
What is Hepatitis E
Hepatitis E is a liver infection caused by the Hepatitis E virus (HEV): a small virus, with a positive-sense, single-stranded ribonucleic acid (RNA) genome that is approximately 27 to 34 nm in diameter 1, 2. Hepatitis E virus (HEV) is unique, in that it has a different clinical and epidemiologic profile depending on where the infection is acquired 3. This can be attributed largely to the viral genotypes circulating in different parts of the world (Table 1). Four genotypes of hepatitis E virus (genotypes 1, 2, 3 and 4) cause illness in humans, each displaying different epidemiologic and clinical characteristics in developing and developed countries (see Table 1). Genotype 1 and 2 are found only in humans are transmitted through the fecal-oral route from contaminated water (the most common source of hepatitis E virus infection) and are found mainly in developing countries in Africa, Asia, Central America and the Middle East 4. Genotype 3 and 4 hepatitis E viruses circulate in several animals (including pigs, wild boars, and deer) without causing any disease, and occasionally infect humans. Genotype 3 and 4 are mainly found in animals (zoonitics) are transmitted to humans by eating undercooked meat such as pork and deer and are mainly found in developed countries such as the United States, Australia, Japan and China 5. Consumption of shellfish was a risk factor in a recently described outbreak that occurred among cruise ship passengers 6. Hepatitis E virus genotype 4, detected in China, Taiwan, and Japan, has also been associated with foodborne transmission 7. Recently, a new genotype (genotype 7) was identified in a liver-transplant recipient from UAE with chronic hepatitis E virus infection who frequently consumed camel meat and milk 8.
According to the World Health Organization (WHO), Hepatitis E virus causes about 20 million new infections and over 55,000 deaths annually 9. Hepatitis E typically causes acute, or short-term, infection. In most cases, hepatitis E is a short-term infection as people’s bodies are able to recover and fight off the infection and the virus goes away. People usually get better without treatment after several weeks. However, acute infection can become chronic in rare cases, primarily in people who have received solid-organ transplants 10.
While rare in the United States, Hepatitis E is common in many parts of the world. It is transmitted from ingestion of fecal matter, even in microscopic amounts, and is usually associated with contaminated water supply in countries with poor sanitation. There is currently no FDA-approved vaccine for Hepatitis E, however, in 2012 a recombinant vaccine was approved for use in China 3.
Cases of hepatitis E typically present in one of two ways: either as large outbreaks and sporadic cases in areas where hepatitis E virus (HEV) is endemic (genotype 1 in Asia and Africa, genotype 2 in Mexico and west Africa, and genotype 4 in Taiwan and China) or as isolated cases in developed countries like the United States (genotype 3). Recently, a new genotype (genotype 7) was identified in a liver-transplant recipient from UAE with chronic hepatitis E virus infection who frequently consumed camel meat and milk 8.
Hepatitis E virus Genotypes 1 and 2 are usually seen in young adults (15-40) as part of outbreaks, causing acute infection that is self-limited and does not progress to chronic infection. However, acute infections in pregnant patients or patients with chronic liver disease can be severe with progression to fulminant liver failure 5. Hepatitis E virus Genotype 3 and 4 usually cause sporadic cases and are mainly see in older adults (older than 40). They can cause acute infections with a possibiltiy of progression to chronic infections mainly in immunocompromised patients such as solid organ transplant patients on immunosupprasants and HIV patients with AIDS 5.
Table 1. Hepatitis E genotypes and geographic locations
| Characteristics | Genotype 1 | Genotype 2 | Genotype 3 | Genotype 4 |
| Geographic Location | Africa and Asia | Mexico, West Africa | Developed Countries | China, Taiwan, Japan |
| Transmission route | Waterborne fecal- oral person-to-person | Waterborne fecal-oral | Food-borne | Food-borne |
| Groups at high risk for infection | Young Adults | Young Adults | Older Adults (>40 years) and males, immuno-compromised persons | Young Adults |
| Zoonotic transmission | No | No | Yes | Yes |
| Chronic Infection | No | No | Yes | No |
| Occurrence of Outbreaks | Common | Smaller scale outbreaks | Uncommon | Uncommon |
Hepatitis E Key facts 1:
- Hepatitis E is a liver disease caused by infection with a virus known as hepatitis E virus (HEV).
- Every year, there are an estimated 20 million hepatitis E virus (HEV) infections worldwide, leading to an estimated 3.3 million symptomatic cases of hepatitis E 11.
- The World Health Organization (WHO) estimates that hepatitis E caused approximately 44 000 deaths in 2015 (accounting for 3.3% of the mortality due to viral hepatitis).
- The virus is transmitted via the faecal-oral route, principally via contaminated water.
- Hepatitis E is found worldwide, but the prevalence is highest in East and South Asia.
- A vaccine to prevent hepatitis E virus infection has been developed (2011) and is licensed in China, but is not yet available elsewhere.
Hepatitis E typically causes acute, or short-term, infection. People usually get better without treatment after several weeks.
What is Acute hepatitis E infection?
Acute hepatitis E is a short-term infection. In most cases, people’s bodies are able to recover and fight off the infection and the virus goes away. People usually get better without treatment after several weeks.
Can Hepatitis E become chronic?
To date, there is no report of progression of acute hepatitis E to chronic Hepatitis E in developing countries where hepatitis E virus (HEV) genotypes 1 and 2 are the predominant causes of illness. However, more and more cases of Hepatitis E with progression to chronic hepatitis and chronic liver disease are being reported among hepatitis E virus (HEV) genotype 3 cases acquired in the developed countries. These chronic cases are exclusively among persons who are on immunosuppressive treatment for solid organ transplant.
What is Chronic hepatitis E?
Chronic hepatitis E is a long-lasting infection that occurs when your body isn’t able to fight off the virus and the virus does not go away. Chronic hepatitis E is rare and only occurs in people with weakened immune systems. For example, hepatitis E may become chronic in people taking medicines that weaken their immune system after an organ transplant, or in people who have HIV or AIDS.
How serious is hepatitis E?
Most people with Hepatitis E recover completely. During hepatitis E virus outbreaks, the overall case-fatality rate is about 1% 12.
The types of hepatitis E that are common in developing countries are likely to cause severe infections, especially in pregnant women.
For pregnant women, Hepatitis E can be a serious illness with mortality reaching 10%–30% in their third trimester of pregnancy 13. Hepatitis E could also be serious among persons with preexisting chronic liver disease resulting in decompensated liver disease and death. Similarly high mortality occurs solid organ transplant recipients on immunosuppressive therapy.
The types of hepatitis E that are common in developed countries are often mild and cause no symptoms. Many people don’t know they’ve had these types of hepatitis E 3.
Can animals spread the hepatitis E virus to humans?
Yes. Hepatitis E can infect certain mammals, and consumption of uncooked or undercooked meat or organs from infected animals can lead to foodborne transmission to humans. hepatitis E virus RNA (genotypes 3 and 4) has been extracted from pork, boar, and deer meat 14.
How soon after exposure will symptoms appear?
When symptoms occur, they usually develop 15–60 days (mean: 40 days) after exposure 3.
Who should be tested for hepatitis E?
Hepatitis E virus infection should be considered in any person with symptoms of viral hepatitis who tests negative for serologic markers of hepatitis A, hepatitis B, hepatitis C, other hepatotropic viruses, and all other causes of acute liver injury. Any symptomatic person who has traveled either to or from an hepatitis E-endemic area or outbreak-afflicted region should also be evaluated for hepatitis E virus infection. A detailed history regarding travel, sources of drinking water, uncooked food, and contact with jaundiced persons should be obtained from these patients to aid in diagnosis. Because domestically acquired cases of hepatitis E are occurring in the United States, hepatitis E virus infection also should be considered in any person with unexplained symptoms of liver injury, regardless of travel history.
How common is Hepatitis E in the United States?
Hepatitis E is believed to be uncommon in the United States 15. However, some studies have found a high prevalence of antibodies to hepatitis E virus (HEV) in the general population. When symptomatic hepatitis E does occur, it is usually the result of travel to a developing country where hepatitis E is endemic. Increasingly, sporadic Hepatitis E cases not associated with travel have been identified in developed countries. No clear exposure was identified for these domestically acquired (non-travel related) cases 16. Sporadic cases of hepatitis E in developed countries, including the United States, are primarily caused by HEV genotype 3 and largely affect older men (those >40 years of age).
Where is Hepatitis E most common?
Hepatitis E virus infection has a global distribution; however, it is most common in the developing countries, where sanitation is poor and access to clean water is limited. Hepatitis E epidemics involving large numbers of people have been reported in Asia, the Middle East, Africa, and Central America 17. Hepatitis E virus (HEV) is the second most common cause of sporadic hepatitis in North Africa and the Middle East 18. People living in crowded camps or temporary housing, including refugees and people who are internally displaced, are at particularly high risk. Sporadic cases have been described in western countries and have mostly been limited to visitors who have traveled to hepatitis E virus endemic areas 19. The overall seroprevalence of hepatitis E virus in the US was estimated at 6% between 2009 and 2010. Although experts used to think hepatitis E was rare in the United States, recent research suggests that about 20 percent of the population has had hepatitis E 20. The risk of hepatitis E virus seropositivity is related to increasing age, birth outside of the United States, Hispanic race, and consumption of meat (> 10 times/month) 21. Although hepatitis E virus was previously thought to be prevalent only in the developing countries of Asia and Africa, more recently it has been found to be a zoonotic disease prevalent in high-income countries of Europe where it is acquired from pigs 22.
Hepatitis E infection is found worldwide. Two different patterns are observed, where hepatitis E is found in:
- resource-poor areas with frequent water contamination; and
- areas with safe drinking water supplies.
Hepatitis E is common in resource-limited countries with limited access to essential water, sanitation, hygiene and health services. In these areas, the disease occurs both as outbreaks and as sporadic cases. The outbreaks usually follow periods of fecal contamination of drinking water supplies and may affect several hundred to several thousand persons. Some of these outbreaks have occurred in areas of conflict and humanitarian emergencies, such as war zones, and in camps for refugees or internally displaced populations, situations where sanitation and safe water supply pose special challenges.
Sporadic cases are also believed to be related to contamination of water or food, albeit at a smaller scale. The cases in these areas are caused mostly by infection with genotype 1 virus, and much less frequently by genotype 2 virus.
In areas with better sanitation and water supply, hepatitis E disease is infrequent with only occasional sporadic cases. Most of these cases are caused by genotype 3 virus, and are caused by infection with virus originating in animals, usually through ingestion of undercooked animal meat (including animal liver) and are not related to contamination of water or other foods.
Serological evidence of prior exposure to the virus has been found in most areas, with higher seroprevalence rates [proportion of people who test positive for IgG antibodies to hepatitis E virus (HEV)] in regions with lower standards of sanitation and thus higher risk for transmission. However, presence of these antibodies does not imply presence of or increased risk of disease. The usefulness of such data for epidemiological purposes may also be limited due to variable and possible sub-optimal performance of available serological assays, and possible disappearance of the antibody with the passage of time among those exposed to the virus.
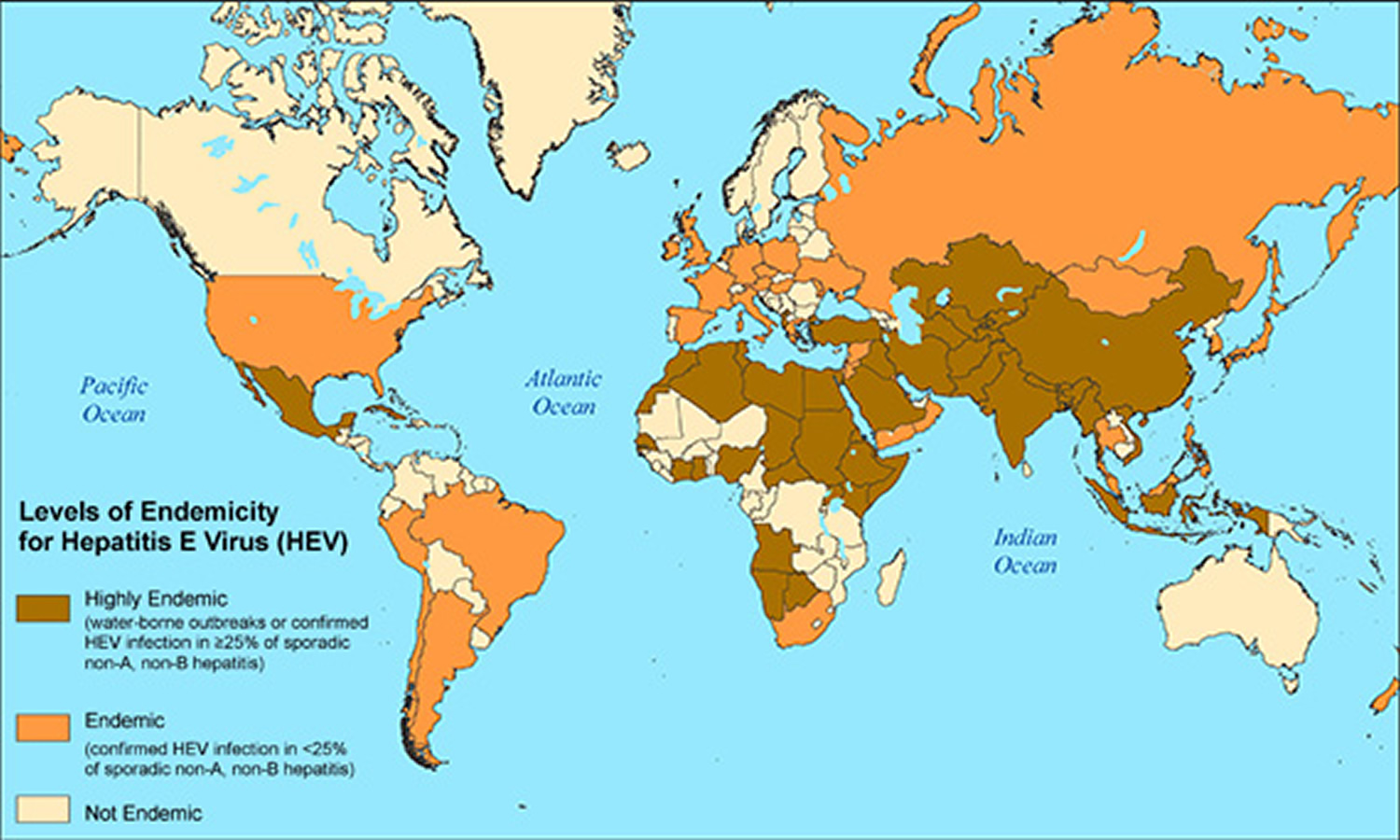
Figure 1. Hepatitis E worldwide locations
How is the hepatitis E virus spread?
Hepatitis E virus is usually spread by the fecal-oral route. In developing countries, where hepatitis E virus genotypes 1 and 2 predominate, the most common source of hepatitis E virus infection is contaminated drinking water. In developed countries, sporadic cases of hepatitis E virus genotype 3 have occurred following consumption of uncooked/undercooked pork or deer meat. Consumption of shellfish was a risk factor in a recently described outbreak that occurred among cruise ship passengers 6. Hepatitis E virus genotype 4, detected in China, Taiwan, and Japan, has also been associated with foodborne transmission 7.
What causes hepatitis E?
The hepatitis E virus causes hepatitis E. In developing countries, hepatitis E typically spreads through drinking contaminated water. In developed countries, such as the United States, hepatitis E typically spreads from animals to people, when people eat undercooked pork or wild game, such as deer. Person-to-person transmission is rare. Research suggests that hepatitis E can also spread through blood transfusion, particularly in endemic areas, but this is very rare 23. Hepatitis E virus (HEV) can also be transmitted vertically from infected mothers to their infants (also known as vertical transmission) and can result in significant perinatal mortality and fetal loss 24. There is insufficient data regarding transmission of hepatitis E virus via breast milk; however, hepatitis E virus has been isolated in breast milk, and serum titers were noted to be comparable 25.
The incubation period of hepatitis E virus infection ranges from 28 to 40 days 4. After ingestion of hepatitis E virus, the virus is absorbed through the gastrointestinal mucosa into the portal circulation to reach the liver. Hepatitis E virus (HEV) replication has not been observed in tissues other than the liver. Hepatitis E virus can produce morphologic changes in the liver that resemble both cholestatic and classic acute hepatitis, but these features are not diagnostic for hepatitis E 26. Hepatitis E virus is excreted in feces.
How do you get Hepatitis E?
The hepatitis E virus is transmitted mainly through the fecal-oral route due to fecal contamination of drinking water. The virus is shed in the stools of infected persons, and enters the human body through the intestine. It is transmitted mainly through contaminated drinking water. This route accounts for a very large proportion of clinical cases with hepatitis E disease. Usually hepatitis E infection is self-limiting and resolves within 2–6 weeks. Occasionally a serious disease, known as fulminant hepatitis (acute liver failure) develops, and a proportion of people with hepatitis E can die.
- Some types are spread by drinking contaminated water. These types are more common in developing countries, including parts of Africa, Asia, Central America, and the Middle East 27.
- Other types are spread by eating under cooked pork or wild game, such as deer. These types are more common in developed countries, such as the United States, Australia, Japan, and parts of Europe and East Asia 27. The ingestion of raw or uncooked shellfish may be the source of sporadic cases in endemic areas.
- Other routes of transmission have been identified, but appear to account for a much smaller number of clinical cases:
- transfusion of infected blood products; and
- vertical transmission from a pregnant woman to her fetus.
The risk factors for hepatitis E are related to poor sanitation, allowing virus excreted in the faeces of infected people to reach drinking water supplies.
Who is more likely to get hepatitis E?
Different types of hepatitis E are more likely to affect different groups of people. The types of hepatitis E that are more common in developing countries are more likely to affect adolescents and young adults 28.
In contrast, the types of hepatitis E that are more common in developed countries most often affect older men 28.
How can I protect myself from hepatitis E infection?
When traveling in a developing country, drink bottled water. Use bottled water to brush your teeth, make ice cubes, and wash fruits and vegetables.
Also, make sure any pork or deer you eat is thoroughly cooked, both in developing countries and in developed countries such as the United States.
How can I prevent spreading hepatitis E to others?
Research suggests that it is uncommon for people to spread hepatitis E directly to other people. If you have hepatitis E, you can reduce your chance of spreading the infection by washing your hands with warm, soapy water after using the toilet and before preparing food. Talk with a blood donation center before you donate blood.
Is a hepatitis E vaccine available?
No vaccine for hepatitis E is available in the United States. Vaccines have been developed and are used in China 1.
Hepatitis E virus infection and Pregnancy
Hepatitis E virus infection during pregnancy can result in poor prognosis 29 and vertical transmission (i.e. transmission directly from the mother to an embryo, fetus, or baby during pregnancy or childbirth). Unlike hepatitis B virus and hepatitis C virus, which normally do not cause death cases in acute infection of pregnant women 30, hepatitis E virus infection by genotype 1 strains in pregnant women results in up to 30% case fatality, while infection by hepatitis E virus genotype 3 strains is usually subclinical 31.
Early antiviral response is critical for the host to control virus infection. In pregnant women with acute infection of genotype 1 hepatitis E virus, the expression of TLR3, 7, and 9 in monocytes and macrophages is upregulated 32. But when acute liver failure develops, their expression is reduced, which may account for the defective immune response in acute liver failure patients 33. Also, the interferon (IFN) response in placental cells is reported to be weaker than hepatocytes for genotype 1 but not genotype 3 hepatitis E virus 34. These data suggest that genotype 1 hepatitis E virus might be able to evade the early antiviral response in a certain population of pregnant women and cause an adverse consequence 32.
Genotype 1 hepatitis E virus infection might interfere with adaptive immunity in some subjects. One study shows that in the second and third trimester of pregnancy, hepatitis E virus-infected pregnant women with fulminant hepatic failure have lower CD4+ T cell counts and higher CD8+ T cell counts than hepatitis E virus-negative women with fulminant hepatic failure 35. Other studies show a significant infiltration of activated CD8+ T cells containing granzymes in liver biopsies from hepatitis E virus-infected patients with fulminant hepatic failure, which suggests the role of CD8+ T cells in the liver injury 36. Clinical investigation in hepatitis E virus-infected women with acute liver failure revealed that the cytokine level, such as TNF-α, IL-6, and IFN-γ, is higher than in non-infected pregnant women, and the level of these cytokines are positively correlated to adverse pregnancy outcome 37. These data suggest that genotype 1 hepatitis E virus induces an overactive inflammatory response leading to a poor prognosis in a certain population of pregnant women.
The genotype 1 hepatitis E virus is also implicated in invading the placenta more effectively than genotype 3 32. A recent study demonstrates that the genotype 1 hepatitis E virus grows much more dynamically than genotype 3 hepatitis E virus in the ex-vivo maternal-fetal interface model using the decidua basalis and fetal placenta 38. Genotype 1 hepatitis E virus induces a higher level of apoptosis of decidua and placenta cells than genotype 3 hepatitis E virus and provokes a higher level of IL-6, CCL-3, and CCL-4, which positively correlates with the viral load. Meanwhile, UV-treated culture supernatant harvested from genotype 1 hepatitis E virus-infected explants causes more tissue injury in fresh decidua and placenta organ culture than the genotype 3 hepatitis E virus-infected cultures 38. Further studies are needed to compare the genetic characteristics of genotype 1 and 3, and identify the key factors in genotype 1 infection that determine severe disease outcome.
In addition to immunological factors, hormone variation during pregnancy may contribute to viral replication. Pregnant women with acute hepatitis E virus hepatitis have increased estrogen and progesterone level 35. These hormones are known to dampen the cell-mediated immune response 39.
Similarly, the estradiol level in hepatitis E virus-infected pregnant women during the third trimester is significantly higher than hepatitis E virus-negative pregnant women. An in vitro experiment shows that the estradiol treatment facilitates hepatitis E virus replication in A549 cells 40. Thus, the variation in hormone level is also speculated to be one of the factors that contribute to the severe disease progress of hepatitis E virus-infected pregnant women.
Collectively, the immune-tolerant environment may subject pregnant women to become more vulnerable to hepatitis E virus infection. hepatitis E virus infection with genotype 1 might dysregulate the balance maintaining the maternal-fetal tolerance and effective immunity, or alter the immunological mechanisms that maintain the balance, which leads to the dire consequence of fulminant hepatic failure in pregnant women 32. The potential mechanisms that genotype 1 hepatitis E virus employs to produce the mortality of pregnant women need to be investigated. Why infection of different genotypes results in different disease outcomes and what determines the chronicity of hepatitis E virus infection remain unclear 32. Both virus and host factors possibly contribute to the disease’s progress. In terms of the viral factors, genetic variations of the different genotypes and host adaptability may account for the different outcomes. Conversely, the immune-tolerant environment and associated factors that may be better exploited by genotype 1 hepatitis E virus in a certain vulnerable population might contribute to the development of acute liver failure in infected pregnant women. So far, most fatality cases of hepatitis E virus infection during pregnancy are found in South Asia 32. Due to the different geographical environments and food habits, the gut microbiota in South Asia might vary from other areas and might be a risk factor for acute liver failure development in hepatitis E virus-infected pregnant women. Further research on this front is needed to address this speculation.
Prevention of Hepatitis E
Prevention is the most effective approach against the disease. Prevention of hepatitis E relies primarily on good sanitation and the availability of clean drinking water. Travelers to developing countries can reduce their risk for infection by not drinking unpurified water. Boiling and chlorination of water will inactivate hepatitis E virus. Avoiding raw pork and venison can reduce the risk of hepatitis E virus genotype 3 transmission. Immune globulin is not effective in preventing hepatitis E.
At the population level, transmission of hepatitis E virus and hepatitis E disease can be reduced by:
- maintaining quality standards for public water supplies;
- establishing proper disposal systems for human feces.
On an individual level, infection risk can be reduced by:
- maintaining hygienic practices such as hand-washing with safe water, particularly before handling food;
- avoiding consumption of water and/or ice of unknown purity; and
- adhering to World Health Organization (WHO) safe food practices.
Immune globulin is not effective in preventing Hepatitis E.
Hepatitis E Vaccine
In 2011, a recombinant subunit vaccine to prevent hepatitis E virus infection was registered in China. It has not yet been approved in other countries 1. No FDA-approved vaccine for Hepatitis E is currently available in the United States.
Hepatitis E Symptoms
The incubation period following exposure to the hepatitis E virus ranges from 2 to 10 weeks, with an average of 5–6 weeks. The infected persons are believed to excrete the virus beginning a few days before to around 3-4 weeks after the onset of disease.
Many people infected with hepatitis E have no symptoms. Some people have symptoms 15 to 60 days (mean: 40 days) after they become infected with the virus 41.
The ratio of symptomatic to asymptomatic infection ranges from 1:2 to 1:13.
Typical signs and symptoms of hepatitis include:
- feeling tired
- nausea and vomiting
- poor appetite (anorexia)
- pain over the liver, in the upper part of the abdomen
- a slightly enlarged, tender liver (hepatomegaly).
- itching (without skin lesions), skin rash, or joint pain.
- darkening of the color of urine
- pale stools
- yellowish tint to the whites of the eyes and skin, called jaundice
People with hepatitis E typically get better without treatment after several weeks.
In areas with high disease endemicity, symptomatic infection is most common in young adults aged 15–40 years. In these areas, although infection does occur in children, they often have either no symptoms or only a mild illness without jaundice that goes undiagnosed.
These symptoms are often indistinguishable from those experienced during other liver illnesses and typically last between 1–6 weeks.
In rare cases, acute hepatitis E can be severe, and results in fulminant hepatitis (acute liver failure); these patients are at risk of death. Fulminant hepatitis occurs more frequently when hepatitis E occurs during pregnancy. Pregnant women with hepatitis E, particularly those in the second or third trimester, are at an increased risk of acute liver failure, fetal loss and mortality. Case fatality rates as high as 20–25% have been reported among pregnant women in their third trimester.
Cases of chronic hepatitis E infection have been reported in immunosuppressed people, particularly organ transplant recipients on immunosuppressive drugs, with genotype 3 or 4 hepatitis E virus infection.
Who is most likely to have symptomatic hepatitis E virus infection?
Symptomatic Hepatitis E in developing countries commonly occurs among older adolescents and young adults (aged 15–44 years). Pregnant women are more likely to experience severe illness including fulminant hepatitis and death.
In developed countries, sporadic cases due to hepatitis E virus genotype 3 mainly affect older men (>40 years of age). Acute and chronic hepatitis E virus infection occur in solid organ transplant recipients on immunosuppressant therapy.
How long does an hepatitis E virus (HEV)-infected person remain infectious?
The period of infectiousness has not been clearly determined, but virus excretion in stool has been demonstrated from one week prior to onset up to 30 days after the onset of jaundice. Chronically infected persons shed virus as long as infected.
Hepatitis E complications
Acute hepatitis E complications
Most people recover from acute hepatitis E without complications. In some cases, acute hepatitis E may cause acute liver failure, a condition in which the liver fails suddenly. Acute liver failure due to hepatitis E is more common in:
- pregnant women
- people who have other liver diseases
In pregnant women, hepatitis E can cause other complications for the mother and baby, such as stillbirth, premature birth or low birthweight.
Chronic hepatitis E complications
Chronic hepatitis E is rare and only occurs in people with weakened immune systems—may lead to complications such as cirrhosis or liver failure.
Hepatitis E diagnosis
Cases of hepatitis E are not clinically distinguishable from other types of acute viral hepatitis. Doctors diagnose hepatitis E based on symptoms and blood tests. A health care professional will take a blood sample from you and send the sample to a lab. Blood tests can detect antibodies to the hepatitis E virus and show whether you have hepatitis E. The virus can also be detected in blood and in stool samples taken during acute hepatitis E infection.
Laboratory diagnosis of hepatitis E virus infection is difficult due to the lack of standardized testing. Definitive diagnosis of hepatitis E infection is usually based on the detection of specific IgM antibodies to the virus in a person’s blood; this is usually adequate in areas where disease is common. Many commercial kits have been developed to test for anti-hepatitis E virus IgM and IgG, but the utility is limited as there are many false positives and negatives. In general, diagnosis of acute hepatitis E virus infection can be made with a positive serum hepatitis E virus IgM in the right clinical setting 42. Patients should also be tested for other viral hepatitis such as A, B, and C. Definitive diagnosis is made with the detection hepatitis E virus RNA in blood and/or stool by reverse transcriptase polymerase chain reaction (RT-PCR); this assay requires specialized laboratory facilities. This test is particularly needed in areas where hepatitis E is infrequent, and in cases with chronic hepatitis E virus infection. Because the viremia from hepatitis E virus can be relatively short-lived, especially in immunocompetent patients, a negative hepatitis E virus PCR does not exclude the possibility of recent hepatitis E virus infection 4. Serology may be more beneficial in these cases. The role of serological testing is, however, limited in immunocompromised individuals who may not mount an antibody response. PCR testing should be the cornerstone of diagnosis in this patient population 43. Diagnosis of chronic hepatitis E virus infection can be made by the persistent isolation of hepatitis E virus RNA in the serum or stool after 6 months of initial infection.
Both serologic and nucleic acid tests are commercially available, but they have not been approved by the U.S. Food and Drug Administration (FDA) for use in the United States. These tests are used for research purposes, but some commercial laboratories use commercially available assays from other countries.
In European countries, the 2018 European Association for the Study of the Liver (EASL) guidelines recommend both serology and NAT (nucleic acid amplification technique) for diagnosis of acute hepatitis E virus infection and NAT for diagnosis of chronic hepatitis E virus infection 22.
A test for viral antigen detection in serum has been developed; its place in the diagnosis of hepatitis E is currently being studied.
Treatment Hepatitis E virus (HEV) Infection
There is no specific treatment capable of altering the course of acute hepatitis E. As the disease is usually self-limiting, hospitalization is generally not required. Treatment for acute hepatitis E includes resting, drinking plenty of liquids, and eating healthy foods to help relieve symptoms.
Hospitalization is only required for people with fulminant hepatitis, however, and should also be considered for symptomatic pregnant women.
Talk with your doctor before taking any prescription or over-the-counter medicines, vitamins or other dietary supplements or complementary or alternative medicines—any of these could damage your liver. You should avoid alcohol until your doctor tells you that you have completely recovered from hepatitis E.
See your doctor regularly to make sure your body has fully recovered.
Doctors may treat chronic hepatitis E with ribavirin or peginterferon alfa-2a (Pegasys).
Immunosuppressed people with chronic hepatitis E benefit from treatment using ribavirin, an antiviral drug 43. In some specific situations, interferon has also been used successfully.
The role of antiviral therapy such as Ribavirin, for acute hepatitis E virus infection in immunocompromised patients is uncertain. Ribavirin should not be used in patients who are pregnant and have acute hepatitis E virus infection due to the risk of teratogenicity.
What should I eat and drink if I have hepatitis E?
If you have hepatitis E, you should eat a balanced, healthy diet. Talk with your doctor about healthy eating. You should also avoid alcohol because it can cause more liver damage.
Hepatitis E prognosis
Hepatitis E virus is typically a self-limited disease. Except for the rare occurrence of chronic hepatitis E in people with compromised immune systems, most people recover fully from the disease without any complications. Some patients, may develop acute complications such as acute hepatic failure, cholestatic jaundice, or chronic hepatitis E virus infection. Extrahepatic manifestations have been reported with Hepatitis E virus genotype 3 which mainly neurological including inflammatory polyradiculopathy, Guillain-Barre syndrome, peripheral neuropathy, encephalitis and ataxia 44.
- Hepatitis E. http://www.who.int/mediacentre/factsheets/fs280/en/[↩][↩][↩][↩]
- Yamashita, T., Mori, Y., Miyazaki, N., Cheng, R. H., Yoshimura, M., Unno, H., Shima, R., Moriishi, K., Tsukihara, T., Li, T. C., Takeda, N., Miyamura, T., & Matsuura, Y. (2009). Biological and immunological characteristics of hepatitis E virus-like particles based on the crystal structure. Proceedings of the National Academy of Sciences of the United States of America, 106(31), 12986–12991. https://doi.org/10.1073/pnas.0903699106[↩]
- Hepatitis E Questions and Answers for Health Professionals. https://www.cdc.gov/hepatitis/hev/hevfaq.htm[↩][↩][↩][↩][↩]
- Waqar S, Sharma B, Koirala J. Hepatitis E. [Updated 2021 Jul 18]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK532278[↩][↩][↩]
- Hoofnagle JH, Nelson KE, Purcell RH. Hepatitis E. N Engl J Med. 2012 Sep 27;367(13):1237-44. doi: 10.1056/NEJMra1204512[↩][↩][↩]
- Said B, Ijaz S, Kafatos G, et al. Hepatitis E outbreak on cruise ship. Emerg Infect Dis 2009;15(11):1738-44.[↩][↩]
- Kanayama A, Arima Y, Yamagishi T, et al. Epidemiology of domestically acquired hepatitis E virus infection in Japan: assessment of the nationally reported surveillance data, 2007-2013. J Med Microbiol 2015;64(7):752-8.[↩][↩]
- Lee GH, Tan BH, Teo EC, et al. Chronic infection with Camelid Hepatitis E virus in a liver transplant recipient who regularly consumes camel meat and milk. Gastroenterology. 2016; 150(2):355-7.[↩][↩]
- The global prevalence of hepatitis E virus infection and susceptibility. https://www.who.int/publications/i/item/WHO-IVB-10.14[↩]
- Marion O, Abravanel F, Lhomme S, Izopet J, Kamar N. Hepatitis E in transplantation. Curr Infect Dis Rep 2016;18(3):8.[↩]
- The global burden of hepatitis E virus genotypes 1 and 2 in 2005. Hepatology. 2012 Apr;55(4):988-97. doi: 10.1002/hep.25505. https://www.ncbi.nlm.nih.gov/pubmed/22121109[↩]
- Teshale EH, Hu DJ, Holmberg SD. The two faces of hepatitis E virus. Clin Infect Dis 2010;51(3):328-34.[↩]
- Patra S, Kumar A, Trivedi SS, Puri M, Sarin SK. Maternal and fetal outcomes in pregnant women with acute hepatitis E virus infection. Ann Intern Med 2007;147(1):28-33.[↩]
- Feagins AR, Opriessnig T, Guenette DK, Halbur PG, Meng XJ. Detection and characterization of infectious Hepatitis E virus from commercial pig livers sold in local grocery stores in the USA. J Gen Virol 2007;88(Pt 3):912-7.[↩]
- Hepatitis E FAQs for Health Professionals. https://www.cdc.gov/hepatitis/hev/hevfaq.htm[↩]
- Tohme RA, Drobeniuc J, Sanchez R, et al. Acute hepatitis associated with autochthonous hepatitis E virus infection–San Antonio, Texas, 2009. Clin Infect Dis 2011 Oct;53(8):793-6.[↩]
- Teshale EH, Hu DJ. Hepatitis E: epidemiology and prevention. World J Hepatol 2011;Dec 27;3(12):285-91.[↩]
- Emerson SU, Purcell RH. Running like water–the omnipresence of hepatitis E. N Engl J Med. 2004 Dec 2;351(23):2367-8. doi: 10.1056/NEJMp048285[↩]
- Centers for Disease Control and Prevention (CDC). Hepatitis E among U.S. travelers, 1989-1992. MMWR Morb Mortal Wkly Rep. 1993 Jan 15;42(1):1-4.[↩]
- Hepatitis E. https://emedicine.medscape.com/article/178140-overview[↩]
- Ditah I, Ditah F, Devaki P, Ditah C, Kamath PS, Charlton M. Current epidemiology of hepatitis E virus infection in the United States: low seroprevalence in the National Health and Nutrition Evaluation Survey. Hepatology. 2014 Sep;60(3):815-22. doi: 10.1002/hep.27219[↩]
- European Association for the Study of the Liver. Electronic address: [email protected]; European Association for the Study of the Liver. EASL Clinical Practice Guidelines on hepatitis E virus infection. J Hepatol. 2018 Jun;68(6):1256-1271. doi: 10.1016/j.jhep.2018.03.005[↩][↩]
- Khuroo MS, Kamili S, Yattoo GN. Hepatitis E virus infection may be transmitted through blood transfusions in an endemic area. J Gastroenterol Hepatol. 2004 Jul;19(7):778-84. doi: 10.1111/j.1440-1746.2004.03437.x[↩]
- Khuroo MS, Kamili S, Jameel S. Vertical transmission of hepatitis E virus. Lancet. 1995 Apr 22;345(8956):1025-6. doi: 10.1016/s0140-6736(95)90761-0[↩]
- Rivero-Juarez A, Frias M, Rodriguez-Cano D, Cuenca-López F, Rivero A. Isolation of Hepatitis E Virus From Breast Milk During Acute Infection. Clin Infect Dis. 2016 Jun 1;62(11):1464. doi: 10.1093/cid/ciw186[↩]
- Kamar N, Bendall R, Legrand-Abravanel F, Xia NS, Ijaz S, Izopet J, Dalton HR. Hepatitis E. Lancet. 2012 Jun 30;379(9835):2477-2488. doi: 10.1016/S0140-6736(11)61849-7. Epub 2012 Apr 30. Erratum in: Lancet. 2012 Aug 25;380(9843):730.[↩]
- Hepatitis E. https://www.niddk.nih.gov/health-information/liver-disease/viral-hepatitis/hepatitis-e[↩][↩]
- Hoofnagle JH, Nelson KE, Purcell RH. Hepatitis E. The New England Journal of Medicine. 2012;367(13):1237-1244.[↩][↩]
- Navaneethan U., Al Mohajer M., Shata M.T. Hepatitis E and pregnancy: Understanding the pathogenesis. Liver Int. 2008;28:1190–1199. doi: 10.1111/j.1478-3231.2008.01840.x[↩]
- Dibba P., Cholankeril R., Li A.A., Patel M., Fayek M., Dibble C., Okpara N., Hines A., Ahmed A. Hepatitis C in Pregnancy. Diseases. 2018;6:31. doi: 10.3390/diseases6020031[↩]
- Nimgaonkar I., Ding Q., Schwartz R.E., Ploss A. Hepatitis E virus: Advances and challenges. Nat. Rev. Gastroenterol. Hepatol. 2018;15:96–110. doi: 10.1038/nrgastro.2017.150[↩]
- Lin, S., & Zhang, Y. J. (2021). Advances in Hepatitis E Virus Biology and Pathogenesis. Viruses, 13(2), 267. https://doi.org/10.3390/v13020267[↩][↩][↩][↩][↩][↩]
- Sehgal R., Patra S., David P., Vyas A., Khanam A., Hissar S., Gupta E., Kumar G., Kottilil S., Maiwall R., et al. Impaired monocyte-macrophage functions and defective Toll-like receptor signaling in hepatitis E virus-infected pregnant women with acute liver failure. Hepatology. 2015;62:1683–1696. doi: 10.1002/hep.28143[↩]
- Knegendorf L., Drave S.A., Dao Thi V.L., Debing Y., Brown R.J.P., Vondran F.W.R., Resner K., Friesland M., Khera T., Engelmann M., et al. Hepatitis E virus replication and interferon responses in human placental cells. Hepatol. Commun. 2018;2:173–187. doi: 10.1002/hep4.1138[↩]
- Jilani N., Das B.C., Husain S.A., Baweja U.K., Chattopadhya D., Gupta R.K., Sardana S., Kar P. Hepatitis E virus infection and fulminant hepatic failure during pregnancy. J. Gastroenterol. Hepatol. 2007;22:676–682. doi: 10.1111/j.1440-1746.2007.04913.x[↩][↩]
- Agrawal V., Goel A., Rawat A., Naik S., Aggarwal R. Histological and immunohistochemical features in fatal acute fulminant hepatitis E. Indian J. Pathol. Microbiol. 2012;55:22–27. doi: 10.4103/0377-4929.94849[↩]
- Kumar A., Devi S.G., Kar P., Agarwal S., Husain S.A., Gupta R.K., Sharma S. Association of cytokines in hepatitis E with pregnancy outcome. Cytokine. 2014;65:95–104. doi: 10.1016/j.cyto.2013.09.022[↩]
- Gouilly J., Chen Q., Siewiera J., Cartron G., Levy C., Dubois M., Al-Daccak R., Izopet J., Jabrane-Ferrat N., El Costa H. Genotype specific pathogenicity of hepatitis E virus at the human maternal-fetal interface. Nat. Commun. 2018;9:4748. doi: 10.1038/s41467-018-07200-2[↩][↩]
- Tibbetts T.A., DeMayo F., Rich S., Conneely O.M., O’Malley B.W. Progesterone receptors in the thymus are required for thymic involution during pregnancy and for normal fertility. Proc. Natl. Acad. Sci. USA. 1999;96:12021–12026. doi: 10.1073/pnas.96.21.12021[↩]
- Yang C., Yu W., Bi Y., Long F., Li Y., Wei D., Hao X., Situ J., Zhao Y., Huang F. Increased oestradiol in hepatitis E virus-infected pregnant women promotes viral replication. J. Viral Hepat. 2018;25:742–751. doi: 10.1111/jvh.12865[↩]
- Centers for Disease Control and Prevention. Hepatitis E FAQs for Health Professionals. https://www.cdc.gov/hepatitis/hev/hevfaq.htm[↩]
- Takahashi, M., Kusakai, S., Mizuo, H., Suzuki, K., Fujimura, K., Masuko, K., Sugai, Y., Aikawa, T., Nishizawa, T., & Okamoto, H. (2005). Simultaneous detection of immunoglobulin A (IgA) and IgM antibodies against hepatitis E virus (HEV) Is highly specific for diagnosis of acute HEV infection. Journal of clinical microbiology, 43(1), 49–56. https://doi.org/10.1128/JCM.43.1.49-56.2005[↩]
- Khuroo MS, Khuroo MS. Hepatitis E: an emerging global disease – from discovery towards control and cure. J Viral Hepat. 2016 Feb;23(2):68-79. doi: 10.1111/jvh.12445[↩][↩]
- Kamar, N., Bendall, R. P., Peron, J. M., Cintas, P., Prudhomme, L., Mansuy, J. M., Rostaing, L., Keane, F., Ijaz, S., Izopet, J., & Dalton, H. R. (2011). Hepatitis E virus and neurologic disorders. Emerging infectious diseases, 17(2), 173–179. https://doi.org/10.3201/eid1702.100856[↩]





{kind=link}