
Lewy Body Dementia
Lewy body dementia is a disease associated with abnormal deposits of a protein called alpha-synuclein in the brain 1. These deposits, called Lewy bodies, affect chemicals in the brain whose changes, in turn, can lead to problems with thinking, movement, behavior, and mood. Lewy body dementia is one of the most common causes of dementia, after Alzheimer’s disease and vascular disease dementia. People affected by this condition may experience a variety of symptoms such as changes in alertness and attention; hallucinations; problems with movement and posture; muscle stiffness; confusion; and/or memory loss 2.
There are two types of Lewy body dementia 3:
- Dementia with Lewy bodies (DLB). Dementia with Lewy bodies causes problems with thinking ability that seem similar to Alzheimer’s disease. Later, it also causes other symptoms, such as movement symptoms, visual hallucinations, and certain sleep disorders. It also causes more trouble with mental activities than with memory.
- Parkinson’s disease dementia (PDD). Parkinson’s disease dementia starts as a movement disorder. It first causes the symptoms of Parkinson’s disease: slowed movement, muscle stiffness, tremor, and a shuffling walk. Later on, it causes dementia.
Lewy body dementias are the second most common form of degenerative dementia. The only other form of degenerative dementia that is more common than Lewy body dementia is Alzheimer’s disease 4. Lewy body dementias affect an estimated 1.4 million individuals and their families in the United States. And currently there is no cure for Lewy body dementia 5.
Lewy body dementia is an umbrella term for dementia associated with the presence of Lewy bodies (abnormal deposits of a protein called alpha-synuclein) in the brain. Lewy body dementia usually occurs sporadically in people with no family history of the condition. Rarely, more than one family member may be affected. There is currently no cure for Lewy body dementia; however, medications may be available to help manage the associated symptoms 6, 7, 8.
Lewy body dementia can have three common presentations. Regardless of the initial symptom, over time all three presentations of Lewy body dementia will develop very similar cognitive, physical, sleep and behavioral features 4:
- Some individuals will start out with a movement disorder leading to the diagnosis of Parkinson’s disease and later develop dementia. This is diagnosed as Parkinson’s disease dementia.
- Another group of individuals will start out with a cognitive/memory disorder that may be mistaken for Alzheimer’s disease, but over time two or more distinctive features become apparent leading to the diagnosis of ‘dementia with Lewy bodies’ (DLB).
- Lastly, a small group will first present with neuropsychiatric symptoms, which can include hallucinations, behavioral problems, and difficulty with complex mental activities, also leading to an initial diagnosis of dementia with Lewy bodies.
The most common features of dementia with Lewy bodies (DLB) are progressive cognitive impairment leading eventually to full-blown dementia, parkinsonian motor symptoms (tremor, slowed
mobility, stiffness of muscles, stooped posture, shuffling gait), visual hallucinations, and fluctuations in levels of alertness and cognitive acuity. Other symptoms include acting out dreams (REM sleep behavior disorder) and disturbances of autonomic function (low blood pressure, constipation and urinary frequency) 9. Severe sensitivity or over-reaction to antipsychotic drugs (neuroleptics) are also common.
Lewy body dementia is often misdiagnosed as Alzheimer’s disease, especially in those individuals who have few, if any signs of motor parkinsonism 10.
Diagnosing Lewy body dementia can be challenging for a number of reasons. Early Lewy body dementia symptoms are often confused with similar symptoms found in other brain diseases like Alzheimer’s disease. Also, Lewy body dementia can occur alone or along with Alzheimer’s or Parkinson’s disease.
Many physicians and other medical professionals are not familiar with Lewy body dementia, so patients may consult several doctors before receiving a diagnosis. Visiting a family doctor is often the first step for people who are experiencing changes in thinking, movement, or behavior. However, neurologists— doctors who specialize in disorders of the brain and nervous system—generally have the expertise needed to diagnose Lewy body dementia. Geriatric psychiatrists, neuropsychologists, and geriatricians may also be skilled in diagnosing the condition.
There are two types of Lewy body dementia
- Dementia with Lewy bodies (DLB). Dementia with Lewy bodies causes problems with thinking ability that seem similar to Alzheimer’s disease. Later, it also causes other symptoms, such as movement symptoms, visual hallucinations, and certain sleep disorders. It also causes more trouble with mental activities than with memory.
- Parkinson’s disease dementia (PDD). Parkinson’s disease dementia starts as a movement disorder. It first causes the symptoms of Parkinson’s disease: slowed movement, muscle stiffness, tremor, and a shuffling walk. Later on, it causes dementia.
The earliest signs of these two diseases differ but reflect the same biological changes in the brain. And, over time, they can cause similar symptoms. The main difference is in when the cognitive (thinking) and movement symptoms start. The two diseases are demarcated clinically from one another by the so-called 1-year rule, based on the temporal onset of motor relative to cognitive symptoms (ie, in Parkinson’s disease dementia [PDD] the motor symptoms precede the onset of dementia by at least one year) 9. Individuals with dementia with Lewy bodies (DLB) present with dementia as the early disabling symptom, plus other Lewy body dementia symptoms, one of which may be parkinsonism. Others will present with motor symptoms resulting in a diagnosis of Parkinson’s disease and may also have some mild cognitive impairment (MCI) initially or in the early stages of the disease; over time, usually several years or more, some will progress to Parkinson’s disease dementia (PDD) 3.
Dementia with Lewy Bodies
People with dementia with Lewy bodies (DLB) have a decline in thinking ability that may look somewhat like Alzheimer’s disease. But over time they also develop movement and other distinctive symptoms that suggest dementia with Lewy bodies. Symptoms that distinguish this form of dementia from others may include:
- visual hallucinations early in the course of dementia
- fluctuations in cognitive ability, attention, and alertness
- slowness of movement, difficulty walking, or rigidity (parkinsonism)
- sensitivity to medications used to treat hallucinations
- REM sleep behavior disorder (RBD), in which people physically act out their dreams by yelling, flailing, punching bed partners, and falling out of bed
- more trouble with complex mental activities, such as multitasking, problem solving, and analytical thinking, than with memory
Parkinson’s Disease Dementia
This type of Lewy body dementia starts as a movement disorder, with symptoms such as slowed movement, muscle stiffness, tremor, and a shuffling walk. These symptoms are consistent with a diagnosis of Parkinson’s disease. Later on, cognitive symptoms of dementia and changes in mood and behavior may arise. Not all people with Parkinson’s develop dementia, and it is difficult to predict who will. Being diagnosed with Parkinson’s late in life is a risk factor for Parkinson’s disease dementia.
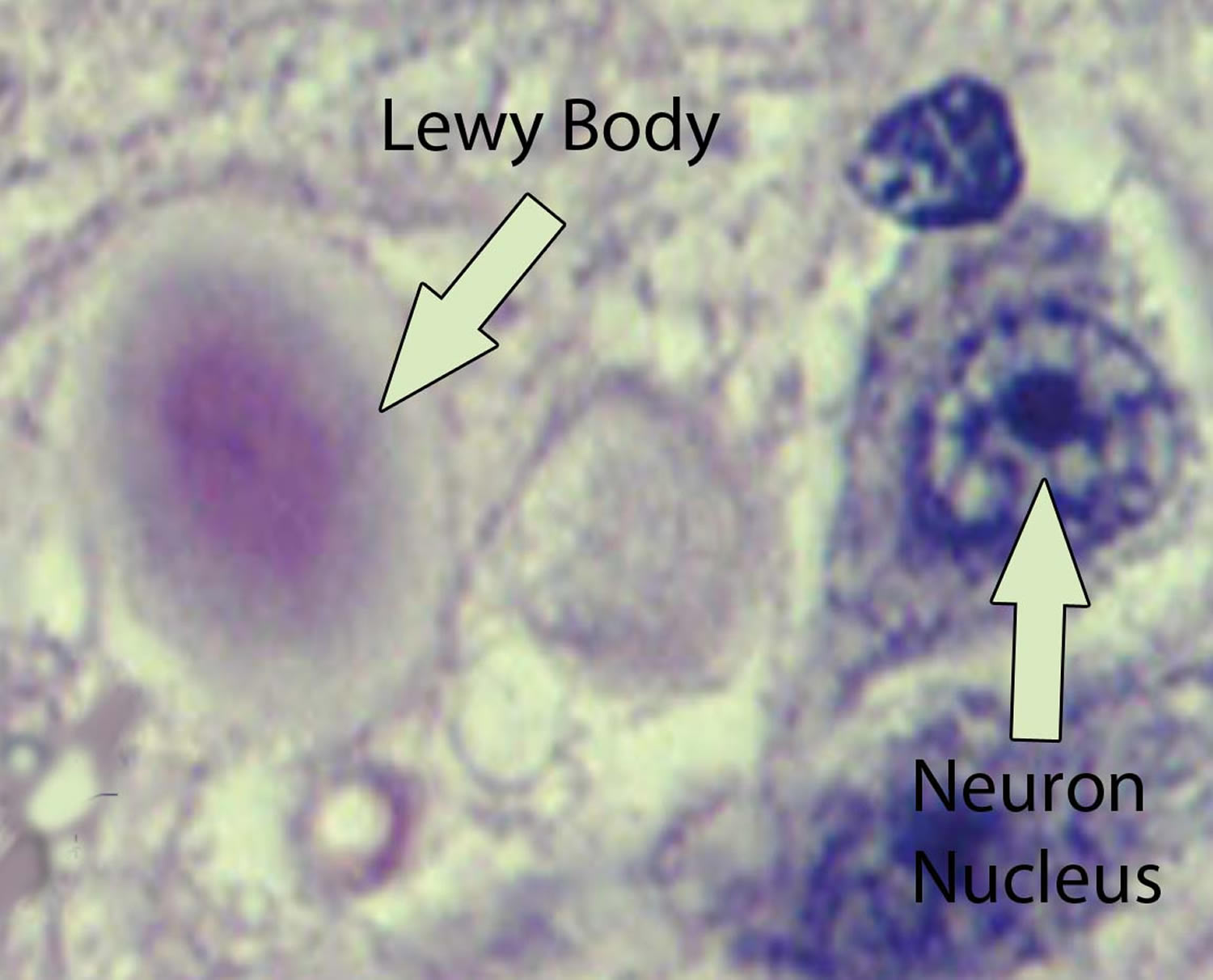
What are Lewy Bodies?
Lewy bodies are named for Dr. Friederich Lewy, a German neurologist. In 1912, he discovered abnormal protein deposits that disrupt the brain’s normal functioning in people with Parkinson’s disease 1. These abnormal deposits are now called “Lewy bodies.”
Lewy bodies are made of a protein called alpha-synuclein 1. In the healthy brain, alpha-synuclein plays a number of important roles in neurons (nerve cells) in the brain, especially at synapses, where brain cells communicate with each other. In Lewy body dementia, alpha-synuclein forms into clumps inside neurons, starting in particular regions of the brain. This process causes neurons to work less effectively and, eventually, to die. The activities of brain chemicals important to brain function are also affected. The result is widespread damage to certain parts of the brain and a decline in abilities affected by those brain regions.
Lewy bodies affect several different brain regions in Lewy body dementia:
- The cerebral cortex, which controls many functions, including information processing, perception, thought, and language
- The limbic cortex, which plays a major role in emotions and behavior
- The hippocampus, which is essential to forming new memories
- The midbrain, including the substantia nigra, which is involved in movement
- The brain stem, which is important in regulating sleep and maintaining alertness
- Brain regions important in recognizing smells (olfactory pathways)
Who is affected by Lewy body dementia?
Lewy body dementia affects more than 1 million individuals in the United States 1. Lewy body dementia typically begins at age 50 or older, although sometimes younger people have it. Lewy body dementia appears to affect slightly more men than women.
Lewy body dementia is a progressive disease, meaning symptoms start slowly and worsen over time. The disease lasts an average of 5 to 7 years from the time of diagnosis to death, but the time span can range from 2 to 20 years 1. How quickly symptoms develop and change varies greatly from person to person, depending on overall health, age, and severity of symptoms.
In the early stages of Lewy body dementia, usually before a diagnosis is made, symptoms can be mild, and people can function fairly normally. As the disease advances, people with Lewy body dementia require more and more help due to a decline in thinking and movement abilities. In the later stages of the disease, they may depend entirely on others for assistance and care.
Some Lewy body dementia symptoms may respond to treatment for a period of time. Currently, there is no cure for the disease 1. Research is improving our understanding of this challenging condition, and advances in science may one day lead to better diagnosis, improved care, and new treatments.
Lewy body dementia signs and symptoms
People with Lewy body dementia may not have every Lewy body dementia symptom, and the severity of symptoms can vary greatly from person to person 11. Throughout the course of the disease, any sudden or major change in functional ability or behavior should be reported to a doctor.
Lewy body dementia signs and symptoms can include:
- Visual hallucinations. Hallucinations — seeing things that aren’t there — might be one of the first symptoms, and they often recur. People with Lewy body dementia might hallucinate shapes, animals or people. Sound (auditory), smell (olfactory) or touch (tactile) hallucinations are possible.
- Movement disorders. Signs of Parkinson’s disease (parkinsonian signs), such as slowed movement, rigid muscles, tremor or a shuffling walk can occur. This can lead to falling.
- Poor regulation of body functions (autonomic nervous system dysfunction). Blood pressure, pulse, sweating and the digestive process are regulated by a part of the nervous system that is often affected by Lewy body dementia. This can result in sudden drops in blood pressure upon standing (orthostatic hypotension), dizziness, falls, loss of bladder control (urinary incontinence) and bowel issues such as constipation.
- Cognitive problems. You might have thinking (cognitive) problems similar to those of Alzheimer’s disease, such as confusion, poor attention, visual-spatial problems and memory loss.
- Sleep difficulties. You might have rapid eye movement (REM) sleep behavior disorder, which can cause you to physically act out your dreams while you’re asleep. This might involve behavior such as punching, kicking, yelling and screaming while sleeping.
- Fluctuating attention. Episodes of drowsiness, long periods of staring into space, long naps during the day or disorganized speech are possible.
- Depression. You might develop depression.
- Apathy. You might lose motivation.
Early, suggestive indicators of Lewy body dementia:
- Often recognized only in retrospect, possibly extending back 1-3 years. Occasional minor episodes of forgetfulness, sometimes described as lapses of concentration or ‘switching off’.
- An initial brief period of delirium in association with genuine physical illness and/or surgical procedures, return to baseline, followed by a subsequent mental and physical decline.
Lewy body dementia is progressive. Signs and symptoms worsen, causing:
- Severe dementia
- Aggressive behavior. Increasing behavioral disturbances, including shouting, aggression on approach and evidence of persisting delirium.
- Depression
- Increased risk of falling and injury
- Worsening of parkinsonian signs and symptoms, such as tremors
- Death, on average about seven to eight years after symptoms start. Death is usually due to respiratory or cardiac disease, or injuries sustained in falls.
The symptoms of Lewy body dementia are treatable:
All medications prescribed for Lewy body dementia are approved for a course of treatment for symptoms related to other diseases such as Alzheimer’s disease and Parkinson’s disease with dementia and offer symptomatic benefits for cognitive, movement and behavioral problems.
The most common symptoms include changes in cognition, movement, sleep, and behavior 11.
Table 1. Main Symptoms of Lewy Body Dementia
| Symptom | Dementia with Lewy Bodies | Parkinson’s Disease Dementia |
|---|---|---|
| Dementia | Primary symptom (appears within a year of movement problems) | Primary symptom (appears later in the disease, after movement problems) |
| Movement problems (parkinsonism) | Primary symptom (appear at the same time as or after dementia) | Primary symptom (appear before dementia) |
| Fluctuating cognition, attention, alertness | Primary symptom | Primary symptom |
| Visual hallucinations | Primary symptom | Primary symptom |
| REM sleep behavior disorder | Common symptom (may develop years before other symptoms) | Common symptom (may develop years before other symptoms) |
| Extreme sensitivity to antipsychotic medications | Common symptom | Common symptom |
| Changes in personality and mood (depression, delusions, apathy) | Common symptom | Common symptom |
| Changes in autonomic (involuntary) nervous system (blood pressure, bladder and bowel control) | Common symptom | Common symptom |
Cognitive symptoms
Lewy body dementia causes changes in thinking abilities. These changes may include:
- Dementia—Severe loss of thinking abilities that interferes with a person’s capacity to perform daily activities. Dementia is a primary symptom in Lewy body dementia and usually includes trouble with visual and spatial abilities (judging distance and depth or misidentifying objects), planning, multitasking, problem solving, and reasoning. Memory problems may not be evident at first but often arise as Lewy body dementia progresses. Dementia can also include changes in mood and behavior, poor judgment, loss of initiative, confusion about time and place, and difficulty with language and numbers.
- Cognitive fluctuations—Unpredictable changes in concentration, attention, alertness, and wakefulness from day to day and sometimes throughout the day. A person with Lewy body dementia may stare into space for periods of time, seem drowsy and lethargic, or sleep for several hours during the day despite getting enough sleep the night before. His or her flow of ideas may be disorganized, unclear, or illogical at times. The person may seem better one day, then worse the next day. These cognitive fluctuations are common in Lewy body dementia but are not always easy for a doctor to identify.
- Hallucinations—Seeing or hearing things that are not present. Visual hallucinations occur in up to 80 percent of people with Lewy body dementia, often early on. They are typically realistic and detailed, such as images of children or animals. Auditory hallucinations are less common than visual ones but may also occur. Hallucinations that are not disruptive may not require treatment. However, if they are frightening or dangerous (for example, if the person attempts to fight a perceived intruder), then a doctor may prescribe medication.
Movement Symptoms
Some people with Lewy body dementia may not experience significant movement problems for several years. Others may have them early on. At first, signs of movement problems, such as a change in handwriting, may be very mild and thus overlooked. Parkinsonism is seen early on in Parkinson’s disease dementia but can also develop later on in dementia with Lewy bodies. Specific signs of parkinsonism may include:
- Muscle rigidity or stiffness
- Shuffling gait, slow movement, or frozen stance
- Tremor or shaking, most commonly at rest
- Balance problems and falls
- Stooped posture
- Loss of coordination
- Smaller handwriting than was usual for the person
- Reduced facial expression
- Difficulty swallowing
- A weak voice
Sleep Disorders
Sleep disorders are common in people with Lewy body dementia but are often undiagnosed. A sleep specialist can play an important role on a treatment team, helping to diagnose and treat sleep disorders. Sleep-related disorders seen in people with Lewy body dementia may include:
- REM sleep behavior disorder (RBD)—A condition in which a person seems to act out dreams. It may include vivid dreaming, talking in one’s sleep, violent movements, or falling out of bed. Sometimes only the bed partner of the person with Lewy body dementia is aware of these symptoms. REM sleep behavior disorder appears in some people years before other Lewy body dementia symptoms.
- Excessive daytime sleepiness—Sleeping 2 or more hours during the day.
- Insomnia—Difficulty falling or staying asleep, or waking up too early.
- Restless leg syndrome—A condition in which a person, while resting, feels the urge to move his or her legs to stop unpleasant or unusual sensations. Walking or moving usually relieves the discomfort.
Behavioral and Mood Symptoms
Changes in behavior and mood are possible in Lewy body dementia. These changes may include:
- Depression—A persistent feeling of sadness, inability to enjoy activities, or trouble with sleeping, eating, and other normal activities.
- Apathy—A lack of interest in normal daily activities or events; less social interaction.
- Anxiety—Intense apprehension, uncertainty, or fear about a future event or situation. A person may ask the same questions over and over or be angry or fearful when a loved one is not present.
- Agitation—Restlessness, as seen by pacing, hand wringing, an inability to get settled, constant repeating of words or phrases, or irritability.
- Delusions—Strongly held false beliefs or opinions not based on evidence. For example, a person may think his or her spouse is having an affair or that relatives long dead are still living. Another delusion that may be seen in people with Lewy body dementia is Capgras syndrome, in which the person believes a relative or friend has been replaced by an imposter.
- Paranoia—An extreme, irrational distrust of others, such as suspicion that people are taking or hiding things.
Other Lewy body dementia Symptoms
People with Lewy body dementia can also experience significant changes in the part of the nervous system that regulates automatic functions such as those of the heart, glands, and muscles. The person may have:
- Changes in body temperature
- Problems with blood pressure
- Dizziness
- Fainting
- Frequent falls
- Sensitivity to heat and cold
- Sexual dysfunction
- Urinary incontinence
- Constipation
- A poor sense of smell.
Lewy body dementia causes
The cause of Lewy body dementia is still unknown 13. Lewy body dementia is characterized by the abnormal buildup of proteins into masses known as Lewy bodies, which are a microscopic aggregation of a specific abnormal protein called alpha-synuclein (α-synuclein). This protein is also associated with Parkinson’s disease. People who have Lewy bodies in their brains also have the plaques and tangles associated with Alzheimer’s disease.
Brain pathological changes in Lewy body dementia involve selective damage and loss of nerve cells in certain regions of the brain (example: substantia nigra in the brainstem). Affected, but less damaged cells contain Lewy bodies. The Lewy body is the pathological signature of Lewy body dementia that overwhelms the cell’s normal biological functions and causes it to die 14.
There are many possible causes of Lewy body dementia but researchers are just beginning to understand the reasons why some people are more susceptible to developing Lewy body dementia. One important reason that has recently come to light is the discovery of an increasing number of genetic variants that increase the likelihood that a person will develop Lewy body dementia. Dementia with Lewy bodies (DLB) and Parkinson’s disease dementia (PDD) are clinically similar, except for the timing of onset of cognitive impairment, but the pathology of the two is almost identical. This is both a surprise and a mystery, since there is no good explanation for the variability of the motor-cognitive interval among people with Lewy body dementia. In other words, why do some people develop serious cognitive impairment at the earliest stage of a Lewy body disorder, whereas others remain cognitively normal for many years before impairment develops or never develop dementia?
Another puzzling fact is the frequent coexistence of the pathology of Alzheimer’s disease (amyloid plaques and neurofibrillary tangles) in dementia with Lewy bodies (DLB) compared with Parkinson’s disease dementia (PDD). Alzheimer’s disease differs from Lewy body dementia clinically because of its distinctive cognitive profile (mostly a disorder of memory without the other features typical of Lewy body dementia) and its lack of parkinsonian features except in late stages. The clinical overlap between Alzheimer’s disease and dementia with Lewy bodies (DLB) in the absence of a specific diagnostic test leads to misdiagnosis in a significant minority of patients. Currently, the only way to definitively diagnose Lewy body dementia is with an autopsy 3. These facts underscore the current concept of a neurodegenerative continuum with boundaries that are frequently blurred. It is only through research that these and other fundamental questions will be answered.
Risk factors for developing Lewy body dementia
A few factors seem to increase the risk of developing Lewy body dementia, including:
- Older age. Older age is the greatest risk factor for Lewy body dementia, with most diagnoses being made in individuals over the age of 50. There is some evidence that the age of onset of the symptoms of dementia with Lewy bodies (DLB) is younger than in Parkinson’s disease dementia (PDD) and the rate of progression/duration of disease is slightly faster in dementia with Lewy bodies (DLB) 15.
- Sex. Lewy body dementia affects more men than women.
- Family history. Those who have a family member with Lewy body dementia or Parkinson’s disease are at greater risk. Mutations in over a dozen genes have been shown to “cause” Parkinson’s disease 16. Individuals with such rare genetic variants have a very high risk of developing Parkinson’s disease during their lifetime, and many of them will later develop dementia. Mutations in one of these genes (SNCA) can occasionally result in a clinical picture that resembles dementia with Lewy bodies (DLB) 17. However, no more than 2% of patients with Parkinson’s disease, and likely even fewer with dementia with Lewy bodies (DLB), carry a disease-causing mutation in a known gene. In most instances Parkinson’s disease and dementia with Lewy bodies (DLB) are thought to arise through a complex interaction between common genetic and environmental factors, each one with a small-to-modest effect. Two important common genetic risk factors that have recently come to light are variants in the APOE and GBA genes. The
APOE ε4 allele has long been known to increase the risk of developing Alzheimer’s disease, but there is now strong evidence that it does the same for dementia with Lewy bodies (DLB) 18. Furthermore, patients with Parkinson’s disease who carry APOE ε4 have (on average) more severe cognitive problems 19. A number of variants in the GBA gene have been shown to increase risk for
both Parkinson’s disease and dementia with Lewy bodies (DLB) 20. In addition, patients with Parkinson’s disease who have one of these GBA variants have a more rapid cognitive decline and are more likely to develop dementia 21. Since mutations that cause Lewy body dementia are rare, and no treatments have been discovered to reverse the effects of known genetic risk factors, genetic testing is not currently recommended for routine screening. However, if a family has multiple individuals with Parkinson’s disease (with or without dementia) and/or dementia with Lewy bodies (DLB), it is reasonable to consider genetic testing for some or all of the known genes. The rationale for considering such testing would be to (1) confirm a diagnosis and (2) provide genetic counseling for family members, if the results are positive. These decisions need to be made carefully with family members and the individual’s healthcare provider. It is prudent to undergo pre- and post-testing counseling so that the individual fully understands the risks and benefits of learning about their genetic status. In addition, certain research centers at academic institutions and the National Institutes of Health are investigating genetic risk and are actively seeking people who would like to volunteer as research subjects. - Rapid eye movement (REM) sleep behavior disorder (RBD), a condition characterized by dream enactment, is a common risk factor for dementia with Lewy bodies (DLB), Parkinson’s disease and other synucleinopathies, often occurring many years before the onset of parkinsonism or cognitive impairment 22. Pre-Parkinson’s sleep behavior disorder is thought to increase the risk of cognitive impairment when the motor phase of Parkinson’s disease evolves, compared with Parkinson’s disease that has no REM sleep behavior disorder prodrome. Parkinson’s disease is a risk factor for developing dementia, since the majority of those with Parkinson’s disease will eventually suffer from cognitive impairment.
Lewy body dementia diagnosis
Lewy body dementia diagnosis is challenging because the order of symptom appearance, their relative severity and the combination of features present varies among individuals 3. Currently, the only way to definitively diagnose Lewy body dementia is with an autopsy 3.
A diagnosis of Lewy body dementia requires a progressive decline in your ability to think, as well as at least two of the following:
- Fluctuating alertness and thinking function
- Repeated visual hallucinations
- Parkinsonian symptoms
- REM sleep behavior disorder, in which people act out their dreams during sleep
Autonomic dysfunction, which involves instability in blood pressure and heart rate, poor regulation of body temperature, sweating, and related signs and symptoms, supports a Lewy body dementia diagnosis. So does sensitivity to antipsychotic drugs, particularly first-generation antipsychotics such as haloperidol (Haldol). Medications like haloperidol aren’t used for people with Lewy body dementia because they can cause a severe reaction.
Clinicians and researchers use the “1-year rule” to diagnose which form of Lewy body dementia a person has. If cognitive symptoms appear within a year of movement problems, the diagnosis is dementia with Lewy bodies (DLB). If cognitive problems develop more than a year after the onset of movement problems, the diagnosis is Parkinson’s disease dementia (PDD).
No single test can diagnose Lewy body dementia. The diagnosis is based the on signs and symptoms you have and ruling out other conditions that can cause similar signs and symptoms. Tests might include:
- Neurological and physical examination
- Your doctor may check for signs of Parkinson’s disease, strokes, tumors or other medical conditions that can affect the brain and physical function. A neurological examination tests:
- Reflexes
- Strength
- Walking
- Muscle tone
- Eye movements
- Balance
- Sense of touch
- Your doctor may check for signs of Parkinson’s disease, strokes, tumors or other medical conditions that can affect the brain and physical function. A neurological examination tests:
- Assessment of mental abilities
- A short form of this test, which assesses your memory and thinking skills, can be done in less than 10 minutes in your doctor’s office. It’s not generally useful in distinguishing Lewy body dementia from Alzheimer’s disease but can determine whether cognitive impairment is present. Longer tests that take several hours help identify Lewy body dementia.
- Blood tests
- These can rule out physical problems that can affect brain function, such as vitamin B-12 deficiency or an underactive thyroid gland.
- Brain scans
- Your doctor might order an MRI or CT scan to identify a stroke or bleeding and to rule out a tumor. While dementias are diagnosed based on the medical history and physical examination, certain features on imaging studies can suggest different types of dementia, such as Alzheimer’s or Lewy body dementia.
- If the diagnosis is unclear or the signs and symptoms aren’t typical, your doctor might suggest additional imaging tests, including these that can support a diagnosis of Lewy body dementia:
- Fluorodeoxyglucose PET brain scans, which assess brain function.
- Single-photon emission computerized tomography (SPECT) or PET imaging, which can determine whether dopamine transporter uptake is reduced in the brain.
- Sleep evaluation
- Your doctor might order a sleep evaluation called a polysomnogram to check for REM sleep behavior disorder or an autonomic function test to look for signs of heart rate and blood pressure instability.
- Heart test
- In some countries, doctors might also order a heart test called myocardial scintigraphy to check the blood flow to your heart for indications of Lewy body dementia. However, the test isn’t used in the United States.
Emerging biomarkers
Research is ongoing into other indicators of Lewy body dementia. These biomarkers might eventually enable early diagnosis of Lewy body dementia before the full disease develops.
Talking to both patients and caregivers helps doctors make a diagnosis.
It is important for the patient and a close family member or friend to tell the doctor about any symptoms involving thinking, movement, sleep, behavior, or mood. Also, discuss other health problems and provide a list of all current medications, including prescriptions, over-the-counter drugs, vitamins, and supplements. Certain medications can worsen Lewy body dementia symptoms.
Caregivers may be reluctant to talk about a person’s symptoms when that person is present. Ask to speak with the doctor privately if necessary. The more information a doctor has, the more accurate a diagnosis can be.
Lewy body dementia treatment
Currently there’s no cure for Lewy body dementia but many of the symptoms can improve with targeted treatments.
Lewy body dementia medications
- Cholinesterase inhibitors or acetylcholinesterase inhibitors (AChEIs). These Alzheimer’s disease medications, such as rivastigmine (Exelon), donepezil (Aricept) and galantamine (Razadyne), work by increasing the levels of chemical messengers in the brain (neurotransmitters) believed to be important for memory, thought and judgment. This can help improve alertness and cognition and might reduce hallucinations and other behavioral problems. Possible side effects include gastrointestinal upset, muscle cramps and frequent urination. It can also increase the risk of certain cardiac arrhythmias. In some people with moderate or severe dementia, an N-methyl-d-aspartate (NMDA) receptor antagonist called memantine (Namenda) might be added to the cholinesterase inhibitor.
- Parkinson’s disease medications. These medications, such as carbidopa-levodopa (Sinemet, Rytary, Duopa) can help reduce parkinsonian signs and symptoms, such as rigid muscles and slow movement. However, these medications can also increase confusion, hallucinations and delusions.
- Medications to treat other symptoms. Your doctor might prescribe medications to treat other signs and symptoms associated with Lewy body dementia, such as sleep or movement problems.
Certain medications can worsen memory. Try to avoid over-the-counter sleep aids that contain diphenhydramine (Advil PM, Aleve PM) and medications used to treat urinary urgency such as oxybutynin (Ditropan XL).
Also limit sedatives and sleeping tablets, and talk to your doctor about whether any of the drugs you take might make your memory worse.
Antipsychotic drugs can cause severe confusion, severe parkinsonism, sedation and sometimes death. It is estimated that a high percentage of dementia with Lewy bodies (DLB) patients exhibit worsening parkinsonism, sedation, immobility, or even neuroleptic malignant syndrome (NMS) after exposure to antipsychotics. Neuroleptic malignant syndrome is a rare, life-threatening medical emergency characterized by fever, generalized rigidity and breakdown of muscle tissue that can cause renal failure and death. The heightened risk of neuroleptic malignant syndrome in dementia with Lewy bodies (DLB) mandates that typical or traditional antipsychotics (such as haloperidol, fluphenazine or thioridazine) should be avoided. Second-generation antipsychotics have been available for treating mental illness for 25 years and may be safer to use in patients with dementia with Lewy bodies (DLB), but only with extreme caution. Very rarely, certain second-generation antipsychotics, such as quetiapine (Seroquel) or clozapine (Clozaril, Versacloz) might be prescribed for a short time at a low dose but only if the benefits outweigh the risks. Patients with Parkinson’s disease dementia (PDD) appear to have a lower risk of an adverse reaction to antipsychotics, but all patients with Lewy body dementia should be carefully managed with any antipsychotic drug.
Medications to AVOID
- Anticholinergics, may worsen cognitive impairment, confusion, and hallucinations.
- Benzodiazepines are best avoided unless specifically indicated (e.g. clonazepam for REM sleep behavior disorder [RBD]), given their risk of sedation, increasing risk of falls, worsening cognition, and potentially paradoxical agitation.
- Inhaled anesthetics should be avoided when possible to minimize delirium and a decrease in functional ability.
- OTC sleep agents such as Tylenol or Advil PM and bladder-control medications may cause agitation. Many of these drugs contain diphenhydramine (Benadryl), an antihistamine with anticholinergic effects.
Cognitive symptoms
Medications called acetylcholinesterase inhibitors (AChEIs) or cholinesterase inhibitors are considered the standard treatment for cognitive and psychiatric symptoms in Lewy body dementia. These medications were developed to treat Alzheimer’s disease. However, some researchers believe that people with Lewy body dementia may be even more responsive to these types of medications than those with Alzheimer’s disease.
Three acetylcholinesterase inhibitors have been approved by the FDA for treatment of Alzheimer’s disease; donepezil (Aricept), rivastigmine (Exelon), and galantamine (Razadyne). Rivastigmine is the only one of the three that is FDA-approved for treating Lewy body dementia, specifically Parkinson’s disease dementia (PDD). The other two are used “off label.” There is no compelling
evidence that any one of the three is superior to the other two in treating Lewy body dementia 23.
Acetylcholinesterase inhibitors are generally well-tolerated by patients with Lewy body dementia, but not always. For example, in a study of rivastigmine in Parkinson’s disease dementia (PDD), approximately 10% of patients experienced worsening of tremor, but it was not usually clinically significant 24.
Memantine (Namenda) is another drug (with a different pharmacological mechanism of action) approved for Alzheimer’s disease but not Lewy body dementia and is also used off label as an add-on therapy to cholinesterase inhibitors, typically in patients with more severe dementia. Only a few studies of memantine have been done in Lewy body dementia, with mixed results 25, 26.
Movement symptoms
Movement symptoms may be treated with a Parkinson’s disease medication called levodopa, but if the symptoms are mild, it may be best to not treat them in order to avoid potential medication side-effects. Furthermore, most patients with Lewy body dementia respond with improvement in motor function, without side effects, as long as the dosing is kept at the lowest, most effective level 27. However, all patients with Lewy body dementia are vulnerable to the development of medication-induced behavioral or psychotic symptoms. Not everyone with Lewy body dementia requires anti-parkinsonian treatment, particularly those with dementia with Lewy bodies (DLB). In fact, some patients with dementia with Lewy bodies (DLB) may go years before showing signs of parkinsonism. Given the potential for adverse effects, healthcare providers should use levodopa in this setting only when symptoms are truly bothersome and should start with a low dose and titrate up slowly.
Dopamine agonists are less effective than levodopa for treating motor symptoms and are more likely to cause non-motor side effects, especially drug-induced psychosis even at low doses. Dopamine agonists may also cause excessive daytime sleepiness and swelling of the legs. Other Parkinson’s disease medications such as amantadine, COMT inhibitors, MAO inhibitors, and anticholinergics, likewise, can induce psychosis and exacerbate cognitive impairment and should be avoided in dementia with Lewy bodies (DLB). Furthermore, dementia is a contraindication to deep brain stimulation, even when the patient is an otherwise good candidate 28.
Behavioral changes
The overarching goal of managing psychotic and behavioral disturbances in Lewy body dementia is to improve outcome without compromising safety of the patient and others. If hallucinations (usually visual hallucinations) are not frightening to the patient, even if they are considered bothersome by the family, treatment with a drug may not be needed, especially if the patient understands that the hallucinations are not real. On the other hand, delusions (a false belief held with strong conviction despite evidence to the contrary), are often socially disruptive and in most cases, should be treated, most productively by a mental health professional.
The first line intervention should be non-pharmacologic measures including evaluation for acute physical ailments that may be provoking behavioral disturbances (e.g., fecal impaction, pain, decubitus ulcers, urinary tract infection and other febrile illnesses). Medications that can potentially cause agitation, especially those with anticholinergic properties, including amantadine, certain antidepressants, and those antihistamines with significant anticholinergic effects should be reviewed for need and stopped if possible. It may be necessary to reduce or discontinue all Parkinson’s disease medications other than low dose levodopa.
Behavioral medications to AVOID
- Typical antipsychotics (neuroleptics) should always be avoided in the management of patients with Lewy body dementia, especially dementia with Lewy bodies (DLB), who risk severe worsening of all symptoms, and, as mentioned above, may develop potentially fatal neuroleptic malignant syndrome (NMS) 29.
- Atypical antipsychotics, especially those with high D2 receptor antagonism (such as olanzapine and risperidone), should also be avoided due to the risk of severe neuroleptic sensitivity reactions, neuroleptic malignant syndrome, worsening parkinsonism, somnolence and orthostatic hypotension 30. Quetiapine and clozapine are two from this class of drugs that have been shown to be well tolerated in low doses for treatment of psychosis
- Benzodiazepines and benzodiazepine-like sedative hypnotic medications (such as zolpidem) should not be first-line agents given their risk of sedation and paradoxical agitation. (One exception is clonazepam at night for management of REM sleep behavior disorder.)
- Opiates or tramadol should be avoided; alternatives for pain management include nonsteroidal anti-inflammatory agents and acetaminophen.
Acetylcholinesterase inhibitor for behavioral symptoms
Deficits in the brain’s supply of the neurotransmitter acetylcholine probably contribute to cognitive impairment and psychosis in Lewy body dementia. Visual hallucinations may predict a favorable response to treatment with an acetylcholinesterase inhibitor. By comparison, a meta-analysis of 6 large trials in Alzheimer’s disease, which also causes depletion of acetylcholine in the brain, showed a small but significant benefit of acetylcholinesterase inhibitor treatment in decreasing neuropsychiatric symptoms. Moreover, acetylcholinesterase inhibitors may selectively reduce psychosis and anxiety compared with other psychiatric symptoms.
A few published reports have shown behavioral improvement in patients with Lewy body dementia treated with the acetylcholinesterase inhibitor rivastigmine. In a large multicenter trial, rivastigmine resulted in improvement by 30% from baseline in psychiatric symptoms 31. In a comparator study of rivastigmine in patients with clinical diagnoses of dementia with Lewy bodies (DLB) and Alzheimer’s disease, treatment was associated with improvement in hallucinations, anxiety, and sleep disturbances only in the dementia with Lewy bodies (DLB) group 32.
Atypical antipsychotics
If long-term treatment with acetylcholinesterase inhibitors is ineffective, or more acute symptom control of behavior is required, it may be difficult to avoid a cautious trial of an atypical antipsychotic. When medications are needed to modify behaviors, they should be used for the shortest duration possible. Quetiapine and clozapine are preferred when psychosis warrants drug treatment.
- Clozapine has been demonstrated to be effective for Parkinson’s disease psychosis in several randomized clinical trials. However, due to the infrequent but serious risk of potentially fatal agranulocytosis (severe depression of white blood cells), and the corresponding need for intrusively frequent blood monitoring to prevent such a reaction, clozapine is not the drug of first choice.
- Quetiapine is a safer alternative atypical antipsychotic in Parkinson’s disease dementia (PDD) and dementia with Lewy bodies (DLB), typically in the dose range of 6.25 mg to 50 mg a day, although higher doses may be used if tolerated and necessary.
As with any drug in this setting the low slow approach is required. Pimavanserin, now FDA-approved for the treatment of psychosis in Parkinson’s disease 33, has not yet been studied in dementia with Lewy bodies (DLB).
Black box warning
The FDA’s ‘black box warning’ indicates both typical and atypical antipsychotics are associated with an increased risk of mortality and morbidity in elderly patients with dementia-related psychosis. However, if used carefully according to the guidelines mentioned above, the risk of mortality is extremely low. Physicians should discuss the risks and benefits of these types of medications, so that patients with Lewy body dementia and caregivers can weigh the impact of the symptoms against the potential risks associated with these medications.
REM Sleep Behavior Disorder (RBD) and insomnia
Clonazepam has been the mainstay of medical therapy for REM sleep behavior disorder (RBD) 34. Melatonin is a safe, over-the-counter natural substance that may also offer benefit either as monotherapy without risk or in conjunction with clonazepam.
For insomnia, treatment can be attempted with antidepressants (such as trazodone or mirtazapine), low doses of benzodiazepines (such as clonazepam) or specific sedative-hypnotic agents (such as zolpidem). These medications have not been extensively studied in Lewy body dementia, and worsening confusion and daytime sedation is a potential side effect of sedative-hypnotics, such as zolpidem.
Autonomic dysfunction symptoms
Orthostatic hypotension (drop in blood pressure) is a common manifestation of Lewy body dementia, often presenting as lightheadedness or fainting, mainly when standing. Initial management consists of simple measures such as arising slowly from a reclining or seated position, leg elevation when sitting, elastic stockings, increasing salt and fluid intake, and if possible avoiding medications that are known to exacerbate orthostasis. If simple measures fail, medications such as midodrine, fludrocortisone or the more-recently-approved droxidopa can be used.
Medications with anticholinergic activity, such as oxybutynin, tolterodine tartrate, bethanechol chloride, and propantheline, can be used to treat urinary urgency, frequency and urge incontinence. They should be used cautiously however, given their risk of exacerbating cognitive problems because of their anticholinergic properties.
Constipation can usually be treated by exercise and modifications of the daily diet to include foods with high fiber content (fruits and vegetables) and bran cereal. Laxatives, stool softeners and mechanical disimpaction may be needed.
Erectile dysfunction (ED), loss of libido and impotence in Lewy body dementia is likely multifactorial. While autonomic dysfunction is a possible cause, other factors often contribute, such as depression, poor bed mobility, pain and co-morbid illnesses. Treatment can be complex, requiring a urologic and/or psychiatric consultation. Medications for erectile dysfunction include three inhibitors of phosphodiesterase-5 (sildenafil [Viagra], tadalfil [Cialis], and vardenafil [Levitra]), the natural substance yohimbine, or the intracavernal injectables phentolamine and prostaglandid E. If immobility in bed is a major problem, a bedtime dose of levodopa is worth a try. If mood disturbances are associated with sexual dysfunction, psychotherapy or a trial of an antidepressant can be considered, although antidepressants often cause erectile dysfunction.
Lewy body dementia therapies
Because antipsychotic drugs can worsen Lewy body dementia symptoms, it might be helpful to first try nondrug approaches, such as:
- Tolerating the behavior. Some people with Lewy body dementia aren’t distressed by the hallucinations. In these cases, the side effects of medication might be worse than the hallucinations themselves.
- Modifying the environment. Reducing clutter and noise can make it easier for someone with dementia to function. Caregivers’ responses sometimes worsen behavior. Avoid correcting and quizzing a person with dementia. Offer reassurance and validation of his or her concerns.
- Creating daily routines and keeping tasks simple. Break tasks into easier steps and focus on successes, not failures. Structure and routine during the day can be less confusing.
Alternative medicine
Frustration and anxiety can worsen dementia symptoms. To promote relaxation, consider:
- Music therapy, which involves listening to soothing music
- Pet therapy, which involves the use of animals to improve moods and behaviors in people with dementia
- Aromatherapy, which uses fragrant plant oils
- Massage therapy
Lewy body dementia home remedies
Symptoms and progression are different for everyone with Lewy body dementia. Caregivers and care partners may need to adapt the following tips to individual situations:
- Speak clearly and simply. Maintain eye contact and speak slowly, in simple sentences, and don’t rush the response. Present only one idea or instruction at a time. Use gestures and cues, such as pointing to objects.
- Encourage exercise. Benefits of exercise include improvements in physical function, behavior and depression. Some research shows exercise might slow cognitive decline in people with dementia.
- Provide mind stimulation. Participating in games, crossword puzzles and other activities that involve thinking skills might help slow mental decline in people with dementia. Encourage artistic and creative activities, such as painting, singing or making music.
- Create opportunities for social activity. Talk to friends. Participate in religious services.
- Establish bedtime rituals. Behavior issues can worsen at night. Create calming bedtime rituals without the distraction of television, meal cleanup and active family members. Leave night lights on to prevent disorientation.
Limiting caffeine during the day, discouraging daytime napping and offering opportunities for daytime exercise might help prevent nighttime restlessness.
Vitamins and Supplements
The use of vitamins and supplements to treat Lewy body dementia symptoms has not been studied extensively and is not recommended as part of standard treatment. Vitamins and supplements can be dangerous when taken with other medicines. People with Lewy body dementia should tell their doctors about every medication they take. Be sure to list prescription and over-the-counter medicines, as well as vitamins and supplements.
Lewy body dementia coping and support
People with Lewy body dementia often have a mixture of emotions, such as confusion, frustration, anger, fear, uncertainty, grief and depression. Offer support by listening, reassuring the person that he or she still can enjoy life, being positive, and doing your best to help the person retain dignity and self-respect.
If you’re a caregiver or care partner for someone with Lewy body dementia, watch the person closely to make sure he or she doesn’t fall, lose consciousness or react negatively to medications. Provide reassurance during times of confusion, delusions or hallucinations.
Looking after yourself
Caring for a person with Lewy body dementia can be exhausting physically and emotionally. You may have anger, guilt, frustration, discouragement, worry, grief or social isolation. Help prevent caregiver burnout by:
- Asking friends or other family members for help when you need it. Consider in-home health services to help you care for the person with Lewy body dementia.
- Exercising regularly and eating a healthy diet.
- Learning about the disease. Ask questions of doctors, social workers and others on the care team.
- Joining a support group.
Many people with Lewy body dementia and their families can benefit from counseling or local support groups. Contact your local agencies on health or aging to get connected with support groups, doctors, resources, referrals, home care agencies, supervised living facilities, a telephone help line and educational seminars.
Non-Medical Treatments
Physical therapy options include cardiovascular, strengthening, and flexibility exercises, as well as gait training. Physicians may also recommend general physical fitness programs such as aerobic, strengthening, or water exercise.
Speech therapy may be helpful for low voice volume and poor enunciation. Speech therapy may also improve muscular strength and swallowing difficulties.
Occupational therapy may help maintain skills and promote function and independence. In addition to these forms of therapy and treatment, music and aroma therapy can also reduce anxiety and improve mood.
Individual and family psychotherapy can be useful for learning strategies to manage emotional and behavioral symptoms and to help make plans that address individual and family concerns about the future.
Support groups may be helpful for caregivers and persons with Lewy body dementia to identify practical solutions to day-to-day frustrations, and to obtain emotional support from others.
Lewy body dementia prognosis
Like Alzheimer’s disease and Parkinson’s disease, Lewy body dementia is a neurodegenerative disorder that results in progressive intellectual and functional deterioration. There are no known therapies to stop or slow the progression of Lewy body dementia. Average survival after the time of diagnosis is similar to that in Alzheimer’s disease, about 8 years, with progressively increasing disability. It is possible, though, for the time span to be anywhere from 2 to 20 years, depending on several factors, including the person’s overall health, age and severity of symptoms.
Defining the stages of disease progression for Lewy body dementia is difficult. The symptoms, medicine management and duration of Lewy body dementia vary greatly from person to person. To further complicate the stages assessment, Lewy body dementia has a progressive but vacillating clinical course, and one of its defining symptoms is fluctuating levels of cognitive abilities, alertness and attention. Sudden decline is often caused by medications, infections or other compromises to the immune system and usually the person with Lewy body dementia returns to their baseline upon resolution of the problem. But for some individuals, it may also be due to the natural course of the disease.
Advice for People Living with Lewy Body Dementia
Coping with a diagnosis of Lewy body dementia and all that follows can be challenging. Getting support from family, friends, and professionals is critical to ensuring the best possible quality of life. Creating a safe environment and preparing for the future are important, too. Take time to focus on your strengths, enjoy each day, and make the most of your time with family and friends. Here are some ways to live with Lewy body dementia day to day.
Building a Care Team
After receiving a diagnosis, a person with Lewy body dementia may benefit from seeing a neurologist who specializes in dementia and/or movement disorders. A good place to find an Lewy body dementia specialist is at a dementia or movement disorders clinic in an academic medical center in your community. If such a specialist cannot be found, a general neurologist should be part of the care team. Ask a primary care physician for a referral.
Depending on an individual’s particular symptoms, other professionals may also be helpful:
- Physical therapists can help with movement problems through cardiovascular, strengthening, and flexibility exercises, as well as gait training and general physical fitness programs.
- Speech therapists may help with low voice volume, voice projection, and swallowing difficulties.
- Occupational therapists help identify ways to more easily carry out everyday activities, such as eating and bathing, to promote independence.
- Music or expressive arts therapists may provide meaningful activities that can reduce anxiety and improve well-being.
- Mental health counselors can help people with Lewy body dementia and their families learn how to manage difficult emotions and behaviors and plan for the future.
- Palliative care specialists can help improve a person’s quality of life by relieving disease symptoms at any stage of illness.
Support groups are another valuable resource for both people with Lewy body dementia and caregivers. Sharing experiences and tips with others in the same situation can help people identify practical solutions to day-to-day challenges and get emotional and social support.
Getting Help
Your family and close friends are likely aware of changes in your thinking, movement, or behavior. You may want to tell others about your diagnosis so they can better understand the reason for these changes and learn more about Lewy body dementia. For example, you could say that you have been diagnosed with a brain disorder called Lewy body dementia, which can affect thinking, movement, and behavior. You can say that you will need more help over time. By sharing your diagnosis with those closest to you, you can build a support team to help you manage Lewy body dementia.
As Lewy body dementia progresses, you will likely have more trouble managing everyday tasks such as taking medication, paying bills, and driving. You will gradually need more assistance from family members, friends, and perhaps professional caregivers. Although you may be reluctant to get help, try to let others partner with you so you can manage responsibilities together. Remember, Lewy body dementia affects your loved ones, too. You can help reduce their stress when you accept their assistance.
Finding someone you can talk with about your diagnosis—a trusted friend or family member, a mental health professional, or a spiritual advisor—may be helpful.
Consider Safety
The changes in thinking and movement that occur with Lewy body dementia require attention to safety issues. Consider these steps:
- Fill out and carry the Lewy body dementia Medical Alert Wallet Card and present it any time you are hospitalized, require emergency medical care, or meet with your doctors. It contains important information about medication sensitivities.
- Consider subscribing to a medical alert service, in which you push a button on a bracelet or necklace to access an emergency phone line if you need emergency help.
- Address safety issues in your home, including areas of fall risk, poor lighting, stairs, or cluttered walkways. Think about home modifications that may be needed, such as installing grab bars in the bathroom or modifying stairs with ramps. Ask your doctor to refer you to a home health agency for a home safety evaluation.
- Talk with your doctor about Lewy body dementia and driving, and have your driving skills evaluated, if needed.
Plan for Your Future
There are many ways to plan ahead. Here are some things to consider:
- If you are working, consult with a legal and financial expert about planning for disability leave or retirement. Symptoms of Lewy body dementia will interfere with work performance over time, and it is essential to plan now to obtain benefits you are entitled to.
- Consult with an attorney who specializes in elder law or estate planning to help you write or update important documents, such as a living will, healthcare power of attorney, and will.
- Identify local resources for home care, meals, and other services before you need them so you know whom to call when the time comes.
- Explore moving to a retirement or continuing care community where activities and varying levels of care can be provided over time, as needed. Ask about staff members’ experience caring for people with Lewy body dementia.
Find Enjoyment Every Day
It is important to focus on living with Lewy body dementia. Your attitude can help you find enjoyment in daily life. Despite the many challenges and adjustments, you can have moments of humor, tenderness, and gratitude with the people closest to you.
Make a list of events and activities you can still enjoy—then find a way to do them! For example, listening to music, exercising, or going out for a meal allows you to enjoy time with family and friends. If you can’t find pleasure in daily life, consult your doctor or another healthcare professional to discuss effective ways to cope and move forward. Let your family know if you are struggling emotionally so they can offer support.
- National Institutes of Health. National Institute on Aging. What Is Lewy Body Dementia ? https://www.nia.nih.gov/health/what-lewy-body-dementia[↩][↩][↩][↩][↩][↩]
- Genetic and Rare Diseases Information Center. Lewy body dementia. https://rarediseases.info.nih.gov/diseases/3243/lewy-body-dementia[↩]
- Diagnosing and Managing Lewy Body Dementia. A Comprehensive Guide for Healthcare Professionals. https://www.lbda.org/wp-content/uploads/2011/02/3737-lbda-physicians-book-22dec17.pdf[↩][↩][↩][↩][↩]
- Lewy Body Dementia Association. 10 Things You Should Know about LBD. https://www.lbda.org/content/10-things-you-should-know-about-lbd[↩][↩]
- The National Institute of Neurological Disorders and Stroke. Dementia With Lewy Bodies Information Page. https://www.ninds.nih.gov/Disorders/All-Disorders/Dementia-Lewy-Bodies-Information-Page[↩]
- NINDS Dementia With Lewy Bodies Information Page. National Institute of Neurological Disorders and Stroke (NINDS). November 2015; http://www.ninds.nih.gov/disorders/dementiawithlewybodies/dementiawithlewybodies.htm.[↩]
- Howard A Crystal, MD. Dementia With Lewy Bodies. Medscape Reference. April 2014; http://emedicine.medscape.com/article/1135041-overview#a4.[↩]
- U.S. National Library of Medicine. MedlinePlus. Lewy Body Disease. https://medlineplus.gov/lewybodydisease.html[↩]
- McKeith, I. G., Boeve, B. F., Dickson, D. W., Halliday, G., Taylor, J. P., Weintraub, D., Aarsland, D., Galvin, J., Attems, J., Ballard, C. G., Bayston, A., Beach, T. G., Blanc, F., Bohnen, N., Bonanni, L., Bras, J., Brundin, P., Burn, D., Chen-Plotkin, A., Duda, J. E., … Kosaka, K. (2017). Diagnosis and management of dementia with Lewy bodies: Fourth consensus report of the DLB Consortium. Neurology, 89(1), 88–100. https://doi.org/10.1212/WNL.0000000000004058[↩][↩]
- Barker WW, Luis CA, Kashuba A, Luis M, Harwood DG, Loewenstein D, Waters C, Jimison P, Shepherd E, Sevush S, Graff-Radford N, Newland D, Todd M, Miller B, Gold M, Heilman K, Doty L, Goodman I, Robinson B, Pearl G, Dickson D, Duara R. Relative frequencies of Alzheimer disease, Lewy body, vascular and frontotemporal dementia, and hippocampal sclerosis in the State of Florida Brain Bank. Alzheimer Dis Assoc Disord. 2002 Oct-Dec;16(4):203-12. doi: 10.1097/00002093-200210000-00001[↩]
- National Institutes of Health. National Institute on Aging. Symptoms of Lewy Body Dementia. https://www.nia.nih.gov/health/symptoms-lewy-body-dementia[↩][↩]
- Lewy Body Dementia Association, DLB and PDD Diagnostic Criteria. http://www.lbda.org/node/470[↩]
- Haider A, Spurling BC, Sánchez-Manso JC. Lewy Body Dementia. [Updated 2021 Jul 12]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482441[↩]
- Osterberg, V. R., Spinelli, K. J., Weston, L. J., Luk, K. C., Woltjer, R. L., & Unni, V. K. (2015). Progressive aggregation of alpha-synuclein and selective degeneration of lewy inclusion-bearing neurons in a mouse model of parkinsonism. Cell reports, 10(8), 1252–1260. https://doi.org/10.1016/j.celrep.2015.01.060[↩]
- Savica, R., Grossardt, B. R., Bower, J. H., Boeve, B. F., Ahlskog, J. E., & Rocca, W. A. (2013). Incidence of dementia with Lewy bodies and Parkinson disease dementia. JAMA neurology, 70(11), 1396–1402. https://doi.org/10.1001/jamaneurol.2013.3579[↩]
- Kim CY, Alcalay RN. Genetic Forms of Parkinson’s Disease. Semin Neurol. 2017 Apr;37(2):135-146. doi: 10.1055/s-0037-1601567[↩]
- Zarranz JJ, Alegre J, Gómez-Esteban JC, Lezcano E, Ros R, Ampuero I, Vidal L, Hoenicka J, Rodriguez O, Atarés B, Llorens V, Gomez Tortosa E, del Ser T, Muñoz DG, de Yebenes JG. The new mutation, E46K, of alpha-synuclein causes Parkinson and Lewy body dementia. Ann Neurol. 2004 Feb;55(2):164-73. doi: 10.1002/ana.10795[↩]
- Bras, J., Guerreiro, R., Darwent, L., Parkkinen, L., Ansorge, O., Escott-Price, V., Hernandez, D. G., Nalls, M. A., Clark, L. N., Honig, L. S., Marder, K., Van Der Flier, W. M., Lemstra, A., Scheltens, P., Rogaeva, E., St George-Hyslop, P., Londos, E., Zetterberg, H., Ortega-Cubero, S., Pastor, P., … Hardy, J. (2014). Genetic analysis implicates APOE, SNCA and suggests lysosomal dysfunction in the etiology of dementia with Lewy bodies. Human molecular genetics, 23(23), 6139–6146. https://doi.org/10.1093/hmg/ddu334[↩]
- Mata, Ignacio F et al. “APOE, MAPT, and SNCA genes and cognitive performance in Parkinson disease.” JAMA neurology vol. 71,11 (2014): 1405-12. https://doi.org/10.1001/jamaneurol.2014.1455[↩]
- Nalls, M. A., Duran, R., Lopez, G., Kurzawa-Akanbi, M., McKeith, I. G., Chinnery, P. F., Morris, C. M., Theuns, J., Crosiers, D., Cras, P., Engelborghs, S., De Deyn, P. P., Van Broeckhoven, C., Mann, D. M., Snowden, J., Pickering-Brown, S., Halliwell, N., Davidson, Y., Gibbons, L., Harris, J., … Sidransky, E. (2013). A multicenter study of glucocerebrosidase mutations in dementia with Lewy bodies. JAMA neurology, 70(6), 727–735. https://doi.org/10.1001/jamaneurol.2013.1925[↩]
- Davis, M. Y., Johnson, C. O., Leverenz, J. B., Weintraub, D., Trojanowski, J. Q., Chen-Plotkin, A., Van Deerlin, V. M., Quinn, J. F., Chung, K. A., Peterson-Hiller, A. L., Rosenthal, L. S., Dawson, T. M., Albert, M. S., Goldman, J. G., Stebbins, G. T., Bernard, B., Wszolek, Z. K., Ross, O. A., Dickson, D. W., Eidelberg, D., … Zabetian, C. P. (2016). Association of GBA Mutations and the E326K Polymorphism With Motor and Cognitive Progression in Parkinson Disease. JAMA neurology, 73(10), 1217–1224. https://doi.org/10.1001/jamaneurol.2016.2245[↩]
- Boeve BF, Silber MH, Saper CB, Ferman TJ, Dickson DW, Parisi JE, Benarroch EE, Ahlskog JE, Smith GE, Caselli RC, Tippman-Peikert M, Olson EJ, Lin SC, Young T, Wszolek Z, Schenck CH, Mahowald MW, Castillo PR, Del Tredici K, Braak H. Pathophysiology of REM sleep behaviour disorder and relevance to neurodegenerative disease. Brain. 2007 Nov;130(Pt 11):2770-88. doi: 10.1093/brain/awm056[↩]
- Bhasin M, Rowan E, Edwards K, McKeith I. Cholinesterase inhibitors in dementia with Lewy bodies: a comparative analysis. Int J Geriatr Psychiatry. 2007 Sep;22(9):890-5. doi: 10.1002/gps.1759[↩]
- Emre M, Aarsland D, Albanese A, Byrne EJ, Deuschl G, De Deyn PP, Durif F, Kulisevsky J, van Laar T, Lees A, Poewe W, Robillard A, Rosa MM, Wolters E, Quarg P, Tekin S, Lane R. Rivastigmine for dementia associated with Parkinson’s disease. N Engl J Med. 2004 Dec 9;351(24):2509-18. doi: 10.1056/NEJMoa041470[↩]
- Wang HF, Yu JT, Tang SW, Jiang T, Tan CC, Meng XF, Wang C, Tan MS, Tan L. Efficacy and safety of cholinesterase inhibitors and memantine in cognitive impairment in Parkinson’s disease, Parkinson’s disease dementia, and dementia with Lewy bodies: systematic review with meta-analysis and trial sequential analysis. J Neurol Neurosurg Psychiatry. 2015 Feb;86(2):135-43. doi: 10.1136/jnnp-2014-307659[↩]
- Stinton C, McKeith I, Taylor JP, Lafortune L, Mioshi E, Mak E, Cambridge V, Mason J, Thomas A, O’Brien JT. Pharmacological Management of Lewy Body Dementia: A Systematic Review and Meta-Analysis. Am J Psychiatry. 2015 Aug 1;172(8):731-42. doi: 10.1176/appi.ajp.2015.14121582[↩]
- Goldman JG, Goetz CG, Brandabur M, Sanfilippo M, Stebbins GT. Effects of dopaminergic medications on psychosis and motor function in dementia with Lewy bodies. Mov Disord. 2008 Nov 15;23(15):2248-50. doi: 10.1002/mds.22322[↩]
- Rothlind JC, York MK, Carlson K, Luo P, Marks WJ Jr, Weaver FM, Stern M, Follett K, Reda D; CSP-468 Study Group. Neuropsychological changes following deep brain stimulation surgery for Parkinson’s disease: comparisons of treatment at pallidal and subthalamic targets versus best medical therapy. J Neurol Neurosurg Psychiatry. 2015 Jun;86(6):622-9. doi: 10.1136/jnnp-2014-308119[↩]
- McKeith, I., Fairbairn, A., Perry, R., Thompson, P., & Perry, E. (1992). Neuroleptic sensitivity in patients with senile dementia of Lewy body type. BMJ (Clinical research ed.), 305(6855), 673–678. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1882909/pdf/bmj00092-0017.pdf[↩]
- Culo S, Mulsant BH, Rosen J, Mazumdar S, Blakesley RE, Houck PR, Pollock BG. Treating neuropsychiatric symptoms in dementia with Lewy bodies: a randomized controlled-trial. Alzheimer Dis Assoc Disord. 2010 Oct-Dec;24(4):360-4. doi: 10.1097/WAD.0b013e3181e6a4d7[↩]
- McKeith I, Del Ser T, Spano P, Emre M, Wesnes K, Anand R, Cicin-Sain A, Ferrara R, Spiegel R. Efficacy of rivastigmine in dementia with Lewy bodies: a randomised, double-blind, placebo-controlled international study. Lancet. 2000 Dec 16;356(9247):2031-6. doi: 10.1016/S0140-6736(00)03399-7[↩]
- Rozzini L, Chilovi BV, Bertoletti E, Conti M, Delrio I, Trabucchi M, Padovani A. Cognitive and psychopathologic response to rivastigmine in dementia with Lewy bodies compared to Alzheimer’s disease: a case control study. Am J Alzheimers Dis Other Demen. 2007 Feb-Mar;22(1):42-7. doi: 10.1177/1533317506297517[↩]
- Cummings J, Isaacson S, Mills R, Williams H, Chi-Burris K, Corbett A, Dhall R, Ballard C. Pimavanserin for patients with Parkinson’s disease psychosis: a randomised, placebo-controlled phase 3 trial. Lancet. 2014 Feb 8;383(9916):533-40. doi: 10.1016/S0140-6736(13)62106-6. Epub 2013 Nov 1. Erratum in: Lancet. 2014 Jul 5;384(9937):28.[↩]
- Aurora, R. N., Zak, R. S., Maganti, R. K., Auerbach, S. H., Casey, K. R., Chowdhuri, S., Karippot, A., Ramar, K., Kristo, D. A., Morgenthaler, T. I., Standards of Practice Committee, & American Academy of Sleep Medicine (2010). Best practice guide for the treatment of REM sleep behavior disorder (RBD). Journal of clinical sleep medicine : JCSM : official publication of the American Academy of Sleep Medicine, 6(1), 85–95. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2823283[↩]





{kind=link}