What is prognathism
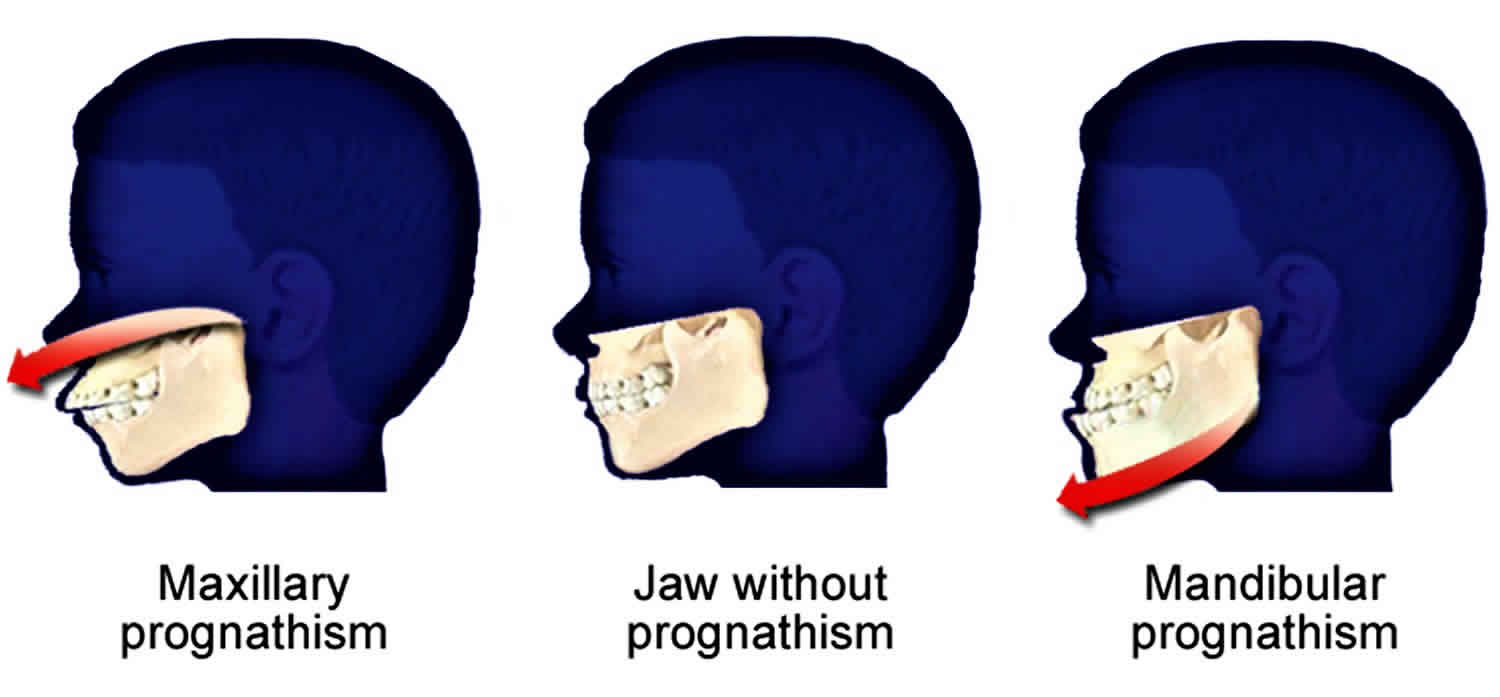
Prognathism is an extension or bulging forward (protrusion) of the lower jaw (mandibular prognathism) or upper jaw (maxillary prognathism). Prognathism occurs when the teeth are not properly aligned due to the shape of the face bones. Prognathism may cause malocclusion (misalignment of the biting surfaces of the upper and lower teeth). Prognathism can give a person an angry, or fighter’s appearance. Prognathism may be a symptom of other syndromes or conditions.
Prognathism may be treated with surgery. An oral surgeon, plastic facial surgeon, or ENT specialist may perform this surgery.
A dentist or orthodontist may be able to treat abnormal alignment of the jaw and teeth. Your primary health care provider should also be involved to check for underlying medical disorders that can be associated with prognathism.
See a dentist or orthodontist if:
- You or your child have difficulty talking, biting, or chewing related to the abnormal jaw alignment.
- You have concerns about jaw alignment.
Prognathism types
Alveolar prognathism
Not all alveolar prognathism is anomalous, and significant differences can be observed among different ethnic groups.[2]
Harmful habits such as thumb sucking or tongue thrusting can result in or exaggerate an alveolar prognathism, causing teeth to misalign. Functional appliances can be used in growing children to help modify bad habits and neuro-muscular function, with the aim of correcting this condition.
Alveolar prognathism can also easily be corrected with fixed orthodontic therapy. However, relapse is quite common, unless the cause is removed or a long-term retention is used.
Figure 1. Alveolar prognathism

Maxillary prognathism
In disease states, maxillary prognathism is associated with Cornelia de Lange syndrome; however, so-called false maxillary prognathism, or more accurately, retrognathism, where there is a lack of growth of the mandible, is by far a more common condition.
Prognathism, if not extremely severe, can be treated in growing patients with orthodontic functional or orthopedic appliances. In adult patients this condition can be corrected by means of a combined surgical/orthodontic treatment, where most of the time a mandibular advancement is performed. The same can be said for mandibular prognathism.
Mandibular prognathism
Mandibular prognathism is a dentofacial deformity characterized by overgrowth of the lower jaw with or without undergrowth of the upper jaw 1. Mandibular prognathism is a dentofacial anomaly characterized by protrusion of the mandible, with lower incisors often overlapping the upper incisors. The protruding lower jaw is caused by a forward positioning of the mandible itself. The discrepancy between the upper and lower jaw can cause a deficiency in speech articulation and low masticatory efficiency 2. Epidemiological data indicate that mandibular prognathism prevalence rates range from 0.48% to 4.3% in Caucasian populations and from 2.1% to 10% in Chinese populations 3. According to OMIM (Online Mendelian Inheritance in Man), mandibular prognathism can occur as non-syndromic condition or as one phenotype of systemic diseases, such as Apert syndrome and Crouzon syndrome 4.
Numerous risk factors have been reported in association with mandibular prognathism. Both genetic and environmental factors contribute to this occlusion disorder 5. To date, 11 common genetic loci have been reported to be associated with mandibular prognathism 6, including 1p22.1, 1q32.2, 3q26.2, 11q22, 12q13.13, 12q23, 1p36, 6q25, 19p13.2, 14q24.3-31.2, and 4p16.1. Moreover, 1p22.3 and 1q32.2 have also been reported to be associated with mandibular prognathism using genome-wide association study 6. Among these studies, Yamaguchi et al. 7 and Li et al. 8 investigated largely on the mandibular prognathic subtype, whereas Frazier-Bowers et al. 9 found that affected individuals were mostly maxillary deficient. There also have a host of genes which might influence mandibular prognathism, such as: GHR 10, EPB41 11, MATN1 12, MYO1H 13. Recently, Nikopensius et al 14 performed whole-exome sequencing on five siblings from an Estonian family affected by class III malocclusion and identified a mutation of DUSP6, c.545C>T (p.Ser182Phe), which is likely a causal variant of class III malocclusion. The family members they studied exhibited maxillary retrusion or mandibular protrusion. Due to the highly variable subphenotypes (mandibular protrusion, maxillary retrusion, or a combination of both) and clinical heterogeneity of mandibular prognathism, genetic mechanism for this malformation remains uncertain 15.
Figure 2. Mandibular prognathism

Prognathism causes
An extended (protruding) jaw can be part of a person’s normal face shape that is present at birth.
Prognathism can also be caused by inherited conditions, such as Crouzon syndrome or basal cell nevus syndrome.
Prognathism may develop over time in children or adults as the result of conditions such as gigantism or acromegaly.
Prognathism diagnosis
Your doctor, dentist or orthodontist will perform a physical exam and ask questions regarding your medical history. Questions may include:
- Is there any family history of an unusual jaw shape?
- Is there difficulty talking, biting, or chewing?
- What other symptoms do you have?
Diagnostic tests may include:
- Skull x-ray (panoramic and cephalometric)
- Dental x-rays
- Imprints of the bite (a plaster mold is made of the teeth)
Prognathism treatment
Orthognathic surgery in conjunction with orthodontic treatment is required for the correction of adult mandibular prognathism 16. The two most commonly applied surgical procedures to correct mandibular prognathism are sagittal split ramus osteotomy and intraoral vertical ramus osteotomy. Both procedures are suitable for patients in whom a desirable occlusal relationship can be obtained with a setback of the mandible, and each has its own advantages and disadvantages. In bilateral sagittal split ramus osteotomy, the intentional ostectomy of the posterior part of the distal segment can offer long-term positioned stability. This may be attributable to reduction of tension in the pterygomasseteric sling that applies force in the posterior mandible.
Rigid fixation has been recognized as a successful method for preventing relapse, although applying the distal ostectomy technique (intentionalostectomy of the posterior part of the distal segment) in addition to bilateral sagittal split ramus osteotomy is even more effective as it offers even better long-term positional stability 17.This may be due to the reductionof tension in the pterygomasseteric sling that appliesforce in the posterior mandible.
References- van Vuuren C. A review of the literature on the prevalence of Class III malocclusion and the mandibular prognathic growth hypotheses. Aust Orthod J 12, 23–28, 1991
- Taher A. Speech defect associated with Class III jaw relationship. Plast Reconstr Surg 99, 1200, 1997
- Chang H. P., Tseng Y. C. & Chang H. F. Treatment of mandibular prognathism. J Formos Med Assoc 105, 781–790, 2006.
- Mandibular prognathism. http://omim.org/entry/176700?search=Prognathism&highlight=prognathism
- Chang H. P., Tseng Y. C. & Chang H. F. Treatment of mandibular prognathism. J Formos Med Assoc 105, 781–790, 2006
- Ikuno K. et al. Microsatellite genome-wide association study for mandibular prognathism. Am J Orthod Dentofacial Orthop 145, 757–762, 2014
- Yamaguchi T., Park S. B., Narita A., Maki K. & Inoue I. Genome-wide linkage analysis of mandibular prognathism in Korean and Japanese patients. J Dent Res 84, 255–259, 2005
- Li Q., Li X., Zhang F. & Chen F. The identification of a novel locus for mandibular prognathism in the Han Chinese population. J Dent Res 90, 53–57, 2011
- Frazier-Bowers S., Rincon-Rodriguez R., Zhou J., Alexander K. & Lange E. Evidence of linkage in a Hispanic cohort with a Class III dentofacial phenotype. J Dent Res 88, 56–60 (2009).
- Sasaki Y. et al. The P561T polymorphism of the growth hormone receptor gene has an inhibitory effect on mandibular growth in young children. Eur J Orthod 31, 536–541, 2009
- Identification of SNP markers on 1p36 and association analysis of EPB41 with mandibular prognathism in a Chinese population. Xue F, Wong R, Rabie AB. Arch Oral Biol. 2010 Nov; 55(11):867-72.
- Jang J. Y. et al. Polymorphisms in the Matrilin-1 gene and risk of mandibular prognathism in Koreans. J Dent Res 89, 1203–1207, 2010
- Tassopoulou-Fishell M., Deeley K., Harvey E. M., Sciote J. & Vieira A. R. Genetic variation in myosin 1H contributes to mandibular prognathism. Am J Orthod Dentofacial Orthop 141, 51–59
- Nikopensius T. et al. A missense mutation in DUSP6 is associated with Class III malocclusion. J Dent Res 92, 893–898, 2013
- Chen F, Li Q, Gu M, Li X, Yu J, Zhang YB. Identification of a Mutation in FGF23 Involved in Mandibular Prognathism. Sci Rep. 2015;5:11250. Published 2015 Jun 10. doi:10.1038/srep11250 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4462018
- Treatment of Mandibular Prognathism. Journal of the Formosan Medical Association Volume 105, Issue 10, 2006, Pages 781-790 https://doi.org/10.1016/S0929-6646(09)60264-3
- Kim MJ, Kim SG, Park YW. Positional stability following intentional posterior ostectomy of the distal segment infbilateral sagittal split ramus osteotomy for correction ofmandibular prognathism. J Craniomaxillofac Surg2002;30:35–40.





{kind=link}