Paroxysmal hand hematoma
Paroxysmal hand hematoma also known as paroxysmal finger hematoma or Achenbach’s syndrome, refers to a condition in which a patient exhibits episodic pain and swelling in one or more fingers along with the subsequent appearance of a hematoma on the palmar side of the proximal phalanges 1. Achenbach syndrome is a benign condition of unknown cause in which prodromal symptoms, such as pain, tingling, and itching, may occur from minutes to hours before the color change appears 2. The subdermal bleeding usually stops spontaneously or after local pressure is applied. The color changes usually disappear within a few days, without permanent complications. The diagnosis of paroxysmal hand hematoma is based strictly on its clinical features because the results of all routine investigations are usually normal. Physicians should become aware of this condition in order to advise their patients about its benign prognosis and to avoid unnecessary testing.
Women are more commonly affected than men and the age of onset is predominantly over 50 3. The phalanges of the middle and index finger are the most commonly affected 4. Patients report a spontaneous sudden onset of burning or itching sensations in the finger, followed within minutes by the appearance of bruising, usually on the palmar aspect of the fingers 5. The finger then becomes swollen, pale and cold. Movement can be restricted. The recurrence rate is very variable and the haematomas generally resorb within a few days. Associations with acrocyanosis, gastrointestinal disorders, migraines and gall bladder disease have been noted 6. The diagnosis is made on the basis of the clinical assessment, because coagulation, hematological and biochemical parameters, as well conventional radiology and Doppler examination are normal 7.
According to current knowledge, paroxysmal hand hematoma or Achenbach’s syndrome is not among the known causes of mortality or morbidity. However, it is unknown whether it is seen in brain or other vital organs 8. Due to Achenbach’s syndrome, a probable hemorrhage or hematoma in the brain and other vital organs would be life threatening, so the disease should be further investigated. Further research is needed to clarify paroxysmal hand hematoma or Achenbach’s syndrome and to develop a diagnosis and treatment algorithm.
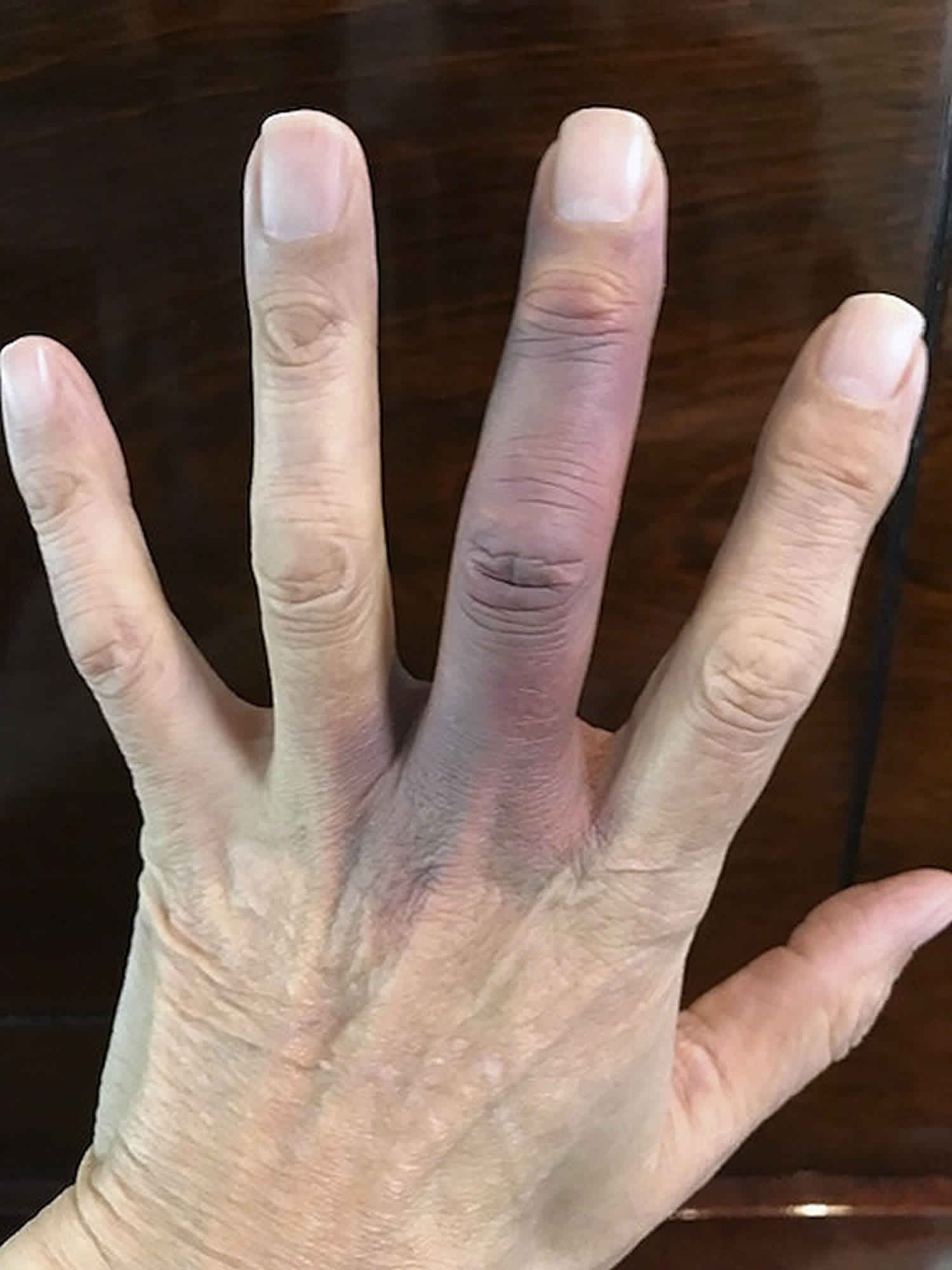
Figure 1. Paroxysmal finger hematoma

Footnote: A 60-year-old non-smoker woman attended an emergency unit with a history of sudden onset of pain in the distal phalange of her thumb. Subsequently bruising appeared on the volar aspect of the pulp accompanied by marked pain and coldness. She had a previous similar episode, which resolved completely and spontaneously within a few days. There was no history of trauma. She had otherwise an unremarkable medical history. Examination revealed thumb swelling at the level of the distal phalange with bruising over its volar surface. The thumb was well perfused and showed an unrestricted mobility. Blood parameters including coagulation tests and radiographs were normal. No consistent findings were noted at a high resolution sonography. Colour Doppler investigation and measurement of finger-tip pressure revealed unaltered perfusion flow. No specific treatment was proposed and spontaneous resolution followed within 2 weeks.
[Source 3 ]Paroxysmal hand hematoma causes
The causes of paroxysmal hand hematoma is still unknown 8, but is probably of vascular origin. Singer 9 has hypothesized that in some patients increased capillary resistance and vascular fragility may trigger this disease even in a minimal trauma. It has also been reported that acrocyanosis, gastrointestinal diseases, migraines, and biliary diseases may be related to the cause of paroxysmal hand hematoma 10. Kämpfen et al 11 have proposed the cause of vasospasm through a case in which anti-migraine medication (ergotamine) was used due to migraine. It has been suggested that Achenbach’s syndrome may be associated with Raynaud’s syndrome and Chilblain’s disease in the secondary data gathered from Carpentier et al 12. In the same study, paroxysmal hand hematoma was found to be associated with tobacco use, alcohol consumption, and estrogen therapy while no relationship was observed with body mass index, education level, marital status, occupation, vibration, and trauma. Paroxysmal hand hematoma or Achenbach’s syndrome is 2-7 times more common in middle-aged women than in men 13.
In a recent publication of two cases of women with paroxysmal hand hematoma or Achenbach’s syndrome authors suggest that there may be an association with a marked reduction in digital blood flow at arteriography 14.
Achenbach’s syndrome is typically characterized by a digital hematoma and bruising that begins suddenly and painfully in one or several fingers and decreases within hours or days. There are no known risk factors such as trauma, drug use, bleeding disorder, or rheumatologic disease associated with the etiology of the syndrome. Paroxysmal hand hematoma or Achenbach’s syndrome was named after German doctor Achenbach as it was first diagnosed by him 15.
Paroxysmal hand hematoma symptoms
Paroxysmal hand hematoma or Achenbach’s syndrome is a rare clinical entity consisting of spontaneous sudden bruising on the palmar side of fingers or hand associated with burning pain and swelling of the digits 3. Blue-colored finger, numbness in the finger and sudden onset pain are the most common symptoms. In addition to these complaints, swelling and paresthesia can be observed in some patients. The subdermal bleeding usually stops spontaneously or after local pressure is applied. The color changes usually disappear within a few days, without permanent complications. In the literature, two cases were identified in which the location of the disease was not the fingers. One of these cases was recurrent subconjunctival hemorrhage in the eye 16 while the other was located in the wrist 17.
Although the most common location of the disease varies in the sources, it has been observed more frequently in the middle and index fingers 12. Paroxysmal hand hematoma or Achenbach’s syndrome is generally episodic 18. In a study by Ada and Kasimzade 8, the average number of episodes was 3.04, and the most common finger was the index finger.
It is important to be aware of paroxysmal hand hematoma as the symptoms these patients present could suggest a more serious vascular disease and lead to invasive investigations.
The clinical presentation of paroxysmal hand hematoma must be distinguished from other conditions such as painful bruising syndrome (autoerythrocyte sensitisation syndrome, which commonly involves the legs and trunk) dermatitis artefacta, spontaneous rupture of the vincula, trauma and Raynaud’s syndrome.
Paroxysmal hand hematoma diagnosis
Physical examination and medical history have a major role in the diagnosis of paroxysmal hand hematoma or Achenbach’s syndrome. Laboratory and imaging techniques may be required for differential diagnosis (Table 1). However, in suspected cases, these methods should be used and unnecessary invasive procedures should be avoided 19. Because of the possibility of mistaking paroxysmal hand hematoma with many vascular, hematologic, dermatologic, and rheumatologic diseases, some laboratory and imaging methods might be required (such as complete blood count, coagulation factors, c-reactive protein, blood lipid level, and arterial and venous Doppler ultrasonography of the concerned extremity) 13. In the literature, biopsies were performed for lesions in two cases 13, 20. In one of these cases, the epidermis showed hyperkeratosis and parakeratosis. In the other case, amorphous, eosinophilic amyloid deposition in the stroma and fibrin accumulation was observed. In both cases, no pathology was detected in microvascular structures. Capillaroscopy examination was not necessary for diagnosis, but Khaira et al 21 performed capillaroscopy in 11 patients, and no pathology was detected. Frerix et al 22 showed capillary hemorrhage in one case. Arterial and venous Doppler ultrasonography is a good non-invasive choice for evaluating the vascular bed 23. No arterial or venous pathology was found in the Doppler ultrasonography in any of the studies performed.
Upon suspicion of arterial microembolism, invasive imaging methods can be used to investigate the origin of the microemboli 24. While in the case reported by Weinberg et al 25, no pathology was observed in the upper extremity angiography, in the case of Robertson et al 26, slow flow was observed in the digital arteries. There are studies in which transthoracic echocardiography was used in the diagnosis of arterial embolism, and no cardiogenic embolic source had been found in these studies 25. In another study, oxygen saturation was measured at the diseased fingertip by pulse oximetry in order to possibly detect microemboli. No abnormal oxygen saturation, which would suggest ischemia or embolism, was found in any of the patients. Achenbach’s syndrome should be considered in the differential diagnosis of symptoms similar to Raynaud’s syndrome with clinical episodic digital ischemia 27. The rheumatologic aspect of the syndrome has been further investigated in case reports, but no rheumatologic relationship has been found other than Achenbach’s syndrome associated with rheumatoid arthritis reported by Manappallil et al 28.
Table 1. Paroxysmal hand hematoma differential diagnoses
| Differential diagnosis | |
| Raynaud’s syndrome or phenomenon | Thoracic outlet syndrome |
| Spontaneous digital venous thrombosis | Trauma |
| Gardner-Diamond syndrome | Collagen vascular disease |
| Atherosclerosis | Buerger disease |
| Takayasu arteritis | Ulnar artery thrombosis |
| Giant cell arteritis | Radial artery thrombosis |
| Aneurysmal disease producing emboli | Microemboli |
| Vibration-induced injury | Polycythemia |
| Cold injury | Cryoglobulinemia |
| Dermatitis artefacta | Spontaneous rupture of the vincula |
| Acute limb ischemia | Chilblain’s disease |
| Acrocyanosis | Acrorygosis |
Paroxysmal hand hematoma treatment
There are many different opinions in the general treatment of paroxysmal hand hematoma. Some of these views suggest that there is no need for treatment because of the benign course of paroxysmal hand hematoma and that only follow-up is sufficient 29. On the other hand, there are publications in which treatment includes sargegrelate hydrochloride, acetylsalicylic acid 81 mg, long-acting diprimadol, heparin, or isosorbidedinitrate 26, 25, 13. Though the cause is unknown, if a bleeding point was definite, experts did not apply anticoagulant, antiplatelet, or vasodilator treatments unless there was another compulsory indication. When necessary, patients were treated with analgesics, or with cream or gel containing mucopolysaccharidepolysulphate; occasionally cold applications were applied or the patient was advised to rest the diseased hand. After 2 weeks of treatment, it was observed that the patients did not have any complaints.
References- Achenbach syndrome (paroxysmal finger hematoma). Vasc Med. 2019 Aug;24(4):361-366. doi: 10.1177/1358863X19849627. Epub 2019 Jun 4. https://doi.org/10.1177/1358863X19849627
- Is Achenbach’s syndrome a surgical emergency? A systematic review. Eur J Trauma Emerg Surg. 2016 Aug;42(4):439-443. doi: 10.1007/s00068-015-0610-0. Epub 2015 Dec 15. https://doi.org/10.1007/s00068-015-0610-0
- A Painful Blue Thumb: A Case of Achenbach’s Syndrome. EJVES Extra Volume 10, Issue 4, October 2005, Pages 84-85 https://doi.org/10.1016/j.ejvsextra.2005.07.004
- J.C.J. Eikenboom, S.C. Cannegeiter, E. Breit Paroxysmal finger haematoma: A neglected syndrome Thromb Haemost, 66 (1991), p. 266
- L. Zimmerli, C. Dobler. Aschwanden. Recurrent paroxysmal finger hematoma (Achenbach syndrome). Schweiz Rundsch Med Prax, 91 (40) (2002), pp. 1664-1666
- A.M. Layton, J.A. Cotterill. A case of Achenbach’s syndrome. Clin Exp Dermatol, 18 (1993), pp. 60-61
- H.S. Khaira, D. Rittoo, S.R.G. Smith. The non-ischaemic blue finger. Ann R Coll Surg, 83 (2001), pp. 154-157
- Ada F, Kasimzade F. Analysis of 24 patients with Achenbach’s syndrome. World J Clin Cases. 2019;7(10):1103–1110. doi:10.12998/wjcc.v7.i10.1103 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6547318
- Sınger R. On the symptoms and diagnosis of finger apoplexy (paroxysmal hematoma of the hand) Wien Klin Wochenschr. 1962;74:741–743.
- Layton AM, Cotterill JA. A case of Achenbach’s syndrome. Clin Exp Dermatol. 1993;18:60–61.
- Kämpfen S, Santa DD, Fusetti C. A painful blue thumb: a case of Achenbach’s syndrome. EJVES Extra. 2005;10:84–85.
- Carpentier PH, Maricq HR, Biro C, Jiguet M, Seinturier C. Paroxysmal finger haematoma–a benign acrosyndrome occurring in middle-aged women. Vasa. 2016;45:57–62.
- Takeuchi H, Uchida HA, Okuyama Y, Wada J. Acute idiopathic blue fingers: a young man with Achenbach’s syndrome. BMJ Case Rep. 2016;2016:10.1136/bcr–2016-214491
- A. Robertson, M.I. Liddington, S.P. Kay. Paroxysmal finger haematomas (Achenbach’s syndrome) with angiographic abnormalities. J Hand Surg [Br], 27 (4) (2002), pp. 391-393
- Achenbach W. Paroxysmal hematoma of the hand. Medizinische. 1958;52:2138–2140.
- Young B, Okera S. Recurrent subconjunctival haemorrhage in Achenbach’s syndrome. Clin Exp Ophthalmol. 2018;46:965–966.
- Huikeshoven M, de Priester JA, Engel AF. A case of spontaneous wrist haematoma in Achenbach syndrome. J Hand Surg Eur Vol. 2009;34:551–552.
- Yamada T. Achenbach’s syndrome in an elderly woman. J Gen Fam Med. 2018;19:65–66.
- Kordzadeh A, Caine PL, Jonas A, Rhodes KM, Panayiotopolous YP. Is Achenbach’s syndrome a surgical emergency? A systematic review. Eur J Trauma Emerg Surg. 2016;42:439–443.
- Watchorn RE, Babu S, Lewis F, Calonje E, Taibjee SM. Paroxysmal purple palmar macules with a rare aetiology. Clin Exp Dermatol. 2017;42:561–563.
- Khaira HS, Rittoo D, Vohra RK, Smith SR. The non-ischaemic blue finger. Ann R Coll Surg Engl. 2001;83:154–157.
- Frerix M, Richter K, Müller-Ladner U, Hermann W. Achenbach’s syndrome (paroxysmal finger hematoma) with capillaroscopic evidence of microhemorrhages. Arthritis Rheumatol. 2015;67:1073.
- Sidhu MS, Ahmad Z, Jose RM. A case of non-ischaemic blue finger and toe. Eur J Plast Surg. 2015;38:165–166.
- Gaines PA, Swarbrick MJ, Lopez AJ, Cleveland T, Beard J, Buckenham TM, Belli AM, Kessel D. The endovascular management of blue finger syndrome. Eur J Vasc Endovasc Surg. 1999;17:106–110.
- Weinberg I, Jaff MR. Spontaneous blue finger syndrome: a benign process. Am J Med. 2012;125:e1–e2.
- Robertson A, Liddington MI, Kay SP. Paroxysmal finger haematomas (Achenbach’s syndrome) with angiographic abnormalities. J Hand Surg Br. 2002;27:391–393.
- Yetkin U, Gürbüz A. Current Approach To Raynaud’s Phenomenon. Turk Gogus Kalp Dama. 2002;10:56–62.
- Manappallil RG, Jayaraj J. Blue Finger Syndrome: An Unusual Presentation of Rheumatoid Arthritis. J Clin Diagn Res. 2017;11:OD06–OD07
- Yamamoto Y, Yamamoto S. Achenbach’s Syndrome. N Engl J Med. 2017;376:e53





{kind=link}