
What is hemoptysis
Hemoptysis is the medical term for coughing up blood that comes from your lungs or bronchial tubes. Hemoptysis can range from small flecks of blood to a lot of bleeding. If you, or someone you know, has coughed up a lot of blood, or has coughed up blood and also has serious shortness of breath, or if the bleeding does not stop, call your local emergency services number immediately. Don’t self diagnose yourself. Always leave that to a doctor.
Hemoptysis is life threatening in fewer than 1 in 20 cases, but if you cough up blood, it is still very important that you see your doctor to get checked out.
You may cough up small amounts of bright red blood, or frothy blood-streaked sputum (phlegm). The blood is usually from your lungs and is often the result of prolonged coughing or a chest infection.
Coughing up blood does not include having blood in your saliva due to bleeding in your mouth, upper airway or from vomiting of blood from your gut.
If the blood is dark and contains bits of food or what look like coffee grounds, it may be coming from your digestive system. This is a more serious problem and you should go to hospital straight away.
Coughing up blood is not the same as bleeding from the mouth, throat, or gastrointestinal tract.
Blood that comes up with a cough often looks bubbly because it is mixed with air and mucus. It is most often bright red, although it may be rust-colored. Sometimes the mucus contains only streaks of blood.
The volume of blood produced has traditionally been used to differentiate between nonmassive and massive hemoptysis; the cutoff value ranges from 100 to 600 mL of blood produced in a 24-hour period 1. Coughing up of more than 200 mL of blood per 24 hours is considered massive hemoptysis 2. Because of the practical difficulties of quantifying the volume of expectorated blood, others have proposed the term life-threatening hemoptysis to indicate hemoptysis accompanied by measurable parameters, such as abnormal gas exchange and hemodynamic instability, for patients in need of urgent resuscitation and treatment 3. A study of 762,325 patients in a primary care settings evaluated the incidence of hemoptysis as a presenting symptom in the outpatient setting 4. Massive hemoptysis accounts for a minority of cases (5% to 15%) 3.
The outlook depends on what is causing the problem. Most people do well with treatment to treat the symptoms and the underlying disease. People with severe hemoptysis may die.
The most common reasons for coughing up blood are:
- a prolonged, severe cough
- pneumonia or other lung infection – this is more likely if your sputum is discolored or contains pus, you have a fever, or you have a tight feeling in your chest
- bronchitis – an infection of the bronchii (the large tubes going down to your lungs)
- bronchiectasis (a disease where the large airways in your lungs are damaged ) – this is more likely if you’re also wheezy or short of breath
Less common causes of coughing up blood:
- pulmonary embolism (a blood clot in the arteries that supply blood to your lungs) – this usually causes sudden shortness of breath and chest pain
- pulmonary edema (fluid in the lungs due to a heart condition) – your sputum will be pink and frothy, and this usually occurs in people with pre-existing heart problems
- lung cancer – this is more likely if you’re over 40 and smoke
- tuberculosis (TB) – a severe lung infection associated with fever and sweating; this is becoming more common in the US, but can be treated with prolonged antibiotics
- cancer of the throat or windpipe
- taking anticoagulants (blood-thinning medications) – medications that help stop your blood clotting, such as warfarin, rivaroxaban, or dabigatran
- having something stuck in your airway
Sometimes, no cause can be found – even after investigation and it never happens again.
Sometimes a severe nosebleed or bleeding from the mouth or throat can cause blood to come out in your saliva when you cough.
Call your doctor as soon as possible if you cough up blood, even if it’s just a few spots or specks.
Your doctor will check if you might have a serious medical condition that needs to be investigated and treated.
Get medical help right away if you cough up blood and have:
- A cough that produces more than a few teaspoons of blood
- Blood in your urine or stools
- Chest pain
- Dizziness
- Fever
- Lightheadedness
- Severe shortness of breath
Call for an ambulance or go to your nearest accident and emergency (A&E) department immediately if you’re coughing up a lot of blood or are struggling to breathe.
Hemoptysis causes
In outpatient primary care, acute respiratory tract infections, asthma, chronic obstructive pulmonary disease (COPD), cancer and bronchiectasis are the most common diagnoses in patients with hemoptysis 4. In comparison, a study of patients with hemoptysis in a hospital setting showed that bronchiectasis, lung cancer, bronchitis, and pneumonia account for more than 70% of inpatient diagnoses 4. A likely explanation for the difference is that bronchiectasis and lung cancer are more likely to produce massive hemoptysis and lead to hospitalization 5.
The likelihood of tuberculosis infection associated with hemoptysis varies throughout the world. Tuberculosis accounts for 7% to 85% of cases of massive hemoptysis, with the lowest incidence in the United States and highest incidence in South Africa 3. Pulmonary tuberculosis should be suspected in patients with respiratory symptoms and possible tuberculosis exposure, younger age, weight loss, and radiographic findings of cavitation, upper lobe infiltrates, or miliary pattern 6. Approximately 6% to 7% of tuberculosis cases in the United States occur in homeless persons 7 and the rate of tuberculosis in persons born outside the United States is 12 times that of U.S.-born persons 8. Uncommon but well-known causes of hemoptysis include pulmonary embolism, pulmonary endometriosis, Goodpasture syndrome, and foreign body aspiration.
A number of conditions, diseases, and medical tests may make you cough up blood. These include:
- Blood clot in the lung
- Breathing food or other material into the lungs (pulmonary aspiration)
- Bronchoscopy with biopsy
- Bronchiectasis
- Bronchitis
- Cancer
- Cystic fibrosis
- Inflammation of the blood vessels in the lung (vasculitis)
- Injury to the arteries of the lungs
- Irritation of the throat from violent coughing (small amounts of blood)
- Pneumonia or other lung infections
- Pulmonary edema
- Systemic lupus erythematosus
- Tuberculosis
- Very thin blood (from blood thinning medications, most often at higher than recommended levels)
Table 1. Causes of hemoptysis in Outpatient and Inpatient Settings
| Cause | Frequency (%) |
|---|---|
Outpatient (U.K. Primary Care Cohort) | |
Acute respiratory tract infection | 64 |
Asthma | 10 |
Chronic obstructive pulmonary disease | 8 |
Unknown | 8 |
Lung cancer | 6 |
Bronchiectasis | 2 |
Pulmonary embolism | 1 |
Tuberculosis | 0.4 |
Bleeding disorder | 0.3 |
Pulmonary edema | 0.2 |
Mitral valve stenosis | 0.1 |
Aspergillosis | 0.04 |
Inpatient (Israel Inpatient Cohort) | |
Bronchiectasis | 20 |
Lung cancer | 19 |
Bronchitis | 18 |
Pneumonia | 16 |
Unknown | 8 |
Congestive heart failure | 4 |
Hemorrhagic diathesis | 4 |
Tuberculosis | 1 |
Other | 10 |
Primary vascular source
- Arteriovenous malformation
- Pulmonary embolism
- Elevated pulmonary venous pressure
- Pulmonary artery rupture
Pseudohemoptysis
- Upper airway source
- Gastrointestinal source
- Serratia marcescens (gram-negative bacterium that produces a red pigment that may be mistaken for blood)
- Malingering
Pulmonary parenchymal source
- Tuberculosis
- Pneumonia
- Lung abscess
- Lung contusion
- Mycetoma (“fungus ball”)
- Idiopathic pulmonary hemosiderosis
- Wegener granulomatosis
- Lupus pneumonitis
- Goodpasture syndrome
Tracheobronchial source
- Bronchiectasis
- Neoplasm
- Bronchitis
- Broncholithiasis
- Airway trauma
- Foreign body
Miscellaneous and rare causes
- Systemic coagulopathy or thrombolytic agents
- Catamenial hemoptysis (pulmonary endometriosis)
Table 2. Differentiating Features of Pseudohemoptysis
| Cause | Historical findings | Physical examination findings | Confirmatory test or procedure |
|---|---|---|---|
Serratia marcescens (gram-negative bacterium that produces a red pigment that may be mistaken for blood) | Previous hospitalization, use of broad-spectrum antibiotics, mechanical ventilation | Normal | No red blood cells in sputum; positive culture |
Upper gastrointestinal tract source | Coffee ground appearance (not bubbly or frothy), darker blood, nausea, vomiting, gastrointestinal disease | Epigastric tenderness, signs of chronic liver disease (e.g., palmar erythema, spider angiomas, ascites, peripheral edema) | Acidic blood pH, blood mixed with food particles, blood in nasogastric aspiration, esophagogastro-duodenoscopy, barium swallow |
Upper respiratory tract source | Bleeding gums, epistaxis, little or no cough | Gingivitis; telangiectasias; ulceration; varices of the tongue, nose, nasopharynx, oropharynx, or hypopharynx | Nasopharyngoscopy if etiology is not apparent |
Table 3. Historical Findings That Suggest Cause of Hemoptysis
| Finding | Suggested cause |
|---|---|
Anticoagulant use | Coagulopathy |
Cough | Bronchiectasis, COPD, foreign body, pneumonia, tuberculosis |
Fever | Bronchitis, lung abscess, neoplasm, pneumonia, pulmonary embolism, tuberculosis |
Heart disease (valvular or congestive heart failure) | Congestive heart failure |
Immunosuppression | Bronchitis, lung abscess, pneumonia, tuberculosis |
Recent surgery or immobilization | Pulmonary embolism |
Smoking | Bronchitis, COPD, neoplasia |
Sputum production | Bronchiectasis, COPD, pneumonia, tuberculosis |
Trauma | Airway trauma, pulmonary embolism |
Weight loss | COPD, neoplasia, tuberculosis |
Abbreviation: COPD = chronic obstructive pulmonary disease
[Source 5 ]Hemoptysis diagnosis
Haemoptysis is managed according to the amount and rate of bleeding and how sick you are. If your condition is life threatening, you may need to receive urgent treatment to stabilize it before any investigations are done. In an emergency, your doctor will give you treatments to control your condition.
To find out the cause of your coughing up blood, your doctor will likely ask you questions about your cough.
Your doctor will then ask you questions about your cough, such as:
- How much blood are you coughing up? Are you coughing up large amounts of blood at a time?
- Do you have blood-streaked mucus (phlegm)?
- How many times have you coughed up blood and how often does it happen?
- How long have you been coughing up blood for? Is it worse at some times such as at night?
- What other symptoms do you have?
You will probably be asked about your past and current medication and conditions, and whether you smoke.
Your doctor will check you for any signs of diseases that can cause you to cough up blood. They may take your temperature to check for an infection and look up your nose to make sure the bleeding is not from there.
Depending on your condition, you may be asked to have a chest X-ray or CT scan to detect any problems. You may also be asked to have a bronchoscopy, which is a procedure to see the inside of your airways and lungs.
If a blood clot in your lung is suspected, you may need a lung ventilation-perfusion scan, which looks at air flow and blood flow in the lungs.
Other tests that may be done include blood tests and a test to look for infection-causing bacteria in your saliva.
Your doctor will do a complete physical exam and check your chest and lungs. Tests that may be done include:
- Bronchoscopy, a test to view the airways
- Chest CT scan (computed tomography)
- Chest x-ray
- Complete blood count
- Lung biopsy
- Lung scan
- Pulmonary arteriography
- Sputum culture and smear
- Test to see if the blood clots normally, such as PT or PTT
Diagnostic strategy
Figure 1 and 2 outline a recommended approach to the evaluation and management of nonmassive hemoptysis 10. Chest radiography is typically recommended for all patients with hemoptysis, whereas chest computed tomography (CT) or bronchoscopy should be reserved for patients with abnormal radiographic findings, recurrent hemoptysis, or risk factors for cancer. These recommendations are consistent with criteria from the American College of Radiology 10.
American College of Radiology Appropriateness Criteria for Imaging in Patients with Hemoptysis
- Initial evaluation of patients with hemoptysis should include chest radiography
- In patients at high risk of malignancy with normal findings on chest radiography, CT, and bronchoscopy:
- Observation for three years may be considered
- Radiography and CT should be performed at follow-up based on the patient’s risk factors
- Bronchoscopy may be performed in addition to imaging during the observation period
- CT should be used for initial evaluation in patients at high risk of malignancy or with suspicious findings on chest radiography
- CT should be considered in current or former smokers who have normal findings on chest radiography
- Massive hemoptysis can be treated with surgery or percutaneous embolization; multidetector CT before embolization or surgery can define the source of hemoptysis; percutaneous embolization may be used initially to halt the hemorrhage before definitive surgery
Figure 1. Mild hemoptysis diagnostic algorithm
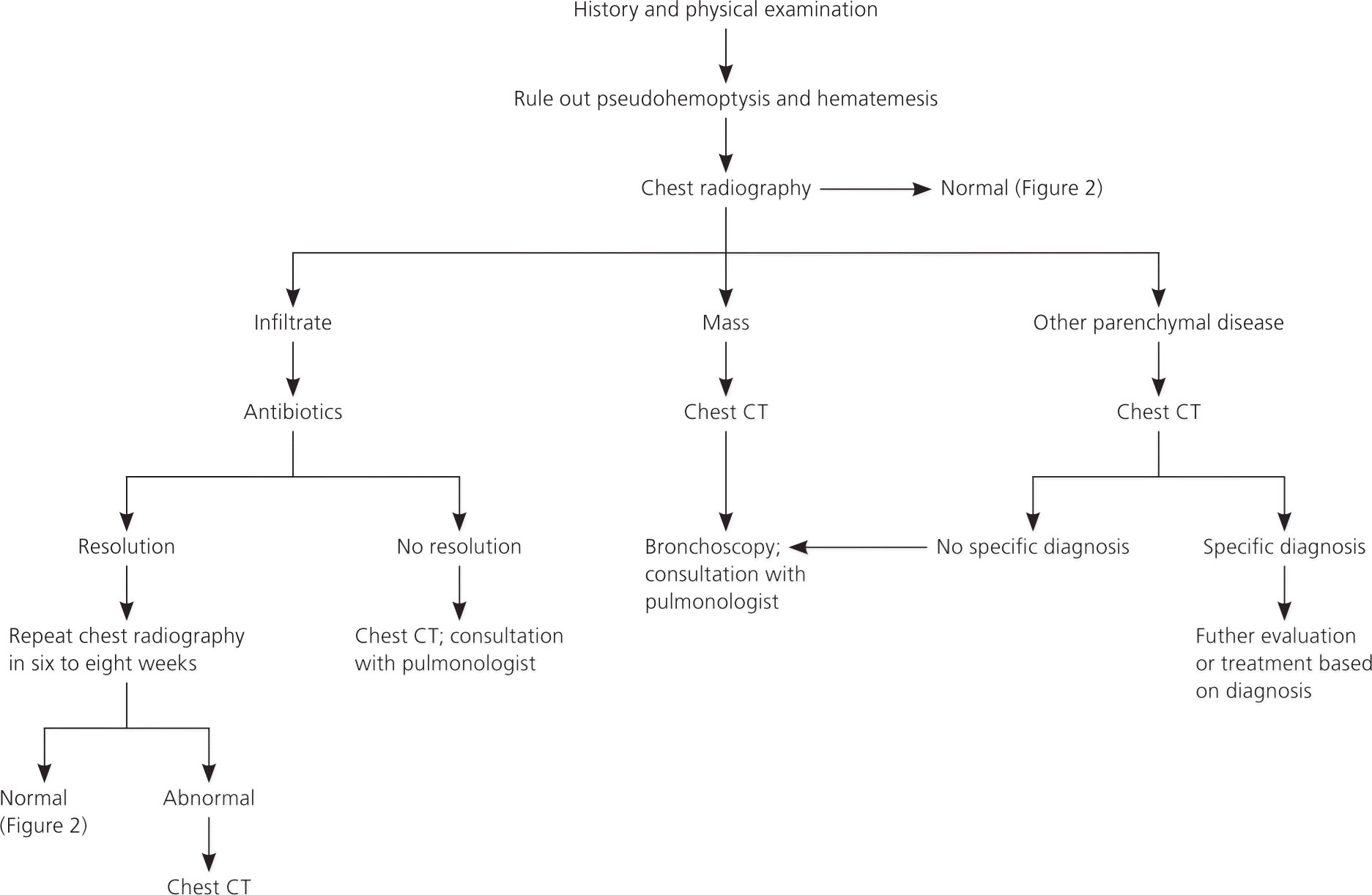
Figure 2. Algorithm for the management of mild hemoptysis in patients with normal findings on chest radiography

Hemoptysis treatment
The type of treatment you may receive will depend on the cause of your coughing up blood. For example, if a bacterial infection is the cause, you will probably be treated with antibiotics.
In severe hemoptysis, you may need a surgical procedure to stop the bleeding even before the cause is found.
For patients with massive hemoptysis, consultation with a pulmonologist and admission to the intensive care unit are usually warranted 11. Resuscitation focusing on the airway, breathing, and circulation should be performed before diagnostic testing. Table 4 outlines suggested initial studies in the evaluation of patients with massive hemoptysis.
Chest radiography may provide clues about the etiology, as well as guide further resuscitation and evaluation. Once the bleeding site has been determined, the patient should be placed in the lateral decubitus position with the affected lung down to prevent pooling of blood in the unaffected bronchial system. Rapid bleeding warrants immediate airway control with rigid bronchoscopy or endotracheal intubation 3. Flexible bronchoscopy is less effective in maintaining a patent airway, but can provide useful diagnostic information. For stable patients with no identifiable lesion on chest radiography or bronchoscopy, chest CT angiography and/or bronchial artery arteriography with or without embolization should be performed to guide treatment. Bronchial artery arteriography is usually reserved for cases in which embolization is planned, and is often performed after CT angiography, which aids in localization of bleeding 3.
Table 4. Suggested Initial Tests in Patients with Massive Hemoptysis
| Test | Indications |
|---|---|
Blood typing and cross-match | For patients with hemodynamic instability from blood loss or those in whom a complete blood count reveals anemia that warrants transfusion |
Chest radiography | For all patients with hemoptysis; may help localize bleeding and identify etiology; provides images for later comparison to evaluate resolution of disease |
Coagulation studies | Reasonable to obtain in patients with a history of coagulopathy or current anticoagulant use |
Complete blood count | Reasonable to obtain in all patients with hemoptysis to rule out thrombocytopenia and to evaluate for anemia and/or microcytosis indicative of chronic blood loss or malignancy |
Renal function testing | Should be obtained before imaging with contrast media and in patients with suspected vasculitis |
Sputum testing (Gram stain, acid-fast bacilli smear, fungal cultures, cytology) | Should be obtained if massive hemoptysis or an infectious etiology is suspected |
Indications for Admission to the Intensive Care Unit or Referral to Specialty Center in Patients with Hemoptysis
- Cause of coughing up blood with high risk of bleeding (e.g., aspergillosis, lesions with pulmonary artery involvement)
- Gas-exchange abnormalities (respiratory rate > 30 breaths per minute, oxygen saturation < 88% in room air, or need for high-flow oxygen [> 8 L per minute] or mechanical ventilation)
- Hemodynamic instability (hemoglobin < 8 g per dL [80 g per L] or a decrease of more than 2 g per dL [20 g per L] from baseline, consumptive coagulopathy, or hypotension requiring fluid bolus or vasopressors)
- Massive hemoptysis (> 200 mL per 48 hours or > 50 mL per episode in patients with chronic pulmonary disease)
- Respiratory comorbidities (e.g., previous pneumonectomy, chronic obstructive pulmonary disease, cystic fibrosis)
- Other comorbidities (e.g., ischemic heart disease, need for anticoagulation)
Table 5. Predictors of In-Hospital Mortality in Patients with Hemoptysis
Chest radiography on admission shows involvement of two or more quadrants (1 point) | ||||||||
Chronic alcoholism (1 point) | ||||||||
Pulmonary artery involvement (1 point) | ||||||||
Aspergillosis (2 points) | ||||||||
Malignancy (2 points) | ||||||||
Mechanical ventilation required (2 points) | ||||||||
Score | 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
Mortality | 1% | 2% | 6% | 16% | 34% | 58% | 79% | 91% |
Footnote: Patients with a score greater than 2 should be admitted to the intensive care unit, and those with a score greater than 5 may require urgent interventional radiology.
[Source 12 ] References- Weinberger SE, Lipson DA. Cough and hemoptysis. In: Fauci AS, Braunwald E, Kasper DL, et al., eds. Harrison’s Principles of Internal Medicine. 17th ed. New York, NY: McGraw-Hill; 2008:225–228.
- Bidwell JL, Pachner RW. Hemoptysis: diagnosis and management. Am Fam Physician. 2005;72(7):1253–1260.
- Sakr L, Dutau H. Massive hemoptysis: an update on the role of bronchoscopy in diagnosis and management. Respiration. 2010;80(1):38–58.
- Jones R, Charlton J, Latinovic R, Gulliford MC. Alarm symptoms and identification of non-cancer diagnoses in primary care: cohort study. BMJ. 2009;339:b3094.
- Hemoptysis: Evaluation and Management. Am Fam Physician. 2015 Feb 15;91(4):243-249. https://www.aafp.org/afp/2015/0215/p243.html
- Solari L, Acuna-Villaorduna C, Soto A, et al. A clinical prediction rule for pulmonary tuberculosis in emergency departments. Int J Tuberc Lung Dis. 2008;12(6):619–624.
- Haddad MB, Wilson TW, Ijaz K, Marks SM, Moore M. Tuberculosis and homelessness in the United States, 1994–2003. JAMA. 2005;293(22):2762–2766.
- Centers for Disease Control and Prevention. Trends in tuberculosis—United States, 2011. MMWR Morb Mortal Wkly Rep. 2012;61(11):181–185.
- Hirshberg B, Biran I, Glazer M, Kramer MR. Hemoptysis: etiology, evaluation, and outcome in a tertiary referral hospital. Chest. 1997;112(2):440–444.
- Ketai LH, Mohammed TL, Kirsch J, et al.; Expert Panel on Thoracic Imaging. ACR appropriateness criteria hemoptysis. J Thorac Imaging. 2014;29(3):W19–W22.
- Ibrahim WH. Massive haemoptysis: the definition should be revised. Eur Respir J. 2008;32(4):1131–1132.
- Fartoukh M, Khoshnood B, Parrot A, et al. Early prediction of in-hospital mortality of patients with hemoptysis: an approach to defining severe hemoptysis. Respiration. 2012;83(2):111.





{kind=link}