
What are causes of pimple on eyelid
The eyelid contains multiple glandular structures and tissue connections that protect and contribute to function of the eye. Understanding the anatomy of the orbital region guides the awareness of pathology and diagnosis of conditions presenting with a swollen red eyelid (Table 1). Issues affecting the skin elsewhere on the body, such as atopic dermatitis, insect bites, cellulitis, and necrotizing fasciitis, can occur on the skin of the eyelid. Methicillin-resistant Staphylococcus aureus (MRSA) colonization and infections can also affect the eyelid. Systemic processes, such as autoimmune disease, metastatic cancer, heart failure, and nephrotic syndrome, can manifest in the orbital region 1.
Anatomy of the Eyelid
The eyelid is a complex, fully functioning skin tissue that consists of eyelashes, lacrimal (tear) glands, sebaceous (oil or meibomian) glands, and sweat glands (glands of Zeis or Moll) 2.
Figure 1 depicts the anatomy of the orbit and eyelid. These structures can develop inflammatory reactions leading to a red, swollen eyelid. The lacrimal glands produce tears that run medially over the cornea and drain into the nasolacrimal sac 2. The eyelid and conjunctivae are colonized by the usual flora of the body, including fungi and S. aureus 3.
The orbits contain the globe, muscles for eye movement, optic nerve, arteries, veins, and surrounding fat. The orbital septum creates an anatomic barrier of connective tissue that runs from the periosteum of the skull through the eyelid. The orbital septum separates preseptal tissues from the orbital tissues.
Anatomically, the eyelid is part of the preseptal tissue. Tumor effect and inflammation posterior to the orbital septum can disrupt blood flow to the globe, impede function of the optic nerve, affect vision, and limit the function of ocular muscles 4.
The paranasal sinuses (maxillary, frontal, ethmoid, and sphenoid) abut the orbit on three sides 5. The lateral aspect of the ethmoid bone is called the lamina papyracea (Latin for “layer of paper”). It forms a thin, bony separation that can allow extravasation of inflammation from the ethmoid sinus into the orbital cavity 6.
Venous flow from the orbital region drains into the ophthalmic veins and subsequently the cavernous sinus. The teeth are in close proximity to the area, and dental pathology can present with orbital symptoms 7.
The eyelid can appear swollen because of processes in the eyelid or mass effects from the tissues posterior to the orbital septum. Prompt diagnosis is vital to guide appropriate therapy and avoid vision loss. Issues that warrant immediate ophthalmology consultation include penetrating trauma through the eyelid or into the globe, a change in vision such as diplopia, and loss of extraocular movements (ophthalmoplegia) 5.
Figure 1. Eye anatomy
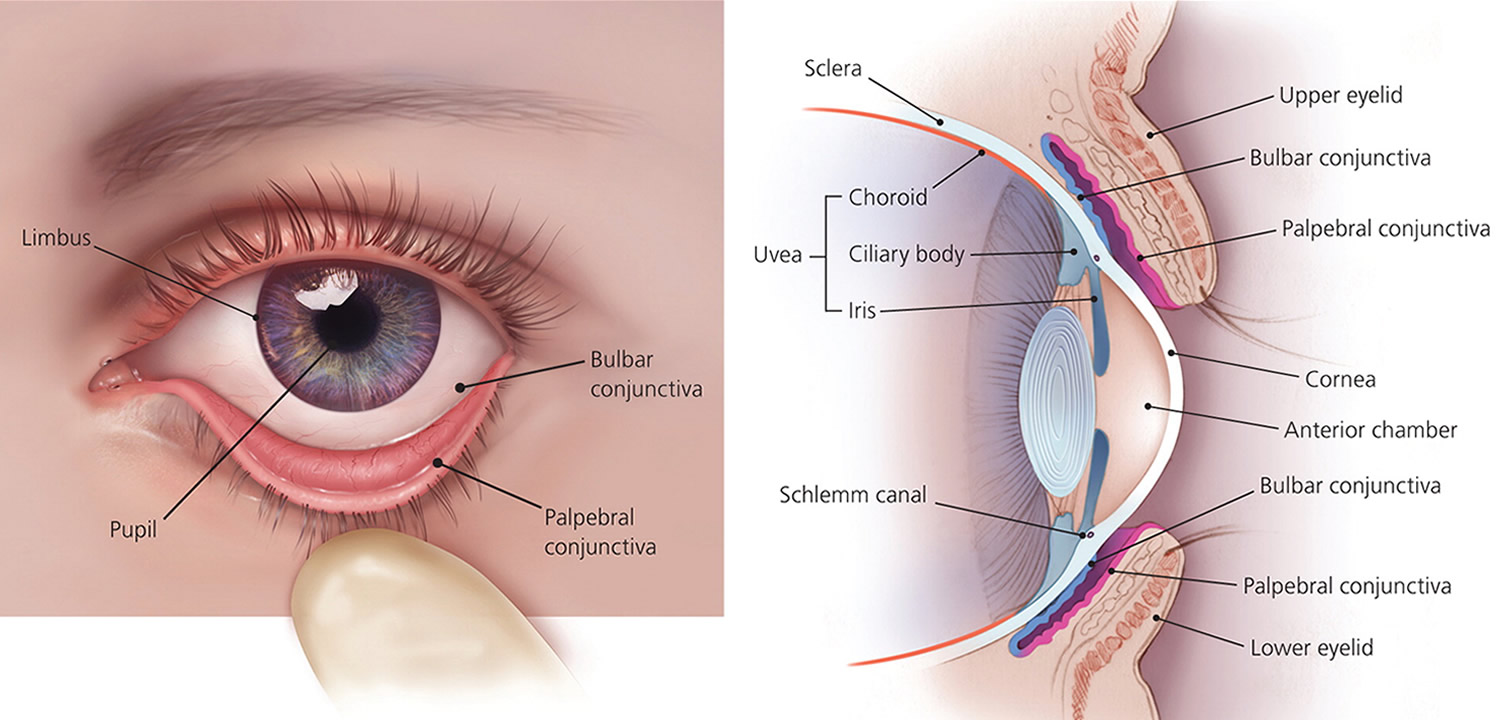
Figure 2. Eye and Eyelid anatomy
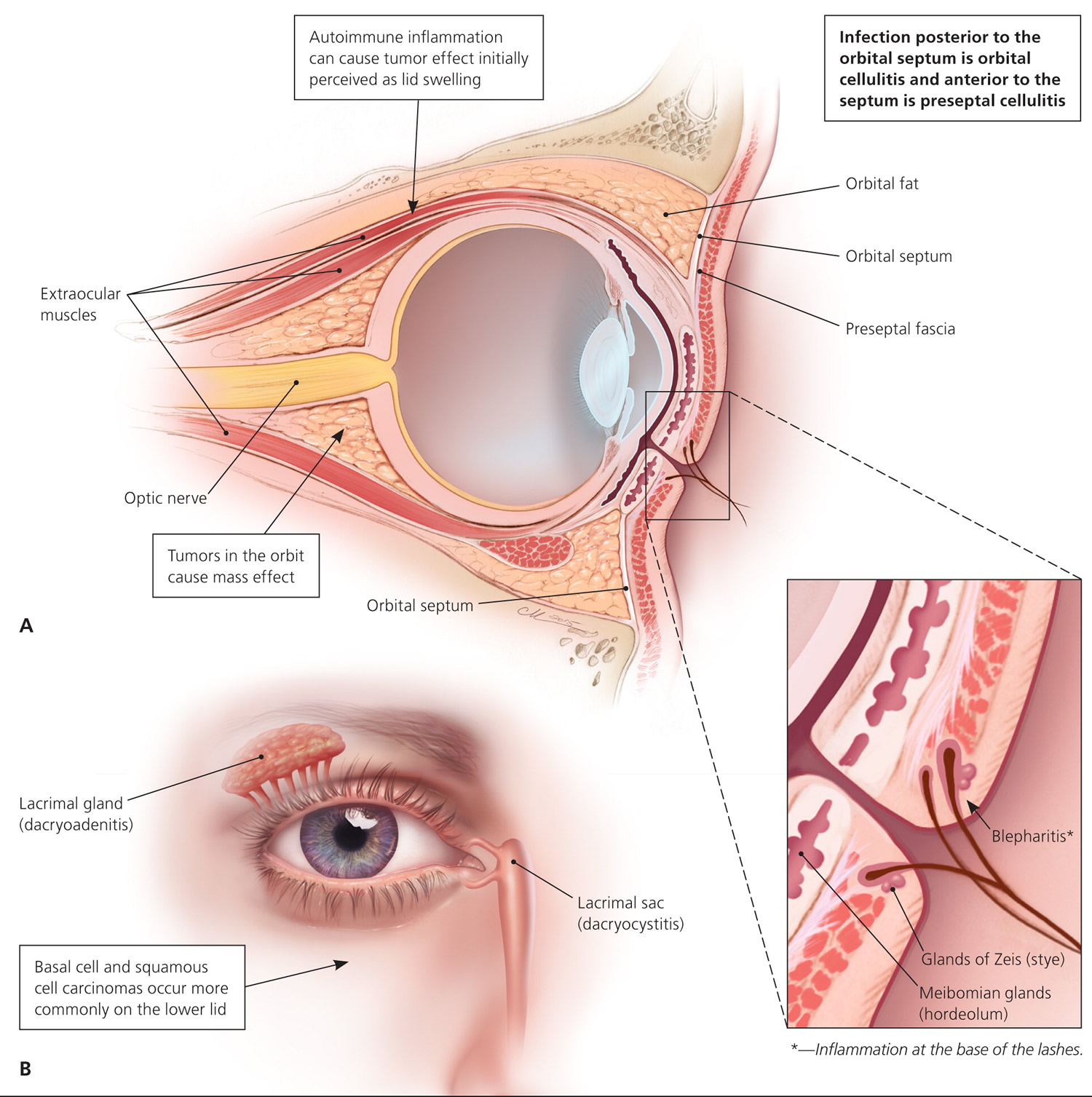
Figure 3. Eyelid anatomy
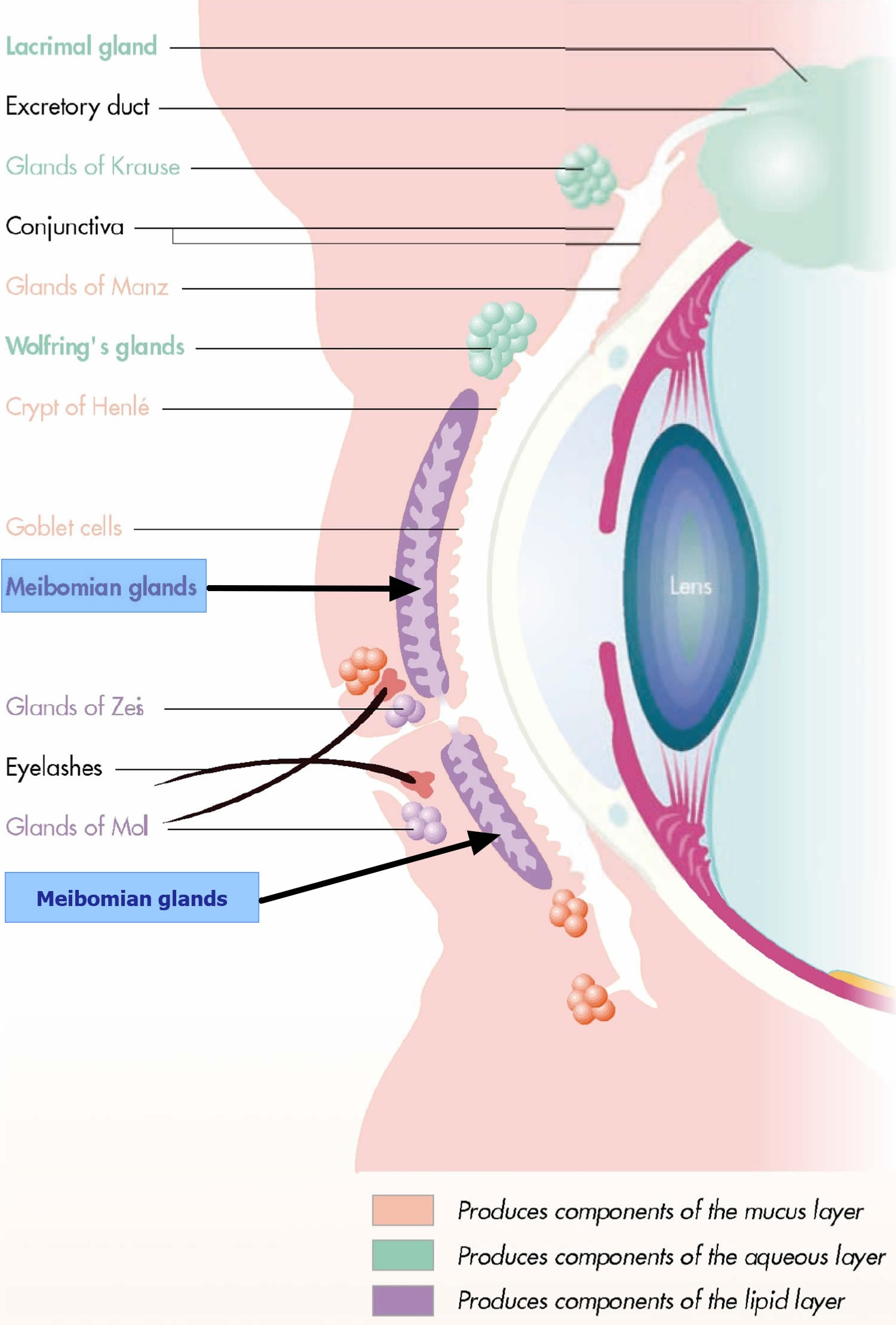
Figure 4. Upper Eyelid anatomy
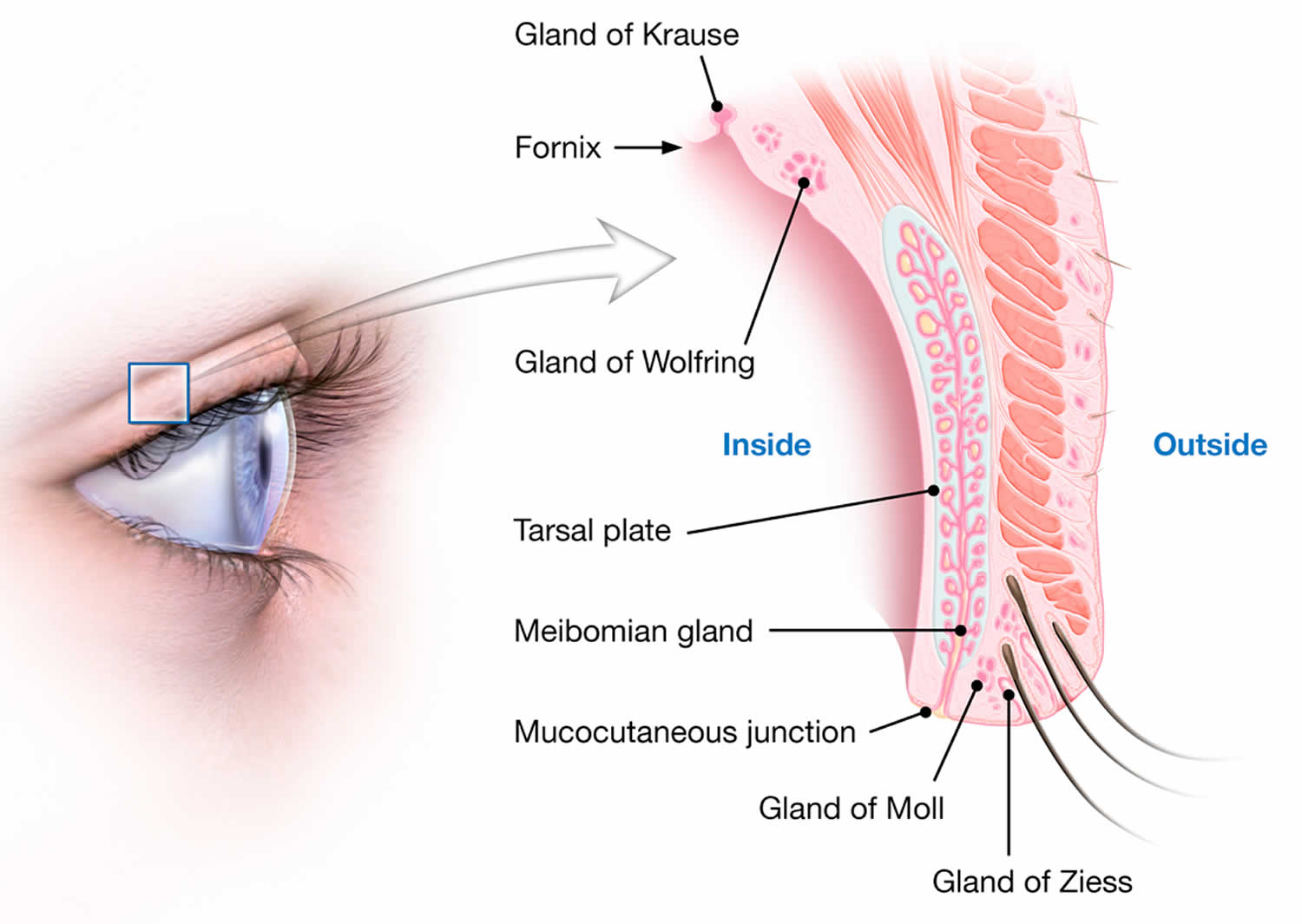
Table 1. Conditions That Present with Eyelid Swelling
| Disease | Causes | Signs and symptoms |
|---|---|---|
| Superficial skin processes | ||
| Atopic dermatitis | Skin manifestation of systemic allergic sensitivity | Raised, dry plaque |
| Basal cell carcinoma | Neoplastic changes | Raised, umbilicated lesion with overlying telangiectasia |
| Capillary hemangioma | Localized growth of capillaries | Flat or raised well-circumscribed erythema; increases in size with crying |
| Contact dermatitis | Local reaction to irritative agent | Irritation, erythema, and edema |
| Herpes zoster ophthalmicus | Varicella zoster virus infection | Vesicles with surrounding erythema, possible bacterial superinfection; distributed unilaterally on forehead and upper eyelid in a dermatome |
| Periorbital ecchymosis (“black eye”) | Blunt trauma to orbit resulting in disruption of blood vessels | Ecchymosis increasing in size over 48 hours, then slowly improving |
| Squamous cell carcinoma | Neoplastic changes | Painless erythematous flaky plaques, nodules, or ulcers |
| Inflammatory eyelid processes | ||
| Blepharitis | Inflammation of the base of the eyelashes and/or distal aspects of the eyelids; inflammation of the lacrimal gland | Irritated lid edges or eyelash |
| Chalazion | Noninfectious obstruction of meibomian tear gland | Discrete mass within the lid present for two or more weeks |
| Dacryoadenitis | Inflammation of the lacrimal gland | Circumscribed tender mass in upper outer lid; if advanced, may appear as the diffuse inflammation of preseptal cellulitis |
| Dacryocystitis | Inflammation of the lacrimal sac and duct | Tender mass at the medial aspect of the lower eyelid; if advanced, may appear as the diffuse inflammation of preseptal cellulitis |
| Hordeolum or stye | Hordeolum: infection of the meibomian (sebaceous) glands | Papule or furuncle at distal lid margin |
| Stye: infection of the sweat gland (gland of Zeis) of the eyelid | ||
| Local infections | ||
| Orbital cellulitis | Infection of the soft tissues within the orbit, posterior to the orbital septum, often due to spread from local sinus disease | Red, swollen, tender eyelid; extraocular movements limited because of pain or muscle edema; vision changes, diplopia; in children, fever and ill appearance |
| Preseptal cellulitis | Infection of lid tissues around the orbit, often with local skin defect | Red, swollen, tender eyelid; full extraocular movements; no vision changes |
| Mass effect from the orbit | ||
| Autoimmune orbital mass effect | Edema and inflammation of ocular muscles | Subacute onset bilateral proptosis, possible limited extraocular movements |
| Cavernous sinus thrombosis | Thrombosed superior ophthalmic vein and cerebral veins | Headache, vomiting, vision changes, stupor |
| Endophthalmitis | Inflammation of the globe, often caused by penetrating trauma | Vision loss |
| Orbital neoplasm | Tumor effect causing proptosis and affecting ocular muscle function and nerve function | Subacute onset, unilateral, painless proptosis |
Superficial Skin Processes
Herpes zoster ophthalmicus is an infection with the varicella zoster virus. It most commonly affects the frontal nerve branch of the fifth cranial nerve. Like those found elsewhere on the body, herpes zoster lesions involve the dermal tissue, leading to erythematous macules, papules, and vesicles. Lesions are typically distributed on the forehead and upper eyelid, and do not cross the midline. Hutchinson sign is the presence of vesicles on the nose, and may indicate a higher risk of ocular involvement. Cutaneous complications include ptosis, lid scarring, entropion, ectropion, depigmentation, and necrosis 9. Recognition of herpes zoster ophthalmicus and treatment with antiviral therapy is important to prevent adverse effects on the cornea and vision 10.
Basal cell carcinoma and squamous cell carcinoma account for most malignant processes of the eyelid. They are more common on the lower eyelid 11. Basal cell carcinoma accounts for 80% to 95% of eyelid and medial canthus malignancies, whereas squamous cell carcinoma accounts for 5% to 10% 12. Malignant melanoma can also involve the eyelid.13 Other less common malignancies have been reported 13.
The red tumorous growth of a capillary hemangioma can occur on the eyelid 14. In an infant, vigorous crying can make the vascular overgrowths more noticeable or larger 15.
Figure 5. Herpes simplex of the upper eyelid

Inflammatory Eyelid Processes
Hordeolum or stye
Hordeolum or stye is an acute, purulent inflammation of the eyelid margin usually caused by obstructed orifices of the sebaceous glands of the eyelid, usually caused by an infected eyelash root commonly caused by bacterial infection of the follicle of the eyelash 16. Stye, which affects sebaceous glands internally or externally, is common. When the meibomian gland in the tarsal plate is affected, internal hordeolum occurs. And when the glands of Zeis or Moll associated with eyelash follicles are affected, external hordeolum, or stye occurs. The onset of hordeolum is usually self limited, and may resolve in about a week with spontaneous drainage of the abscess. When the condition is severe, it can spread to adjacent glands and tissues. Recurrences are very common. As long as an internal hordeolum remains unresolved, it can develop into a chalazion or generalized eyelid cellulitis.
A internal hordeolum is an infection of the internal meibomian (sebaceous) gland, whereas a stye (external hordeolum) is an infection of the external Zeis (sweat) gland 17. These localized masses appear as papules and furuncles located distally at the lid edge 16. They typically resolve spontaneously within a few days or weeks, and warm compresses can help 16. Chronic hordeolum can lead to chalazion 17.
There are two kinds of styes:
- External hordeolum: A stye that begins at the base of your eyelash due to a blockage with secondary inflammation of the Zeiss or Moll sebaceous glands of the eyelid. Most are caused by an infection in the hair follicle. It might look like a pimple.
- Internal hordeolum: A stye inside your eyelid. Most are caused by an infection in an oil-producing internal meibomian (sebaceous) gland in your eyelid.
What is the difference between a stye and a chalazion ?
- Sometimes it can be difficult to tell the difference between a stye and a chalazion.
- A stye is an infection of an oil gland in the eyelid. It is like a small abscess or “boil” on the edge of the eyelid.
- A chalazion is a small or large bump on the eye lid caused by a blocked meibomian sebaceous glands in the eyelid.
You can also get a stye if you have blepharitis. This is a condition that makes your eyelids at the base of the eyelashes red and swollen.
When you first get a stye, your eyelid is probably red and tender to the touch. Your eye may also feel sore and scratchy.
A chalazion is not usually painful. It is a bump that usually develops farther back on the eyelid than a stye. It is caused by a clogged meibomian oil gland. Rarely does it make the entire eyelid swell.
What are the treatment options for stye and chalazion ?
Here are ways to treat your stye or chalazion:
- Warm compresses
Soak a clean washcloth in hot water and hold it to your eyelid for 10–15 minutes at a time, 3–5 times a day. Keep the cloth warm by soaking it in hot water often. For a chalazion, this warm compress helps the clogged oil gland to open and drain. You can help the gland clear itself by gently massaging around the area with your clean finger.
- Antibiotics
Your ophthalmologist may prescribe an antibiotic for an infected stye.
- Steroid shots
If your chalazion is very swollen, your ophthalmologist may give you a steroid shot (cortisone) to reduce the swelling.
- Surgery to drain the area
If your stye or chalazion affects vision or does not go away, you may need to have it drained. This surgery is usually done in the doctor’s office using local anesthesia.
If a stye or chalazion keeps coming back time after time, your ophthalmologist may biopsy it. This is where a tiny piece of tissue is removed and studied. This helps your ophthalmologist check to see if there is a more serious eye problem.
- Do not squeeze or try to pop a stye or chalazion
Doing so could spread the infection into your eyelid. Do not wear eye makeup or contact lenses while you have a stye or chalazion.
What are other treatment options for chalazion ?
Most chalazia resolve by themselves within several days to weeks, but sometimes can take months to completely disappear. Anti-inflammatory eye drops, ointments or an injection into the bump may be needed. Oral antibiotics may be used if the chalazion is associated with bacterial infection of the surrounding eyelid tissues (cellulitis). A large, swollen, or persistent chalazion might require surgical drainage. Although older children and adults can undergo the procedure in a doctor’s office under local anesthesia, general anesthesia is usually necessary to drain chalazia in young children.
Figure 6. Eyelid hordeolum (Stye)

Chalazion
A chalazion is a noninfectious mass surrounding the meibomian gland within the midportion of the eyelid 17. Chalazia tend to present for longer than two weeks compared with the shorter natural history of sties or internal hordeola (stye) 1. Chalazia may develop from hordeola or when sebum clogs the gland 17. The skin of the eyelid appears unremarkable without findings such as a papule 1. The resultant redness of the mass effect can be confused with cellulitis; however, chalazia are not painful 18. Surgical intervention with incision and drainage can be considered for very large chalazia 19. Intralesional steroid injections have also been used for treatment if conservative management with time and warm compresses is ineffective 20.
Figure 7. A chalazion is an enlargement of an oil-producing gland in the eyelid.

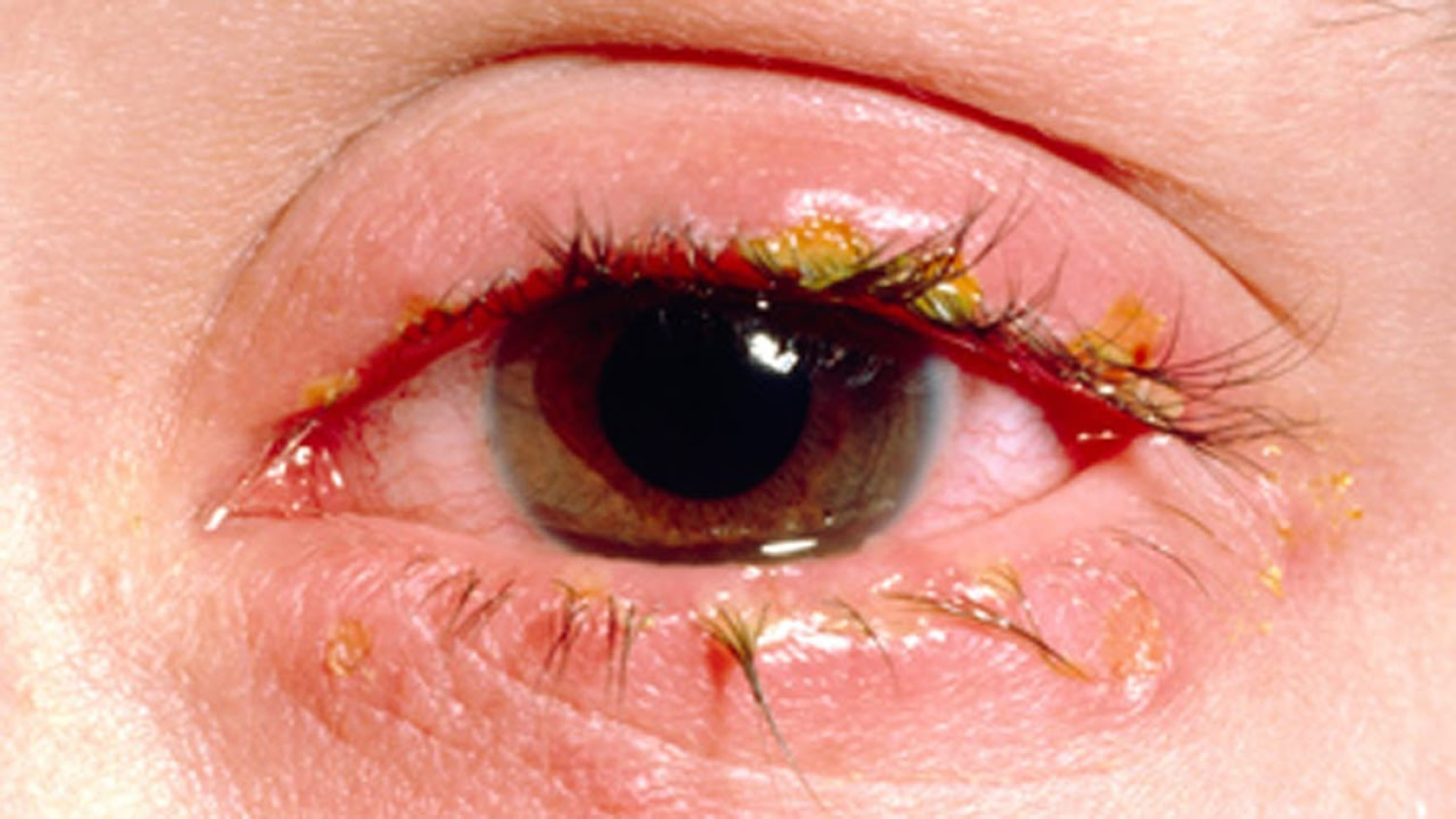
Blepharitis
Blepharitis is inflammation at the base of the eyelashes that can be chronic or acute, and is associated with dry eyes, seborrheic dermatitis, rosacea, and Demodex mite infestation. Symptoms are often worse in the morning. Treatments include warm compresses, gentle massage, washes with diluted baby shampoo, topical antibiotics, topical steroids, oral antibiotics, and combinations of these therapies 21.
Figure 8. Blepharitis
Dacryoadenitis
Dacryoadenitis is inflammation of the lacrimal glands, whereas dacryocystitis is inflammation of the lacrimal sac in the inferior lid 1. Both conditions can be caused by viruses or bacteria. Bacterial infections tend to be tenderer to palpation than viral infections. Staphylococcus, Streptococcus, and gram-negative organisms are common pathogens. Clinically, these processes may mimic preseptal cellulitis.
Other Eyelid skin problems
Bacterial skin infections
- External hordeola (stye, infection of the eyelash follicle, usually caused by staphylococcus bacteria )
- Internal hordeola (infection of the meibomian gland)
- Bacterial conjunctivitis
- Preseptal or orbital erysipelas or cellulitis (infections of the tissues around the eye), which is often due to spread from infection in the sinuses (responsible for 60-80% of orbital cellulitis), respiratory tract, impetigo, abscesses, trauma, or insect bites
Viral skin infections
- Viral conjunctivitis
- Herpes simplex (caused by the cold sore virus)
- Herpes zoster ophthalmicus (shingles, caused by the chickenpox virus)
- Viral warts
- Molluscum contagiosum
Figure 9. Eyelid viral wart

Figure 10. Eyelid molluscum contagiosum

Papules (a small pimple or swelling on the skin) and pustules (a small blister or pimple on the skin containing pus)
- Ocular rosacea
- Blepharitis
- Periorificial dermatitis
- Acne agminata
Growing solitary lesions
Skin cancers progressively enlarge.
- Basal cell carcinoma
- Actinic keratoses
- Intraepidermal carcinoma
- Squamous cell carcinoma
- Keratoacanthoma
- Atypical fibroxanthoma
- Sebaceous carcinoma
- Melanoma
Stable painless solitary lesions
- Mole (melanocytic naevus), including congenital melanocytic naevus
- Seborrhoeic keratosis
- Freckles and brown marks
- Chalazion (lipogranulomatous inflammation of the Zeis sebaceous gland at the base of the eyelash, or of the meibomian gland on the inner aspect of the lid; due to occlusion) – a firm, painless swelling
- Salmon patch (angel’s kiss)
- Suderiferous cyst (transparent papule containing clear fluid)
- Other types of cyst
- Trichoepithelioma.
- Wald ER. Periorbital and orbital infections. Infect Dis Clin North Am. 2007;21(2):393–408, vi.
- Klotz SA, Penn CC, Negvesky GJ, Butrus SI. Fungal and parasitic infections of the eye. Clin Microbiol Rev. 2000;13(4):662–685.
- Roscoe DL, Hoang L. Microbiologic investigations for head and neck infections. Infect Dis Clin North Am. 2007;21(2):283–304, v.
- Baynham JT, Newman SA. Ocular vaccinia with severe restriction of extraocular motility. Arch Ophthalmol. 2009;127(12):1688–1690.
- Lessner A, Stern GA. Preseptal and orbital cellulitis. Infect Dis Clin North Am. 1992;6(4):933–952.
- Givner LB. Periorbital versus orbital cellulitis. Pediatr Infect Dis J. 2002;21(12):1157–1158.
- Rudloe TF, Harper MB, Prabhu SP, Rahbar R, Vanderveen D, Kimia AA. Acute periorbital infections: who needs emergent imaging? Pediatrics. 2010;125(4):e719–e726.
- Differential Diagnosis of the Swollen Red Eyelid. Am Fam Physician. 2015 Jul 15;92(2):106-112. http://www.aafp.org/afp/2015/0715/p106.html
- Liesegang TJ. Herpes zoster ophthalmicus natural history, risk factors, clinical presentation, and morbidity. Ophthalmology. 2008;115(2 suppl):S3–S12.
- Severson EA, Baratz KH, Hodge DO, Burke JP. Herpes zoster ophthalmicus in Olmsted County, Minnesota: have systemic antivirals made a difference? Arch Ophthalmol. 2003;121(3):386–390.
- Gupta A, Stacey S, Amissah-Arthur KN. Eyelid lumps and lesions. BMJ. 2014;348:g3029
- Kolk A, Wolff KD, Smeets R, Kesting M, Hein R, Eckert AW. Melanotic and non-melanotic malignancies of the face and external ear—a review of current treatment concepts and future options. Cancer Treat Rev. 2014;40(7):819–837.
- Koay SY, Lee RM, Hugkulstone C, Rodrigues IA. A rapidly growing lid lump. BMJ Case Rep. Published online August 14, 2014.
- Peralta RJ, Warner TF, Potter HA, Albert DM. Adult capillary hemangioma. Arch Ophthalmol. 2012;130(8):999.
- Haik BG, Jakobiec FA, Ellsworth RM, Jones IS. Capillary hemangioma of the lids and orbit: an analysis of the clinical features and therapeutic results in 101 cases. Ophthalmology. 1979;86(5):760–792.
- Lindsley K, Nichols JJ, Dickersin K. Interventions for acute internal hordeolum. Cochrane Database Syst Rev. 2013;(4):CD007742.
- Lederman C, Miller M. Hordeola and chalazia. Pediatr Rev. 1999;20(8):283–284.
- Arbabi EM, Kelly RJ, Carrim ZI. Chalazion. BMJ. 2010;341:c4044.
- Gupta A, Stacey S, Amissah-Arthur KN. Eyelid lumps and lesions. BMJ. 2014;348:g3029.
- Wong MY, Yau GS, Lee JW, Yuen CY. Intralesional triamcinolone acetonide injection for the treatment of primary chalazions. Int Ophthalmol. 2014;34(5):1049–1053.
- American Academy of Ophthalmology Cornea/External Disease Panel. Preferred practice pattern guidelines. Blepharitis. San Francisco, Calif: American Academy of Ophthalmology; 2013. https://www.aao.org/eye-health/diseases/what-is-blepharitis





{kind=link}