
What is tendonitis
Tendons are connective tissues that attach muscles to bones and and transfer muscular tension to bones. Tendinitis is the severe swelling of a tendon 1 and/or a form of bursitis in which a tendon sheath is inflamed 2.
Tendinitis or bursitis often involves the shoulder, elbow, wrist, hip, knee and ankle. The pain it causes may be quite severe and often occurs suddenly. As in arthritis, the pain is worse during movement. Unlike arthritis, the pain is often in parts of the body far from a joint. Tendinitis often results from repetitive use (overuse). Though the problem can recur or be chronic (long term) in some people, it is most often short term, mainly if treated early.
- Tendinitis or bursitis can be painful. Seek medical attention early to prevent joint stiffness and chronic problems that may follow.
- It also is important to rest the limb or the joint, at least until movement is free of pain.
- Failure to rest it most often delays full healing.
Tendinitis usually happens after repeated injury to an area such as the wrist or ankle. It causes pain and soreness around a joint. Some common forms of tendinitis are named after the sports that increase their risk. They include tennis elbow, golfer’s elbow, pitcher’s shoulder, swimmer’s shoulder, and jumper’s knee.
Bursitis is a painful condition that affects the small, fluid-filled sacs — called bursae (singular, bursa) — that cushion the bones, tendons and muscles near your joints. If a muscle or tendon is pulling around a corner of a bone, or over a bone, a healthy bursa protects it from fraying and stress. Bursitis occurs when bursae become inflamed. When a bursa is inflamed, it becomes very painful, even during rest.
The most common locations for bursitis are in the shoulder, elbow and hip. But you can also have bursitis by your knee, heel and the base of your big toe. Bursitis often occurs near joints that perform frequent repetitive motion.
Doctors diagnose tendinitis with your medical history, a physical exam, and imaging tests. The first step in treatment is to reduce pain and swelling. Rest, wrapping or elevating the affected area, and medicines can help. Ice is helpful for recent, severe injuries. Other treatments include ultrasound, physical therapy, steroid injections, and surgery.
Tips for living with tendinitis or bursitis include:
- Rest the painful tendon. Avoid heavy activity or any activity that causes pain.
- Ice the area for 10 – 15 minutes once or twice a day.
- Seek medical help at once if pain worsens, if redness and swelling appear or if the problem does not improve in 3 – 6 weeks.
- Avoid overuse of any part of the body, such as doing the same motion over and over.
- Warm up by exercising at a relaxed pace before doing more strenuous activity.
When to see a doctor:
Consult your doctor if you have:
- Disabling joint pain
- Sudden inability to move a joint
- Excessive swelling, redness, bruising or a rash in the affected area
- Sharp or shooting pain, especially when you exercise or exert yourself
- A fever
What causes tendinitis and bursitis ?
Tendinitis can occur from a sudden intense injury. Most often, though, it results from a repeated, minor injury of that tendon. Doctors call this repetitive stress or overuse. For example:
- Painting a ceiling for four hours or more, typing long hours, improper body position while using a keyboard, chopping, cutting or sawing may result in tendinitis or bursitis hours or days later.
- Tight clenching while using hand tools or while driving a long time.
- Using a backhand, mainly single handed, in an early-season game of tennis (“tennis elbow”).
- Wearing improper running shoes or not getting the proper training before sports.
Persons with gout, pseudogout, or blood or kidney diseases often develop bursitis as part of that disease. Older persons are more prone to get tendinitis and bursitis. Rarely, some drugs can cause tendinitis and tendon rupture (spontaneous tear). These include fluoroquinolone antibiotics and statins drugs that lower cholesterol).
The most common causes of bursitis are repetitive motions or positions that put pressure on the bursae around a joint.
Examples include:
- Throwing a baseball or lifting something over your head repeatedly
- Leaning on your elbows for long periods
- Extensive kneeling for tasks such as laying carpet or scrubbing floors
Other causes include injury or trauma to the affected area, inflammatory arthritis such as rheumatoid arthritis, gout and infection.
Risk factors for bursitis
Anyone can develop bursitis, but certain factors can increase your risk:
- Age. Bursitis becomes more common with aging.
- Occupations or hobbies. If your work or hobby requires repetitive motion or pressure on particular bursae, your risk of developing bursitis increases. Examples include carpet laying, tile setting, gardening, painting and playing a musical instrument.
- Other medical conditions. Certain systemic diseases and conditions — such as rheumatoid arthritis, gout and diabetes — increase your risk of developing bursitis. Being overweight can increase your risk of developing hip and knee bursitis.
How are tendinitis and bursitis diagnosed ?
To determine the cause of these problems, a health care provider asks about your medical history and does a careful physical exam. Tenderness along the tendon or its sheath (bursa), or at one specific point in the tendon, suggests tendinitis/bursitis. Pain occurs when the muscle to which the tendon is attached is worked against resistance as part of the exam.
Most patients at first do not need imaging tests like X-rays, magnetic resonance imaging (often referred to as MRI) or ultrasound scans. Imaging and blood tests are done only if the problem recurs or does not go away. A blood test also can help detect an infection. Signs of an infection include redness, warmth and swelling. If bursitis is the result of infection, fluid must be drained from the bursa at once and promptly studied.
How are tendinitis and bursitis treated ?
Treatment depends on the cause. In overuse or injury, you must reduce the causing force or stress. If tendinitis is job related, the doctor or physical therapist should review proper ergonomics, so you can work safely. Some patients may need joint protection advice and support of the involved region. There is little proof that therapeutic ultrasound helps these problems, and most doctors do not recommend it.
Bursitis generally gets better on its own. Conservative measures, such as rest, ice and taking a pain reliever, can relieve discomfort. If conservative measures don’t work, you might require other treatments.
Treatment can consist of any of the following:
- Rest. You should rest the injured limb or joint, at least for a short time. Failure to rest it will most likely continue your symptoms. If the problem is in a hip, leg or foot, you may need to stop stressful weightbearing activities for a short time. This lets the inflammation lessen.
- Ice. Ice may help reduce inflammation and pain. Ice the area for 10–15 minutes once or twice a day. When you’re first injured, ice is a better choice than heat — especially for about the first three days or so. Ice numbs pain and causes blood vessels to constrict, which helps reduce swelling. Stick to icing the area for just 15 to 20 minutes every four to six hours — and make sure that you put a towel or cloth in between the ice pack and your skin.
- After the first three days, heat may provide better benefit for chronic tendinitis pain. Heat can increase blood flow to an injury, which may help promote healing. Heat also relaxes muscles, which promotes pain relief.
- Medicine. If your pain persists, you may need nonsteroidal anti-inflammatory drugs—often referred to as NSAIDs – such as aspirin, ibuprofen or naproxen. Topical (applied to the skin) forms of NSAIDs are now available and may reduce pain and inflammation without stomach upset. Acetaminophen (Tylenol) also can help relieve pain.
- Injections. A corticosteroid drug injected into the bursa can relieve pain and inflammation in your shoulder or hip. This treatment generally works quickly and, in many cases, one injection is all you need. The most common side effects of joint and soft tissue injections are irritation and swelling of the tissues 3. This is known as a post-injection “flare” and may last up to 48 hours. Other possible side effects include infection, tendon rupture and muscle damage. In order to reduce your risk of infection, follow your doctor’s instructions carefully and keep the injection site clean.
Corticosteroid injections may provide short-term benefit in certain forms of tendinitis, and may be considered if you are unable to take NSAIDs. If an infection is present, you most often will need a proper antibiotic. (Daily drainage of fluid with a needle also may be needed.) If crystals of gout are found in joint fluid, there is medicine that controls the disease.
- Supports. Use of a cane in the opposite hand can help a painful hip. Splints or braces for the affected body part help rest and reduce stress on the body. Off-the-shelf supports may be enough. If not, you may need custom-made braces and referral to an occupational therapist.
For ankle tendinitis, you may need orthotics to reduce the stress at the ankle or in the foot. An orthotic is a device that goes inside the shoe, which changes the support and the angle of the foot. This improves foot mechanics and relieves pain or pressure. They can be custom made or off the shelf.
- Physical therapy. Some tendon problems do not go away despite standard treatment. If tendinitis lasts beyond a few weeks, you may need a referral to a physical therapist or a rheumatologist. The doctor or therapist can give you exercises to do that will maintain strength and function. If the tendinitis or bursitis has begun to limit joint movement, or already restricts movement, seeing a physical therapist is wise. For instance, if pain in a shoulder has gone away, but you can no longer raise your arm as high as your healthy arm, a “frozen shoulder” or other rotator cuff problems are developing. You can prevent this problem with early treatment.
- Surgery. If, after a few months of treatment, tendinitis still limits an essential activity, you may want to consider surgery. Ask your doctor to refer you to an experienced orthopaedic surgeon. Some patients with an infection or adhesions of the tendon or bursa may need a cortisone injection or an operation. Sometimes an inflamed bursa must be surgically drained, but only rarely is surgical removal of the affected bursa necessary.
A possibly serious complication of tendinitis is rupture of a tendon. The most common rupture is a tear of the Achilles tendon in the lower calf. It most often needs surgery.
Preventing Tendinitis and Bursitis
There are ways you can prevent these problems from occurring. These tips apply to all joints:
- Before strenuous exercise, warm up and stretch.
- Using kneeling pads. Use some type of padding to reduce the pressure on your knees if your job or hobby requires a lot of kneeling.
- Properly train for a new activity. Slowly increase the intensity of your workout.
- Lifting properly. Bend your knees when you lift. Failing to do so puts extra stress on the bursae in your hips.
- Engage in exercise and sports daily or near daily rather than just on weekends.
- Wheeling heavy loads. Carrying heavy loads puts stress on the bursae in your shoulders. Use a dolly or a wheeled cart instead.
- Learn and maintain proper posture and body mechanics.
- Taking frequent breaks. Alternate repetitive tasks with rest or other activities.
- Make sure sports equipment is the right size and fit for you, and designed for the sport you are doing.
- Maintaining a healthy weight. Being overweight places more stress on your joints.
- Avoid staying in one position for too long. Take rest breaks or change positions every 20–40 minutes.
- Stop any activity that causes pain.
- Avoid compulsive behavior, like “I’m going to finish this job even if it kills me!”
How to protect certain joints
Shoulder Joint Protection
- Face an object you are reaching for, rather than reaching sideways or backward.
- Rise from a chair by pushing off with your thigh muscles, not your shoulders or hands.
- Do pushups from the wall, not the floor.
- When reaching for a heavy object overhead, keep the load centered in front of you and use both hands.
Elbow and Wrist Joint Protection
- Recognize and avoid hand clenching or gripping tools or other objects too hard. Use power tools. In the kitchen, use aids such as jar openers. Pad your car steering wheel.
- Use your stomach muscles to help roll over when getting out of bed.
- Avoid carrying heavy items in one hand or at the side of your body.
Knee and Ankle Joint Protection
- Avoid sitting with a leg folded under.
- Wear shoes that give support and comfort, with room for the toes to extend fully during weightbearing.
- Check shoes often for signs of wear, and replace them when worn.
- If you walk or stand on concrete, cushion the inside bottom of your shoes with pads or wear walking or running shoes with cushioned soles.
- Keep leg muscles strong. Do leg lifts with ankle weights (5–20 pounds) while seated.
Shoulder tendonitis
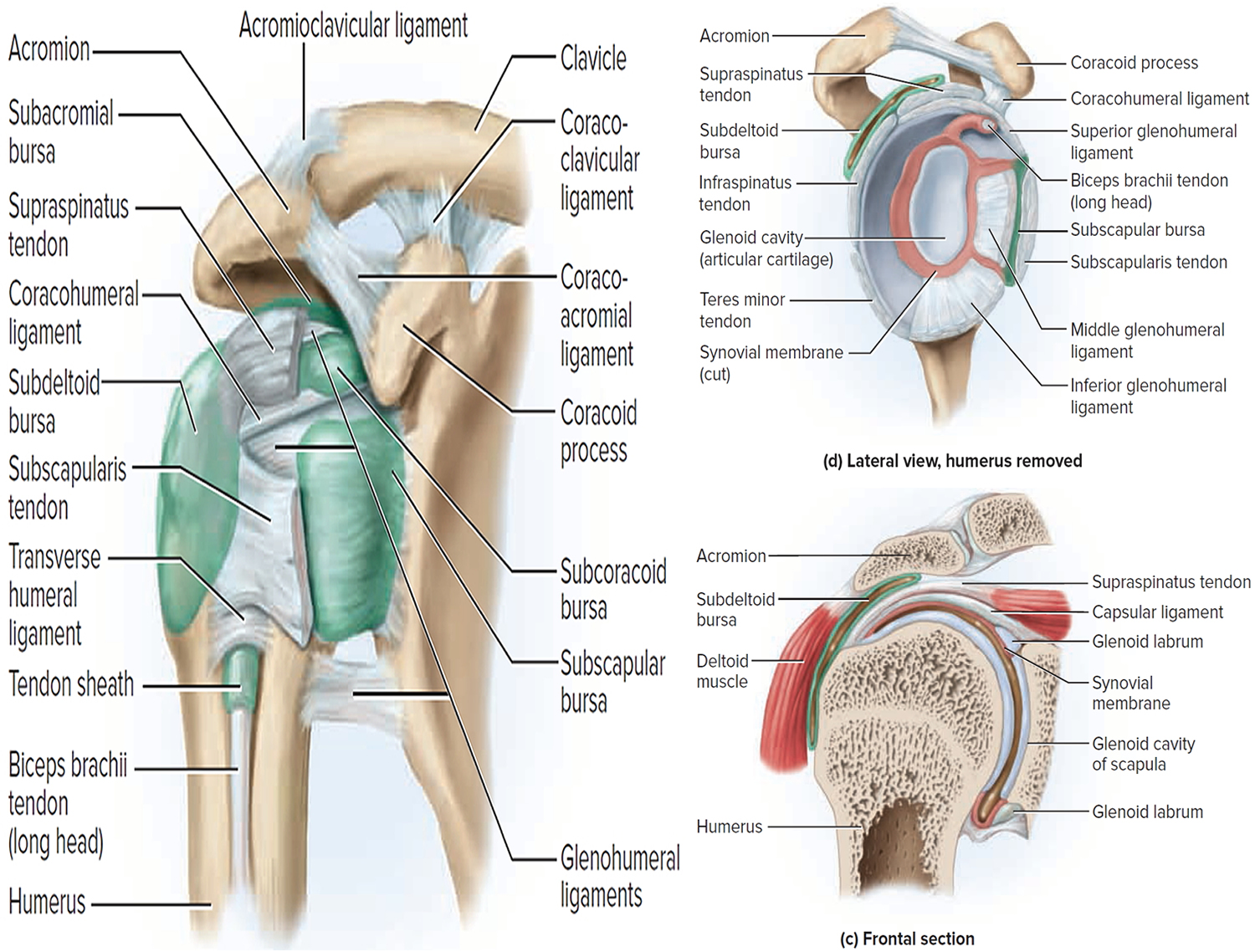
The main joint in the shoulder is formed by the arm bone and the shoulder blade. The joint socket is shallow, allowing a wide range of motion in the arm. The rotator cuff is made up of 4 muscles that surround the arm bone (see Figure 1). This cuff keeps the shoulder steady as the arm moves.
The supraspinatus muscle rests on top of the shoulder. Its tendon travels under the bone on the outside of the shoulder (the acromion). This tendon is the one most often injured because of its position between the bones. As the tendon becomes inflamed (sore and swollen), it can become pinched between the 2 bones. The sac of fluid that cushions the tendon can also be damaged.
A common cause of shoulder pain is soreness of the tendon (a cord that attaches a muscle to a bone) of the rotator cuff. This is the part of the shoulder that helps circular motion. Another common cause is soreness of the subacromial bursa (a sac of fluid under the highest part of the shoulder). You might experience soreness after painting, lifting items, or playing a sport—anything that requires you to lift your arms. Or you may not remember any specific injury, but you still feel pain in your shoulder.
The rotator cuff is a common source of pain in the shoulder and the pain can be the result of:
- Tendinitis. The rotator cuff tendons can be irritated or damaged.
- Bursitis. The bursa can become infl amed and swell with more fluid causing pain.
- Impingement. When you raise your arm to shoulder height, the space between the acromion and rotator cuff narrows. The acromion can rub against (or “impinge” on) the tendon and the bursa, causing irritation and pain.
Figure 1. Shoulder joint
Causes of shoulder tendonitis
Rotator cuff pain is common in both young athletes and middle-aged people. Young athletes who use their arms overhead for swimming, baseball, and tennis are particularly vulnerable. Those who do repetitive lifting or overhead activities using the arm, such as paper hanging, construction, or painting are also susceptible.
Pain may also develop as the result of a minor injury. Sometimes, it occurs with no apparent cause 4.
Symptoms of shoulder tendonitis
Rotator cuff pain commonly causes local swelling and tenderness in the front of the shoulder. You may have pain and stiffness when you lift your arm. There may also be pain when the arm is lowered from an elevated position.
Beginning symptoms may be mild. Patients frequently do not seek treatment at an early stage.
These symptoms may include:
- Minor pain that is present both with activity and at rest
- Pain radiating from the front of the shoulder to the side of the arm
- Sudden pain with lifting and reaching movements
- Athletes in overhead sports may have pain when throwing or serving a tennis ball
As the problem progresses, the symptoms increase:
- Pain at night
- Loss of strength and motion
- Difficulty doing activities that place the arm behind the back, such as buttoning or zippering
If the pain comes on suddenly, the shoulder may be severely tender. All movement may be limited and painful.
Diagnosis of shoulder tendonitis
After discussing your symptoms and medical history, your doctor will examine your shoulder. He or she will check to see whether it is tender in any area or whether there is a deformity. To measure the range of motion of your shoulder, your doctor will have you move your arm in several different directions. He or she will also test your arm strength.
Your doctor will check for other problems with your shoulder joint. He or she may also examine your neck to make sure that the pain is not coming from a “pinched nerve,” and to rule out other conditions, such as arthritis.
Imaging Tests
Other tests which may help your doctor confirm your diagnosis include:
- X-rays. Because x-rays do not show the so tissues of your shoulder like the rotator cuff , plain x-rays of a shoulder with rotator cuff pain are usually normal or may show a small bone spur. A special x-ray view, called an “outlet view,” sometimes will show a small bone spur on the front edge of the acromion.
- Magnetic resonance imaging (MRI) and ultrasound. These studies can create better images of so tissues like the rotator cuff tendons. They can show fluid or
inflammation in the bursa and rotator cuff. In some cases, partial tearing of the rotator cuff will be seen.
Treatment for shoulder tendonitis
The goal of treatment is to reduce pain and restore function. In planning your treatment, your doctor will consider your age, activity level, and general health.
Nonsurgical Treatment
In most cases, initial treatment is nonsurgical. Although nonsurgical treatment may take several weeks to months, many patients experience a gradual improvement and return to function.
Rest. Your doctor may suggest rest and activity modification, such as avoiding overhead activities.
Non-steroidal anti-inflammatory (NSAIDs) medicines. Drugs like ibuprofen and naproxen reduce pain and swelling.
Physical therapy. A physical therapist will initially focus on restoring normal motion to your shoulder. Stretching exercises to improve range of motion are very helpful. If you have difficulty reaching behind your back, you may have developed tightness of the posterior capsule of the shoulder (capsule refers to the inner lining of the shoulder and posterior refers to the back of the shoulder). Specific stretching of the posterior capsule can be very effective in relieving pain in the shoulder.
Once your pain is improving, your therapist can start you on a strengthening program for the rotator cuff muscles.
The following exercises may help you. Ask your doctor if you should do other exercises, too.
Range of motion
Stand up and lean over so you’re facing the floor. Let your sore arm dangle straight down. Draw circles in the air with your sore arm. Start with small circles, and then draw bigger ones. Repeat these exercises 5 to 10 times during the day. If you have pain, stop. You can try again later.
Rotator cuff strengthening
Use a piece of rubber tubing for these exercises. Stand next to a closed door with a doorknob. Loop the tubing around the knob. With your hand that is closest to the door, bend your arm at a 90° angle (at the elbow) and grab the loop of the tubing. Pull the band across your tummy. At first, do 1 set of 10 exercises. Try to increase the number of sets as your shoulder pain lessens. Do these exercises every day.
Upper extremity strengthening
As your pain goes away, try adding a general upper body weight-lifting program using weight machines or free weights. Lie on your right side with your left arm at your side. With a weight in your left hand and your forearm across your tummy, raise your forearm. Keep your elbow near your side.
Steroid injection. If rest, medications, and physical therapy do not relieve your pain, an injection of a local anesthetic and a cortisone preparation may be helpful. Cortisone is a very effective anti-inflammatory medicine. Injecting it into the bursa beneath the acromion can relieve pain.
Surgical Treatment for Shoulder Tendonitis
When nonsurgical treatment does not relieve pain, your doctor may recommend surgery.
The goal of surgery is to create more space for the rotator cuff. To do this, your doctor will remove the inflamed portion of the bursa. He or she may also perform
an anterior acromioplasty, in which part of the acromion is removed. This is also known as a subacromial decompression. These procedures can be performed using either an arthroscopic or open technique.
Arthroscopic technique
In arthroscopy, thin surgical instruments are inserted into two or three small puncture wounds around your shoulder. Your doctor examines your shoulder through a fiberoptic scope connected to a television camera. He or she guides the small instruments using a video monitor, and removes bone and so tissue. In most cases, the front edge of the acromion is removed along with some of the bursal tissue.
Your surgeon may also treat other conditions present in the shoulder at the time of surgery. These can include arthritis between the clavicle (collarbone) and the acromion (acromioclavicular arthritis), inflammation of the biceps tendon (biceps tendonitis), or a partial rotator cuff tear.
Open surgical technique
In open surgery, your doctor will make a small incision in the front of your shoulder. This allows your doctor to see the acromion and rotator cuff directly.
Rehabilitation
After surgery, your arm may be placed in a sling for a short period of time. This allows for early healing. As soon as your comfort allows, your doctor will remove the sling to begin exercise and use of the arm.
Your doctor will provide a rehabilitation program based on your needs and the findings at surgery. This will include exercises to regain range of motion of the shoulder and strength of the arm. It typically takes 2 to 4 months to achieve complete relief of pain, but it may take up to a year.
Elbow tendonitis
Tennis elbow or lateral epicondylitis, is a painful condition of the elbow caused by overuse 5. Not surprisingly, playing tennis or other racquet sports can cause this condition. However, several other sports and activities can also put you at risk.
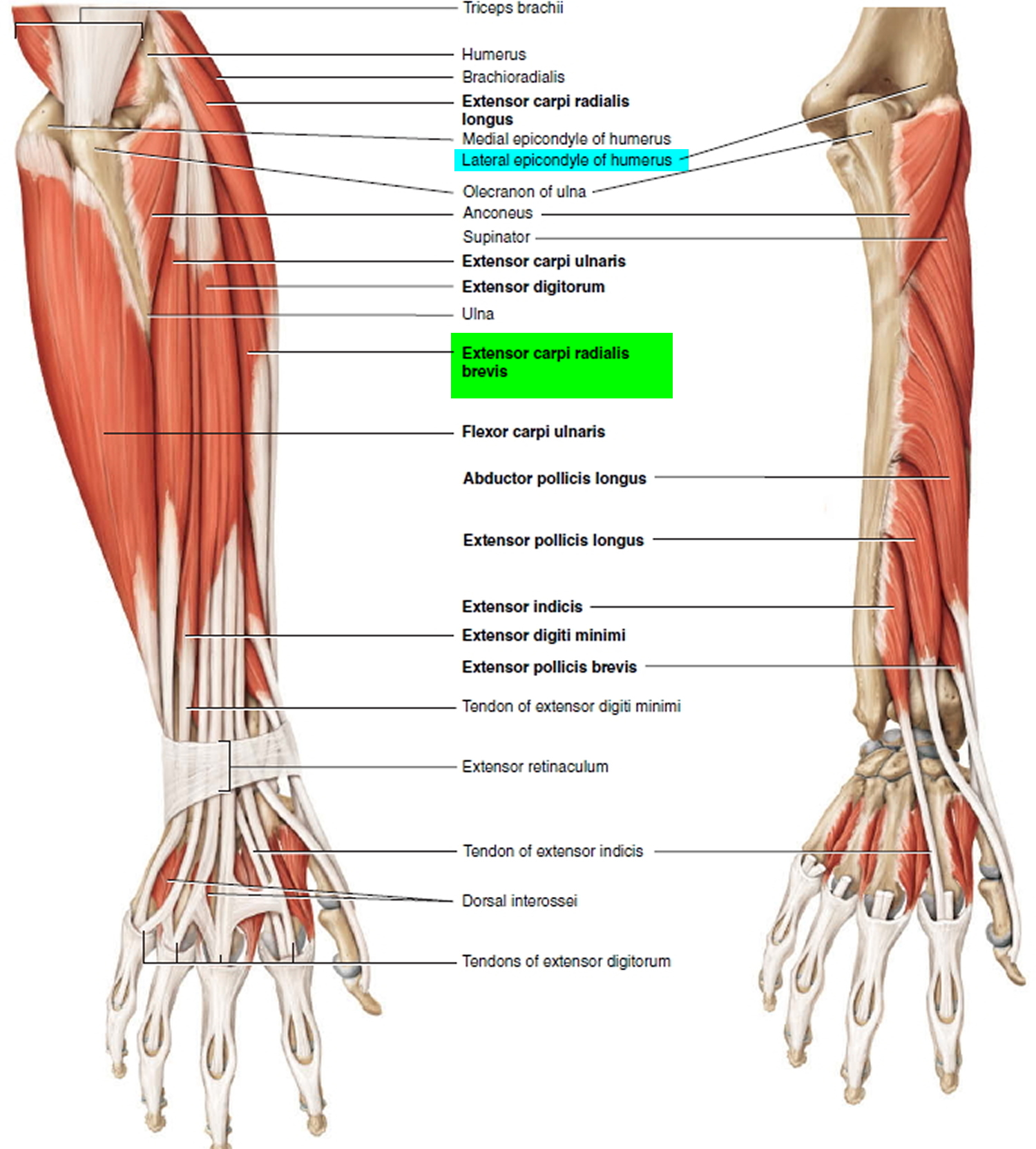
Tennis elbow is an inflammation of the tendons (usually the origin of the extensor carpi radialis brevis muscle) that join the forearm muscles on the outside of the elbow. The tendon usually involved in tennis elbow is called the Extensor Carpi Radialis Brevis. The extensor carpi radialis brevis muscle originates on the lateral epicondyle (thus the name lateral epicondylitis) of the humerus and inserts into metacarpal #3. Its function is extends and abducts the hand at the wrist joint. The forearm muscles and tendons become damaged from overuse — repeating the same motions again and again. This leads to pain and tenderness on the outside of the elbow.
There are many treatment options for tennis elbow. In most cases, treatment involves a team approach. Primary doctors, physical therapists, and, in some cases, surgeons work together to provide the most effective care.
Figure 2. Elbow joint
Causes of Elbow tendonitis
Overuse
Recent studies show that tennis elbow is often due to damage to a specific forearm muscle. The extensor carpi radialis brevis muscle helps stabilize the wrist when the elbow is straight. This occurs during a tennis groundstroke, for example. When the extensor carpi radialis brevis muscle is weakened from overuse, microscopic tears form in the tendon where it attaches to the lateral epicondyle. This leads to inflammation and pain.
The extensor carpi radialis brevis muscle may also be at increased risk for damage because of its position. As the elbow bends and straightens, the muscle rubs against bony bumps. This can cause gradual wear and tear of the muscle over time.
Activities
Athletes are not the only people who get tennis elbow. Many people with tennis elbow participate in work or recreational activities that require repetitive and vigorous use of the forearm muscle.
Painters, plumbers, and carpenters are particularly prone to developing tennis elbow. Studies have shown that auto workers, cooks, and even butchers get tennis elbow more often than the rest of the population. It is thought that the repetition and weight lifting required in these occupations leads to injury.
Age
Most people who get tennis elbow are between the ages of 30 and 50, although anyone can get tennis elbow if they have the risk factors. In racquet sports like tennis, improper stroke technique and improper equipment may be risk factors.
Unknown
Lateral epicondylitis can occur without any recognized repetitive injury. This occurence is called “insidious” or of an unknown cause.
Symptoms of Elbow tendonitis
The symptoms of tennis elbow develop gradually. In most cases, the pain begins as mild and slowly worsens over weeks and months. There is usually no specific injury associated with the start of symptoms.
Common signs and symptoms of tennis elbow include:
- Pain or burning on the outer part of your elbow
- Weak grip strength
The symptoms are often worsened with forearm activity, such as holding a racquet, turning a wrench, or shaking hands. Your dominant arm is most often affected; however both arms can be affected.
Diagnosis of Elbow tendonitis
Your doctor will consider many factors in making a diagnosis. These include how your symptoms developed, any occupational risk factors, and recreational sports participation.
Your doctor will talk to you about what activities cause symptoms and where on your arm the symptoms occur. Be sure to tell your doctor if you have ever injured
your elbow. If you have a history of rheumatoid arthritis or nerve disease, tell your doctor.
During the examination, your doctor will use a variety of tests to pinpoint the diagnosis. For example, your doctor may ask you to try to straighten your wrist and fingers against resistance with your arm fully straight to see if this causes pain. If the tests are positive, it tells your doctor that those muscles may not be healthy.
Tests:
- X-rays. These tests provide clear images of dense structures like bone. They may be taken to rule out arthritis of the elbow.
- Magnetic resonance imaging (MRI) scan. If your doctor thinks your symptoms are related to a neck problem, an MRI scan may be ordered. MRIs scans show details of soft tissues, and will help your doctor see if you have a possible herniated disk or arthritis in your neck. Both of these conditions often produce arm pain.
- Electromyography (EMG). Your doctor may order an EMG to rule out nerve compression. Many nerves travel around the elbow, and the symptoms of nerve compression are similar to those of tennis elbow.
Treatment of Elbow tendonitis
Nonsurgical Treatment
Approximately 80% to 95% of patients have success with nonsurgical treatment.
Rest. The first step toward recovery is to give your arm proper rest. This means that you will have to stop participation in sports or heavy work activities for several weeks.
Non-steroidal anti-inflammatory (NSAIDs) medicines. Drugs like aspirin or ibuprofen reduce pain and swelling.
Equipment check. If you participate in a racquet sport, your doctor may encourage you to have your equipment checked for proper fit. Stiffer racquets and looser-
strung racquets often can reduce the stress on the forearm, which means that the forearm muscles do not have to work as hard. If you use an oversized racquet,
changing to a smaller head may help prevent symptoms from recurring.
Physical therapy. Specific exercises are helpful for strengthening the muscles of the forearm. Your therapist may also perform ultrasound, ice massage, or muscle-stimulating techniques to improve muscle healing.
Brace. Using a brace centered over the back of your forearm may also help relieve symptoms of tennis elbow. This can reduce symptoms by resting the muscles and tendons.
Steroid injections. Steroids, such as cortisone, are very effective anti-inflammatory medicines. Your doctor may decide to inject your damaged muscle with a steroid to relieve your symptoms.
Extracorporeal shock wave therapy. Shock wave therapy sends sound waves to the elbow. These sound waves create “microtrauma” that promote the body’s natural healing processes. Shock wave therapy is considered experimental by many doctors, but some sources show it can be effective.
Platelet-rich plasma is currently being investigated for its effectiveness in speeding the healing of a variety of tendon injuries. Platelet-rich plasma is a preparation developed from a patient’s own blood. It contains a high concentration of proteins called growth factors that are very important in the healing of injuries. Current research on platelet-rich plasma and lateral epicondylitis is very promising. A few treatment centers across the country are incorporating platelet-rich plasma injections into the nonsurgical treatment regimen for lateral epicondylitis. However, this method is still under investigation and more research is necessary to fully prove platelet-rich plasma’s effectiveness.
Surgical Treatment
If your symptoms do not respond after 6 to 12 months of nonsurgical treatments, your doctor may recommend surgery.
Most surgical procedures for tennis elbow involve removing diseased muscle and reattaching healthy muscle back to bone.
The right surgical approach for you will depend on a range of factors. These include the scope of your injury, your general health, and your personal needs. Talk with your doctor about the options. Discuss the results your doctor has had, and any risks associated with each procedure.
Open surgery
The most common approach to tennis elbow repair is open surgery. This involves making an incision over the elbow.
Open surgery is usually performed as an outpatient surgery. It rarely requires an overnight stay at the hospital.
Arthroscopic surgery
Tennis elbow can also be repaired using miniature instruments and small incisions. Like open surgery, this is a same-day or outpatient procedure.
Surgical risks
As with any surgery, there are risks with tennis elbow surgery. The most common things to consider include:
- Infection
- Nerve and blood vessel damage
- Possible prolonged rehabilitation
- Loss of strength
- Loss of flexibility
- The need for further surgery
Rehabilitation
Following surgery, your arm may be immobilized temporarily with a splint. About 1 week later, the sutures and splint are removed.
After the splint is removed, exercises are started to stretch the elbow and restore flexibility. Light, gradual strengthening exercises are started about 2 months after surgery.
Your doctor will tell you when you can return to athletic activity. This is usually 4 to 6 months after surgery. Tennis elbow surgery is considered successful in 80% to 90% of patients. However, it is not uncommon to see a loss of strength.
Bicep tendonitis
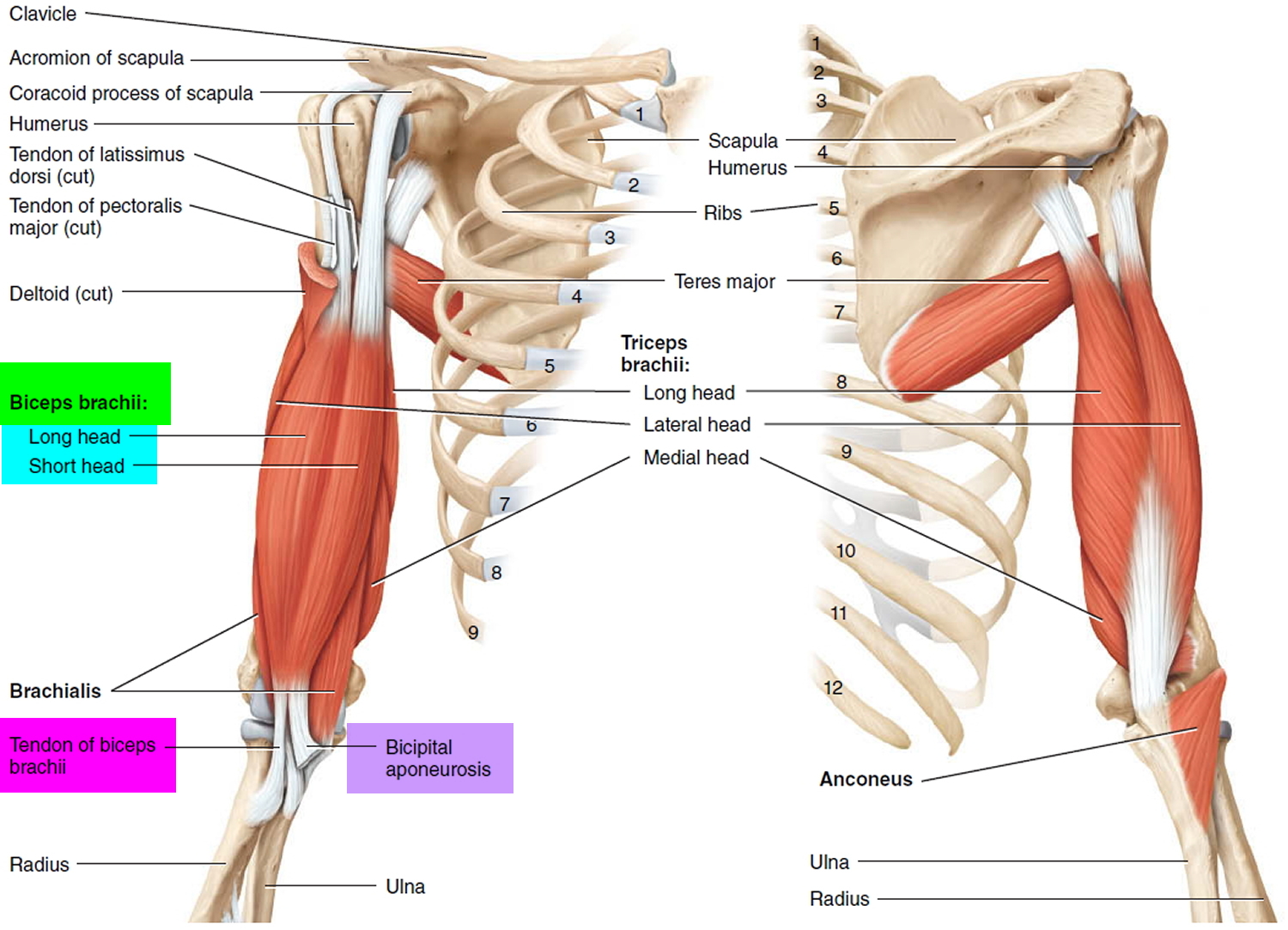
The biceps is the muscle in your upper arm that you flex when you bend your arm or show off your muscles. This muscle also helps you twist your forearm outward. Tough connective tissues called tendons attach the biceps muscle to the elbow and shoulder and help you move your arm.
The tendon that attaches the lower part of the biceps to the elbow is the distal tendon. The tendons that attach the top of the biceps muscle to the shoulder are the proximal tendons.
There are two proximal tendons — the long head and the short head. They attach to your shoulder blade in different places to hold the top of your upper arm bone firmly in your shoulder socket while still allowing it to move.
If any of these tendons become swollen or irritated from overuse, it can lead to a condition called biceps tendonitis. If you have biceps tendonitis, it can hurt just to move your arm. The good news is, most cases heal on their own with rest and medication.
Symptoms and signs of Proximal Biceps Tendonitis
Proximal biceps tendonitis usually starts out slowly and becomes more painful the more a person uses that arm. But sometimes an injury or small tear in the tendon can cause problems right away.
Some of the more common symptoms of proximal biceps tendonitis include 6:
- pain in the front or side of the shoulder and the upper arm
- pain in the arm at night, especially when you sleep on that side
- pain when you move your arm, raise it above your head, or reach behind you
- shoulder weakness and stiffness
- loss of some motion in the arm
Figure 3. Biceps muscles and tendons
What Causes Bicep tendonitis ?
The word “tendonitis” simply means that the tendon is irritated and swollen. In teens, biceps tendonitis is usually an overuse injury. Baseball pitchers, swimmers, tennis players, and people who have to reach above their heads a lot are at greater risk because of the repeated stress on their shoulders and upper arms.
Proximal biceps tendonitis often happens along with other shoulder problems. In most cases, there is also damage to another shoulder tendon called a rotator cuff tendon.
How Do Doctors Diagnose Bicep tendonitis ?
If your shoulder and upper arm hurt when you move your arm, and you’re worried that you might have biceps tendonitis, call a doctor.
The doctor will examine you and ask about any activities you’ve been doing that might have caused the problem. He or she will also check the strength and range of motion in your shoulder and look to see if it feels loose or unstable. For more serious cases (or to rule out other problems), the doctor might want you to have an X-ray, ultrasound, or magnetic resonance imaging (MRI) scan.
How Can you Prevent Biceps Tendonitis ?
The best way to prevent biceps tendonitis is to avoid activities that put your arms above your head a lot. But if you swim or play tennis or baseball, that might not be an option!
If your activities put you at risk for biceps tendonitis, you’ll want to do exercises that strengthen the muscles of your shoulder and upper arm. Strong muscles will keep the entire area more stable and less likely to get injured.
If you play a sport that puts you at greater risk of biceps tendonitis, make sure you know the right way to play. Playing in the wrong way can put your arm in weird positions that may put added stress on your shoulder. As much as you can, try to avoid reaching above your head or doing other things that require a lot of shoulder movement.
Most important, if you feel any pain in your shoulder or upper arm, stop doing the activity that might be causing it right away. Don’t start the activity again until the pain is gone or a doctor has told you it’s OK. Never try to ignore pain or play through it. This will most likely only make the condition worse.
Biceps Tendonitis Treatment
Most cases of biceps tendonitis can be treated at home with fairly simple methods. Although doctors sometimes need to do surgery to repair badly injured proximal biceps tendons, it’s usually for adults. Kids and teens almost never need surgery for this kind of injury.
Treatment can include the following:
- Rest your arm. Stop doing activities that require a lot of shoulder movement and try to avoid using your injured arm for any lifting or reaching.
- Ice the affected area. Apply ice or a cold compress to your shoulder for up to 20 minutes several times a day to help keep the swelling down. (Never apply ice directly to the skin.)
- Take anti-inflammatory medications. Painkillers such as ibuprofen can help relieve pain and reduce swelling in the shoulder and upper arm. The doctor also may recommend a cream or patch that can be applied to the skin. In some cases, doctors may give people steroid injections to ease pain and help reduce swelling.
- Do stretching and strengthening exercises. These will help strengthen your shoulder and restore its range of motion. Strengthening and stretching exercises can help you recover and make you less likely to reinjure your arm. A doctor or a physical therapist can work with you to develop a good exercise program.
The good news about proximal biceps tendonitis is that most cases heal just fine on their own. But it does require patience. The key with this kind of injury is to give your arm plenty of time to rest. You don’t want to jump back into your sport or activity too soon or you’ll risk making things worse and spending even more time on the sidelines.
Wrist Tendonitis
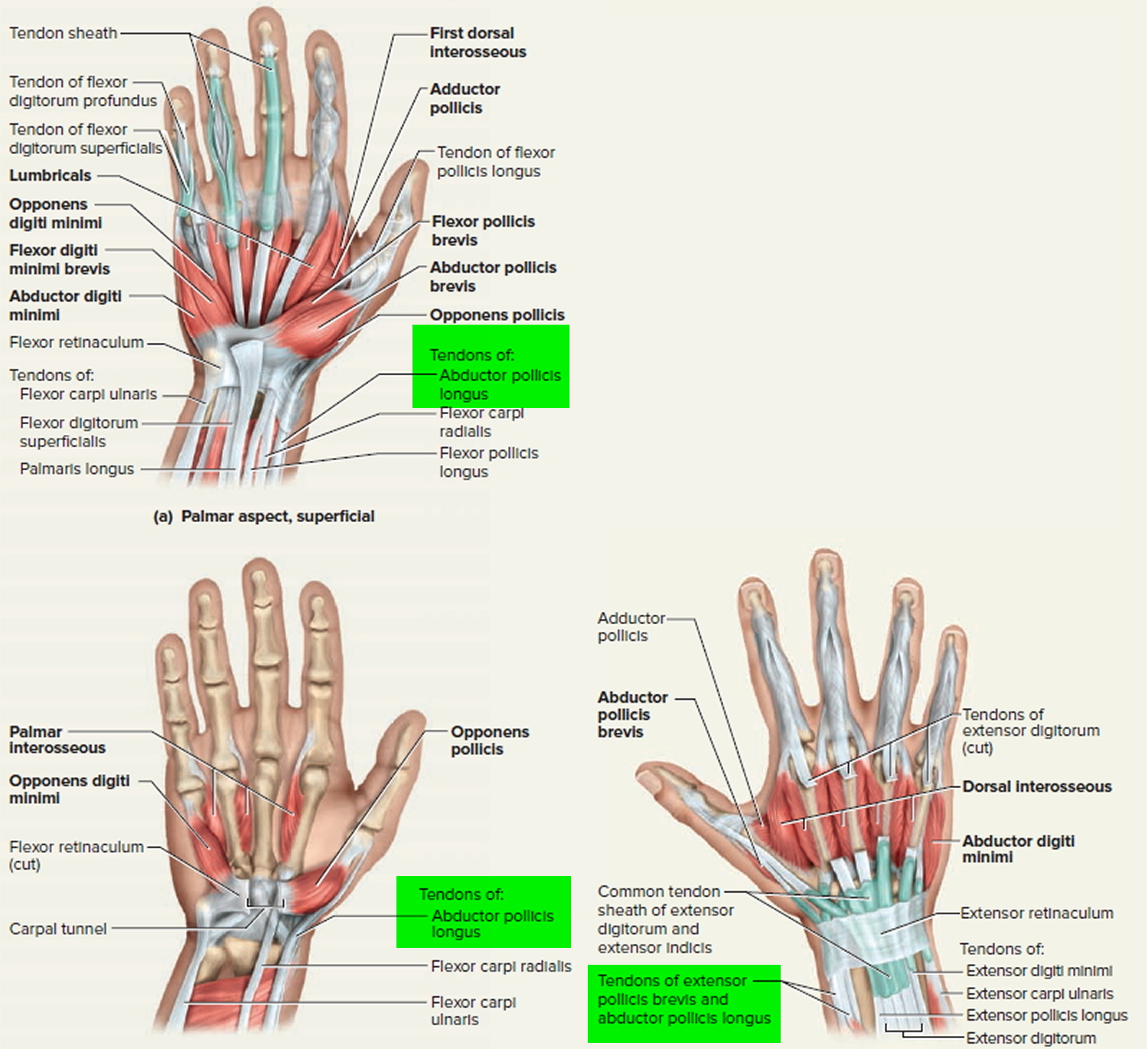
De Quervain’s tenosynovitis is a painful condition that affects the tendons in your wrist. It occurs when the 2 tendons around the base of your thumb become swollen 7. The swelling causes the sheaths (casings) covering the tendons to become inflamed. Swelling of the tendons, and the tendon sheath, can cause pain and tenderness along the thumb side of the wrist. This is particularly noticeable when forming a fi st, grasping or gripping something, or when turning the wrist. The swelling also puts pressure on nearby nerves, causing pain and numbness.
Two of the main tendons to the thumb pass through a tunnel (or series of pulleys) located on the thumb side of the wrist. Tendons are rope-like structures that attach muscle to bone. Tendons are covered by a slippery thin so -tissue layer, called synovium. This layer allows the tendons to slide easily through a fibrous tunnel called a sheath. Any swelling of the tendons and/or thickening of the sheath, results in increased friction and pain with certain thumb and wrist movements.
Figure 4. Wrist tendon (thumb tendons)
Symptoms of wrist tendonitis
The main symptom of de Quervain’s tenosynovitis is pain or tenderness at the base of your thumb. You might also feel pain going up your forearm. The pain may develop slowly or come on suddenly. It may get worse when you use your hand, thumb, or wrist.
Other symptoms include 8:
- Pain may be felt over the thumb side of the wrist. This is the main symptom. The pain may appear either gradually or suddenly. Pain is felt in the wrist and can travel up the forearm. The pain is usually worse when the hand and thumb are in use. This is especially true when forcefully grasping objects or twisting the wrist.
- Swelling near the base of your thumb. This swelling may accompany a fluid-filled cyst in this region.
- Pain and swelling may make it difficult to move the thumb and wrist.
- Numbness along the back of your thumb and index finger.
- A “catching” or “snapping” feeling when you move your thumb.
- A squeaking sound as the tendons move within the swollen sheaths.
What causes wrist tendonitis ?
The most common cause of de Quervain’s tenosynovitis is chronic overuse of the wrist. Repetitive movements day after day cause irritation and pain. One common movement that causes it is lifting a child into a car seat. Another is lifting heavy grocery bags by the handles. Other causes could include a direct injury to the wrist or inflammatory arthritis.
You are more likely to develop de Quervain’s tenosynovitis if:
- You are a woman.
- You are 40 years of age or older.
- Your hobby or job involves repetitive hand and wrist motions. This is a very common cause.
- You have injured your wrist. Scar tissue can restrict the movement of your tendons.
- You are pregnant. Hormonal changes during pregnancy can cause it.
- You have arthritis.
How is wrist tendonitis diagnosed ?
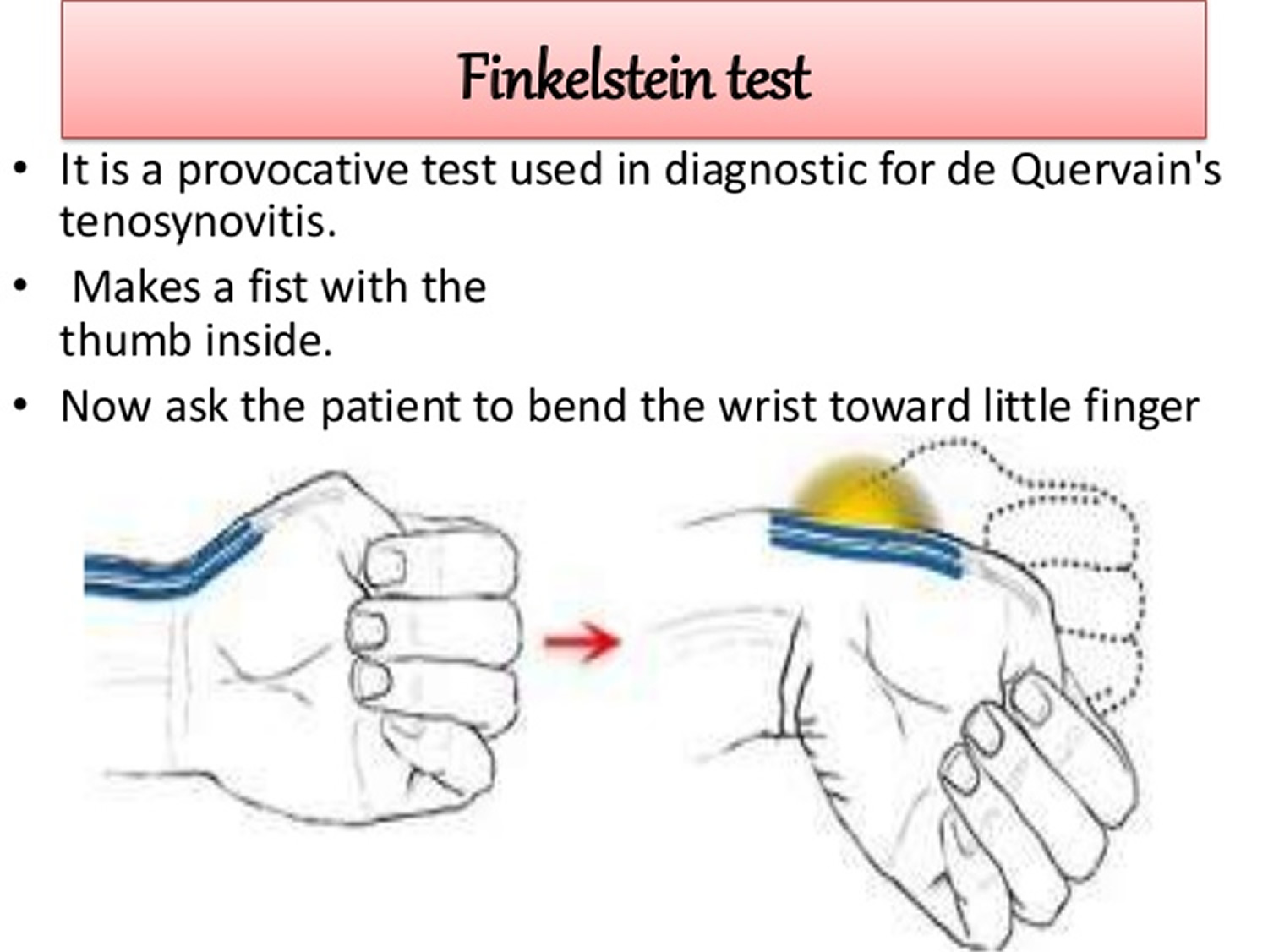
To diagnose de Quervain’s tenosynovitis, your doctor may do a simple test. It is called the Finkelstein test. First, you bend your thumb so it rests across your palm. Then you make a fist, closing your fingers over your thumb. Last, you bend your wrist toward your little finger. If you have tenderness or pain at the base of your thumb, you probably have de Quervain’s tenosynovitis.
Figure 5. Finkelstein test
Other tests such as X-rays usually aren’t needed to diagnose the condition.
Can wrist tendonitis be prevented or avoided ?
The best way to prevent de Quervain’s tenosynovitis is to avoiding repetitive movements. Change your actions to reduce the stress on your wrists. Take frequent breaks to rest if you are using your wrists. Wear a brace or splint on your thumb and wrist, if necessary.
Follow the exercise routine suggested by your doctor or physical therapist. Be sure to tell him or her about any activities that cause pain, numbness, or swelling.
Treatment for wrist tendonitis
Treatment for de Quervain’s tenosynovitis focuses on reducing pain and swelling. It includes:
- Applying heat or ice to the affected area.
- Taking a nonsteroidal anti-inflammatory drug (NSAID). These include ibuprofen (Advil, Motrin) or naproxen (Aleve).
- Avoiding activities that cause pain and swelling. Especially avoid those that involve repetitive hand and wrist motions.
- Wearing a splint 24 hours a day for 4 to 6 weeks to rest your thumb and wrist.
- Getting injections of corticosteroids or a local anesthetic (numbing medicine) into the tendon sheath. These injections are very effective and are used regularly.
A physical therapist or occupational therapist can show you how to change the way you move. This can reduce stress on your wrist. He or she can also teach you exercises to strengthen your muscles.
Most people notice improvement after 4 to 6 weeks of treatment. They are able to use their hands and wrists without pain once the swelling is gone.
You might need surgery if your case is severe or if other treatments don’t relieve your pain.
Surgical Treatment
Surgery may be recommended if symptoms are severe or do not improve. The goal of surgery is to open the thumb compartment (covering) to make more room for the irritated tendons.
Regardless of the treatment, normal use of the hand usually can be resumed once comfort and strength have returned. Your orthopaedic surgeon can advise you on the best treatment for your situation.
Patellar tendonitis
Jumper’s knee — also known as patellar tendonitis or patellar tendinopathy — is an inflammation or injury of the patellar tendon, the cord-like tissue that joins the patella (kneecap) to the tibia (shin bone). Jumper’s knee is an overuse injury (when repeated movements cause tissue damage or irritation to a particular area of the body) 9.
Constant jumping, landing, and changing direction can cause strains, tears, and damage to the patellar tendon. So kids who regularly play sports that involve a lot of repetitive jumping — like track and field (particularly high-jumping), basketball, volleyball, gymnastics, running, and soccer — can put a lot of strain on their knees.
Jumper’s knee can seem like a minor injury that isn’t really that serious. Because of this, many athletes keep training and competing and tend to ignore the injury or attempt to treat it themselves. But it’s important to know that jumper’s knee is a serious condition that can get worse over time and ultimately require surgery. Early medical attention and treatment can help prevent continued damage to the knee.
How the Knee Works
To understand how jumper’s knee happens, it helps to understand how the knee works. The knee, which is the largest joint in the body, provides stability to the leg and allows it to bend, swivel, and straighten. Several parts of the body interact to allow the knee to function properly:
Bones like the femur (thighbone), the tibia (shinbone), and the patella (kneecap) give the knee the strength needed to support the weight of the body. The bones that meet at the knee allow it to bend smoothly.
Muscles provide the tug on the bones needed to bend, straighten, and support joints. The muscles around the knee include the quadriceps (at the front of the thigh) and the hamstring (on the back of the thigh). The quadriceps muscle helps straighten and extend the leg, and the hamstring helps bend the knee.
Tendons are strong bands of tissue that connect muscles to bones. The tendons in the front of the knee are the quadriceps tendon and the patellar tendon. The quadriceps tendon connects to the top of the patella and allows the leg to extend. The patellar tendon connects to the bottom of the kneecap and attaches to the top of the tibia.
Similar to tendons, ligaments are strong bands of tissue that connect bones to other bones.
By working together, bones, muscles, tendons, and ligaments enable the knee to move, bend, straighten, provide strength to jump, and stabilize the leg for landing.
When the knee is extended, the quadriceps muscle pulls on the quadriceps tendon, which in turn pulls on the patella. Then, the patella pulls on the patellar tendon and the tibia and allows the knee to straighten. In contrast, when bending the knee, the hamstring muscle pulls on the tibia, which causes the knee to flex.
In jumper’s knee, the patellar tendon is damaged. Since this tendon is crucial to straightening the knee, damage to it causes the patella to lose any support or anchoring. This causes pain and weakness in the knee, and leads to difficulty in straightening the leg.
Figure 6. Ligaments and tendons of the knee
Symptoms of Patellar tendonitis
Common symptoms of jumper’s knee include:
- pain directly over the patellar tendon (or more specifically, below the kneecap)
- stiffness of the knee, particularly while jumping, kneeling, squatting, sitting, or climbing stairs
- pain when bending the knee
- pain in the quadriceps muscle
- leg or calf weakness
Less common symptoms include:
- balance problems
- warmth, tenderness, or swelling around the lower knee
Treatment of Patellar tendonitis
Jumper’s knee is first evaluated by a grading system that measures the extent of the injury (grades range from 1 to 5, with grade 1 being pain only after intense activity and grade 5 being daily constant pain and the inability to participate in any sporting activities).
While examining the knee, a doctor or medical professional will ask the person to run, jump, kneel, or squat to determine the level of pain. In addition, an X-ray or MRI might be recommended. Depending on the grade of the injury, treatment can range from rest and icepacks to surgery.
For mild to moderate jumper’s knee, treatment includes:
- resting from activity or adapting a training regimen that greatly reduces any jumping or impact
- icing the knee to reduce pain and inflammation
- wearing a knee support or strap (called an intrapatellar strap or a Chopat strap) to help support the knee and patella. The strap is worn over the patellar tendon, just beneath the kneecap. A knee support or strap can help minimize pain and relieve strain on the patellar tendon.
- elevating the knee when it hurts (for example, placing a pillow under the leg)
- anti-inflammatory medications, like ibuprofen, to minimize pain and swelling
- massage therapy
- minimum-impact exercises to help strengthen the knee
- rehabilitation programs that include muscle strengthening, concentrating on weight-bearing muscle groups like the quadriceps and calf muscles
- specialized injections to desensitize nerve endings and reduce inflammation
On rare occasions, such as when there’s persistent pain or the patellar tendon is seriously damaged, jumper’s knee requires surgery. Surgery includes removing the damaged portion of the patellar tendon, removing inflammatory tissue from the lower area (or bottom pole) of the patella, or making small cuts on the sides of the patellar tendon to relieve pressure from the middle area.
After surgery, a rehabilitation program involving strengthening exercises and massage is followed for several months to a year.
Recovery
Recovering from jumper’s knee can take a few weeks to several months. It’s best to stay away from any sport or activity that can aggravate the knee and make conditions worse.
But, recovering from jumper’s knee doesn’t mean that someone can’t participate in any sports or activities. Depending on the extent of the injury, low-impact sports or activities can be substituted (for instance, substituting swimming for running). Your doctor will let you know what sports and activities are off-limits during the healing process.
Preventing Jumper’s Knee
The most important factor in preventing jumper’s knee is stretching. A good warm-up regimen that involves stretching the quadriceps, hamstring, and calf muscles can help prevent jumper’s knee. It’s always a good idea to stretch after exercising, too.
Peroneal tendonitis
The peroneal (fibularis muscles) tendons run on the outside of the ankle just behind the bone called the fibula. Tendons connect muscle to bone and allow them to exert their force across the joints that separate bones. Ligaments, on the other hand, connect bone to bone. Tendinitis implies that there is inflammation, enlargement and thickening with swelling of the tendon. This usually occurs in the setting of overuse, meaning a patient or athlete does a repetitive activity that irritates the tendon over long periods of time. However, in studies that have taken the tendons and looked at them under a microscope, there really are not the types of inflammatory cells once thought. There is really more of an enlargement and thickening of the tendon. This is better termed tendinosis.
People with peroneal tendinitis typically have either tried a new exercise or have markedly increased their activities. Characteristic activities include marathon running or others which require repetitive use of the ankle. Patients will usually present with pain right around the back of the ankle. There is usually no history of a specific injury.
What causes peroneal tendinitis ?
As discussed above, improper training or rapid increases in training and poor shoewear can lead to peroneal tendinitis. Also, patients who have a hindfoot varus (turning inward) posture may be more susceptible. This is because in those patients, the heel is slightly turned inwards which requires that the peroneal tendons work harder. Their main job is to evert or turn the ankle to the outside, which fights against the varus position. The harder the tendons work, the more likely they are to develop tendinitis.
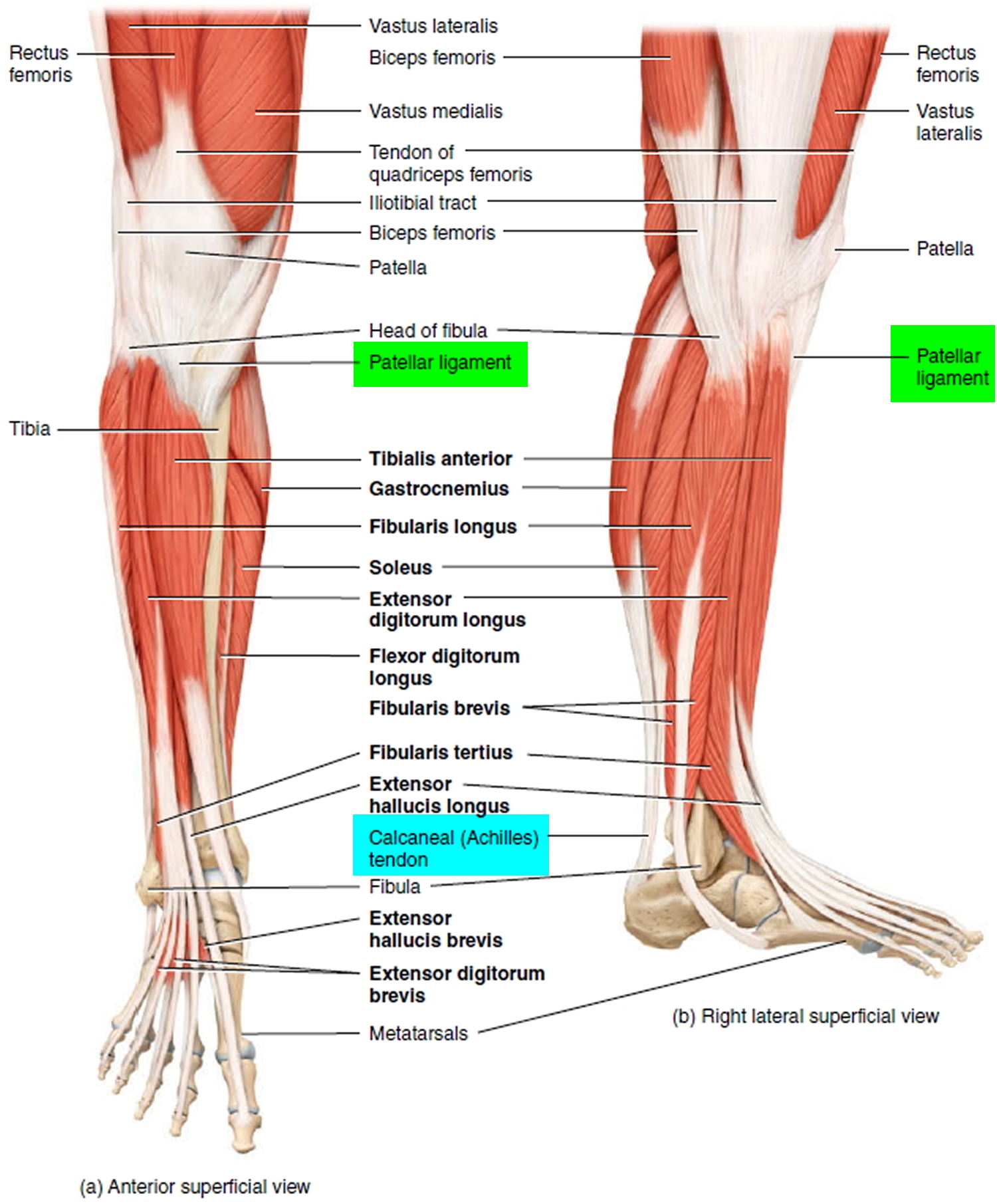
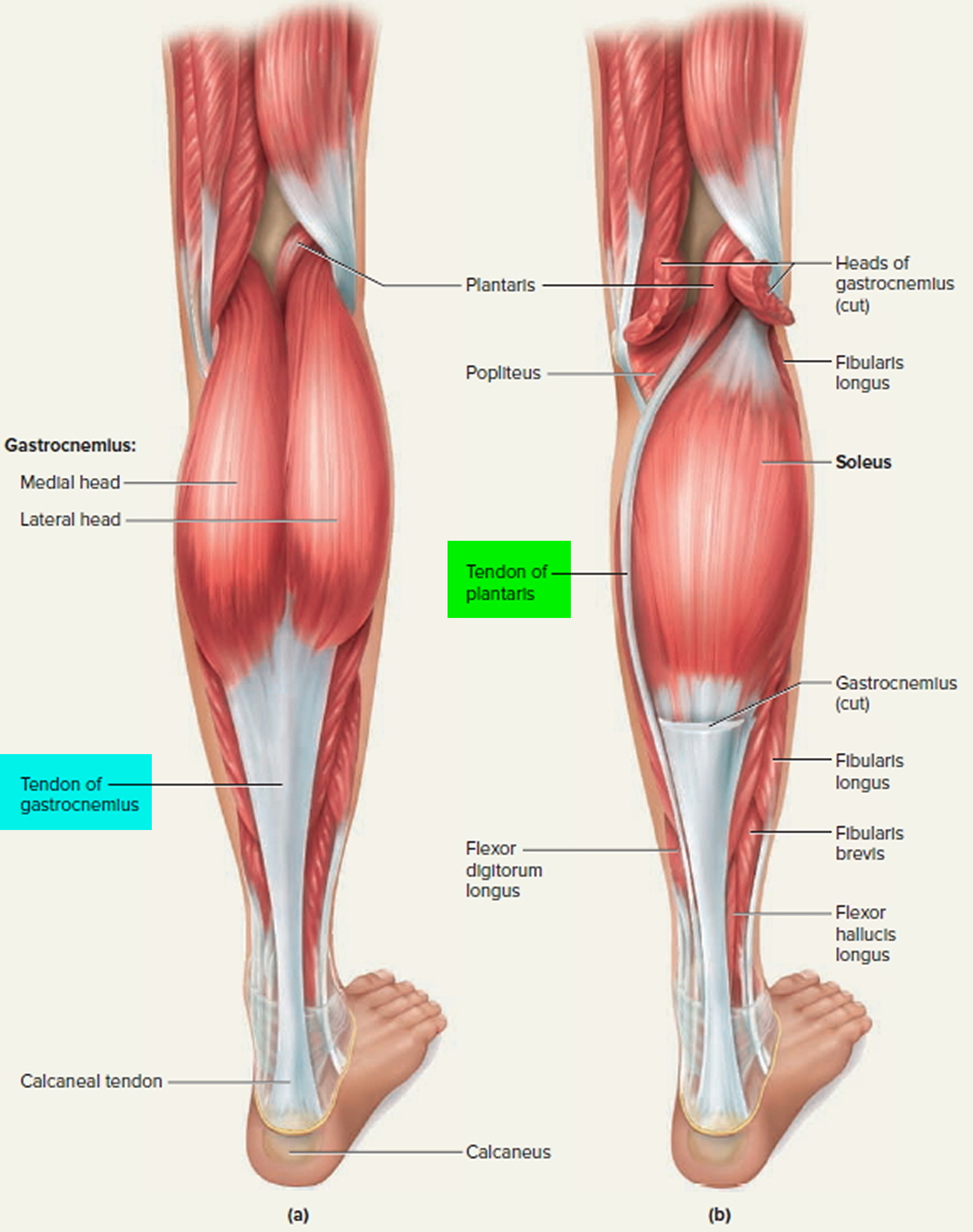
Figure 7. Tendons of the calf and foot (back of leg)
How is peroneal tendonitis diagnosed ?
The diagnosis of peroneal tendonitis can be made in large part by history (i.e. the story a patient tells). As noted above, patients will have an overuse activity, rapid increase in recent activity, or other training errors and will have pain in the back and outside of the ankle. There is pain on exam to palpation right on the peroneal tendons. I t is important to distinguish this from pain over the fibula, which might indicate a different problem (i.e. stress reaction of the bone). Pain on the fibula occurs directly over the bone which is easily palpated. Pain in the peroneals occurs slightly further behind. There is also pain with inversion or carrying the ankle to the outside. Patients may also have weakness in trying to bring the ankle to the outside (i.e. in eversion). It is important to look for the varus posturing of the heel which, as noted above, means that the heel is turned inwards. This can predispose a patient to the problem. The workup can also include using radiology. X-rays will typically be normal. Ultrasound is a very effective and relatively inexpensive way to assess the tendons and can show an abnormal appearance or tear which sometimes occurs. An MRI is also equally important and can also show a tear.
What are treatment options for peroneal tendonitis ?
The vast majority of peroneal tendinosis will heal without surgery. This is because it is an overuse injury and can heal with rest. If there is significant pain, a CAM Walker boot for several weeks is a good idea. If there really is no tenderness with walking, an ankle brace might be the next best step. Patients should very much limit how much they are walking or on their feet until the pain abates. This usually takes several weeks. Resumption of training can then occur, but must occur very slowly and be based on pain. For those patients who have hindfoot varus, as noted above, an orthotic that tilts the ankle to the opposite side may well help to offload the tendons. It is important to talk to your doctor about changing your training. This includes using new shoes for running or also cross-training, which means alternating activities each day. Physical therapy is also very important. This, as with ankle sprains, can be done to strengthen the tendons.
There is some interest at the moment in using platelet-rich plasma to help stimulate healing growth. Currently, there are no studies showing that this works for the peroneal tendons. Steroids are probably best avoided as they can actually damage tendon. Surgical treatment is indicated if the pain does not get better with rest. Conservative treatment – that is, without surgery – should last, however, even up to a year before considering surgery. If there is a tear, meaning a split that runs along the length of the tendons, one could consider cleaning it out and repairing the tendon. Sometimes, making the groove in the back of the bone of the fibula deeper allows the tendons more space and can help as well. Finally, if the tendon is very bad, one may need to resect the tendon and connect both the longus and brevis together. Only the specific tendon involved should be addressed. Occasionally, both may be involved.
How long is the recovery for peroneal tendonitis ?
Patients usually recover fully but this can take considerable time. You must be patient and allow the tendon to heal before going back to activity. If you need surgery, your recovery time may be substantial. You may be instructed not to put your foot down with weight for about six weeks. Your orthopaedic foot and ankle surgeon likely will order physical therapy ensue.
The outcome is usually good. However, sometimes it takes time for people to get back to their activity. When a tear develops and there is chronic thickening of the tendon, the outcomes are not as good.
Potential Complications of peroneal tendonitis
If the tendinosis is not addressed, tearing of the tendon can occur. Also, weakness of the tendons can lead to an ankle sprain. In the case of surgery, infection can develop. Nerve damage can occur if the sural nerve which runs along the side of the foot and provides sensation to the foot is cut or stretched. Instability itself can lead to many sprains which can damage the cartilage on the inside of the ankle.
Posterior tibial tendonitis
The posterior tibial tendon serves as one of the major supporting structures of the foot, helping it to function while walking. Posterior tibial tendon dysfunction (PTTD) is a condition caused by changes in the tendon, impairing its ability to support the arch. This results in flattening of the foot.
Posterior tibial tendon dysfunction is often called adult acquired flatfoot because it is the most common type of flatfoot developed during adulthood. Although this condition typically occurs in only one foot, some people may develop it in both feet. Posterior tibial tendon dysfunctionis usually progressive, which means it will keep getting worse, especially if it is not treated early.
Causes of Posterior tibial tendonitis
Overuse of the posterior tibial tendon is often the cause of posterior tibial tendon dysfunction. In fact, the symptoms usually occur after activities that involve the tendon, such as running, walking, hiking or climbing stairs.
Symptoms of Posterior tibial tendonitis
The symptoms of posterior tibial tendon dysfunction may include pain, swelling, a flattening of the arch and an inward rolling of the ankle. As the condition progresses, the symptoms will change.
For example, when posterior tibial tendon dysfunctioninitially develops, there is pain on the inside of the foot and ankle (along the course of the tendon). In addition, the area may be red, warm and swollen.
Later, as the arch begins to flatten, there may still be pain on the inside of the foot and ankle. But at this point, the foot and toes begin to turn outward and the ankle rolls inward.
As posterior tibial tendon dysfunction becomes more advanced, the arch flattens even more and the pain often shifts to the outside of the foot, below the ankle. The tendon has deteriorated considerably, and arthritis often develops in the foot. In more severe cases, arthritis may also develop in the ankle.
Nonsurgical Treatment of Posterior tibial tendonitis
Because of the progressive nature of posterior tibial tendon dysfunction, early treatment is advised. If treated early enough, your symptoms may resolve without the need for surgery, and progression of your condition can be arrested.
In contrast, untreated posterior tibial tendon dysfunction could leave you with an extremely flat foot, painful arthritis in the foot and ankle and increasing limitations on walking, running or other activities.
In many cases of posterior tibial tendon dysfunction, treatment can begin with nonsurgical approaches that may include:
- Orthotic devices or bracing. To give your arch the support it needs, your foot and ankle surgeon may provide you with an ankle brace or a custom orthotic device that fits into the shoe.
- Immobilization. Sometimes a short-leg cast or boot is worn to immobilize the foot and allow the tendon to heal, or you may need to completely avoid all weightbearing for a while.
- Physical therapy. Ultrasound therapy and exercises may help rehabilitate the tendon and muscle following immobilization.
- Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation.
- Shoe modifications. Your foot and ankle surgeon may advise changes to your shoes and may provide special inserts designed to improve arch support.
When Is Surgery Needed ?
In cases of posterior tibial tendon dysfunction that have progressed substantially or have failed to improve with nonsurgical treatment, surgery may be required. For some advanced cases, surgery may be the only option. Your foot and ankle surgeon will determine the best approach for you.
Foot Tendonitis
Achilles (calcaneal) tendinitis occurs when the tendon that connects the back of your leg to your heel becomes swollen and painful near the bottom of the foot. This tendon is called the Achilles tendon. It allows you to push your foot down. You use your Achilles tendon when walking, running, and jumping.
Achilles tendinitis is a common condition that causes pain along the back of the leg near the heel.
Types of foot (Achilles) tendinitis
Noninsertional Achilles Tendinitis
- In noninsertional Achilles tendinitis, fibers in the middle portion of the tendon have begun to break down with tiny tears (degenerate), swell, and thicken.
- Tendinitis of the middle portion of the tendon more commonly affects younger, active people.
Insertional Achilles Tendinitis
- Insertional Achilles tendinitis involves the lower portion of the heel, where the tendon attaches (inserts) to the heel bone.
In both noninsertional and insertional Achilles tendinitis, damaged tendon fibers may also calcify (harden). Bone spurs (extra bone growth) often form with insertional Achilles tendinitis.
Tendinitis that affects the insertion of the tendon can occur at any time, even in patients who are not active.
Causes of foot tendonitis
There are two large muscles in the calf. These create the power needed to push off with the foot or go up on the toes. The large Achilles tendon connects these muscles to the heel.
Heel pain is most often due to overuse of the foot – from repetitive stress to the tendon. Rarely, it is caused by an injury.
Tendinitis due to overuse is most common in younger people. It can occur in walkers, runners, or other athletes.
This often happens when you push your bodies to do too much, too soon, but other factors can make it more likely to develop tendinitis, including 10:
- There is a sudden increase in the amount or intensity of an activity.
- Your calf muscles are very tight (not stretched out). Having tight calf muscles and suddenly starting an aggressive exercise program can put extra stress on the Achilles tendon.
- Bone spur—Extra bone growth where the Achilles tendon attaches to the heel bone can rub against the tendon and cause pain.
- You run on hard surfaces, such as concrete.
- You run too often.
- You jump a lot (such as when playing basketball).
- You DO NOT wear shoes that give your feet proper support.
- Your foot suddenly turns in or out.
Tendinitis from arthritis is more common in middle-aged and older adults. A bone spur or growth may form in the back of the heel bone. This may irritate the Achilles tendon and cause pain and swelling. Flat feet will put more tension on the tendon.
Prevention foot tendonitis
Exercises to keep your calf muscles strong and flexible will help reduce the risk of tendinitis. Overusing a weak or tight Achilles tendon makes you more likely to develop tendinitis.
Symptoms of foot tendonitis
Common symptoms of Achilles tendinitis include:
- Pain in the heel and along the length of the calcaneal (Achilles) tendon when walking or running.
- Pain and stiffness along the Achilles tendon in the morning.
- Severe pain the day afer exercising.
- The tendon may be painful to touch or move.
- Thickening of the tendon.
- The area may be swollen and warm.
- You may have trouble standing up on one toe.
- Swelling that is present all the time and gets worse throughout the day with activity.
Achilles tendinitis diagnosis
The health care provider will perform a physical exam. They will look for tenderness along the tendon and pain in the area of the tendon when you stand on your toes.
X-rays can help diagnose bone problems.
An MRI of the foot scan may be done if you are considering surgery or there is a chance that you have a tear in the Achilles tendon.
Treatment of foot tendonitis
The main treatments for Achilles tendinitis DO NOT involve surgery 11. It is important to remember that it may take at least 2 to 3 months for the pain to go away.
Try putting ice on the Achilles tendon area for 15 to 20 minutes, 2 to 3 times per day. Remove the ice if the area gets numb.
Changes in activity may help manage the symptoms:
- Decrease or stop any activity that causes pain.
- Run or walk on smoother and softer surfaces.
- Switch to biking, swimming, or other activities that put less stress on the Achilles tendon.
Your provider or physical therapist can show you stretching exercises for the Achilles tendon.
You may also need to make changes in your footwear, such as:
- Using a brace, boot or cast to keep the heel and tendon still and allow the swelling to go down
- Placing heel lifts in the shoe under the heel
- Wearing shoes that are softer in the areas over and under the heel cushion
Nonsteroidal anti-inflammatory drugs (NSAIDs), such as aspirin and ibuprofen, can help ease pain or swelling.
If these treatments DO NOT improve symptoms, you may need surgery to remove inflamed tissue and abnormal areas of the tendon. If there is a bone spur irritating the tendon, surgery can be used to remove the spur.
Extracorporeal shock wave therapy may be an alternative to surgery for people who have not responded to other treatments 12. This treatment uses low-dose sound waves. Extracorporeal shock wave therapy has not shown consistent results and therefore, is not commonly performed. However, because of the minimal risk involved, extracorporeal shock wave therapy is sometimes tried before surgery is considered.
Exercise
The following exercise can help to strengthen the calf muscles and reduce stress on the Achilles tendon.
- Calf stretch: Lean forward against a wall with one knee straight and the heel on the ground. Place the other leg in front, with the knee bent. To stretch the calf muscles and the heel cord, push your hips toward the wall in a controlled fashion. Hold the position for 10 seconds and relax. Repeat this exercise 20 times for each foot. A strong pull in the calf should be felt during the stretch.
- Eccentric Strengthening Protocol 13. Eccentric strengthening is defined as contracting (tightening) a muscle while it is getting longer. Eccentric strengthening exercises can cause damage to the Achilles tendon if they are not done correctly. At first, they should be performed under the supervision of a physical therapist. Once mastered with a therapist, the exercises can then be done at home. These exercises may cause some discomfort, however, it should not be unbearable.
- Frequency: Three sets of 15 exercises, twice daily (total of 90 repetitions).
- Progression: Use same weight for first 1 to 2 weeks to achieve relative comfort with recommended daily frequency, then add weight (e.g., loaded backpacks, weighted vests) as comfort allows.
- Duration: Typical regimens last 12 weeks. Goal is a return to pain-free function with provocative activities, such as running.
Figure 8. Eccentric exercises for Achilles tendinitis
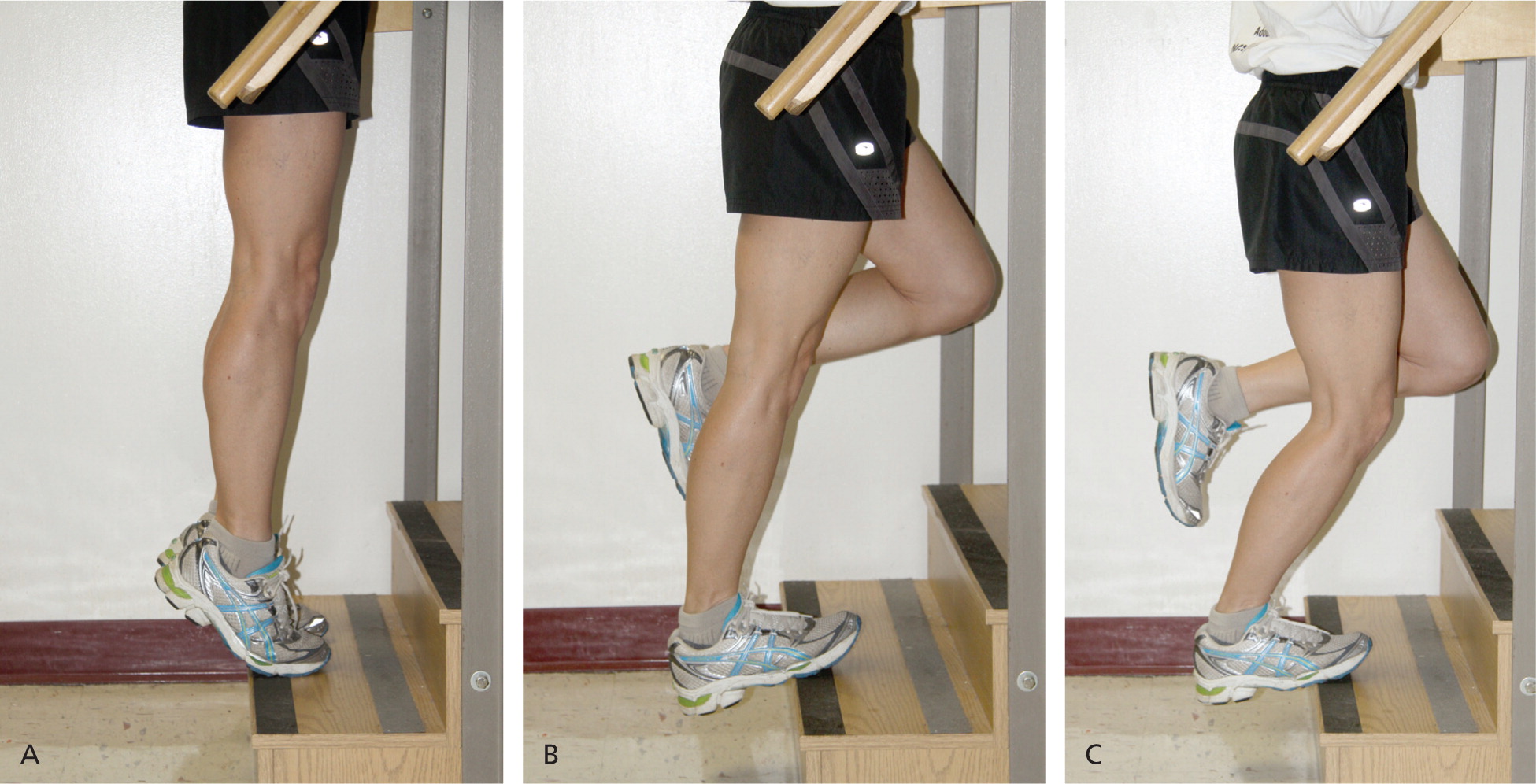
Note: (A) Patients begin with a straight leg and the ankle in flexion. (B) The ankle of the injured leg is then lowered to full dorsiflexion and returned to its original position with the assistance of the uninjured leg. (C) The exercise is repeated with the knee bent to approximately 45 degrees.
[Source 14]Supportive shoes and orthotics
Pain from insertional Achilles tendinitis is often helped by certain shoes, as well as orthotic devices. For example, shoes that are softer at the back of the heel can reduce irritation of the tendon. In addition, heel lifts can take some strain off the tendon.
Heel lifts are also very helpful for patients with insertional tendinitis because they can move the heel away from the back of the shoe, where rubbing can occur. They also take some strain off the tendon. Like a heel lift, a silicone Achilles sleeve can reduce irritation from the back of a shoe.
If your pain is severe, your doctor may recommend a walking boot for a short time. This gives the tendon a chance to rest before any therapy is begun. Extended use of a boot is discouraged, though, because it can weaken your calf muscle.
Surgical Treatment
Surgery should be considered to relieve Achilles tendinitis only if the pain does not improve after 6 months of nonsurgical treatment. The specific type of surgery
depends on the location of the tendinitis and the amount of damage to the tendon.
Gastrocnemius recession
This is a surgical lengthening of the calf (gastrocnemius) muscles. Because tight calf muscles place increased stress on the Achilles tendon, this procedure is useful for patients who still have difficulty flexing their feet, despite consistent stretching.
In gastrocnemius recession, one of the two muscles that make up the calf is lengthened to increase the motion of the ankle. The procedure can be performed with a traditional, open incision or with a smaller incision and an endoscope—an instrument that contains a small camera. Your doctor will discuss the procedure that best meets your needs. Complication rates for gastrocnemius recession are low, but can include nerve damage.
Gastrocnemius recession can be performed with or without débridement, which is removal of damaged tissue.
Debridement and repair (tendon has less than 50% damage)
The goal of this operation is to remove the damaged part of the Achilles tendon. Once the unhealthy portion of the tendon has been removed, the remaining tendon is repaired with sutures, or stitches to complete the repair.
In insertional tendinitis, the bone spur is also removed. Repair of the tendon in these instances may require the use of metal or plastic anchors to help hold the Achilles tendon to the heel bone, where it attaches. After débridement and repair, most patients are allowed to walk in a removable boot or cast within 2 weeks, although this period depends upon the amount of damage to the tendon.
Debridement with tendon transfer (tendon has greater than 50% damage)
In cases where more than 50% of the Achilles tendon is not healthy and requires removal, the remaining portion of the tendon is not strong enough to function alone. To prevent the remaining tendon from rupturing with activity, an Achilles tendon transfer is performed. The tendon that helps the big toe point down is moved to the heel bone to add strength to the damaged tendon. Although this sounds severe, the big toe will still be able to move, and most patients will not notice a change in the way they walk or run.
Depending on the extent of damage to the tendon, some patients may not be able to return to competitive sports or running.
Recovery after surgery
Most patients have good results from surgery. The main factor in surgical recovery is the amount of damage to the tendon. The greater the amount of tendon involved, the longer the recovery period, and the less likely a patient will be able to return to sports activity.
Physical therapy is an important part of recovery. Many patients require 12 months of rehabilitation before they are pain-free.
Complications after surgery
Moderate to severe pain after surgery is noted in 20% to 30% of patients and is the most common complication. In addition, a wound infection can occur and the infection is very difficult to treat in this location.
Outlook (Prognosis) for foot tendonitis
In most cases, lifestyle changes help improve symptoms. Keep in mind that symptoms may return if you DO NOT limit activities that cause pain, or if you DO NOT maintain the strength and flexibility of the tendon.
Possible Complications of foot tendonitis
Achilles tendinitis may make you more likely to have an Achilles rupture. This condition most often causes a sharp pain that feels as if you have been hit in the back of the heel with a stick. Surgical repair is necessary. However, the surgery may not be as successful as usual because there is already damage to the tendon.
- Tendinitis. Medline Plus. https://medlineplus.gov/tendinitis.html[↩]
- Tendinitis (Bursitis). American College of Rheumatology. https://www.rheumatology.org/I-Am-A/Patient-Caregiver/Diseases-Conditions/Tendinitis-Bursitis[↩]
- Joint and Soft Tissue Injection. Am Fam Physician. 2002 Jul 15;66(2):283-289. http://www.aafp.org/afp/2002/0715/p283.html[↩]
- Shoulder Impingement/Rotator Cuff Tendinitis. http://orthoinfo.aaos.org/PDFs/A00032.pdf[↩]
- Tennis Elbow (Lateral Epicondylitis). http://orthoinfo.aaos.org/PDFs/A00068.pdf[↩]
- Proximal Biceps Tendonitis. https://kidshealth.org/en/teens/biceps-tendonitis.html[↩]
- De Quervain’s Tendinosis. http://orthoinfo.aaos.org/PDFs/A00007.pdf[↩]
- de Quervain’s Tenosynovitis. American Academy of Family Physicians. https://familydoctor.org/condition/de-quervains-tenosynovitis[↩]
- Jumper’s Knee. https://kidshealth.org/en/teens/jumpers-knee.html[↩]
- Irwin TA. Tendon injuries of the foot and ankle. In: Miller MD, Thompson SR, eds. DeLee and Drez’s Orthopaedic Sports Medicine. 4th ed. Philadelphia, PA: Elsevier Saunders; 2015:chap 117.[↩]
- Biundo JJ. Bursitis, tendinitis, and other periarticular disorders and sports medicine. In: Goldman L, Schafer AI, eds. Goldman-Cecil Medicine. 25th ed. Philadelphia, PA: Elsevier Saunders; 2016:chap 263.[↩]
- Yin MC, Ye J, Yao M, et al. Is extracorporeal shock wave therapy clinical efficacy for relief of chronic, recalcitrant plantar fasciitis? A systematic review and meta-analysis of randomized placebo or active-treatment controlled trials. Arch Phys Med Rehabil. 2014;95(8):1585-1593. PMID: 24662810 www.ncbi.nlm.nih.gov/pubmed/24662810[↩]
- Alfredson H, Pietilä T, Jonsson P, Lorentzon R. Heavy-load eccentric calf muscle training for the treatment of chronic Achilles tendinosis. Am J Sports Med. 1998;26(3):360–366.[↩]
- Management of Chronic Tendon Injuries. Am Fam Physician. 2013 Apr 1;87(7):486-490. www.aafp.org/afp/2013/0401/p486.html[↩]





{kind=link}