
Solar urticaria
Solar urticaria describes a relatively rare type of urticaria or hives which is triggered by exposing the skin of susceptible individuals to sunlight (UV radiation or visible light) 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12. Solar urticaria is a rare form of chronic inducible urticaria in which the skin swells within minutes of exposure to natural sunlight or an artificial light source emitting ultraviolet radiation 13. The reaction may subside within a few minutes or it may persist for up to an hour or more where it can become very disabling 13, 14.
In the largest series of patients, a history of atopy is noticed in less than 30% of cases. Atopy refers to the genetic predisposition of experiencing an exaggerated immune response to allergens via the overproduction of immunoglobulin E (IgE). The association of solar urticaria with other types of chronic urticaria may be seen in up to 16% of patients 15, 16.
Solar urticaria is rare but is found worldwide. Solar urticaria accounts for less than 0.5% of all urticaria cases and 7% of all photodermatoses 14. Solar urticaria can occur in both males and females at any time of life. The mean age of onset is 35 years, but it has occurred in infants through to elderly persons aged 70 years, it appears to be those aged between 20 and 40 who are most affected. There is a female predominance but no ethnic difference.
Urticaria is also known as hives, weals or nettle rash. Urticaria are welts on the skin that often itch. These welts can appear on any part of the skin. Urticaria vary in size from as small as a pen tip to as large as a dinner plate. They may connect to form even larger welts.
A hive often goes away in 24 hours or less. New hives may appear as old ones fade, so hives may last for a few days or longer. A bout of hives usually lasts less than 6 weeks. These urticaria are called acute urticaria. If hives last more than 6 weeks, they are called chronic urticaria.
As soon as a patient is shielded from sun exposure the rash begins to disappear spontaneously within several minutes to a few hours. The rash clears away completely without leaving a mark.
Patients with solar urticaria must take measures to avoid or minimize sun exposure by following sun protection strategies including sunscreen and sun protective clothing. Oral antihistamines may be helpful in reducing weals and minimizing itch but they rarely prevent the reaction altogether.
For patients that react severely and are unable to manage their condition through preventative measures, phototherapy and/or photochemotherapy may be considered. These treatments desensitize the patient to UV radiation and are often performed prior to the summer months. Desensitization is often short-lived and repeated therapy may be needed.
Can solar urticaria be cured?
Some cases of solar urticaria do spontaneously go away, however for the majority of cases it persists. If it does persist then the treatments described below may provide control by reducing the appearance and symptoms of the solar urticaria.
Solar urticaria causes
Exposure of skin to sunlight causes solar urticaria. The radiation spectrum of action for solar urticaria ranges from ultraviolet B to visible light (wavelength of 300 nanometers to 500 nanometers) and is variable from one patient to another 17. Occasionally, solar urticaria is triggered by an exogenous substance, such as some medications. Some examples include atorvastatin, chlorpromazine, tetracycline, or oral contraceptives 18, 19, 20.
Solar urticaria occurs when sunlight causes the release of histamine from cells in the skin called mast cells. It is an immediate hypersensitivity reaction, which might be immunoglobulin E (IgE)-mediated, occurring after exposure to the sun. Direct evidence for histamine release in solar urticaria comes mostly from blood histamine assessment: 2 patients with confirmed solar urticaria were challenged and histamine was measured by Soter et al. 21. Serum histamine rose from baseline of <0.1 ng/ml to peak levels of 7.0 and 37 ng/ml at 5 minutes. Levels returned to baseline by 20 minutes. Hawk et al. 22 studied histamine release in four solar urticaria patients provoked by UVB. The results showed that two patients had increased histamine levels of 20 ng/ml and 8.5 ng/ml at 2 and 5 minutes after irradiation, respectively while the other two showed smaller increases. Additionally, electron microscopy of skin specimens taken after challenge showed numerous mast cells undergoing exocytotic changes, characteristically seen during histamine release, whereas in some cells no signs of degranulation were found. Keahey et al. 23 measured venous blood histamine levels in three patients before and after UVA irradiation with various intervals up to 30 min compared with after induction of tolerance by repeated exposure to UVA. The results showed small and variable histamine release, which was reduced by tolerance induction. Watanabe et al. 24 reported increase in venous histamine in two solar urticaria patients when wheals developed approximated 30 minutes after UV irradiation. There is only one study, of Kaplan et al. 25, that performed histamine measurements in the skin. Solar urticaria was induced in one patient by ultraviolet (UV) light filtered through window glass for 30 seconds. Histamine levels in suction blisters induced over urticarial lesions and the contralateral non-urticarial skin were 127 ng/ml and 24 ng/ml, respectively.
As for indirect evidence, Baart de Faille et al. 26 reported that histological evaluation revealed higher numbers of mast cells in irradiated specimens, as well as appearance of degranulation 24 hours after irradiation, implying histamine release. Also, antihistamines treatment is of benefit in 35-75% of solar urticaria patients 27, 28, 29.
Exactly how and why certain types of sunlight cause this is currently uncertain but may be due to an antigen-antibody reaction. It seems that a chemical created in the body (a photoallergen) reacts with UV radiation to cause an allergic reaction that manifests as urticaria.
The UV radiation may activate an endogenous substance called a chromophore, which could be present in the serum and/or the dermis, turning it into an immunologically active photoallergen. This later induces the degranulation of mast cells (histamine release), resulting in lesions of urticaria 30, 31 . The intradermal positive reaction after injection of the patient’s irradiated serum is consistent with the hypothesis of a circulating chromophore.
Certain radiation wavelengths (usually long ones) may inhibit the immunological reaction induced by other wavelengths (usually short ones). This is called the double spectrum of action.
The appearance of solar urticaria can be quite dramatic as it usually develops within just a few minutes after exposure to the causative light. The ‘types’ of light responsible for solar urticaria are long wavelength ultraviolet (UVA) and/or short wavelength ultraviolet (UVB), along with visible light (e.g. sunlight not containing ultraviolet).
Solar urticaria prevention
Sun exposure must be avoided or minimized because it is the primary causative agent of solar urticaria. Practical measures include the following 32:
- Wearing protective clothing
- Applying sunscreens with adequate protection against the causative wavelengths
- Using UV protective shields over glass windows
- Altering lifestyle to minimize time spent outside during the day, e.g., changing job hours and shifting to indoor recreational activities
Some patients with UV-A or visible light induced solar urticaria may find it helpful to use self-tanning lotions containing dihydroxyacetone.
If medical therapy is unsuccessful, some patients benefit from complete avoidance or, possibly, a combination of avoidance and medical therapy.
Solar urticaria symptoms
The main symptoms of solar urticaria are itchy rash develops within minutes after a short period (less than 30 minutes) of sun exposure, stinging and burning. The rash may look like weals and be red and swollen. Often the rash affects areas of exposed skin that are normally shielded from sunlight by clothing, e.g. back. The face and upper sides of the hands that are constantly exposed to the sun may be unaffected or only slightly affected. This may be put down to acclimatization or ‘hardening’ of these chronically exposed areas. Rarely the rash is accompanied by symptoms such as headache, nausea, vomiting, breathing difficulties and low blood pressure.
If large areas of the body are affected, the loss of fluid into the skin may result in light-headedness, headache, nausea and vomiting.
Areas covered with thin clothing may also be affected, depending on the ultraviolet rays being emitted and the sheerness of the fabric.
What does solar urticaria look like?
Solar urticaria looks like flat red marks or raised red or white weals on the skin. The weals may come together with sharp cut off lines at clothing. Sites affected depend on areas exposed to sunlight. Solar urticaria may develop on skin apparently covered by clothing especially if the clothing is thin.
The rash may last a few minutes, or hours, and usually disappears within a day. Rarely, it may last longer than 24 hours, even if further exposure to the causative light is avoided. No scarring is left behind.
Figure 1. Solar urticaria

Figure 2. Solar urticaria appears as red itchy wheals
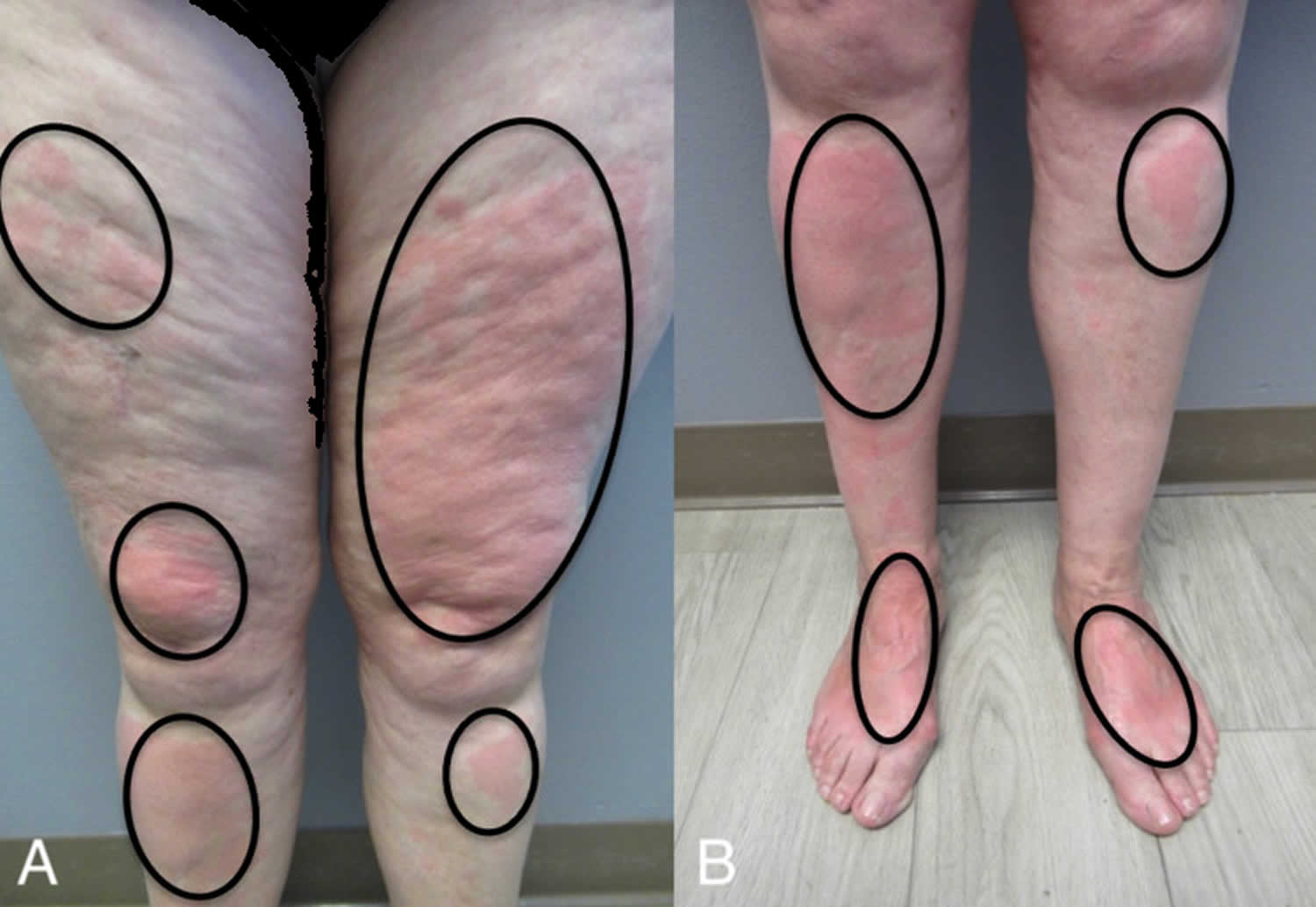
Footnote: Closer views of the anterior thighs (A), pretibial legs (A and B), distal legs (B), and dorsal feet (B) showed erythematous areas of urticaria (black ovals).
[Source 5 ]How is solar urticaria diagnosed?
The diagnosis is usually based on its appearance and/or a history of the rash appearing minutes after sunlight exposure which then settles down within a few hours. Photographs of the rash may help with making the diagnosis.
Defining features of solar urticaria include:
- Rash appearing within a few minutes of exposure. In rare cases, some solar urticaria patients may show a delayed reaction to sunlight.
- Upon cessation of sun exposure the rash quickly disappears (within minutes to a few hours, rarely lasting more than 24 hours).
Phototesting (trying to reproduce the rash by testing the skin with different wavelengths of ultraviolet and visible light, also known as monochromator light testing) is used to confirm the diagnosis. Phototesting requires referral to a specialized center. Other tests such as blood tests and a skin biopsy may be needed in some cases.
The histopathology of solar urticaria almost mirrors other urticarias; the dermis shows mild edema with mixed infiltrate of neutrophils and eosinophils around the vasculature.
Figure 3. Solar urticaria phototesting

Footnote: Solar urticaria phototesting of 27 year old male. (A) Visible light exposure (380–700 nm) directed to the lower back with (B) development of raised, erythematous wheals 15 min post exposure. (C) UVB (290–320 nm) challenge testing and (D) positive urticarial reaction at 75, 150 and 200 mJoules of UVB (but not at 25 mJ)
[Source 4 ]Solar urticaria treatment
Treating solar urticaria can be difficult, especially if it is visible light causing the problem. Taking measures to avoid sunlight exposure is important to prevent its occurrence and may require major adjustments to a person’s lifestyle. If medication is needed to help control, this can be taken episodically to prevent/treat flares or regularly, depending on severity. Such steps to help prevent eruptions include the following:
- Behavioral modifications. Spend time in the shade between 10am and 3pm when it’s sunny.
- Clothing. Simple measures include the wearing of clothes made from tightly woven cloth, long sleeves, a hat (ideally brimmed); shoes rather than sandals, and gloves, particularly for driving.
- Sunscreens. Solar urticaria is characterised by sensitivity mainly to visible light and ultraviolet A, and more rarely ultraviolet B. Individuals may be sensitive to just one of these wavebands, or all. Phototesting can help to determine which wavelengths are important to avoid in individual patients. Conventional sunscreens are formulated to protect against ultraviolet B and A light (particularly UVB) and may therefore not be effective in those with solar urticaria being triggered by visible light. Reflectant sunscreens that are based on titanium dioxide or zinc oxide will be more effective as they cover UVA, UVB, and visible light. In the US, the SPF (sun protection factor) number tells you how effective the sunscreen is for UVB, and the star rating (usually found on the back of the bottle, with a maximum 4 stars) gives a measure of the UVA protection. Your doctor will advise on which sunscreens you should use.
- A tinted reflectant sunscreen ‘Dundee Reflectant Sunscreen’, which is available in 3 colors, is available on prescription from Tayside Pharmaceuticals and is effective at blocking visible light. These can be mixed to obtain a good color match with your skin.
- Using photoprotective window films. Some people may need to apply special photoprotective window films to the windows of their car and home in order to block out UVA and UVB light. These protective films may stop working and need replacing after about five years. Some car manufacturers offer UV protective glass as standard or as an optional extra, however most car windows do not block UV light. Your dermatologist may be able to advise you about suppliers of UV protective film. The British Photodermatology Group has released a consensus statement on UV protective films.
- Antihistamines. Once solar urticaria develops it can be treated with antihistamine tablets which block the effects of histamine release. Antihistamines can reduce the symptoms and appearance of the weals of urticaria and can be an extremely effective treatment for some patients. The success of antihistamine therapy depends on disease severity. For example, antihistamine monotherapy would probably not benefit someone who develops hives after just a few seconds of sun exposure, but it would help a patient who requires at least 10 minutes’ sun exposure before hives appear. Antihistamines seem to block wheal response and minimize itch, but they do not entirely eliminate the redness reaction. This should be explained to the patient.
- Montelukast. If antihistamines are ineffective then montelukast, usually used to treat asthma, can be added.
- Steroids. Steroid tablets may occasionally be used to relieve severe flares.
- Phototherapy. If you are still having problems, then phototherapy (where carefully measured artificial doses of UVA/UVB are delivered to your skin in a special cabin by specially trained nurses) may be an additional treatment option. This induce tolerance (hardening) process should be based on the spectrum of action and the minimal urticarial dose. PUVA or photochemotherapy is a combination treatment which consists of Psoralens (P) and then exposing the skin to UVA (long wave ultraviolet radiation) seems to give a longer-lived response than phototherapy alone. Phototherapy with UV-A, broadband UV-B, or narrowband UV-B or photochemotherapy with oral methoxsalen (8-MOP, a form of psoralen) plus UV-A is also effective for treating solar urticaria 33, 34.
- Other treatments. These are tried if other treatments do not work and include ciclosporin, anti-IgE antibody (omalizumab), afamelanotide, plasma exchange, photophoresis and intravenous immunoglobulin.
Omalizumab, an anti-IgE antibody approved for use for chronic spontaneous urticaria, has been reported to be effective in the treatment of solar urticaria 35, 36, 37, 38. The 2017 European Academy of Allergology and Clinical Immunology, the Global Allergy and Asthma European Network, the European Dermatology Forum and and the World Allergy Organization guidelines recommend the use of omalizumab as third–line of treatment for the management of chronic spontaneous urticaria in adults and adolescents aged ≥12 years with inadequate response to H1-antihistamines 39. Omalizumab use in patients younger than 12 years is still off-label for chronic spontaneous urticaria despite emerging data suggesting safety and efficacy in this population 40. Use of omalizumab for solar urticaria is currently off-label 41, 42. A small, single-arm, French study administered 300-mg subcutaneous doses of omalizumab every 4 weeks for 3 total visits; despite some improvement, results were lackluster 43. A recent systematic review, covering a total of 48 patients with antihistamine refractory solar urticaria, reported that treatment with omalizumab resulted in clinical improvement for 80% of patients, and 50% of them became symptom free 44. About 20% of patients failed to achieve any clinical response under a monthly dosage of 150–300 mg of omalizumab. Mild adverse events (i.e. gastrointestinal intolerance, periorbital edema, local reaction, and short-term asthenia) were recorded in only 11% of subjects 44. However, most studies have short follow-up periods which are limited to a few months. A recent a case report by Kieselova et al 2 related that a 60-year-old male patient was cured of solar urticaria after administration of omalizumab 300 mg subcutaneous once per month for 6 months.
Plasma exchange therapy has been effective in a few cases, especially in patients with a circulating factor in their serum demonstrated by a positive intradermal test finding 45. However, therapy has been reported to be ineffective in some centers. Until definitive studies are conducted to evaluate the efficacy of this therapy, it should be reserved as a last resort.
A case report described 2 cases of idiopathic solar urticaria treated with intravenous (IV) immunoglobulin, with durable remissions of 13 months and 4 years. Treatment was with 2 g/kg over several 5-day courses approximately 1 month apart 46. Another case report also described successful treatment of solar urticaria with IV immunoglobulin and suggested that it be discussed as a therapeutic option if high-dose antihistamines provide unsatisfactory results 47, 48.
Vitamin D advice
The evidence relating to the health effects of serum Vitamin D levels, sunlight exposure and Vitamin D intake remains inconclusive. Avoiding all sunlight exposure if you suffer from light sensitivity, or to reduce the risk of melanoma and other skin cancers, may be associated with Vitamin D deficiency.
Individuals avoiding all sun exposure should consider having their serum Vitamin D measured. If levels are reduced or deficient they may wish to consider taking supplementary vitamin D3, 10-25 micrograms per day, and increasing their intake of foods high in Vitamin D such as oily fish, eggs, meat, fortified margarines and cereals. Vitamin D3 supplements are widely available from health food shops.
Solar urticaria prognosis
Solar urticaria remains a puzzling disorder that is not well understood 14. While the diagnosis is simple, its management is difficult. Solar urticaria usually develops in the third decade of life and becomes a chronic disease 14. The symptoms are managed with a range of treatments, but remission relies on a phenomenon known as “hardening” and is not achieved by all patients 14. This is the process where continued exposure to ultraviolet radiation decreases the likelihood of attacks. The probability of spontaneous resolution has been estimated as being 15% at 5 years and 25% at 10 years after the onset of the condition 49.
Overall, the prognosis for patients with severe urticaria is poor. Many patients are restricted indoors and lead a poor quality of life.
References- Kulthanan K, Church MK, Grekowitz EM, Hawro T, Kiefer LA, Munprom K, Nanchaipruek Y, Rujitharanawong C, Terhorst-Molawi D, Maurer M. Evidence for histamine release in chronic inducible urticaria – A systematic review. Front Immunol. 2022 Jul 28;13:901851. doi: 10.3389/fimmu.2022.901851
- Kieselova K, Santiago F, Henrique M. Incapacitating solar urticaria: successful treatment with omalizumab. An Bras Dermatol. 2019 Jul 29;94(3):331-333. doi: 10.1590/abd1806-4841.20198109
- Choudhary S, Srivastava A. Wood’s Lamp as an Inexpensive, Handy Tool to Diagnose Solar Urticaria. Indian Dermatol Online J. 2020 Sep 19;11(5):833-834. doi: 10.4103/idoj.IDOJ_625_19
- Komarow HD, Eisch AR, Young M, Nelson C, Metcalfe DD. Solar Urticaria. J Allergy Clin Immunol Pract. 2015 Sep-Oct;3(5):789-90. doi: 10.1016/j.jaip.2015.04.006
- Diehl KL, Erickson C, Calame A, Cohen PR. A Woman With Solar Urticaria and Heat Urticaria: A Unique Presentation of an Individual With Multiple Physical Urticarias. Cureus. 2021 Aug 6;13(8):e16950. doi: 10.7759/cureus.16950
- Hochstadter EF, Ben-Shoshan M. Solar urticaria in a 1-year-old infant: diagnosis and management. BMJ Case Rep. 2014 Apr 17;2014:bcr2013202333. doi: 10.1136/bcr-2013-202333
- De Martinis M, Sirufo MM, Ginaldi L. Solar Urticaria, a Disease with Many Dark Sides: Is Omalizumab the Right Therapeutic Response? Reflections from a Clinical Case Report. Open Med (Wars). 2019 Jun 7;14:403-406. doi: 10.1515/med-2019-0042
- Iannelli M, Passanisi S, Crisafulli G, Arasi S, Caminiti L, Zirilli G, Pajno GB. Long term treatment with omalizumab in adolescent with refractory solar urticaria. Ital J Pediatr. 2021 Sep 28;47(1):195. doi: 10.1186/s13052-021-01151-z
- Milanesi N, Gola M, Francalanci S. Evaluation of nine patients with solar urticaria during summer. G Ital Dermatol Venereol. 2020 Dec;155(6):800-802. doi: 10.23736/S0392-0488.19.06176-5
- I. Snast and others, Real‐life experience in the treatment of solar urticaria: retrospective cohort study, Clinical and Experimental Dermatology, Volume 44, Issue 5, 1 July 2019, Pages e164–e170, https://doi.org/10.1111/ced.13960
- Photiou, L., Foley, P. and Ross, G. (2019), Solar urticaria – An Australian case series of 83 patients. Australas J Dermatol, 60: 110-117. https://doi.org/10.1111/ajd.12975
- Lyons, A.B., Peacock, A., Zubair, R., Hamzavi, I.H. and Lim, H.W. (2019), Successful treatment of solar urticaria with UVA1 hardening in three patients. Photodermatol Photoimmunol Photomed, 35: 193-195. https://doi.org/10.1111/phpp.12447
- Solar urticaria. https://dermnetnz.org/topics/solar-urticaria
- Harris BW, Crane JS, Schlessinger J. Solar Urticaria. [Updated 2023 May 2]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK441986
- Fityan A, McGibbon D, Fassihi H, Sarkany RS. Paediatric solar urticaria: a case series. Br J Dermatol. 2018 Jun;178(6):1453-1454. doi: 10.1111/bjd.16325
- Raigosa M, Toro Y, Sánchez J. Urticaria solar. Reporte de un caso y revisión de la literatura [Solar urticaria. Case report and literature review]. Rev Alerg Mex. 2017 Jul-Sep;64(3):371-375. Spanish. doi: 10.29262/ram.v64i3.202
- Snyder M, Turrentine JE, Cruz PD Jr. Photocontact Dermatitis and Its Clinical Mimics: an Overview for the Allergist. Clin Rev Allergy Immunol. 2019 Feb;56(1):32-40. doi: 10.1007/s12016-018-8696-x
- Griffin LL, Haylett AK, Rhodes LE. Evaluating patient responses to omalizumab in solar urticaria. Photodermatol Photoimmunol Photomed. 2019 Jan;35(1):57-65. doi: 10.1111/phpp.12434
- Chicharro P, Rodríguez-Jiménez P, Capusan TM, Herrero-Moyano M, de Argila D. Induction of Light Tolerance Using Narrowband UV-B in Solar Urticaria. Actas Dermosifiliogr (Engl Ed). 2018 Dec;109(10):888-892. English, Spanish. doi: 10.1016/j.ad.2018.06.005
- Farr PM. Erythropoietic protoporphyria and solar urticaria. Br J Dermatol. 2018 Aug;179(2):542. doi: 10.1111/bjd.16684
- Soter NA, Wasserman SI, Pathak MA, Parrish JA, Austen KF. Solar urticaria: Release of mast cell mediators into the circulation after experimental challenge. J Invest Dermatol (1979) 72(5):282.
- Hawk JL, Eady RA, Challoner AV, Kobza-Black A, Keahey TM, Greaves MW. Elevated blood histamine levels and mast cell degranulation in solar urticaria. Br J Clin Pharmacol (1980) 9(2):183–6. doi: 10.1111/j.1365-2125.1980.tb05831.x
- Keahey TM, Lavker RM, Kaidbey KH, Atkins PC, Zweiman B. Studies on the mechanism of clinical tolerance in solar urticaria. Br J Dermatol (1984) 110(3):327–38. doi: 10.1111/j.1365-2133.1984.tb04639.x
- Watanabe M, Matsunaga Y, Katayama I. Solar urticaria: A consideration of the mechanism of inhibition spectra. Dermatology (1999) 198(3):252–5. doi:10.1159/000018124
- Kaplan AP, Horáková Z, Katz SI. Assessment of tissue fluid histamine levels in patients with urticaria. J Allergy Clin Immunol (1978) 61(6):350–4. doi: 10.1016/0091-6749(78)90113-6
- Baart de la Faille H, Rottier PB, Baart de la Faille-Kuyper EH. Solar urticaria. a case with possible increase of skin mast cells. Br J Dermatol (1975) 92(1):101–7. doi: 10.1159/000144432
- Haylett AK, Koumaki D, Rhodes LE. Solar urticaria in 145 patients: Assessment of action spectra and impact on quality of life in adults and children. Photodermatol Photoimmunol Photomed (2018) 34(4):262–8. doi: 10.1111/phpp.12385
- Beattie PE, Dawe RS, Ibbotson SH, Ferguson J. Characteristics and prognosis of idiopathic solar urticaria: A cohort of 87 cases. Arch Dermatol (2003) 139(9):1149–54 doi: 10.1001/archderm.139.9.1149
- Du-Thanh A, Debu A, Lalheve P, Guillot B, Dereure O, Peyron JL. Solar urticaria: A time-extended retrospective series of 61 patients and review of literature. Eur J Dermatol (2013) 23(2):202–7. doi: 10.1684/ejd.2013.1933
- Botto NC, Warshaw EM. Solar urticaria. J Am Acad Dermatol. 2008 Dec;59(6):909-20; quiz 921-2. doi: 10.1016/j.jaad.2008.08.020
- Goetze S, Elsner P. Solar urticaria. J Dtsch Dermatol Ges. 2015 Dec;13(12):1250-3. doi: 10.1111/ddg.12809
- Solar Urticaria Treatment & Management. https://emedicine.medscape.com/article/1050485-treatment#d8
- Dawe RS, Ferguson J. Prolonged benefit following ultraviolet A phototherapy for solar urticaria. Br J Dermatol. 1997 Jul;137(1):144-8.
- Solar Urticaria Treatment & Management. https://emedicine.medscape.com/article/1050485-treatment
- Saini SS, MacGlashan DW Jr, Sterbinsky SA, Togias A, Adelman DC, Lichtenstein LM, Bochner BS. Down-regulation of human basophil IgE and FC epsilon RI alpha surface densities and mediator release by anti-IgE-infusions is reversible in vitro and in vivo. J Immunol. 1999 May 1;162(9):5624-30.
- Combalia A, Fernández-Sartorio C, Aguilera P. Refractory solar urticaria successfully treated with omalizumab with normalization of phototest. Actas Dermosifiliogr. 2017 Jul-Aug;108(6):593-594. English, Spanish. doi: 10.1016/j.ad.2016.11.015
- Levi A, Tal Y, Dranitzki Z, Shalit M, Enk CD. Successful omalizumab treatment of severe solar urticaria in a 6-year-old child. Pediatr Allergy Immunol. 2015 Sep;26(6):588-90. doi: 10.1111/pai.12441
- Moncourier M, Assikar S, Matei I, Souyri N, Couture M, Rigot E, Delauménie S, Bédane C. Visible light-induced solar urticaria is improved by omalizumab. Photodermatol Photoimmunol Photomed. 2016 Sep;32(5-6):314-316. doi: 10.1111/phpp.12271
- Zuberbier, T, Aberer, W, Asero, R, et al. Endorsed by the following societies: AAAAI, AAD, AAIITO, ACAAI, AEDV, APAAACI, ASBAI, ASCIA, BAD, BSACI, CDA, CMICA, CSACI, DDG, DDS, DGAKI, DSA, DST, EAACI, EIAS, EDF, EMBRN, ESCD, GA²LEN, IAACI, IADVL, JDA, NVvA, MSAI, ÖGDV, PSA, RAACI, SBD, SFD, SGAI, SGDV, SIAAIC, SIDeMaST, SPDV, TSD, UNBB, UNEV and WAO. The EAACI/GA²LEN/EDF/WAO guideline for the definition, classification, diagnosis and management of urticaria. Allergy. 2018; 73: 1393- 1414. https://doi.org/10.1111/all.13397
- Chang J, Cattelan L, Ben-Shoshan M, Le M, Netchiporouk E. Management of Pediatric Chronic Spontaneous Urticaria: a review of current evidence and guidelines. J Asthma Allergy. 2021;14:187–199. doi: 10.2147/JAA.S249765
- Waibel KH, Reese DA, Hamilton RG, Devillez RL. Partial improvement of solar urticaria after omalizumab. J Allergy Clin Immunol. 2010;125(2):490–491. doi: 10.1016/j.jaci.2009.11.007
- Moncourier M, Assikar S, Matei I, Souyri N, Couture M, Rigot E, Delauménie S, Bédane C. Visible light-induced solar urticaria is improved by omalizumab. Photodermatol Photoimmunol Photomed. 2016;32(5-6):314–316. doi: 10.1111/phpp.12271
- Aubin F, Avenel-Audran M, Jeanmougin M, Adamski H, Peyron JL, Marguery MC, Léonard F, Puyraveau M, Viguier M; Société Française de Photodermatologie. Omalizumab in patients with severe and refractory solar urticaria: A phase II multicentric study. J Am Acad Dermatol. 2016 Mar;74(3):574-5. doi: 10.1016/j.jaad.2015.11.021
- Snast I, Kremer N, Lapidoth M, Enk CD, Tal Y, Rosman Y, Confino-Cohen R, Hodak E, Levi A. Omalizumab for the treatment of solar urticaria: case series and systematic review of the literature. J Allergy Clin Immunol Pract. 2018;4(4):1198–1204. doi: 10.1016/j.jaip.2018.02.032
- Collins P, Ahamat R, Green C, Ferguson J. Plasma exchange therapy for solar urticaria. Br J Dermatol. 1996 Jun;134(6):1093-7.
- Hughes R, Cusack C, Murphy GM, Kirby B. Solar urticaria successfully treated with intravenous immunoglobulin. Clin Exp Dermatol. 2009 Dec;34(8):e660-2. doi: 10.1111/j.1365-2230.2009.03374.x
- Maksimovic L, Frémont G, Jeanmougin M, Dubertret L, Viguier M. Solar urticaria successfully treated with intravenous immunoglobulins. Dermatology. 2009;218(3):252-4. doi: 10.1159/000193998
- Adamski H, Bedane C, Bonnevalle A, Thomas P, Peyron JL, Rouchouse B, Cambazard F, Jeanmougin M, Viguier M. Solar urticaria treated with intravenous immunoglobulins. J Am Acad Dermatol. 2011 Aug;65(2):336-340. doi: 10.1016/j.jaad.2010.05.040
- Beattie PE, Dawe RS, Ibbotson SH, Ferguson J. Characteristics and prognosis of idiopathic solar urticaria: a cohort of 87 cases. Arch Dermatol. 2003 Sep;139(9):1149-54. doi: 10.1001/archderm.139.9.1149





{kind=link}