Kluver Bucy syndrome
Kluver Bucy syndrome is a rare neuro-psychiatric disorder characterized by inappropriate sexual behaviors and putting objects in mouths 1. Other signs and symptoms, include a diminished ability to visually recognize objects (visual agnosia), loss of normal fear and anger responses, memory loss, distractibility, seizures, and dementia. Kluver Bucy syndrome is associated with damage to both of the anterior temporal lobes of the brain, especially hippocampus and amygdala 2. Cases have been reported in association with herpes encephalitis and head trauma 3.
Kluver Bucy syndrome is a very rare disease that affects males and females equally. Human Kluver Bucy syndrome is more or less restricted to case series and reports. Hence the exact prevalence is difficult to estimate.
Treatment is symptomatic and supportive and may include the use of psychotropic medications 3.
Kluver Bucy syndrome cause
Kluver Bucy syndrome is the result of damage to the temporal lobes of the brain. This may be the result of trauma to the brain itself, or the result of other degenerative brain diseases, tumors, or it can be caused by some brain infections, most commonly herpes simplex encephalitis (a viral brain infection).
Kluver Bucy syndrome is known to be associated with several pathologies. The most common pathologies leading to the development of Kluver Bucy syndrome are head injury and stroke in adults and herpes simplex encephalitis in children. There are many case reports of several conditions (listed below) ranging from infections like shigellosis to methamphetamine withdrawal. But how Kluver Bucy syndrome occurred in these conditions remains unclear.
- Herpes simplex encephalitis 4
- Stroke (temporal lobe infarction – usually bilateral) 5
- Listeria meningoencephalitis 6
- Traumatic brain injury 7
- Central nervous system tuberculosis 8
- Primary cerebral Whipple disease 9
- Alzheimer disease 10
- Pick disease 11
- Hypoglycemia 12
- Acute sporadic porphyria 13
- Huntington disease 14
- Juvenile neuronal lipofuscinosis 15
- Toxoplasmosis
- Epilepsy 16
- Parkinson disease
- Heat stroke 17
- Shigellosis 18
- Methamphetamine withdrawal 19
- Systemic lupus erythematosus 20
- Anoxic-ischemic encephalopathy 21
- Neurocysticercosis 21
- Non-Hodgkin lymphoma 22
- Mycoplasmal bronchitis 23
- Methotrexate leukoencephalopathy 24
- Subdural hygroma 25
Kluver Bucy syndrome pathophysiology
The significant clinical symptoms of Kluver Bucy syndrome are produced by the destruction of either the temporal neocortex or the amygdala bilaterally. The full syndrome is rarely seen in humans because the anterior temporal lobe dysfunction is usually less severe in humans when compared to that following total temporal lobe resection in monkeys 26.
The exact anatomical basis of Kluver Bucy syndrome is still controversial. Kluver Bucy syndrome is thought to occur due to the disturbances in the temporal portions of limbic networks that connect with multiple cortical and subcortical circuits to modulate emotional behavior and affect 26. A sine qua non for Kluver Bucy syndrome is the involvement of medial temporal lobe regions along with bilateral lesions of the Ammon horn 27. Even though Kluver Bucy syndrome is always thought to follow bilateral malfunctions of the temporal lobes, it is important to note that the amygdala, uncus, hippocampus, orbitofrontal and cingulate gyri, and insular cortex have an important role in its pathogenesis.
Theories regarding the cause of Kluver Bucy syndrome:
- Norman Geschwind theory: Interruption of visual input to limbic circuit leading to disconnection syndrome produces Kluver Bucy syndrome 28.
- Muller theory: Disconnection of the pathways connecting the dorsomedial thalamus with the prefrontal cortex and other limbic areas lead to Kluver Bucy syndrome. These pathways are essential for memory and emotional regulation 29.
The origin of various symptoms of Kluver Bucy syndrome are explainable as follows:
- Rage is produced by the involvement of the ventromedian nucleus of thalamus and amygdala 30.
- A permanent “hypersexed state,” produced by discrete bilateral lesions of the lateral amygdaloid nucleus. Temporal lobe seizures may produce a transient state.
- Visual agnosia results from bilateral ventral temporal ablations and temporal lobectomies.
Kluver Bucy syndrome symptoms
Kluver Bucy syndrome major symptoms may include excessive oral tendencies with an urge to put all kinds of objects into the mouth, hypermetamorophosis (a need to explore everything), memory loss, emotional changes, extreme sexual behavior, indifference, placidity, visual distractibility and visual agnosia (difficulty identifying and processing visual information). An almost uncontrollable appetite for food may also be noted. There may also be other symptoms associated with dementia (loss of reason) as well.
The following clinical features characterize Kluver Bucy syndrome 2:
- Hyperorality – Socially inappropriate lickings and a strong compulsion to place objects inside the mouth
- Hypermetamorphosis (excessive attentiveness to visual stimuli with a tendency to touch every such stimulus)
- Hypersexuality – Lack of social restraint in terms of sexuality, with inappropriate sexual activity and attempted copulation with inanimate objects
- Eating disorder – Objects are placed in the mouth and explored with the tongue to counteract visual agnosia.
- Bulimia, which is an eating disorder characterized by binge eating, followed by purging, is also markedly seen and may cause weight gain.
- Placidity – Flat affect and reduced response to emotional stimuli
- Visual agnosia (psychic blindness) – Inability to recognize familiar objects or faces presented visually
- Amnesia.
Patients having a combination of three or more different elements listed above are described as having partial Kluver Bucy syndrome 8.
Kluver Bucy syndrome symptoms in adults
Kluver Bucy syndrome clinical features in adults:
- Hyperorality
- Hypersexuality
- Eating disorder – Objects are placed in the mouth and explored with the tongue to counteract visual agnosia. Bulimia, which is an eating disorder characterized by binge eating, followed by
- purging, is also markedly seen and may cause weight gain.
- Placidity
- Visual agnosia
- Amnesia.
Placidity, hyperorality, and dietary changes are the most commonly occurring symptoms in Kluver Bucy syndrome.
Kluver Bucy syndrome symptoms in children
Kluver Bucy syndrome in children usually occurs secondary to herpes simplex encephalitis with classic features occurring only in a few.
- Marked indifference
- Bulimia and hyperorality
- Lack of emotional attachment towards the family
- Hypersexuality:
- The frequent holding of genitals
- Intermittent pelvic thrusts
- Rubbing of genitals to the bed after lying prone
Kluver Bucy syndrome complications
Due to hyperorality and hypermetamorphosis, the patient may try to put whatever objects he comes across into his mouth, which can be dangerous.
Due to hypersexuality, he may try to engage in sex with others whom he does not even know, leading to criminal procedures against the patient there is no awareness of the diagnosis.
Bulimia can cause weight gain, electrolyte disturbance, and poor oral hygiene.
Kluver Bucy syndrome diagnosis
The diagnosis of Kluver Bucy syndrome is mainly clinical. Once diagnosed, proper evaluation to find out the underlying pathology will be helpful in the overall management.
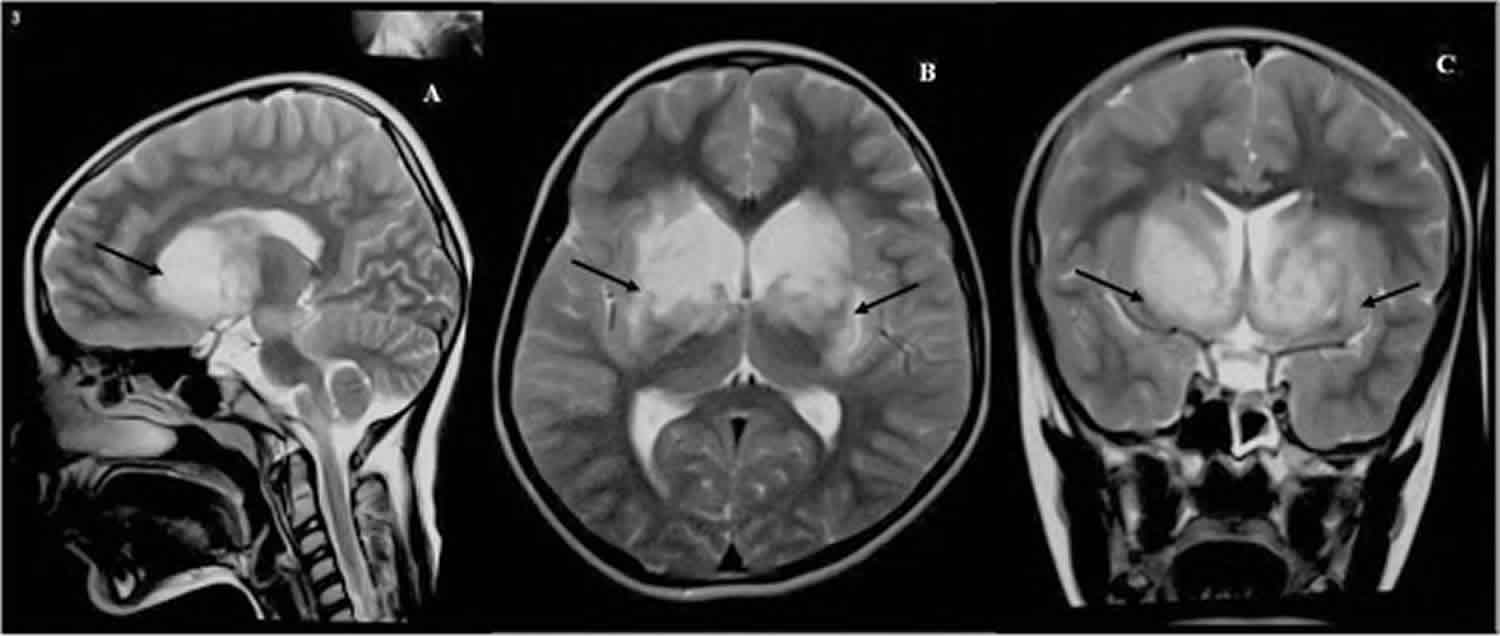
Magnetic resonance imaging of the brain is useful in identifying the extent of temporal lobe damage.
Electroencephalogram is also useful to identify seizures originating especially from the temporal lobe.
In head injury and other conditions producing a long duration of loss of consciousness, the appropriate staging of the consciousness is possible with the Modified Innsbruck Remission Scale, which includes the Kluver Bucy phase as well 31.
Kluver Bucy syndrome treatment
The treatment of Kluver Bucy syndrome can be challenging due to the facts that there is no specific treatment for the condition, and the clinical course will vary from patient to patient. Most of the treatment focuses on managing the symptoms. The main drugs used in the management are:
- Mood stabilizers
- Antidepressants (selective serotonin reuptake inhibitors)
- Antipsychotic drugs
- Carbamazepine
- Leuprolide
Carbamazepine and leuprolide are used to reduce the sexual behavioral abnormality, whereas haloperidol and anticholinergics are useful in treating behavioral abnormalities associated with Kluver Bucy syndrome 32.
Kluver Bucy syndrome prognosis
There is no cure for Kluver Bucy syndrome 33. The disorder is not life-threatening, but the patient can be difficult to manage. With treatment, symptoms may slowly decline.
Some Kluver Bucy syndrome features (i.e., hyperorality, placidity, hypermetamorphosis) persist indefinitely, whereas others gradually resolve over several years.
The clinical course of Kluver Bucy syndrome varies among the case reports.
Kluver Bucy syndrome occurring secondary to epileptic seizures, infections or post-infectious, and traumatic brain injuries may have a better prognosis as many of the damages would be reversible if recognized early and managed appropriately.
References- Kar SK, Das A, Pandey S, Gupta B. Kluver-Bucy Syndrome in an Adolescent Girl: A Sequel of Encephalitis. J Pediatr Neurosci. 2018 Oct-Dec;13(4):523-524.
- M Das J, Siddiqui W. Kluver Bucy Syndrome. [Updated 2019 Dec 3]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK544221
- Klüver-Bucy Syndrome. https://rarediseases.org/rare-diseases/kluver-bucy-syndrome
- Eikmeier G, Forquignon I, Honig H. [Klüver-Bucy syndrome after herpes simplex encephalitis]. Psychiatr Prax. 2013 Oct;40(7):392-3.
- Chou CL, Lin YJ, Sheu YL, Lin CJ, Hseuh IH. Persistent Klüver-Bucy syndrome after bilateral temporal lobe infarction. Acta Neurol Taiwan. 2008 Sep;17(3):199-202.
- Cohen MJ, Park YD, Kim H, Pillai JJ. Long-term neuropsychological follow-up of a child with Klüver-Bucy syndrome. Epilepsy Behav. 2010 Dec;19(4):643-6.
- Morcos N, Guirgis H. A case of acute-onset partial Kluver-Bucy syndrome in a patient with a history of traumatic brain injury. J Neuropsychiatry Clin Neurosci. 2014 Summer;26(3):E10-1.
- Jha KK, Singh SK, Kumar P, Arora CD. Partial Kluver-Bucy syndrome secondary to tubercular meningitis. BMJ Case Rep. 2016 Aug 16;2016
- Leesch W, Fischer I, Staudinger R, Miller DC, Sathe S. Primary cerebral Whipple disease presenting as Klüver-Bucy syndrome. Arch. Neurol. 2009 Jan;66(1):130-1.
- Kile SJ, Ellis WG, Olichney JM, Farias S, DeCarli C. Alzheimer abnormalities of the amygdala with Klüver-Bucy syndrome symptoms: an amygdaloid variant of Alzheimer disease. Arch. Neurol. 2009 Jan;66(1):125-9.
- Cummings JL, Duchen LW. Kluver-Bucy syndrome in Pick disease: clinical and pathologic correlations. Neurology. 1981 Nov;31(11):1415-22.
- Boudjemline AM, Isapof A, Witas JB, Petit FM, Gajdos V, Labrune P. Klüver Bucy syndrome following hypoglycaemic coma in a patient with glycogen storage disease type Ib. J. Inherit. Metab. Dis. 2010 Dec;33 Suppl 3:S477-80.
- Guidotti TL, Charness ME, Lamon JM. Acute intermittent porphyria and the Klüver — Bucy syndrome. Johns Hopkins Med J. 1979 Dec;145(6):233-5.
- Janati A. Kluver-Bucy syndrome in Huntington’s chorea. J. Nerv. Ment. Dis. 1985 Oct;173(10):632-5.
- Lanska DJ, Lanska MJ. Klüver-Bucy syndrome in juvenile neuronal ceroid lipofuscinosis. J. Child Neurol. 1994 Jan;9(1):67-9.
- Naito K, Hashimoto T, Ikeda S. Klüver-Bucy syndrome following status epilepticus associated with hepatic encephalopathy. Epilepsy Behav. 2008 Feb;12(2):337-9.
- Pitt DC, Kriel RL, Wagner NC, Krach LE. Kluver-Bucy syndrome following heat stroke in a 12-year-old girl. Pediatr. Neurol. 1995 Jul;13(1):73-6.
- Guedalia JS, Zlotogorski Z, Goren A, Steinberg A. A reversible case of Klüver-Bucy syndrome in association with shigellosis. J. Child Neurol. 1993 Oct;8(4):313-5.
- Samanta D. Transient Kluver-Bucy syndrome from methamphetamine withdrawal. Neurol India. 2015 Mar-Apr;63(2):267-8.
- Lin HF, Yeh YC, Chen CF, Chang WC, Chen CS. Kluver-Bucy syndrome in one case with systemic lupus erythematosus. Kaohsiung J. Med. Sci. 2011 Apr;27(4):159-62.
- Jha S, Patel R. Kluver-Bucy syndrome — an experience with six cases. Neurol India. 2004 Sep;52(3):369-71.
- Unal E, Koksal Y, Baysal T, Energin Ml, Aydin K, Caliskan U. Kluver-Bucy syndrome in a boy with non-Hodgkin lymphoma. Pediatr Hematol Oncol. 2007 Mar;24(2):149-52.
- Auvichayapat N, Auvichayapat P, Watanatorn J, Thamaroj J, Jitpimolmard S. Kluver-Bucy syndrome after mycoplasmal bronchitis. Epilepsy Behav. 2006 Feb;8(1):320-2.
- Antunes NL, Souweidane MM, Lis E, Rosenblum MK, Steinherz PG. Methotrexate leukoencephalopathy presenting as Klüver-Bucy syndrome and uncinate seizures. Pediatr. Neurol. 2002 Apr;26(4):305-8.
- Duggal HS, Khess CR, Nizamie SH. Subdural hygroma presenting as dementia with kluver-bucy symptoms. Indian J Psychiatry. 1999 Oct;41(4):371-3.
- Lanska DJ. The Klüver-Bucy Syndrome. Front Neurol Neurosci. 2018;41:77-89.
- Olson DA. Klüver-Bucy syndrome as a result of minor head trauma. South. Med. J. 2003 Mar;96(3):323.
- Geschwind N. Disconnexion syndromes in animals and man: Part I. 1965. Neuropsychol Rev. 2010 Jun;20(2):128-57.
- Müller A, Baumgartner RW, Röhrenbach C, Regard M. Persistent Klüver-Bucy syndrome after bilateral thalamic infarction. Neuropsychiatry Neuropsychol Behav Neurol. 1999 Apr;12(2):136-9.
- Rajmohan V, Mohandas E. The limbic system. Indian J Psychiatry. 2007 Apr;49(2):132-9.
- von Wild K, Laureys ST, Gerstenbrand F, Dolce G, Onose G. The vegetative state–a syndrome in search of a name. J Med Life. 2012 Feb 22;5(1):3-15.
- Hooshmand H, Sepdham T, Vries JK. Klüver-Bucy syndrome. Successful treatment with carbamazepine. JAMA. 1974 Sep 23;229(13):1782.
- Klüver-Bucy Syndrome Information Page. https://www.ninds.nih.gov/Disorders/All-Disorders/Kl%C3%BCver-Bucy-Syndrome-Information-Page





{kind=link}