What is POEMS syndrome
POEMS syndrome is a rare paraneoplastic disorder associated with an underlying plasma cell dyscrasia 1. POEMS syndrome is also defined as a rare multisystem autoinflammatory
disorder caused by the improper growth of bone marrow cells, resulting in an abnormal accumulation of proteins (immunoglobulin) in tissues and organs 2. The acronym POEMS, first coined by Bardwick in 1980 3, refers to frequently occurring features of the syndrome that is defined by the presence of a peripheral neuropathy (P), a monoclonal plasma cell disorder (M), and other paraneoplastic features, the most common of which include organomegaly (O), endocrinopathy (E), skin changes (S), papilledema, edema, effusions, ascites, and thrombocytosis 4. Minimal criteria were a sensorimotor peripheral neuropathy and evidence of a monoclonal plasmaproliferative disorder 5. Other names for POEMS syndrome include osteosclerotic myeloma, Crow-Fukase syndrome, or Takatsuki syndrome 6 and it was first reported by Scheinker in 1938 7. POEMS syndrome is slightly more common in men than women with the ratio of male to female of 9 : 5, and the average age was 47.1 years (range: 39–68 years).
Dispenzieri et al 5 proposed widely accepted POEMS syndrome diagnostic criteria in 2003 in an attempt to standardize the various features and investigation findings necessary to make a diagnosis of POEMS syndrome (see Table 1). Polyneuropathy and a monoclonal plasma cell disorder are hallmarks of the clinical disease, and therefore mandatory criteria for diagnosis. As is typical in medicine, textbook definitions rarely reflect what is seen in clinical practice. Although there are clear diagnostic criteria, POEMS syndrome remains notoriously difficult to diagnose. Although 95% of cases have a monoclonal lambda light chain plasma cell dyscrasia 8 coupled with the highly sensitive biomarker VEGF 9, misdiagnosis remains likely. The heterogeneity of clinical presentations, with patients commonly presenting with only a limited number of the features described, contributes to the diagnostic difficulties. The subtlety or lack of bone marrow abnormality provides false reassurance of the absence of a monoclonal plasma cell disorder. The typically inflammatory neuropathy mimics that of the much more familiar chronic inflammatory demyelinating polyradiculoneuropathy; over 60% of patients are initially misdiagnosed with chronic inflammatory demyelinating polyradiculoneuropathy or monoclonal gammopathy of underdetermined significance-associated peripheral neuropathy 10, resulting in treatment with ineffective immunomodulatory therapy and subsequent clinical deterioration due to delayed diagnosis by a median of 12 months 10. Therapies that may be effective in patients with chronic inflammatory demyelinating polyneuropathy and monoclonal gammopathy of underdetermined significance-associated peripheral neuropathy (intravenous gammaglobulin and plasmapheresis) are not effective in patients with POEMS syndrome. Not until additional features of the POEMS syndrome are recognized is the correct diagnosis made and effective therapies initiated. Clues to an early diagnosis include thrombocytosis and sclerotic bone lesions on plain skeletal radiographs.
Features such as endocrinopathy, papilloedema and skin conditions are non-specific, and may not typically be attributed to a neurological syndrome. Furthermore, subtle investigation findings may be misinterpreted or downplayed, resulting in reports that may not synthesise the whole picture. With all the diagnostic uncertainty and misleading information in such a complex disease, it is little wonder clinicians fail to consider the diagnosis.
POEMS stands for these signs and symptoms:
- Polyneuropathy. Numbness, tingling and weakness in your legs — and over time, maybe in your hands — and difficulty breathing.
- Organomegaly. Enlarged spleen, liver or lymph nodes.
- Endocrinopathy. Abnormal hormone levels that can result in underactive thyroid (hypothyroidism), diabetes, sexual problems, fatigue, swelling in your limbs, and problems with metabolism and other essential functions.
- Monoclonal plasmaproliferative disorder. Abnormal bone marrow cells (plasma cells) that produce a protein (monoclonal protein) that can be found in the bloodstream.
- Skin changes. More color than normal on your skin, possibly thicker skin and increased facial or leg hair.
Virtually all patients with POEMS syndrome will have either sclerotic bone lesion(s) or co-existent Castleman’s disease. Not all features of the disease are required to make the diagnosis, and early recognition is important to reduce morbidity. Elevation of proangiogenic and pro-inflammatory cytokines are the hallmark in the pathogenesis of this disorder 11. High levels of interlcukin-1β (IL-1β), interlcukin-6 (IL-6), tumor necrosis factor-α (TNF-α), and vascular endothelial growth factor (VEGF) were detected in the serum of POEMS syndrome patients 12. Among these cytokines, vascular endothelial growth factor (VEGF), probably over-secreted by plasma cells, appears to be the dominant driving cytokine and may be causative for effusions, pulmonary hypertension, and disseminated intravascular coagulation (DIC) in POEMS syndrome 13.
Table 1. Criteria for the diagnosis of POEMS syndrome
| Major criteria | Polyneuropathy |
| Monoclonal plasmaproliferative disorder | |
| Minor criteria | Sclerotic bone lesions† |
| Castleman disease† | |
| Organomegaly (splenomegaly, hepatomegaly, or lymphadenopathy) | |
| Edema (edema, pleural effusion, or ascites) | |
| Endocrinopathy (adrenal, thyroid,‡ pituitary, gonadal, parathyroid, pancreatic‡) | |
| Skin changes (hyperpigmentation, hypertrichosis, plethora, hemangiomata, white nails) | |
| Papilledema | |
| Known associations | Clubbing |
| Weight loss | |
| Thrombocytosis | |
| Polycythemia | |
| Hyperhidrosis | |
| Possible associations | Pulmonary hypertension |
| Restrictive lung disease | |
| Thrombotic diatheses | |
| Arthralgias | |
| Cardiomyopathy (systolic dysfunction) | |
| Fever | |
| Low vitamin B12values | |
| Diarrhea |
* Two major criteria and at least 1 minor criterion are required for diagnosis.
† Osteosclerotic lesion or Castleman disease is usually present.
‡ Because of the high prevalence of diabetes mellitus and thyroid abnormalities, this diagnosis alone is not sufficient to meet this minor criterion.
[Source 5]The cause of POEMS syndrome isn’t known. But people with POEMS syndrome have an increased number of plasma cells. These cells produce an abnormal amount of a type of protein, which can damage other parts of the body.
Once the diagnosis is made, there are still uncertainties regarding treatment. Treatment is directed at the underlying clonal plasma cell disorder and depends on the distribution of the disease and extent of bone marrow involvement. Novel chemotherapeutic agents and autologous stem cell transplantation allow for significant improvement of disease-free survival. Treatment selection, assessing response, monitoring disease and identifying relapses are complex and require multiple investigational modalities. Indeed, the multisystem nature of POEMS and its compounding disabilities requires multidisciplinary support and assistance.
Treatment for POEMS syndrome may improve your symptoms and has improved greatly over the past decade, but doesn’t cure the condition.
- Not all patients with POEMS syndrome present with the classic features described in the acronym.
- All patients presenting with an inflammatory neuropathy should be investigated for a monoclonal plasma cell proliferative disorder; if abnormal, they should be considered for serum VEGF.
- The combination of a demyelinating neuropathy, a lambda light chain paraprotein and raised VEGF is very likely to confirm POEMS syndrome and should prompt further investigations such as bone marrow biopsy and PET scan to ascertain the degree of monoclonal involvement.
- Patients are deemed to have focal or systemic disease based on the extent of monoclonal plasma cell dyscrasia, and this guides subsequent treatment options.
- Significant improvements in the neuropathy of POEMS syndrome can take up to 3 years following treatment.
Poems syndrome life expectancy
What is POEMS syndrome survival rate?
POEMS syndrome is a chronic condition. In many cases, there is progressive peripheral neuropathy that eventually causes mobility disability. A 93-patient follow-up data revealed that the median survival of patients with POEMS syndrome is 165 months or 13.75 years (see Figure 1 below) 5, while those with clubbing or extravascular volume overload (edema, effusion, or ascites) may have median survivals of 2.6 (31 months) and 6.6 years (79 months), respectively 5. These variables were independent of each other. Another research from China showed 80% patients were alive after follow-up time of 25 months, and 10% patients had survived more than 60 months 14. Death usually occurs from lack of nourishment or bronchopneumonia 15, neuropathy, along with stroke and myocardial infarction (heart attack), is the cause of death at last 5, 1. Patients who received radiation therapy and those who had a very good or good response to treatment also had superior survival (Figure 2).
Figure 1. Overall survival for 99 patients with POEMS syndrome evaluated at a single institution.
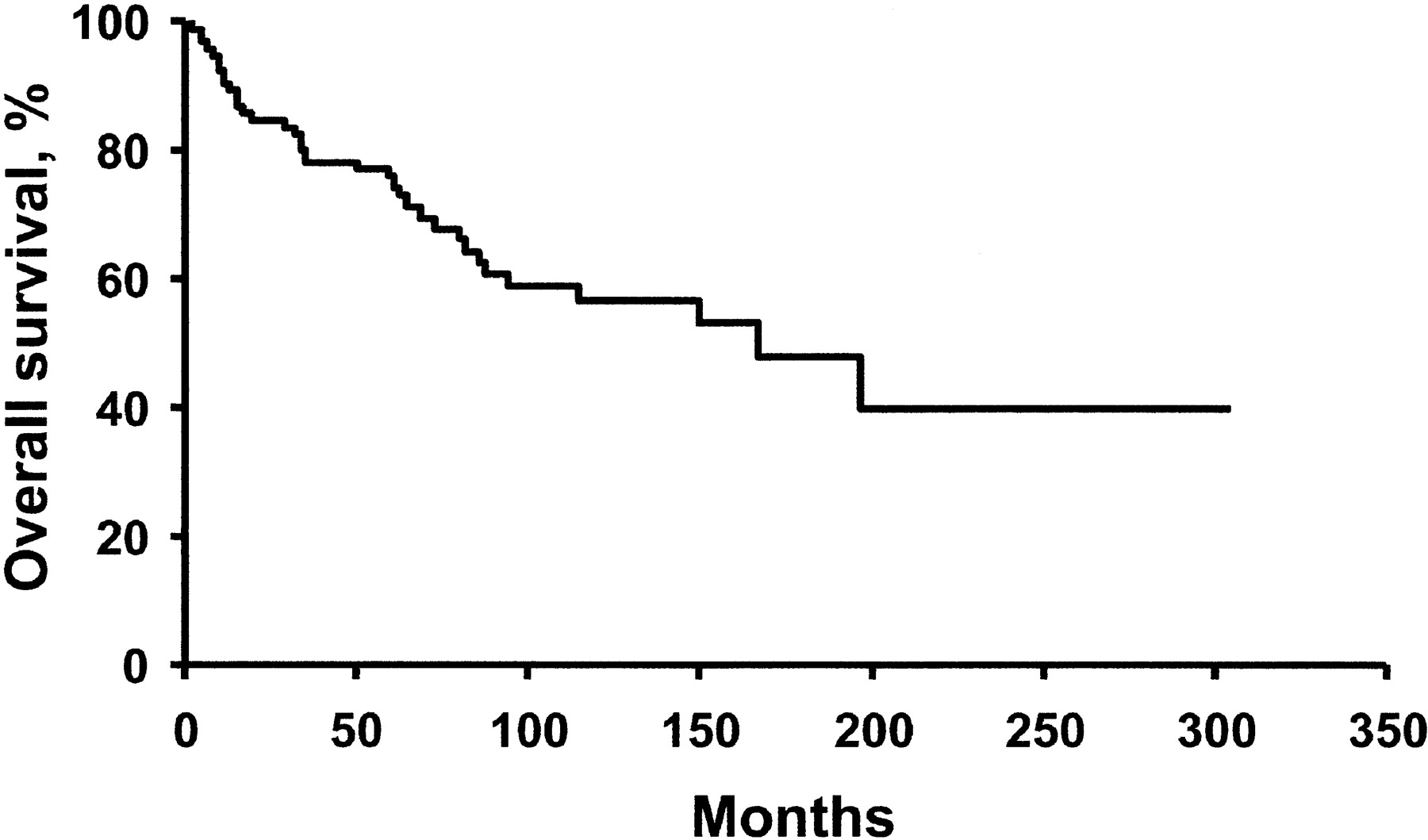
Figure 2. Survival on the basis of treatment with radiation and those who had a very good or good response to treatment survival rate
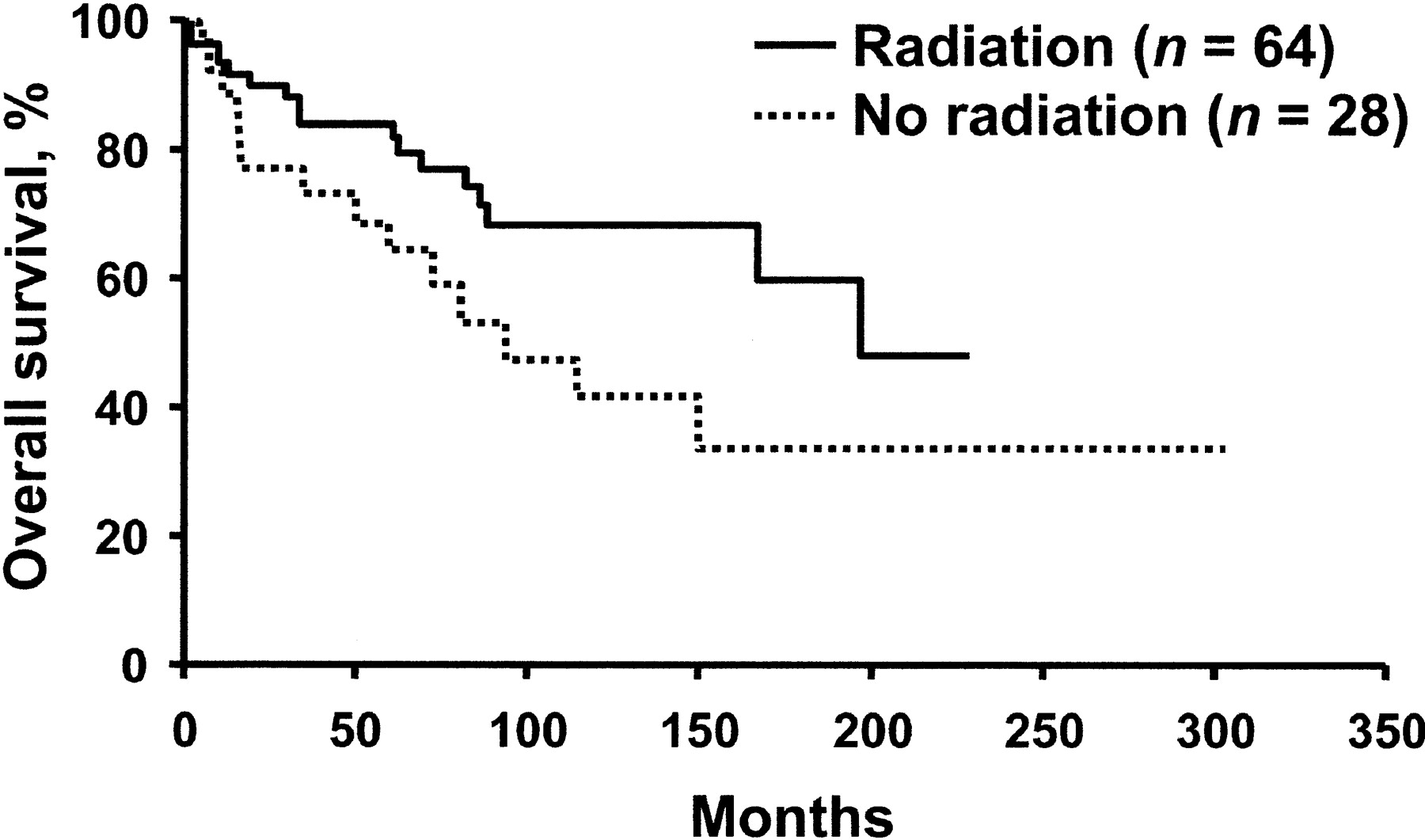
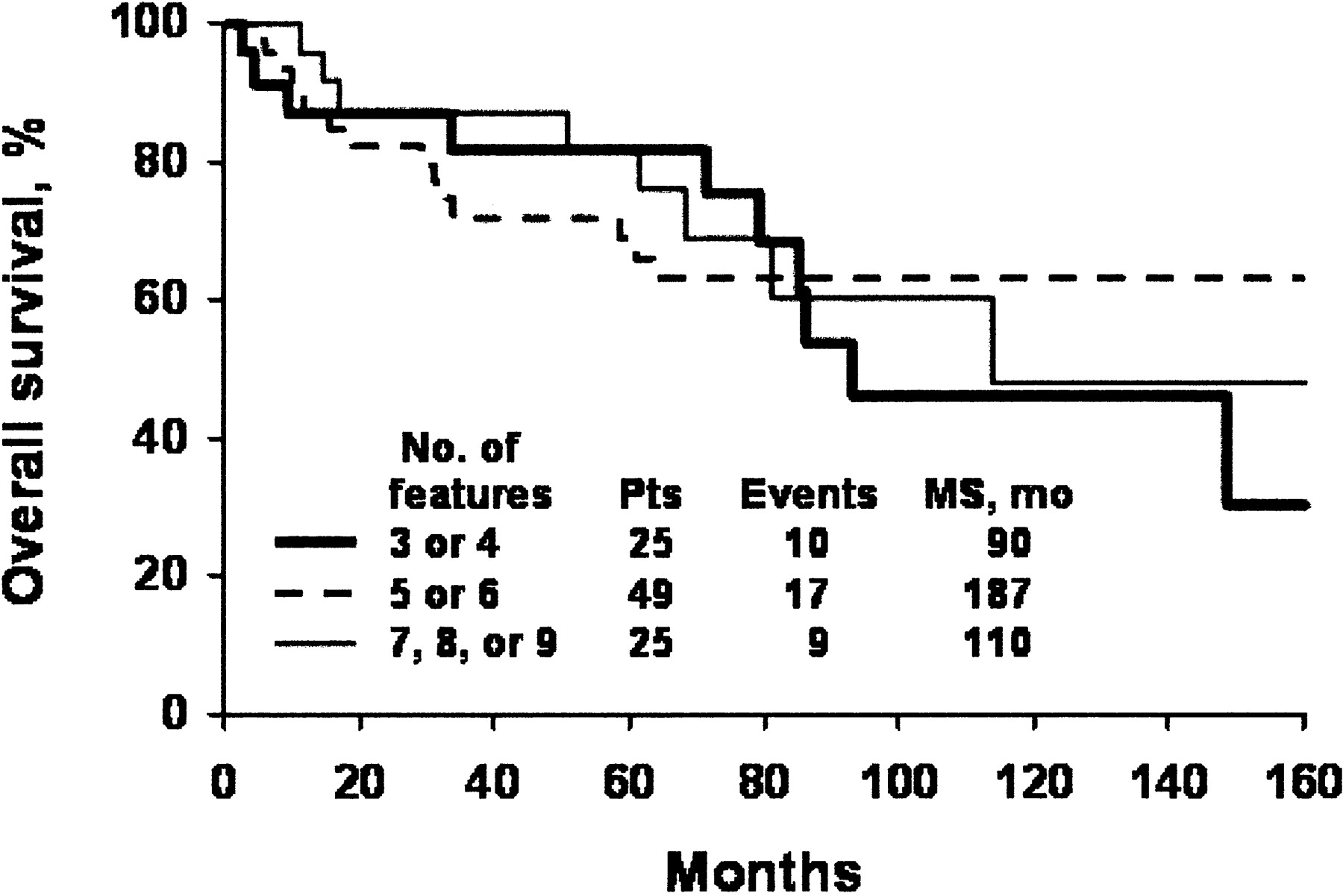
Figure 3. Survival rate on the basis of number of POEMS syndrome features at presentation
POEMS syndrome causes
The cause of POEMS syndrome is not well understood. POEMS syndrome is a paraneoplastic disorder, which means that the signs and symptoms of POEMS syndrome appear as a manifestation of the plasma cell disorder that the patient has (most patients are seen with osteosclerotic myeloma or monoclonal gammopathy of unknown significance); however, the mechanism by which this occurs is unknown. POEMS syndrome is associated with a chronic overproduction of some substances known as pro-inflammatory cytokines (small molecules that act as messengers between cells to promote inflammation). These include interleukins (IL-1b, IL6) which are cytokines that help regulate immune responses, TNFα (Tumor Necrosis Factor alfa is a cytokine which is involved in the inflammatory process) and vascular endothelial growth factor (VEGF – a powerful vasodilator that may cause leaky blood vessels) which seem to be important in this disorder. Reported treatment trials blocking VEGF with bevacizumab resulted in worsening of neuropathy and some deaths 16. VEGF is therefore a useful biomarker for disease detection and monitoring, but its role in pathogenesis is poorly understood.
POEMS syndrome symptoms
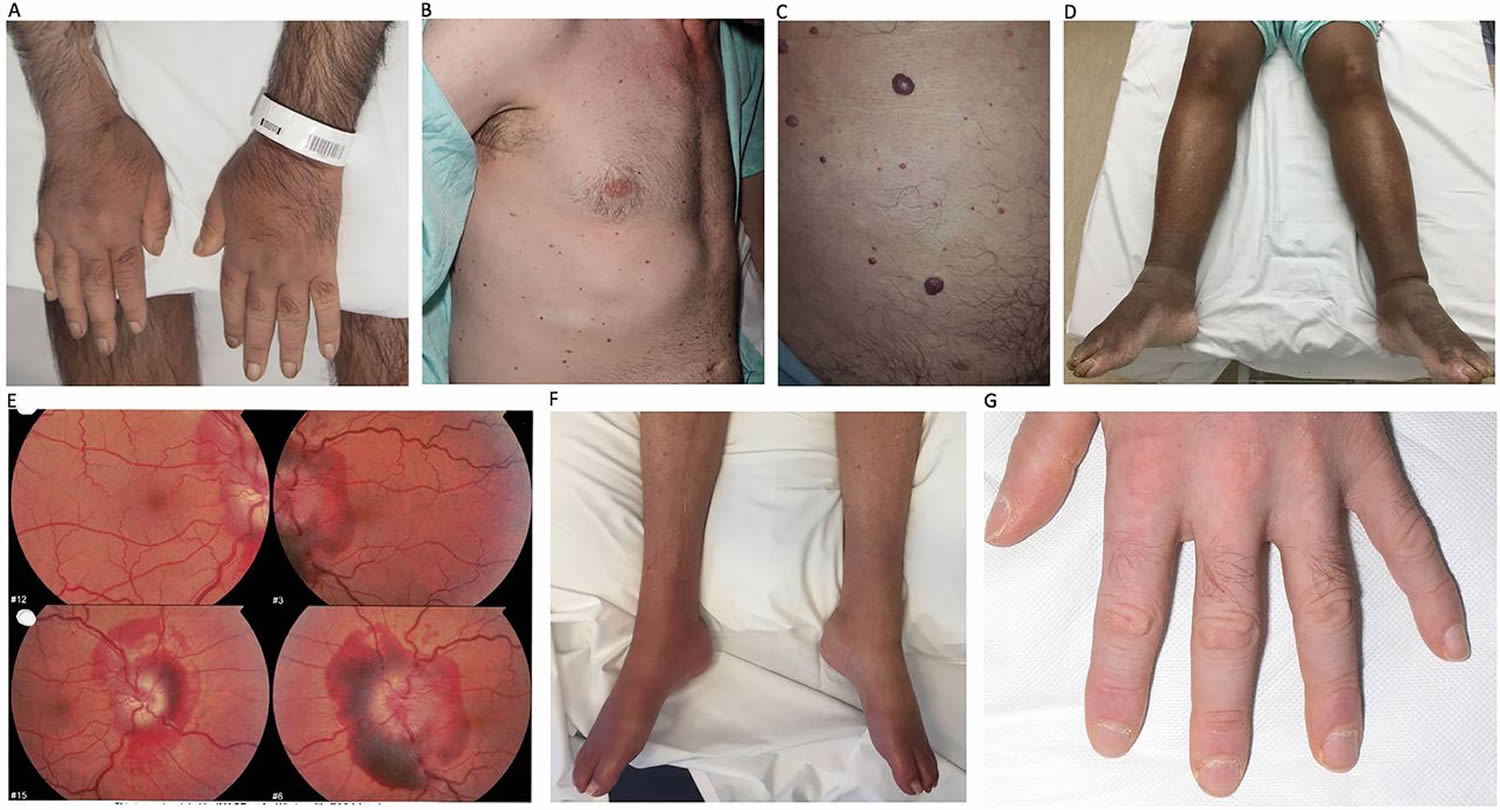
Figure 4 below show the typical features of POEMS syndrome. (A) Evidence of peripheral oedema and hypertrichosis. (B) Multiple glomerular haemangiomata across the trunk with 4x2cm area of vitiligo. (C) A collection of glomerular haemangiomata across the trunk of various sizes. (D) Marked lower limb peripheral oedema. (E) Retinal photography demonstrating bilateral sub-retinal haemorrhagic papilloedema. (F) Characteristic signs of lower limb distal wasting and acrocyanosis (note right lower limb coronary artery bypass graft). (G) Nailfold changes and hypertrichosis.
Figure 4. POEMS syndrome clinical features
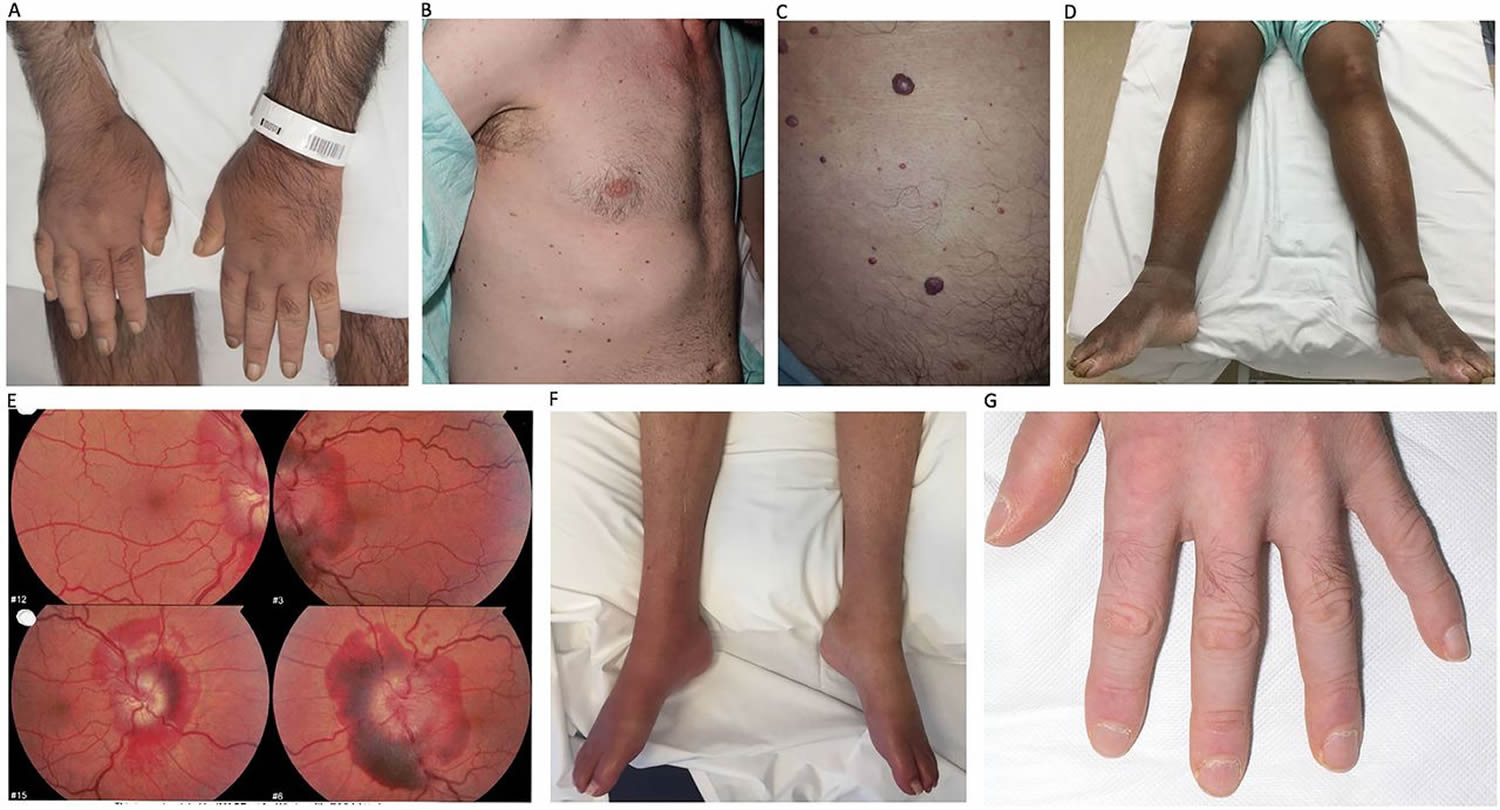
Figure 5. POEMS syndrome clinical features
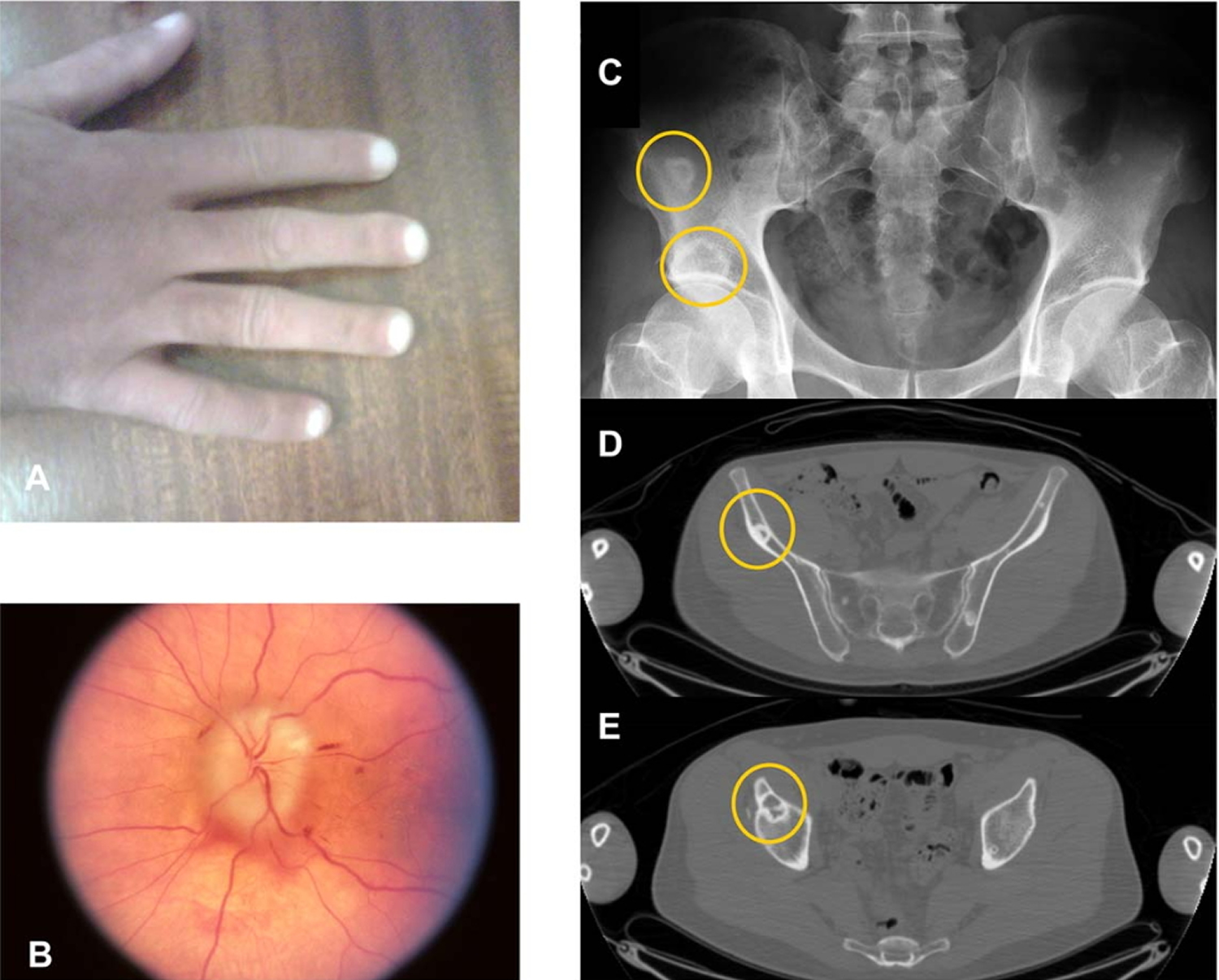
Note: (A) Skin changes including white nails and cyanosis. (B) Optic disc edema. (C-E) Mixed lytic osteosclerotic bone lesions on plain radiograph (C) and CT scan (D and E).
In addition to the characteristics described by the POEMS acronym above and in the tables below, patients may also experience:
- Changes in vision
- Easy fatigue
- Enlarged breast area tissue (in both women and men)
- Failure of ovaries and testes to function
- Fluid retention in the abdomen
- Swollen ankles and legs
- Weakness in the feet, legs, hands and arms caused by nerve damage
All patients with POEMS syndrome have peripheral neuropathy and a monoclonal plasma cell dyscrasia or Castleman disease. Hepatomegaly, splenomegaly, lymphadenopathy, endocrinopathy, skin changes, papilledema, peripheral edema, ascites, sclerotic bone lesions, clubbing, polycythemia, thrombocytosis, and fatigue 5.
The initial clinical manifestation was multifarious, including motorial symptoms (weakness) (57.1%), sensory symptoms (numbness) (35.7%), skin hyperpigmentation (78.6%), edema (50%), and abdominal distention (37.3%). The typical clinical features of these patients were listed in Tables 1 and 2 below.
Blood routine and urinalysis of the 14 patients revealed that five of them had thrombocytosis (35.7%), two had microscopic hematuria (14.3%), and four had proteinuria (28.6%). Renal insufficiency occurred in five patients (35.7%). One of them experienced renal biopsy and was diagnosed with IgA nephropathy.
Laboratory tests exhibited that 10 patients had thyroid hypofunction. Hypoadrenocorticism and hypoparathyroidism were seen in individual patient. The concentration of gonadal hormone lowered significantly in two patients (1 male and 1 female).
Three of the seven patients who had lymphadenopathy underwent lymph node biopsy. All were diagnosed with Castleman disease histopathologically. One sample showed λ-light chain (+) after immunohistochemical staining indicating monoclonal plasmaproliferative disorder.
Nerve conduction/EMG studies of all patients showed prolonged distal motorial latency and slowed velocity of both motorial and sensory nerve conduction. One patient had sural nerve biopsy and showed infiltration of lymphocytes around vessels in epineurium and partial demyelination while neuraxon intact.
Among the 14 patients, 11 had bone marrow aspiration. Two patients (18.2%) had a slight increase in plasma cells (more than 2%). Two (18.2%) had more than 5% plasma cells, but no definite signs of multiple myeloma. The rest had normal plasma cells. In patients who had radiographic bone survey and isotope bone scan, no sclerotic or lytic lesions were found.
Table 2. Presenting clinical characteristics of 99 patients with POEMS syndrome
| Characteristic | % |
|---|---|
| Median age, y (range) | 51 (30-83) |
| Race | |
| African American | 8 |
| Asian | 0 |
| Hispanic | 3 |
| Non-Hispanic white | 89 |
| Male sex | 63 |
| Patients with given no. of classic POEMS features | |
| 2 features | 7 |
| 3 features | 32 |
| 4 features | 31 |
| 5 features | 29 |
| Patients with given no. of revised POEMS features | |
| 3 features | 6 |
| 4 features | 19 |
| 5 features | 32 |
| 6 features | 17 |
| 7 features | 16 |
| 8 features | 7 |
| 9 features | 2 |
| Laboratory value | |
| Albumin less than 3.0 g/dL (range) | 24 (2.3-4.5) |
| Bone marrow plasma cells more than 10% (range) | 14 (0-40) |
| Calcium more than 10.5 mg/dL (range) | 0 (7.8-10.2) |
| Creatinine more than 1.5 mg/dL (range) | 2 (0.5-1.9) |
| Erythrocyte sedimentation rate more than 29 mm/h (range) | 16 (1-58) |
| Hemoglobin less than 11 g/dL (range) | 4 (10.4-18.4) |
| Hemoglobin more than 16 g/dL (range) | 16 (10.4-18.4) |
| Leukocytes more than 10 500/μL (range) | 21 (3700-17 600) |
| Platelets more than 450 × 103/μL (range) | 54 (111-1163) |
| Serum M-spike more than 2.0 g/dL (range) | 7 (0.00-4.1) |
| Urine M-spike more than 0.5 g/24 h (range) | 0 (0.00-0.45) |
| Urine protein more than 1.0 g/24 h (range) | 5 (0.02-3.2) |
Table 3. Comparison of clinical characteristics of POEMS syndrome patients from 3 studies
| Characteristic | Dispenzieri et al study, % N = 99 5 | Soubrier et al, % N = 25 17 | Nakanishi et al, % N = 102 18 |
|---|---|---|---|
| Polyneuropathy | |||
| Peripheral neuropathy | 100 | 100 | 100 |
| Cerebrospinal fluid protein more than 50 mg/dL | 100 | 100 | 97 |
| Organomegaly | 50 | NR | NR |
| Hepatomegaly | 24 | 68 | 78 |
| Splenomegaly | 22 | 52 | 35 |
| Lymphadenopathy | 26 | 52 | 61 |
| Castleman disease | 11 | 24 | 19 |
| Endocrinopathy | 67 | NR | NR |
| Gonadal axis abnormality | 55 | NR | NR |
| Adrenal axis abnormality | 16 | NR | NR |
| Increased prolactin value | 5 | NR | NR |
| Gynecomastia or galactorrhea | 18 | NR | NR |
| Diabetes mellitus | 3 | 36 | 25 |
| Hypothyroidism | 14 | 36 | NR |
| Hyperparathyroidism | 3 | NR | NR |
| Monoclonal plasma cell dyscrasia | 100 | 100 | 75 |
| M component on serum protein electrophoresis | 54 | 100 | 70 |
| Skin changes | 68 | NR | NR |
| Hyperpigmentation | 46 | 48 | 93 |
| Acrocyanosis and plethora | 19 | NR | NR |
| Hemangioma/telangiectasia | 9 | 32 | NR |
| Hypertrichosis | 26 | 24 | 74 |
| Thickening | 5 | 28 | 61 |
| Papilledema | 29 | 40 | 55 |
| Extravascular volume overload | 29 | NR | NR |
| Peripheral edema | 24 | 80 | 89 |
| Ascites | 7 | 32 | 52 |
| Pleural effusion | 3 | 24 | 35 |
| Bone lesions | 97 | 68 | 54 |
| Osteosclerotic only | 47 | 41 | 56 |
| Mixed sclerotic and lytic | 51 | 59 | 31 |
| Lytic only | 2 | 0 | 13 |
| Solitary lesion | 45 | 41 | 45 |
| 2 or 3 lesions | 23 | NR | NR |
| More than 1 lesion | 54 | 59 | 45 |
| More than 3 lesions | 32 | NR | NR |
| Other features | |||
| Weight loss more than 10 pounds | 37 | NR | NR |
| Fatigue | 31 | NR | NR |
| Thrombocytosis: platelet count more than 450 × 103/μL | 54 | 88 | NR |
| Polycythemia: hemoglobin more than 15 g/dL in women and more than 17 g/dL in men | 18 | 12 | 19 |
| Clubbing | 5 | 32 | 49 |
NR indicates not reported.
Table 4. Clinical features of 14 patients with POEMS syndrome in China
| Polyneuropathy | |
| Peripheral neuropathy | 14/14 |
| Papilledema | 5/10 |
| Organomegaly | |
| Hepatomegaly | 8/14 |
| Splenomegaly | 11/14 |
| Lymphadenopathy | 7/14 |
| Endocrinopathy | |
| Hypothyroidism | 10/14 |
| Amenorrhea | 1/14 |
| Impotence | 2/14 |
| Hypoadrenocorticism | 1/14 |
| Hypoparathyroidism | 1/14 |
| M-protein | |
| IgA λ | 6/13 |
| IgA κ | 1/13 |
| IgM λ | 1/13 |
| IgG λ | 2/13 |
| Skin change | |
| Hyperpigmentation | 11/14 |
| Pruritus | 2/14 |
| Edema | |
| Peripheral edema | 7/14 |
| Effusions | 10/14 |
| Ascites | |
| Pleural effusion | 8/14 |
| Hydropericardium | 8/14 |
Polyneuropathy
All the patients had peripheral neuropathy confirmed by nerve conduction/EMG studies. Among these patients, eight had motorial deficit (57.1%), while five had sensory deficit (35.7%). Meanwhile, five patients (35.7%) presented sensorimotor deficit.
The neuropathy is usually symmetrical and ascending, with either insidious or rapidly progressing onset 5, and finally POEMS patients may be confined to a wheelchair.
Patients often describe numbness and dysesthesias followed by a progressive ascending weakness that overshadows the sensory impairment. In most patients, it is the presenting symptom; however, in one series edema preceded neuropathy in 12% of patients and coincided with it in 14% 20. The neuropathy is seldom painful, and autonomic involvement is rare 21. It is typically a chronic, large-fiber sensorimotor neuropathy.
Organomegaly
Organomegaly was the universal signs of all the patients (92.9%), in which splenomegaly (84.6%) was more common than hepatomegaly (61.5%) and lymphadenopathy (50.0%). Multiorganomegaly could be seen in 76.9% of them.
Endocrinopathy
Among the 14 patients of POEMS syndrome, 10 patients suffering from endocrinopathy all presented as hypothyroidism. In these patients, one had amenorrhea, two had impotence, one had hypoadrenocorticism, and one had hypoparathyroidism.
Monoclonal Plasmaproliferative Disorder
Of the 13 patients who had serum immunofixation detection, ten (76.9%) showed positive results of monoclonal plasma proliferative disorder. Six patients had abnormal immunoglobulin A (IgA) λ, two had IgG λ, one had IgA κ, and the rest had IgM λ. Another patient had both serum IgG and IgA elevation, while serum immunofixation remained negative.
Skin Changes
Of all the 14 patients, the most common abnormality was hyperpigmentation (11 patients, 78.6%), followed by pruritus (two patients, 14.2%).
Edema and Effusions
Most of the patients had edema and effusions of varying degrees. Seven had peripheral edema (50%), and 11 had serouscavity effusions (78.6%) including ascites (71.4%), pleural effusion (57.1%), hydropericardium (57.1%). Multiple serous cavity effusions were present in nine patients (64.3%).
Papilledema
Ten patients underwent fundus examination, and five were diagnosed with papilledema.
Sclerotic bone lesions
On presentation, 95 patients had at least one abnormality detected on radiographic bone survey. Of the 4 patients not presenting with a bone lesion, all had 4 or 5 features of POEMS syndrome, including a clonal plasmaproliferative disorder. In one patient, a sclerotic bone lesion developed 18 months later, yielding a total of 96 patients (97%) with abnormal findings on bone radiography. Of the patients with abnormal findings, all but 2 had sclerotic bone lesions. The radiographs for these 2 patients could not be located to establish whether there was any element of sclerosis associated with the lytic lesions. These 2 patients had solitary lytic lesions. Lytic lesions in patients with POEMS syndrome tend to have a sclerotic rim. Forty-nine patients had lesions with mixed sclerotic and lytic components. Forty-three patients had a solitary lesion, 22 had 2 or 3 lesions, and 31 had more than 3 lesions. These findings are consistent with those of previous publications 18. Twenty-two patients underwent biopsy of a sclerotic lesion; results were diagnostic in 20.
POEMS syndrome diagnosis
People who are suspected of having POEMS syndrome should first have their medical history evaluated and undergo a complete physical exam. Features suggestive of POEMS syndrome in the history include complaints of neurological symptoms, skin changes, signs of extravascular volume overload, and symptoms suggestive of an endocrine disorder (such as gynecomastia or irregular periods). A detailed physical exam should include an eye exam for papilledema; a neurologic exam; evaluation for enlargement of organs (organomegaly); examination of the skin; and evaluation for the presence of peripheral edema (swelling due to fluid accumulation), pleural or pericardial effusion (fluid build-up around the lungs or heart), ascites, clubbing (enlargement of the fingertips), heart failure, and cardiomyopathy.
A diagnosis of POEMS syndrome requires both the presence of polyneuropathy and a monoclonal plasma cell proliferative disorder, plus the presence of at least one major and one minor criterion on a physical exam, imaging, or laboratory evaluation. For reasons unknown, gammopathies in POEMS syndrome are characteristically IgA (52%) and IgG (47%), and almost never IgM 5. Lambda light chain predominates and occurs in 95% of POEMS cases 5. A monoclonal plasma cell disorder can be demonstrated through testing serum, urine or bone marrow, or through histopathology of a biopsy specimen. Serum protein electrophoresis, immunofixation and serum free light chain analysis must all be performed to detect a subtle plasma cell disorder with appropriate sensitivity. Many haematology laboratories do not provide immunofixation and serum free light chain analysis if preliminary investigations are unrevealing, and therefore neurologists must work with their laboratories to enable such testing as routine for all suspected POEMS syndrome cases.
POEMS syndrome Major criteria include:
- An osteosclerotic or mixed sclerotic/lytic lesion seen on plain films or CT scan measuring at least 0.8 cm in the longest dimension
- Castleman’s disease
- Elevated serum or plasma vascular endothelial growth factor (VEGF) levels at least 3 to 4 times the upper limit of normal
POEMS syndrome Minor criteria include:
- Organomegaly (enlargement of the spleen, liver, or lymph nodes)
- Extravascular volume overload (peripheral edema, ascites, or pleural effusion)
- Endocrinopathy (excluding diabetes mellitus or hypothyroidism)
- Skin changes
- Papilledema
- Thrombocytosis or polycythemia
Many affected people are initially misdiagnosed as having other disorders, such as chronic inflammatory demyelinating polyradiculoneuropathy. In addition, a number of conditions are associated with a plasma cell disorder and polyneuropathy (with or without osteosclerotic bone lesions), and need to be distinguished from POEMS syndrome.
Table 5. Investigative workup and tests for suspected POEMS syndrome cases
| Feature | Investigation | Typical abnormality | |
| Polyneuropathy | Nerve conduction studies/electromyography | Axonal and demyelinating; preferential lower limbs, intermediate>distal nerve conduction velocity slowing; conduction block (6%) and temporal dispersion unlikely | |
| Nerve biopsy† | Not necessary if diagnosis is clear with elevated VEGF levels; axonal degeneration, diffuse myelinated fibre loss, increased epineurial blood vessels; uncompacted myelin lamellae | ||
| Cerebrospinal fluid* | Albuminocytological dissociation; normal cell count; mild increase opening pressure; not specific so not always necessary | ||
| Organomegaly | CT scan of chest/abdomen/pelvis and PET-CT | Lymph node, spleen, liver | |
| Endocrinopathy† | Adrenal | Cortisol | Typically low: Addisonian |
| Thyroid | TSH, T4 | Hypothyroid or hyperthyroid | |
| Pituitary | LH, FSH, IGF-1, ACTH, prolactin | Typically hypofunctioning | |
| Gonadal | Testosterone, oestradiol | Typically low | |
| Parathyroid | PTH | ||
| Pancreatic | HbA1c, glucose | Typically raised | |
| Monoclonal plasma cell disorder | Serum protein electrophoresis | IgG or IgA lambda monoclonal, low kappa:lambda ratio | |
| Immunofixation | |||
| Serum free light chain analysis | |||
| Urine protein electrophoresis/immunofixation | Bence Jones protein | ||
| Bone marrow biopsy ±Targeted bone lesion biopsy | Presence of plasma cells on immunofixation, typically lambda light chain restricted | ||
| Skin | Clinical diagnosis; history and examination | Acrocyanosis, hypertrichosis, nail changes, glomerular haemangiomas | |
| Papilloedema | Ophthalmological assessment | ||
| Extravascular volume overload/cardiac involvement | Echocardiogram* | Reduction of left or right ventricular ejection fraction, elevation of pulmonary artery pressure; evidence of previous ischaemia | |
| Sclerotic bone lesions | CT bone windows, PET-CT imaging | Sclerotic lesions/mixed lytic with sclerotic | |
| Thrombocytosis | Full blood count | Increased platelets | |
| Pulmonary function | Pulmonary function tests* | Pulmonary hypertension, restrictive disease, respiratory muscle weakness, reduced diffusion capacity | |
*Test not essential for diagnosis, but useful.
†Endocrinopathy bloods should be taken fasted in the morning before breakfast.
PET, positron emission tomography; TSH, thyroid stimulating hormone; T4, thyroxine; LH, luteinising hormone; FSH, follicle stimulating hormone; IGF-1, insulin-like growth factor 1; ACTH, adrenocorticotropic hormone; PTH, parathyroid hormone; HbA1c, glycated hemoglobin; POEMS, polyneuropathy, organomegaly, endocrinopathy, the presence of a monoclonal plasma cell disorder and skin disease; VEGF, vascular endothelial growth factor.
[Source 22]POEMS syndrome treatment
Treatment focuses on alleviating the worst symptom of POEMS syndrome, which is the nerve damage that causes progressive weakness in the body’s extremities. Treatment also attempts to stop the production of the bone marrow cells that create problems in other parts of the body.
For peripheral neuropathy induced by POEMS syndrome:
- Discontinue drugs that cause peripheral neuropathy
- Institute non-drug treatments to reduce pain, such as:
- Avoiding extended periods of standing or walking
- Wearing looser shoes
- Pain medication
- Take safety measures to compensate for loss of sensation
- Ask your doctor about special therapeutic shoes
Currently, the treatments for POEMS syndrome include radiation, alkylators, corticosteroids, autologous-stem cell transplantation, bevacizumab, rituximab, bortezomib, and thalidomide 23, 24, 25, 26. In patients with a dominant sclerotic plasmacytoma, first-line therapy should contain radiation therapy to the lesion. For those patients with systemic manifestation, systemic therapy is indicated. Low dose alkylators with or without corticosteroids are effective in some patients. Furthermore, high-dose chemotherapy with autologous-stem cell transplantation dramatically improved manifestations and outcomes for POEMS syndrome patients 27.
A case of POEMS syndrome associated with Waldenstrom macroglobulinemia was treated by rituximab with thalidomide 28, which effectively decreased CD20-positive lymphoplasmacytic cells and improved patient’s neurological symptoms.
In 2009, Ohwada et al. 29 reported the first case of successful combination induction therapy of bevacizumab (anti-VEGF MoAb) and thalidomide, followed by autologous-stem cell transplantation. Bevacizumab could induce a dramatic decrease in the serum VEGF level, and thereby reduce pleural effusion and ascites with thalidomide to maintain low VEGF level. In summary, bevacizumab is efficacious for POEMS syndrome, when it is used in combination with other chemotherapeutics at the earlier stage. However recent trial results 16, 30 with anti-VEGF monoclonal, bevacizumab, have yielded ineffective, if not detrimental results.
The mainstay of treating POEMS syndrome is therefore through suppression of the monoclonal plasma cell proliferation. This can be done in several ways, depending on the extent of disease, comorbidities and patient fitness.
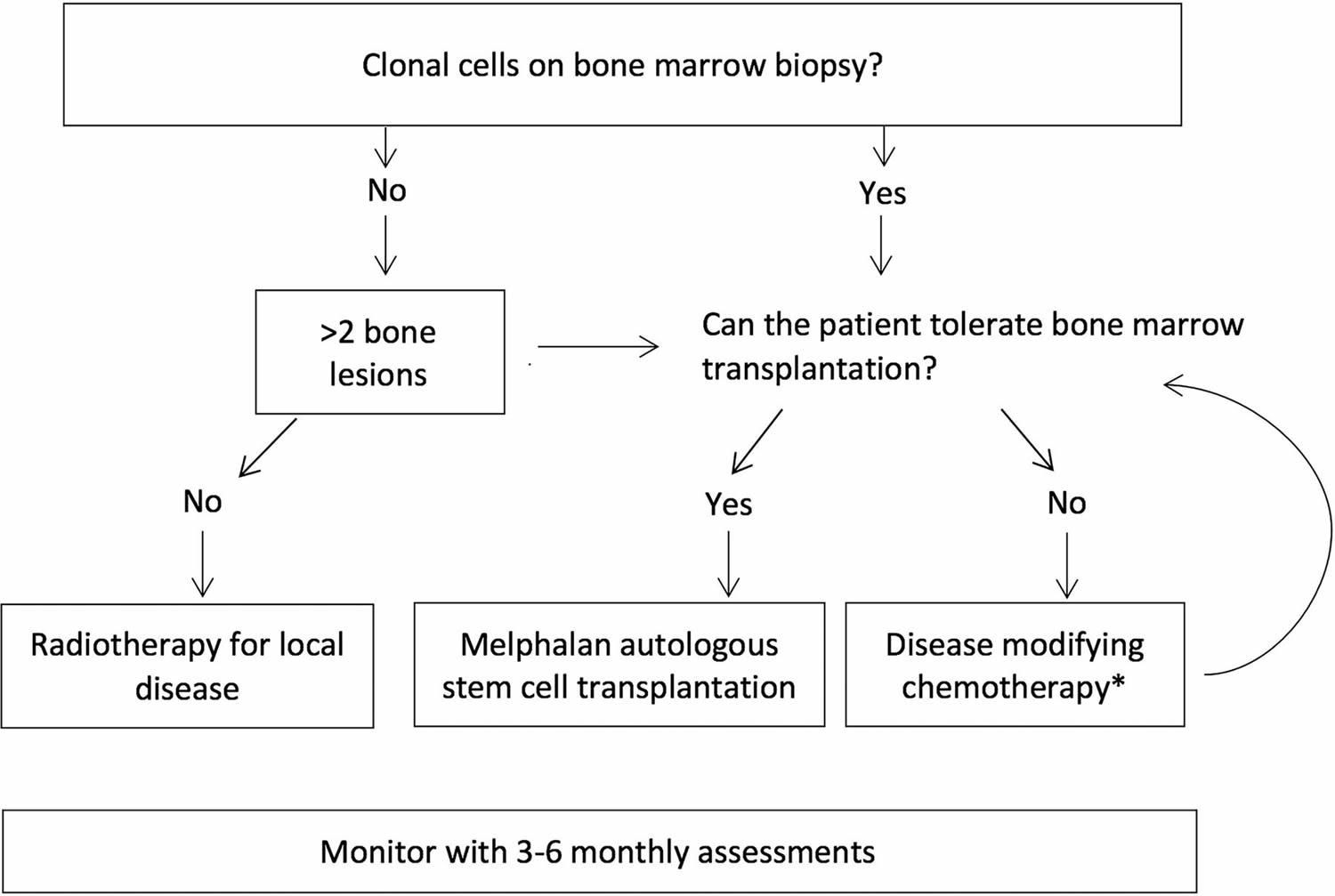
As mentioned before, the monoclonal plasma cell disorder can comprise diffuse bone marrow infiltration and/or solitary/multifocal plasmacytomas. Patients with bone marrow involvement on bone marrow biopsy, or three or more plasmacytomas, are considered to have systemic disease; two or fewer plasmacytomas is considered as focal disease. Figure 5 provides a treatment algorithm that depends on the extent of disease.
Figure 6. POEMS syndrome treatment algorithm
Focal disease (one or two plasmacytomas)
Radiotherapy to two or fewer plasmacytoma lesions is first-line treatment in focal disease. The objective is to obtain complete remission with minimal side effects while avoiding protracted treatment when compared with systemic therapies. From 67 patients with POEMS in this study 22, 22 have received radiotherapy as first line. Eleven went on to have second-line systemic therapy due to clinical or biochemical relapse, after an average of 22 months (median 13 months). Eleven patients have remained clinically stable, with the longest surviving patient at 19 years following radiotherapy.
Generalized disease (three or more plasmacytomas or positive bone marrow histology)
Patients with generalized disease require systemic treatment. Melphalan-conditioned autologous stem cell transplantation is the gold standard, with chemotherapy used for patients deemed unfit for transplantation 22.
Due to small patient numbers, treatment algorithms for POEMS syndrome have been adopted from multiple myeloma or light chain amyloidosis 22. High-dose chemotherapy plus autologous stem cell transplantation is the current gold standard treatment for POEMS syndrome, with good hematological control, with progression-free survival of 98%, 94% and 75% at 1, 2 and 5 years 31, 32, 33, and good organ-specific response levels, with 100% patients achieving ‘a degree of neurological recovery’ 34. The first autologous stem cell transplantation for POEMS syndrome at University College London was performed in 1999 35 on a 56-year-old man who remains in remission, fully ambulant and with a most recent serum VEGF of 276 pg/mL. The same researchers have subsequently performed 36, and only 3 have required further treatment with systemic chemotherapy 22. Age, comorbidities and physiological fitness should be considered before autologous stem cell transplantation. They quote a 5%–10% risk of the need for intensive care treatment, and 3%–5% risk of death, depending on performance status 33. Engraftment syndrome probably occurs in around 20%–50% of patients 33, although the researchers have not seen this in their cohort of 36 treated patients. Patients can relapse, and in such cases low-dose long-term chemotherapy is an option, or a second autologous stem cell transplantation, but there is no evidence for this.
Patients deemed unfit for autologous stem cell transplantation can be treated with chemotherapeutic agents as pretransplant induction therapy, enabling transplantation at a later date, or long term if stem cell transplantation is not an option. Broadly speaking, chemotherapy used to be based on an alkylating agent (such as melphalan or cyclophosphamide) and dexamethasone 31. Thalidomide and lenalidomide, potent inhibitors of tumour secreting cytokines such as interleukin 6, tumour necrosis factor and VEGF, are emerging as treatments for POEMS syndrome. Doctors are now often using lenalidomide as first line. A systematic review of lenalidomide in POEMS syndrome 36 reported neuropathy improvement in 90% of cases and a progression-free survival estimate at 12 months of 93%. Using lenalidomide and dexamethasone, doctors have seen remarkable and rapid improvement in clinical status, particularly in fluid overload, VEGF and hematological response. The risks of peripheral neuropathy with thalidomide, and of thrombosis with both thalidomide and lenalidomide, require careful monitoring and the need for prophylactic low molecular weight heparin. Bortezomib as a single agent, or combined with cyclophosphamide, has shown promising results in 25 patients, but can also cause or worsen peripheral neuropathy 37.
Monitoring treatment response
Assessing response to treatment and monitoring is complex and requires thorough investigation and clinical assessment to determine response. Broadly, doctors use the following categories to assess response:
- Haematological response: This is defined by the clearance of monoclonal proteins from the blood, and clearance of plasma cells from the bone marrow. This can be misleading, as the monoclonal component in POEMS tends to be very subtle, and patients can improve significantly despite the absence of a monoclonal protein response.
- VEGF: VEGF tends to correlate with disease activity and should normalise (serum concentration <771 pg/mL) over 6 months, but again this may not correlate with the treatment response.
- PET-CT imaging: This can help to show reduction in standardised uptake values (SUVmax) of previously avid lesions; such reductions take many months (often more than 12).
- Organ response: Organ response can be difficult to quantify, but the following markers would indicate improvement:
- reduction in weight secondary to resolution of fluid overload
- shrinkage of enlarged organs or lymph nodes
- shrinkage or disappearance of glomeruloid haemangiomas
- improvement in pulmonary and cardiac function
- improvement in neuropathy severity scores such as Rasch-built Overall Disablilty Score (R-ODS)-CIDP or Medical Research Council muscle sum scores.
Collating all the above provides an overall picture of the patient’s disease status. Any worsening of clinical, radiological or haematological indicators should prompt further investigation with the tests highlighted in Table 5 (see Table 5 above under diagnosis), ultimately with consideration of a bone marrow biopsy where appropriate.
Disability management
Multidisciplinary input is essential when caring for patients with POEMS syndrome. Disability management through the use of orthotics, walking aids and home adaptations should be provided through physiotherapy and occupational therapy services, preferably in a multidisciplinary environment. Neuropathy in POEMS classically takes around 2–3 years post-treatment before significant improvement begins. A retrospective review of 60 patients with POEMS syndrome following autologous stem cell transplantation showed a median improvement in the neuropathy impairment score of 18 points (66–48 points) in 12 months and 30 points at a median follow-up of 60 months 34. Healthcare providers typically refer patients for neurorehabilitation both early in the disease and once neuropathy starts to improve. Patients can receive educational and emotional support through specialist nurses and psychologists.
- Dispenzieri A. POEMS syndrome. Blood Reviews. 2007;21(6):285–299. https://www.ncbi.nlm.nih.gov/pubmed/17850941[↩][↩]
- POEMS. https://www.foundationforpn.org/what-is-peripheral-neuropathy/causes/autoimmune-disease/poems/[↩]
- Bardwick PA, Zvaifler NJ, Gill GN, et al. Plasma cell dyscrasia with polyneuropathy, organomegaly, endocrinopathy, M protein, and skin changes: the POEMS syndrome. Report on two cases and a review of the literature. Medicine 1980;59:311–22. https://www.ncbi.nlm.nih.gov/pubmed/6248720[↩]
- POEMS Syndrome. ASH Education Book January 1, 2005 vol. 2005 no. 1 360-367 doi: 10.1182/asheducation-2005.1.360 http://asheducationbook.hematologylibrary.org/content/2005/1/360.long[↩]
- Dispenzieri A, Kyle RA, Lacy MQ, et al. POEMS syndrome: definitions and long-term outcome. Blood. 2003;101(7):2496–2506. http://www.bloodjournal.org/content/101/7/2496.long[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Nakanishi T, Sobue I, Toyokura Y. The Crow-Fukase syndrome: a study of 102 cases in Japan. Neurology. 1984;34(6):712–720. https://www.ncbi.nlm.nih.gov/pubmed/6539431[↩]
- Bardwick PA, Zvaifler NJ, Gill GN. Plasma cell dyscrasia with polyneuropathy, organomegaly, endocrinopathy, M protein, and skin changes: The POEMS syndrome. Report on two cases and a review of the literature. Medicine. 1980;59(4):311–322. https://www.ncbi.nlm.nih.gov/pubmed/6248720[↩]
- Dispenzieri A. POEMS syndrome. Blood Rev 2007;21:285–99.doi:10.1016/j.blre.2007.07.004 https://www.ncbi.nlm.nih.gov/pubmed/17850941[↩]
- D’Souza A, Hayman SR, Buadi F, et al. The utility of plasma vascular endothelial growth factor levels in the diagnosis and follow-up of patients with POEMS syndrome. Blood 2011;118:4663–5.doi:10.1182/blood-2011-06-362392 http://www.bloodjournal.org/content/118/17/4663[↩]
- Nasu S, Misawa S, Sekiguchi Y, et al. Different neurological and physiological profiles in POEMS syndrome and chronic inflammatory demyelinating polyneuropathy. J Neurol Neurosurg Psychiatry 2012;83:476–9.doi:10.1136/jnnp-2011-301706 http://jnnp.bmj.com/content/83/5/476[↩][↩]
- Rose C, Zandecki M, Copin MC, et al. POEMS syndrome: report on six patients with unusual clinical signs, elevated levels of cytokines, macrophage involvement and chromosomal aberrations of bone marrow plasma cells. Leukemia. 1997;11(8):1318–1323. https://www.ncbi.nlm.nih.gov/pubmed/9264387[↩]
- Soubrier M, Sauron C, Souweine B, et al. Growth factors and proinflammatory cytokines in the renal involvement of POEMS syndrome. American Journal of Kidney Diseases. 1999;34(4):633–638. https://www.ncbi.nlm.nih.gov/pubmed/10516342[↩]
- Tokashiki T, Hashiguchi T, Arimura K, Eiraku N, Maruyama I, Osame M. Predictive value of serial platelet count and VEGF determination for the management of DIC in the Crow-Fukase (POEMS) syndrome. Internal Medicine. 2003;42(12):1240–1243. https://www.jstage.jst.go.jp/article/internalmedicine1992/42/12/42_12_1240/_pdf/-char/en[↩]
- Li J, Zhou DB, Huang Z, et al. Clinical characteristics and long-term outcome of patients with POEMS syndrome in China. Annals of Hematology. 2011;90(7):819–826. https://www.ncbi.nlm.nih.gov/pubmed/21221584[↩]
- S Vincent Rajkumar. POEMS syndrome. UpToDate. Waltham, MA: UpToDate; May 15, 2015[↩]
- Kanai K, Kuwabara S, Misawa S, et al. Failure of treatment with anti-VEGF monoclonal antibody for long-standing POEMS syndrome. Intern Med 2007;46:311–3.doi:10.2169/internalmedicine.46.6246 https://www.jstage.jst.go.jp/article/internalmedicine/46/6/46_6_311/_pdf/-char/en[↩][↩]
- Soubrier MJ, Dubost JJ, Sauvezie BJ. POEMS syndrome: a study of 25 cases and a review of the literature. French Study Group on POEMS syndrome. Am J Med. 1994;97:543-553. http://www.amjmed.com/article/0002-9343(94)90350-6/pdf[↩]
- Nakanishi T, Sobue I, Toyokura Y, et al. The Crow-Fukase syndrome: a study of 102 cases in Japan. Neurology. 1984;34:712-720. http://n.neurology.org/content/neurology/34/6/712.full.pdf[↩][↩]
- Ji ZF, Zhang DY, Weng SQ, Shen XZ, Liu HY, Dong L. POEMS Syndrome: A Report of 14 Cases and Review of the Literature. ISRN Gastroenterology. 2012;2012:584287. doi:10.5402/2012/584287. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3321530/[↩]
- Nakanishi T, Sobue I, Toyokura Y, et al. The Crow-Fukase syndrome: a study of 102 cases in Japan. Neurology. 1984;34:712-720. http://n.neurology.org/content/34/6/712[↩]
- Kelly JJ Jr., Kyle RA, Miles JM, Dyck PJ. Osteosclerotic myeloma and peripheral neuropathy. Neurology. 1983;33:202-210. http://n.neurology.org/content/33/2/202[↩]
- Keddie S, D’Sa S, Foldes D, et al. POEMS neuropathy: optimising diagnosis and management. Practical Neurology Published Online First: 06 March 2018. doi: 10.1136/practneurol-2017-001792 http://pn.bmj.com/content/early/2018/03/14/practneurol-2017-001792[↩][↩][↩][↩][↩]
- Dispenzieri A, Gertz MA. Treatment of POEMS syndrome. Current Treatment Options in Oncology. 2004;5(3):249–257. https://www.ncbi.nlm.nih.gov/pubmed/15115653[↩]
- Dispenzieri A, Gertz MA. Treatment options for POEMS syndrome. Expert Opinion on Pharmacotherapy. 2005;6(6):945–953. https://www.ncbi.nlm.nih.gov/pubmed/15952922[↩]
- Rosser GJ, Reitböck PG, Gray MC, Warwicker P. Successful stabilisation of nephropathy in a patient with POEMS (polyneuropathy, organomegaly, endocrinopathy, M-band, skin changes) syndrome on treatment with mycophenolate and steroids: a case report. Journal of Medical Case Reports. 2010;4, article no. 63 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2848064/[↩]
- Chee CE, Dispenzieri A, Gertz MA. Amyloidosis and POEMS syndrome. Expert Opinion on Pharmacotherapy. 2010;11(9):1501–1514. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2874109/[↩]
- Hogan WJ, Lacy MQ, Wiseman GA, Fealey RD, Dispenzieri A, Gertz MA. Successful treatment of POEMS syndrome with autologous hematopoietic progenitor cell transplantation. Bone Marrow Transplantation. 2001;28(3):305–309. https://www.nature.com/articles/1703108[↩]
- Kawano Y, Nakama T, Hata H, et al. Successful treatment with rituximab and thalidomide of POEMS syndrome associated with Waldenstrom macroglobulinemia. Journal of the Neurological Sciences. 2010;297(1-2):101–104. https://www.ncbi.nlm.nih.gov/pubmed/20673674[↩]
- Ohwada C, Nakaseko C, Sakai S, et al. Successful combination treatment with bevacizumab, thalidomide and autologous PBSC for severe POEMS syndrome. Bone Marrow Transplantation. 2009;43(9):739–740. https://www.nature.com/articles/bmt2008381[↩]
- Sekiguchi Y, Misawa S, Shibuya K, et al. Ambiguous effects of anti-VEGF monoclonal antibody (bevacizumab) for POEMS syndrome. J Neurol Neurosurg Psychiatry 2013;84:1346–8.doi:10.1136/jnnp-2012-304874 http://jnnp.bmj.com/content/84/12/1346[↩]
- Dispenzieri A. POEMS syndrome: 2017 Update on diagnosis, risk stratification, and management. Am J Hematol 2017;92:814–29.doi:10.1002/ajh.24802[↩][↩][↩]
- D’Souza A, et al. Long-term outcomes after autologous stem cell transplantation for patients with POEMS syndrome (osteosclerotic myeloma): a single-center experience. 2012;120:56–62.[↩]
- Cook G, Iacobelli S, van Biezen A, et al. High-dose therapy and autologous stem cell transplantation in patients with POEMS syndrome: a retrospective study of the Plasma Cell Disorder sub-committee of the Chronic Malignancy Working Party of the European Society for Blood & Marrow Transplantation. Haematologica 2017;102:160–7.doi:10.3324/haematol.2016.148460 http://www.haematologica.org/content/102/1/160[↩][↩][↩]
- Karam C, Klein CJ, Dispenzieri A, et al. Polyneuropathy improvement following autologous stem cell transplantation for POEMS syndrome. Neurology 2015;84:1981–7.doi:10.1212/WNL.0000000000001565[↩][↩]
- Peggs KS, Paneesha S, Kottaridis PD, et al. Peripheral blood stem cell transplantation for POEMS syndrome. Bone Marrow Transplant 2002;30:401–4.doi:10.1038/sj.bmt.1703670 https://www.nature.com/articles/1703670[↩]
- Zagouri F, Kastritis E, Gavriatopoulou M, et al. Lenalidomide in patients with POEMS syndrome: a systematic review and pooled analysis. Leuk Lymphoma 2014;55:2018–23.doi:10.3109/10428194.2013.869329 https://www.ncbi.nlm.nih.gov/pubmed/24295131[↩]
- He H, Fu W, Du J, et al. Successful treatment of newly diagnosed POEMS syndrome with reduced-dose bortezomib based regimen. Br J Haematol 2017.doi:10.1111/bjh.14497[↩]





{kind=link}