Liver abscess
Liver abscess also known as hepatic abscess, is a localized encapsulated collection of necrotic inflammatory tissue or pus within the liver parenchyma caused by bacterial, parasitic or fungal agents entering directly from an injury through the blood vessels or by the way of the biliary ductal system 1. The usual pathophysiology for pyogenic liver abscesses is bowel content leakage and peritonitis. Bacteria travel to the liver via the portal vein and resides there. Infection can also originate in the biliary system. Hematogenous spreading is also possible 2. Liver abscesses are most commonly due to pyogenic, amebic or mixed infections 3. The pyogenic abscesses are usually polymicrobial, but some organisms are seen more commonly in them; such as E.coli, Klebsiella, Streptococcus, Staphylococcus, and anaerobes 2. Less commonly hepatic abscess may be fungal in origin. The majority of liver abscesses in the Western world are infected with bacteria 4. In developing countries, parasitic liver abscesses are the most common 5. Most amoebic infections are caused by Entamoeba histolytica 2.
The usual pattern of hepatic abscess formation is that there is leakage of bowel in the abdomen that will travel to the liver through the portal vein. Many cases have an infected biliary tract that will cause an abscess via direct contact.
The annual incidence rate is about 2.3 cases per 100,000 people. Males are more frequently affected than females 6. Age plays a factor in the type of abscess one develops. People aged 40-60 years are more vulnerable to developing liver abscess that does not result from trauma.
Liver abscesses can be classified in a variety of ways: One is by location in the liver. 50% of solitary liver abscesses occur in the right liver lobe (a more significant part with more blood supply); less commonly in the left liver lobe or caudate lobe. Another method is by considering the source. Liver abscesses can be divided into three main categories based on the underlying conditions 1:
- Infectious: the majority of liver abscesses can be classified into bacterial (including amebic) and parasitic sources (including hydatiform cyst).
- Malignant,
- Iatrogenic.
Infectious abscesses include those secondary to direct extension from local infection, systemic bacteremia, and intra-abdominal infections that seed the portal system. However, over the years, the causes and risks factors for liver abscess have continued to evolve. Prompt recognition is important for instituting effective management and obtaining good outcomes 7.
Hepatic abscesses can occur via different routes such as 8:
- Hematogenous spread of infection via the portal vein or hepatic arteries
- Biliary spread of infection from ascending cholangitis or cholecystitis
- Direct inoculation in the setting of penetrating trauma or iatrogenic following a procedure
The typical symptoms of liver abscess is one of right upper quadrant pain, fever and jaundice. Anorexia, malaise and weight loss are also frequently seen. Depending on the immune status of the patient, and the organism involved, the presentation may be dramatic or insidious.
Drainage of liver abscess and antibiotic treatment are the cornerstone of treatments. Medical antimicrobial therapy is required in all cases and sometimes suffices if abscesses are small.
Radiology has a major role to play in the percutaneous drainage of hepatic abscesses, which can be performed either under ultrasound or CT guidance.
Surgery is limited to those patients where percutaneous drainage is impossible or has proven ineffective. Additionally, the source of the abscess may require surgical treatment at which time the abscess may also be drained.
Prognosis is highly variable, depending not only on the organism involved and size of the abscess but also the co-morbidities present. In-hospital mortality is estimated at 2.5% to 19% 9. The mortality rate is higher in elderly, ICU admissions, shock, cancer, fungal infections, cirrhosis, chronic renal failure, acute respiratory failure, severe disease, and biliary origin of an abscess. The most common causes of death include sepsis, multiorgan failure, and hepatic failure 10.
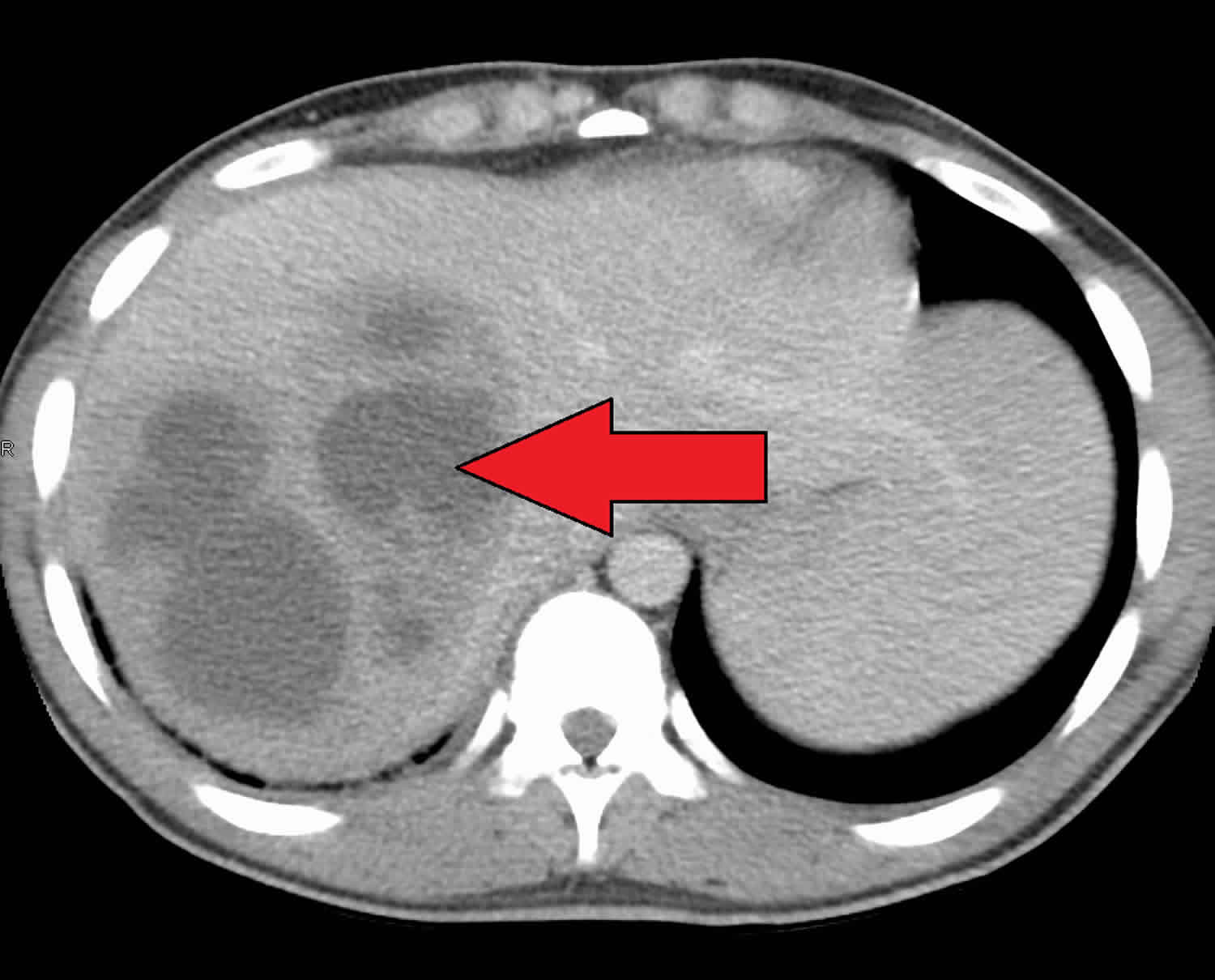
Figure 1. Liver abscess ultrasound

Footnote: Liver abscess rupture in pleural space. There is hepatic abscess in right lobe of liver. Defect is noted in right hemidiaphragm. Right pleural space collection is noted.
[Source 11 ]Liver abscess causes
Appendicitis used to be the main reason why people develop liver abscess but that has decreased to less than 10 % since better diagnosis and management of the disease has been available 2. Nowadays, biliary tract disease (biliary stone, strictures, malignancy and congenital anomalies) are the major causes of pyogenic liver abscesses 2.
Half of the bacterial cases are developed by cholangitis. Less often causes are hepatic artery bacteremia, portal vein bacteremia, diverticulitis, cholecystitis, or penetrating trauma 12. Some may be from a cryptogenic origin. The most common organisms include E.coli, Klebsiella, Streptococcus, Staphylococcus and anaerobic organisms but are generally polymicrobial. If strep or staph is isolated solely, the focus is to find another source of infection (endocarditis) that has hematogenously spread to the liver. Klebsiella pneumoniae is a prominent etiology in Southeast Asia and is thought to be related to or associated with colorectal cancer there as well 13. It is usually present with no hepatobiliary system disease and is exclusively monomicrobial. It happens in a background of diabetes and is more severe than other forms of bacterial abscesses, possibly because of enhanced virulence factors of the bacteria 14.
If the source is anaerobe, the most common organism is Entamoeba histolytica. It affects liver by first causing amebic colitis then seeding the portal system and migrating to the liver and causing an amebic liver abscess. Although rare in the United States, it can still be found in immigrants or travelers from other countries.
Another rare but important parasitic origin organism is Echinococcus granulosus, which causes hydatid cyst of the liver. Infection is caused by the metacestode stage of the tapeworm Echinococcus which is part of the Taeniidae family. Patients typically present with symptoms that include abdominal pain, diarrhea, and hepatomegaly. Hydatid cysts are acquired from dog saliva and can take a while to cause symptoms in the host. Most cases are discovered in the late stages and incidentally 15.
Risk factors for liver abscess
In developed countries, bacterial liver abscesses are most common, usually in the setting of comorbidities such as:
- Infection elsewhere (most common)
- abdominal sepsis most common 16
- necrotizing enterocolitis (portal venous drainage)
- Immunocompromised
- Intravenous drug use
- Trauma
- Endoscopic retrograde cholangiopancreatography (ERCP) 18
- Cryptogenic: 15% 16
- Liver cirrhosis 19
- Biliary disease 20
- Inflammatory bowel disease 21
- Pancreatic disease 22
Liver abscess symptoms
The most frequent symptoms of liver abscess include the following 23:
- Fever (either continuous or spiking)
- Chills
- Right upper quadrant pain
- Anorexia
- Jaundice
- Enlarged liver (hepatomegaly)
- Malaise
- Weight loss
- Nausea and vomiting
- Right shoulder pain
- Weakness
- Abdominal pain
- Night sweats
- Rigors (shivers)
- Diarhhea
- Pleurisy
- Dyspnea (shortness of breath)
- Cough
Cough or hiccoughs due to diaphragmatic irritation may be reported. Referred pain to the right shoulder may be present.
Individuals with solitary lesions usually have a more insidious course with weight loss and anemia of chronic disease. With such symptoms, malignancy often is the initial consideration.
Fever of unknown origin (FUO) frequently can be an initial diagnosis in indolent cases. Multiple abscesses usually result in more acute presentations, with symptoms and signs of systemic toxicity.
Afebrile presentations have been documented.
Fever and tender hepatomegaly are the most common signs. A palpable mass need not be present. Midepigastric tenderness, with or without a palpable mass, is suggestive of left hepatic lobe involvement.
Decreased breath sounds in the right basilar lung zones, with signs of atelectasis and effusion on examination or radiologically, may be present. A pleural or hepatic friction rub can be associated with diaphragmatic irritation or Glisson capsule inflammation.
Jaundice may be present in as many as 25% of cases and usually is associated with biliary tract disease or the presence of multiple abscesses.
Liver abscess complications
Complications of liver abscess may include the following:
- Sepsis
- Empyema resulting from contiguous spread or intrapleural rupture of abscess
- Rupture of abscess with resulting peritonitis
- Endophthalmitis when an abscess is associated with Klebsiella pneumoniae
If untreated, hepatic abscesses can rupture, cause peritonitis and shock. At times the area will get walled off, and chronic pain and discomfort in right upper quadrant with occasional nighttime fever can follow. Complications are also possible after drainage and include liver or kidney failure, intraabdominal lesions, infections or reoccurring liver abscesses 24. Other complications include subphrenic abscess, fistula to organs nearby (such as pleuropulmonary and hypobranchial fistula), acute pancreatitis, abdominal or liver venous thrombosis, and liver pseudoaneurysm. Infectious metastatic complications include endophthalmitis or central nervous system septic emboli.
It is vitally important to follow up with patients after treatment to prevent and recognize some of these complications. Immediate treatment for intraabdominal infection is the best preventive measure for liver abscesses. Four to six weeks of antibiotic therapy post-drainage can prevent almost any complications. Antibiotic prophylaxis during chemoembolization or endoscopic retrograde cholangiography help in the prevention of future abscess formation.
Radiographic abnormalities will take longer than clinical or lab abnormalities to go away, as is with many other medical problems. So enough time should elapse before the graphs go back to normal.
Liver abscess diagnosis
It is vital to perform a thorough history and physical examination before choosing any diagnostic measures. This includes but not limited to gathering the patient’s personal history, occupation, travel, place of origin, recent infections, or treatments. Certain risk factors promote the development of liver abscess; such as diabetes, cirrhosis, male gender, elderly, immunocompromised states, and people with proton pump inhibitor usage.
After gathering a history, the review of systems and physical examination can provide a lot of additional information. On analysis of systems, patients may complain of the following symptoms: fever, chills, night sweats, malaise, nausea or vomiting, right shoulder pain (due to diaphragmatic irritation), right upper quadrant pain, cough, dyspnea, anorexia, or recent unexplained weight loss. Fever is present in 90% and abdominal pain in about 50-75% 25. Dark urine is present much like other hepatitis forms.
On physical exam, a patient can have hepatomegaly with an enlarged mass and jaundice. Although Charcot’s triad (right upper quadrant pain, jaundice, and fever) is a sign of cholangitis, the physician will need to consider liver abscess as a differential 26. A small number of patients with hepatic abscesses may present in distress or even overt shock (septic shock or anaphylactic shock in case of the hydatiform mole rupture).
In case of Klebsiella liver abscesses (happen mostly in southeast Asia), in addition to the symptoms mentioned above, it also sends septic emboli to eye, meninges, and brain. Therefore symptoms of these organ systems can be present, and it can last after the liver abscess is drained.
In the case of Echinococcus infection, there is an initial asymptomatic infection in a child. Years later some of these people will show clinical symptoms from reactivation of the infection 27. The clinical manifestations depend on the type, size, and site of the cysts present. Small cysts in non-vital organs can go undetected, but large ones in critical locations can cause compressive signs or rupture 28. Usual rate of cyst progression is 1 to 5 centimeters in a year. The liver is affected in two-thirds of cases of Echinococcus infection. Symptoms of compression usually start when the diameter is 10 cm and include biliary colic, cholangitis, obstructive jaundice, portal and venous obstruction, Budd-Chiari syndrome, bronchial fistula, If it ruptures, overt peritonitis or anaphylaxis will be present.
After the history and physical, the next step is to obtain laboratory and diagnostic evidence to determine the cause of the patient’s chief complaint and confirm or rule out a liver abscess.
Laboratory studies
Laboratory tests include a complete blood count (CBC) with differential, tests for hepatocellular injury (AST, ALT usually elevated in half the cases), liver synthetic function tests (Prealbumin and INR), alkaline phosphatase (elevated around 90%), C-reactive protein, sedimentation rate, and blood cultures to rule out bacteremia 29.
If an amebic abscess is suspected (residents or travelers from Southeast Asia or Africa), stool test or serology for Entamoeba histolytica should be performed. For hydatid cyst, serology for Echinococcus is needed. Enzyme-linked immunosorbent assay (ELISA) seems to be the most sensitive and specific for Echinococcus. After initial screening with ELISA, confirmatory tests with immunoelectrophoresis and immunoblotting is needed. Serology positivity is dependant on size and site of the cysts. Liver and bone cysts produce positive serology whereas lung, brain, eye, splenic or calcified cysts do not. Calcification is usually a sign of non-viable material.
Many radiographical tests can be performed, and certain tests should take precedence. It is important to limit a patient’s exposure to unnecessary radiation and tests. There can be findings in the chest x-ray pointing to this diagnosis such as elevated hemidiaphragm on the right and pleural effusion over the liver. However, the initial test of choice is an abdominal ultrasound (US) which shows hyper or hypoechoic lesions with occasional debris or septation. Computed tomography (CT) with contrast is the next step, and slightly more sensitive. Rim enhancement and edema are not typical but very specific for infection. The ultrasound or CT is followed by needle aspiration under guidance to identify the exact causative organism which is essential for diagnostic as well as therapeutic purposes (small cysts) 30. Technetium scan is another test with an 80% sensitivity (less than CT); 50-80% for gallium and 90% for indium 31. If inner cyst walls are in-folded (separation of hydatid membrane from the wall of the cyst) during the ultrasound, hydatid disease is more likely.
Stains and cultures should be obtained from direct aspirate. Drains that are in place will get contaminated with skin flora and are not accurate for culture purposes. Stains and cultures should be done for aerobes and anaerobes (special handling might be needed), but occasionally more specific cultures need to be done such as fungi, Mycobacterium, Entamoeba histolytica, and parasites.
Diagnosis is confirmed when there are cystic or solid areas in the liver that upon aspiration will yield fluid with positive cultures. It is important to obtain these tests quickly and start treatment because of the high complication rate if left untreated.
Liver abscess treatment
Drainage of liver abscess and antibiotic treatment are the cornerstone of treatments.
Drainage is needed and can be done under the ultrasound or CAT scan. Needle aspiration (at times repeatedly) might be all that is required for abscesses less than 5 cm but a catheter placement might be warranted if the diameter is more significant than that 32. Percutaneous drainage with catheter placement is probably the most successful procedure for larger than 5 cm abscesses 33. Laparoscopic drainage is at times used. Surgery should be done for peritonitis, thick wall abscesses, ruptured abscess, multiple large abscesses, and prior failed drainage procedures. An operation is performed either by a transperitoneal approach or by the posterior transpleural approach. The former approach drains the abscess and allows for the exploration of undetected ulcers, while the latter is better for posterior abscesses. Size, location, and stage help determine a successful treatment plan. When previous biliary procedures have been done, Endoscopic retrograde cholangiopancreatography (ERCP) drainage might be used 34. Undrained liver abscesses may cause sepsis, peritonitis and empyema.
Empiric antibiotic coverage is essential when the organism is unknown. The antibiotics should cover Enterobacteriaceae, anaerobes, streptococci, enterococci, and Entamoeba histolytica. Such possible regimens are later generation cephalosporins plus metronidazole, Beta-lactam Beta-Lactamase inhibitor plus metronidazole, or synthetic penicillins plus aminoglycosides plus metronidazole. Alternatively, fluoroquinolones or carbapenem can be substituted for cephalosporins or Penicillins in case of allergy or unavailability. Metronidazole should cover Entamoeba histolytica. Duration of treatment varies but is usually from two to six weeks. After initial intravenous treatment, orals can be used safely in most cases to complete the course. Culture results help narrow down the organism so empiric treatment is no longer needed, as it can lead to antibiotic resistance. Anaerobes are hard to culture so sometimes they should be treated for the entire course empirically. For stable patients, antibiotics can be given post-drainage to increase culture yield for proper treatment. Empiric antifungal treatment is crucial in immunosuppressed patients with a risk for chronic disseminated fungemia. Occasionally if the patient is too sick for drainage, antibiotics are used solely for treatment but this is a less than desirable method.
If the source is Echinococcus, treatment includes a benzimidazole such as albendazole. This therapy may last for several years. Although most cases are uncomplicated and can be treated with an antiparasitic drug, complicated cases must be treated delicately. In most complicated cases drainage is necessary. Surgeons must take caution to inject the hydatid cysts before draining them, as sometimes the rupture can cause the patient to go into shock rapidly.
In a study by Abbas, the mean duration of hospital stay for those with pyogenic liver abscesses was 13.6 days. Antibiotic therapy used for them was approximately 34.7 days. One patient expired. On the other hand, patients with amebic liver abscesses had a mean hospital stay of approximately 7.7 days with a mean duration of treatment of 11.8 days where all patients were cured 35.
Liver abscess prognosis
Untreated, pyogenic liver abscess remains uniformly fatal. With new techniques available for drainage and antibiotics specific for appropriate organisms, liver abscesses have a much better prognosis now. In-hospital mortality is estimated at 2.5% to 19% 9. The mortality rate is higher in elderly, ICU admissions, shock, cancer, fungal infections, cirrhosis, chronic renal failure, acute respiratory failure, severe disease, and biliary origin of an abscess. The most common causes of death include sepsis, multiorgan failure, and hepatic failure 10. Indicators of a poor prognosis have been described since 1938 and include multiplicity of abscesses, underlying malignancy, severity of underlying medical conditions, presence of complications, and delay in diagnosis 10. Indicators of a poor prognosis in amebic abscess include a bilirubin level of greater than 3.5 mg/dL, encephalopathy and hypoalbuminemia.
Liver abscess reoccurrence is frequent in patients who present with a biliary tract disease 36.
In hydatic cysts, the prognosis is good. 57% will have a stable cyst, and even if the cyst grows, it will not usually cause symptoms. About 15% will require surgery, and that is often years after diagnosis. 76% of those who did not have surgery were asymptomatic for years 28.
References- Mavilia MG, Molina M, Wu GY. The Evolving Nature of Hepatic Abscess: A Review. J Clin Transl Hepatol. 2016;4(2):158–168. doi:10.14218/JCTH.2016.00004 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4913073
- Akhondi H, Sabih DE. Liver Abscess. [Updated 2019 Jun 4]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK538230
- Singh S, Chaudhary P, Saxena N, Khandelwal S, Poddar DD, Biswal UC. Treatment of liver abscess: prospective randomized comparison of catheter drainage and needle aspiration. Ann Gastroenterol. 2013;26(4):332–339. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3959473
- Lardière-Deguelte S, Ragot E, Armoun K, Piardi T, Dokmak S, Bruno O, et al. Hepatic abscess: diagnosis and management. J Visc Surg. 2015;152:231–243. doi: 10.1016/j.jviscsurg.2015.01.013
- Kumar V, Abbas AK, Fausto N et-al. Robbins and Cotran pathologic basis of disease. W B Saunders Co. (2005) ISBN:0721601871
- Kaplan GG, Gregson DB, Laupland KB. Population-based study of the epidemiology of and the risk factors for pyogenic liver abscess. Clin. Gastroenterol. Hepatol. 2004 Nov;2(11):1032-8.
- Czerwonko ME, Huespe P, Bertone S, Pellegrini P, Mazza O, Pekolj J, de Santibañes E, Hyon SH, de Santibañes M. Pyogenic liver abscess: current status and predictive factors for recurrence and mortality of first episodes. HPB (Oxford). 2016 Dec;18(12):1023-1030.
- Joshi G, Crawford KA, Hanna TN, Herr KD, Dahiya N, Menias CO. US of Right Upper Quadrant Pain in the Emergency Department: Diagnosing beyond Gallbladder and Biliary Disease. (2018) Radiographics : a review publication of the Radiological Society of North America, Inc. 38 (3): 766-793. doi:10.1148/rg.2018170149
- Chen YH, Li YH, Lin YJ, Chen YP, Wang NK, Chao AN, Liu L, Wu WC, Lai CC, Chen TL, Chen KJ. Prognostic Factors and Visual Outcomes of Pyogenic Liver Abscess-Related Endogenous Klebsiella pneumoniae Endophthalmitis: A 20-year retrospective review. Sci Rep. 2019 Jan 31;9(1):1071.
- Chen SC, Huang CC, Tsai SJ, Yen CH, Lin DB, Wang PH, et al. Severity of disease as main predictor for mortality in patients with pyogenic liver abscess. Am J Surg. 2009 Aug. 198 (2):164-72.
- Liver abscess rupture in pleural space. https://radiopaedia.org/cases/liver-abscess-rupture-in-pleural-space
- Lardière-Deguelte S, Ragot E, Amroun K, Piardi T, Dokmak S, Bruno O, Appere F, Sibert A, Hoeffel C, Sommacale D, Kianmanesh R. Hepatic abscess: Diagnosis and management. J Visc Surg. 2015 Sep;152(4):231-43.
- Lai HC, Lin CC, Cheng KS, Kao JT, Chou JW, Peng CY, Lai SW, Chen PC, Sung FC. Increased incidence of gastrointestinal cancers among patients with pyogenic liver abscess: a population-based cohort study. Gastroenterology. 2014 Jan;146(1):129-37.e1
- Yang CC, Yen CH, Ho MW, Wang JH. Comparison of pyogenic liver abscess caused by non-Klebsiella pneumoniae and Klebsiella pneumoniae. J Microbiol Immunol Infect. 2004 Jun;37(3):176-84.
- Sánchez Thevenet P, Alvarez HM, Torrecillas C, Jensen O, Basualdo JA. Dispersion of Echinococcus granulosus eggs from infected dogs under natural conditions in Patagonia, Argentina. J. Helminthol. 2019 Feb 04;:1-7.
- Krige, J E J; Beckingham, I J. ABC of diseases of liver, pancreas, and biliary system: Liver abscesses and hydatid disease BMJ. 322 (7285): 537. doi:10.1136/bmj.322.7285.537
- Yang YF, Wang HJ, Kan WC, et al. Pyogenic liver abscess in ESRD patients undergoing maintenance dialysis therapy. (2006) American journal of kidney diseases : the official journal of the National Kidney Foundation. 47 (5): 856-61. doi:10.1053/j.ajkd.2006.01.032
- Pearce NW, Knight R, Irving H, et al. Non-operative management of pyogenic liver abscess. HPB (Oxford). 2003;5(2):91–95. doi:10.1080/13651820310001126 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2020567
- Mølle I, Thulstrup AM, Jepsen P,et al . Liver cirrhosis is risk factor for pyogenic liver abscesses. (2001) BMJ (Clinical research ed.). 323 (7303): 52-3.
- Chadwick, Matthew, Shamban, Leonid, Neumann, Michael. Pyogenic Liver Abscess with No Predisposing Risk Factors. (2018) Case Reports in Gastrointestinal Medicine. doi:10.1155/2018/9509356
- Thomsen, Reimar W., Jepsen,et al. Diabetes Mellitus and Pyogenic Liver Abscess: Risk and Prognosis. (2007) Clinical Infectious Diseases. 44 (9): 1194. doi:10.1086/513201
- Chadwick, Matthew, Shamban, et al. Pyogenic Liver Abscess with No Predisposing Risk Factors. (2019) Case Reports in Gastrointestinal Medicine. doi:10.1155/2018/9509356
- Liver Abscess Clinical Presentation. https://emedicine.medscape.com/article/188802-clinical
- Dietrick RB. Experience with liver abscess. Am. J. Surg. 1984 Feb;147(2):288-91.
- Mohsen AH, Green ST, Read RC, McKendrick MW. Liver abscess in adults: ten years experience in a UK centre. QJM. 2002 Dec;95(12):797-802.
- Boĭko VV, Tishchenko AM, Gusak IV, Maloshtan AA, Skoryĭ DI, Smachilo RM. [Surgical treatment of a solitary hepatic abscess]. Klin Khir. 2013 Jun;(6):22-5.
- Moro PL, Gilman RH, Verastegui M, Bern C, Silva B, Bonilla JJ. Human hydatidosis in the central Andes of Peru: evolution of the disease over 3 years. Clin. Infect. Dis. 1999 Oct;29(4):807-12.
- Frider B, Larrieu E, Odriozola M. Long-term outcome of asymptomatic liver hydatidosis. J. Hepatol. 1999 Feb;30(2):228-31.
- Rahimian J, Wilson T, Oram V, Holzman RS. Pyogenic liver abscess: recent trends in etiology and mortality. Clin. Infect. Dis. 2004 Dec 01;39(11):1654-9.
- Ahn SJ, Kim JH, Lee SM, Park SJ, Han JK. CT reconstruction algorithms affect histogram and texture analysis: evidence for liver parenchyma, focal solid liver lesions, and renal cysts. Eur Radiol. 2018 Nov 19
- Rassam F, Cieslak KP, Beuers UHW, van Gulik TM, Bennink RJ. Stress test of liver function using technetium-99m-mebrofenin hepatobiliary scintigraphy. Nucl Med Commun. 2019 Apr;40(4):388-392.
- Zerem E, Hadzic A. Sonographically guided percutaneous catheter drainage versus needle aspiration in the management of pyogenic liver abscess. AJR Am J Roentgenol. 2007 Sep;189(3):W138-42.
- Cai YL, Xiong XZ, Lu J, Cheng Y, Yang C, Lin YX, Zhang J, Cheng NS. Percutaneous needle aspiration versus catheter drainage in the management of liver abscess: a systematic review and meta-analysis. HPB (Oxford). 2015 Mar;17(3):195-201.
- Sersté T, Bourgeois N, Vanden Eynden F, Coppens E, Devière J, Le Moine O. Endoscopic drainage of pyogenic liver abscesses with suspected biliary origin. Am. J. Gastroenterol. 2007 Jun;102(6):1209-15.
- Abbas MT, Khan FY, Muhsin SA, Al-Dehwe B, Abukamar M, Elzouki AN. Epidemiology, Clinical Features and Outcome of Liver Abscess: A single Reference Center Experience in Qatar. Oman Med J. 2014 Jul;29(4):260-3.
- You MS, Lee SH, Kang J, Choi YH, Choi JH, Shin BS, Huh G, Paik WH, Ryu JK, Kim YT, Jang DK, Lee JK. Natural Course and Risk of Cholangiocarcinoma in Patients with Recurrent Pyogenic Cholangitis: A Retrospective Cohort Study. Gut Liver. 2019 May 15;13(3):373-379.





{kind=link}