the thyroid. It may also cause an over- or underproduction of thyroxine.
A goiter can have several possible causes, including:
- an overactive thyroid gland (hyperthyroidism)
- an underactive thyroid gland (hypothyroidism)
- hormone changes during puberty, pregnancy or the menopause
- not enough iodine (a trace mineral found in fish and plant foods) in your diet
- taking some types of medication – such as lithium, a medication often used to treat a number of mental health conditions
- an inflamed thyroid gland (thyroiditis)
- having radiation treatment to your neck or chest area – such as radiotherapy for neck cancer
- nodules or cysts within the thyroid – most are benign, but should be assessed
- thyroid cancer – a rare type of cancer in the US
Anyone can develop a goiter, but the chances increase with age. Women are also more likely to develop a goiter.
Risk Factors for thyroid goiter enlargement
Goiters can affect anyone. They may be present at birth and occur at any time throughout life.
Some common risk factors for goiters include:
- Physiological – puberty, pregnancy
- Autoimmune – Graves’ disease, Hashimoto’s disease
- Thyroiditis: acute (de Quervain’s), chronic fibrotic (Reidel’s)
- Iodine deficiency (endemic goiter). People living in areas where iodine is in short supply and who don’t have access to iodine supplements are at high risk of goiters.
- Being female. Because women are more prone to thyroid disorders, they’re also more likely to develop goiters.
- Your age. Goiters are more common after age 40.
- Medical history. A personal or family history of autoimmune disease increases your risk.
- Pregnancy and menopause. For reasons that aren’t entirely clear, thyroid problems are more likely to occur during pregnancy and menopause.
- Certain medications. Some medical treatments, including the heart drug amiodarone (Cordarone, Pacerone, others) and the psychiatric drug lithium (Lithobid, others), increase your risk.
- Radiation exposure. Your risk increases if you’ve had radiation treatments to your neck or chest area or you’ve been exposed to radiation in a nuclear facility, test or accident.
Goiter complications
Small goiters that don’t cause physical or cosmetic problems aren’t a concern. But large goiters can make it hard to breathe or swallow and can cause a cough and hoarseness.
Goiters that result from other conditions, such as hypothyroidism or hyperthyroidism, can be associated with a number of symptoms, ranging from fatigue and weight gain to unintended weight loss, irritability and trouble sleeping.
Goiter symptoms
Not all goiters cause signs and symptoms. When signs and symptoms do occur they may include:
- A visible swelling at the base of your neck that may be particularly obvious when you shave or put on makeup
- A tight feeling in your throat
- Coughing
- Hoarseness
- Difficulty swallowing
- Difficulty breathing.
Goiter diagnosis
If you think you have a goiter, see your doctor. They’ll examine your neck to see whether your thyroid gland is swollen, and may request a thyroid function test to see how well your thyroid gland is working.
A thyroid function test measures the level of certain hormones (chemicals produced by the body) in your blood.
It can show whether you have an underactive or overactive thyroid, both of which are associated with goiter.
If necessary, you may be referred to a specialist in hospital for further tests or treatment.
A hormone test
Blood tests can determine the amount of hormones produced by your thyroid and pituitary glands. If your thyroid is underactive, the level of thyroid hormone will be low. At the same time, the level of thyroid-stimulating hormone (TSH) will be elevated because your pituitary gland tries to stimulate your thyroid gland to produce more thyroid hormone.
A goiter associated with an overactive thyroid usually involves a high level of thyroid hormone in the blood and a lower than normal TSH level.
An antibody test
Some causes of a goiter involve production of abnormal antibodies. A blood test may confirm the presence of these antibodies.
Thyroid function test
A thyroid function test is a type of blood test. A sample of your blood is taken and measured for levels of:
- thyroid-stimulating hormone (TSH)
- thyroxine and triiodothyronine (the thyroid hormones)
If you have lower or higher-than-average levels of these hormones, it could mean you have a thyroid condition or are at risk of developing one in the future.
Your doctor may refer you to a specialist thyroid clinic or a specialist in hormone-related conditions (an endocrinologist) if you have a thyroid swelling and:
- it’s getting bigger
- you have a family history of thyroid cancer
- you’ve had radiation treatment to your neck
- you have swollen lymph nodes in your neck
- you’re a child or teenager
- you’re 65 or over
- your voice has changed
- you’re making a high-pitched noise as you breathe (stridor)
- you’re having difficulty breathing or swallowing
If you’re referred to a specialist, you may have further tests in hospital. These are described in more detail below.
Radioactive iodine scan
This involves a small amount of radioactive iodine being injected into your vein. The iodine builds up in your thyroid gland, which can then be studied using a special camera.
The time needed for the procedure may vary, depending on how long it takes the isotope to reach your thyroid gland. Thyroid scans provide information about the nature and size of your thyroid, but they’re more invasive, time-consuming and expensive than are ultrasound tests.
The scan can provide useful information about the structure and function of your thyroid gland. As the amount of radiation used is very small, it’s perfectly safe for most people. However, it may not be suitable if you’re pregnant.
Ultrasound scan
An ultrasound scan uses high-frequency sound waves to create an image of part of the inside of your body. It can be used to:
- build up a picture of the inside of your thyroid gland
- assess the size of your thyroid gland
- check whether there are any enlarged nodules in your thyroid gland not found during the physical examination
Fine-needle aspiration
Fine-needle aspiration is a procedure where a sample of the goiter is extracted so the cells inside it can be tested. This procedure is often known as a biopsy.
During the procedure, a fine needle on the end of a syringe is inserted into the goiter in your throat. A sample of the fluid or tissue inside the goiter is sucked through the needle into the syringe.
The sample can be examined under a microscope to determine what kind of cells are inside the goiter.
Goiter treatment
Many goiters are small, cause no symptoms and can be observed. In particular, during puberty and pregnancy a goiter associated with euthyroidism (normal thyroid function) rarely requires intervention. The problem will usually fix itself.
Goiters are often removed because of cosmetic reasons or, more commonly, because they compress the trachea and the esophagus and thus make breathing and swallowing difficult. Sometimes goiters will grow into the chest, where they can cause trouble as well.
Although most goiters are usually non-cancerous (benign), it’s estimated that in 1 in 20 cases they may be a sign of thyroid cancer.
Treatment for a goiter can include medication, hormone therapy and surgery.
The treatment you receive will depend on:
- the size of the goiter
- the symptoms the goiter is causing
- whether you have any underlying thyroid condition
Your condition may just be monitored if tests reveal your thyroid gland is working normally and the goiter is small.
If your goiter is interfering with your breathing or swallowing and it hasn’t responded to other forms of treatment, you may need surgery to remove part or all of your thyroid gland. This procedure is known as a thyroidectomy.
Treating thyroid gland problems
If tests reveal a problem with your thyroid gland, you may receive treatment for:
- an overactive thyroid gland (hyperthyroidism) – which may include taking a type of medication known as thionamides or a type of radiotherapy called radioiodine treatment
- an underactive thyroid gland (hypothyroidism) – which usually involves taking a synthetic hormone called levothyroxine to replicate your normal thyroid function (hormone therapy)
Iodine supplements
A well-balanced diet usually provides all the iodine your body needs, and iodine supplements aren’t usually required in developed countries like the US. Your doctor can give more advice about extra supplements, if needed.
Iodine supplements are available in many health food shops without a prescription. However, always consult your doctor before taking them as the amount of iodine needed varies from person to person.
Taking too much iodine may cause other health problems, and it could also have toxic effects.
Lifestyle and home remedies
If your goiter is caused by your diet, these suggestions can help:
- Get enough iodine. To ensure that you get enough iodine, use iodized salt or eat seafood or seaweed — sushi is a good seaweed source — about twice a week. Shrimp and other shellfish are particularly high in iodine. If you live near the coast, locally grown fruits and vegetables are likely to contain some iodine, too, as are cow’s milk and yogurt. Everyone needs about 150 micrograms of iodine a day (the amount in slightly less than half a teaspoon of iodized salt). But adequate amounts are especially important for pregnant and lactating women and for infants and children.
- Avoid excess iodine consumption. Although it’s uncommon, getting too much iodine sometimes leads to a goiter. If excess iodine is a problem, avoid iodine-fortified salt, shellfish, seaweed and iodine supplements.
Goiter surgery
Before a thyroidectomy, you’ll be given a general anesthetic so you’re unconscious and unable to feel anything.
During surgery, the surgeon makes a cut (incision) in the front of your neck so they can see your thyroid gland.
How much of the thyroid gland is removed depends on the underlying condition causing the goiter. The procedure reduces the size of your goiter and the amount of thyroid hormones being produced.
The surgeon will attempt to remove enough of your thyroid gland to relieve your symptoms, while leaving enough so normal thyroid hormone production can continue.
However, if this isn’t possible, you may require hormone therapy after surgery.
Surgery to remove the thyroid gland is usually safe, but as with all surgical procedures there’s a risk of complications, such as postoperative infection.
Complications of a thyroidectomy
The risks of complications occurring after thyroid gland surgery are estimated to be 1-2%. Before having the procedure, you should discuss the risks with your surgeon.
Nerve damage and parathyroid gland damage are two other possible complications of thyroid gland surgery. These are briefly described below.
Nerve damage
The thyroid gland is very close to the two laryngeal nerves, which control your vocal cords. If these are accidentally damaged during surgery, your voice and breathing could be affected.
Permanent damage to the laryngeal nerves affects 1-2 people in every 100 who have this type of surgery. Temporary damage may affect up to 5 people in every 100.
Parathyroid gland damage
The parathyroid glands help regulate the amount of calcium in your body. If the parathyroid glands are damaged, you’ll probably need to take calcium supplements for the rest of your life.
Overactive thyroid (hyperthyroidism) treatment
An overactive thyroid (hyperthyroidism) is usually treatable.
You’ll normally be referred to an endocrinologist (specialist in hormone conditions) to plan your treatment.
The main treatments are:
- medication
- radioiodine treatment
- surgery
Medication
Medicines called thionamides are a common treatment for an overactive thyroid. These stop your thyroid producing excess hormones.
The main types used are methimazole, carbimazole and propylthiouracil.
You’ll usually need to take the medicine for a month or two before you notice any benefit. You may be given another medication called a beta-blocker to quickly relieve your symptoms in the meantime.
Once your thyroid hormone level is under control, your dose may be gradually reduced and then stopped. But some people need to continue taking medication for several years or possibly for life.
Side effects
During the first couple of months, some people experience the following side effects:
- feeling sick
- headaches
- aching joints
- an upset stomach
- an itchy rash
These should pass as your body gets used to the medication.
A less common but more serious side effect is a sudden drop in your white blood cell level (agranulocytosis), which can mean you’re very vulnerable to infections.
Contact your doctor immediately if you get symptoms of agranulocytosis, such as a fever, sore throat or persistent cough so a blood test can be carried out to check your white blood cell level.
Radioiodine treatment
Radioiodine treatment is where radiation is used to damage your thyroid, reducing the amount of hormones it can produce. It’s a highly effective treatment that can cure an overactive thyroid.
You’re given a drink or capsule that contains a low dose of radiation, which is then absorbed by your thyroid. Most people only require a single treatment.
It can take a few weeks or months for the full benefits to be felt, so you may need to take one of the medications mentioned above for a short time.
The dose of radiation you’re given is very low, but there are some precautions you’ll need to take after treatment:
avoid prolonged close contact with children and pregnant women for a few days or weeks
women should avoid getting pregnant for at least six months
men shouldn’t father a child for at least four months
Radioiodine treatment isn’t suitable if you’re pregnant or breastfeeding. It’s also not suitable if your overactive thyroid is causing severe eye problems.
Surgery
Occasionally, surgery to remove all or part of your thyroid may be recommended.
This may be the best option if:
- your thyroid gland is severely swollen (a large goiter)
- you have severe eye problems resulting from an overactive thyroid
- you can’t have the other treatments mentioned above
- your symptoms come back after trying the treatments mentioned above
Removing the entire thyroid gland is normally recommended, as this cures an overactive thyroid and means there’s no chance of the symptoms coming back.
But as a result, you’ll need to take medication for the rest of your life to make up for not having a thyroid – these are the same medications used to treat an underactive thyroid.
Underactive thyroid (hypothyroidism) treatment
An underactive thyroid (hypothyroidism) is usually treated by taking daily hormone replacement tablets called levothyroxine.
Levothyroxine replaces the thyroxine hormone, which your thyroid doesn’t make enough of.
You’ll initially have regular blood tests until the correct dose of levothyroxine is reached. This can take a little while to get right.
You may start on a low dose of levothyroxine, which may be increased gradually, depending on how your body responds. Some people start to feel better soon after beginning treatment, while others don’t notice an improvement in their symptoms for several months
Once you’re taking the correct dose, you’ll usually have a blood test once a year to monitor your hormone levels.
If blood tests suggest you may have an underactive thyroid, but you don’t have any symptoms or they’re very mild, you may not need any treatment. In these cases, your doctor will usually monitor your hormone levels every few months and prescribe levothyroxine if you develop symptoms.
Underactive thyroid and pregnancy
It’s important for the health of you and your baby that an underactive thyroid is treated properly before you become pregnant.
Tell your doctor if you’re pregnant or trying to become pregnant and you have hypothyroidism. They may refer you to a specialist for treatment and monitoring during your pregnancy.
Taking levothyroxine
If you’re prescribed levothyroxine, you should take one tablet at the same time every day. It’s usually recommended that you take the tablets in the morning, although some people prefer to take them at night. This oral medication restores adequate hormone levels, reversing the signs and symptoms of hypothyroidism.
One to two weeks after starting treatment, you’ll notice that you’re feeling less fatigued. The medication also gradually lowers cholesterol levels elevated by the disease and may reverse any weight gain. Treatment with levothyroxine is usually lifelong, but because the dosage you need may change, your doctor is likely to check your TSH level every year.
The effectiveness of the tablets can be altered by other medications, supplements or foods, so they should be swallowed with water on an empty stomach, and you should avoid eating for 30 minutes afterwards.
If you forget to take a dose, take it as soon as you remember, if this is within a few hours of your usual time. If you don’t remember until later than this, skip the dose and take the next dose at the usual time, unless advised otherwise by your doctor.
An underactive thyroid is a lifelong condition, so you’ll usually need to take levothyroxine for the rest of your life.
To determine the right dosage of levothyroxine initially, your doctor generally checks your level of TSH after two to three months. Excessive amounts of the hormone can cause side effects, such as:
- Increased appetite
- Insomnia
- Heart palpitations
- Shakiness
If you have coronary artery disease or severe hypothyroidism, your doctor may start treatment with a smaller amount of medication and gradually increase the dosage. Progressive hormone replacement allows your heart to adjust to the increase in metabolism.
Proper absorption of levothyroxine
Certain medications, supplements and even some foods may affect your ability to absorb levothyroxine. Talk to your doctor if you eat large amounts of soy products or a high-fiber diet or you take other medications, such as:
- Iron supplements or multivitamins that contain iron
- Cholestyramine
- Aluminum hydroxide, which is found in some antacids
- Calcium supplements
If you have subclinical hypothyroidism, discuss treatment with your doctor. For a relatively mild increase in TSH, you probably won’t benefit from thyroid hormone therapy, and treatment could even be harmful. On the other hand, for a higher TSH level, thyroid hormones may improve your cholesterol level, the pumping ability of your heart and your energy level.
Side effects
Levothyroxine causes virtually no side effects when used in the appropriate dose and is relatively inexpensive. If you change brands, let your doctor know to ensure you’re still receiving the right dosage. Also, don’t skip doses or stop taking the drug because you’re feeling better. If you do, the symptoms of hypothyroidism will gradually return.
Side effects usually only occur if you’re taking too much levothyroxine. This can cause problems including sweating, chest pain, headaches, diarrhea and vomiting.
Tell your doctor if you develop new symptoms while taking levothyroxine. You should also let them know if your symptoms get worse or don’t improve.





{kind=link}