
Thumb hypoplasia
Thumb hypoplasia also commonly called hypoplastic thumb, is the medical term for missing or underdeveloped thumbs. Thumb aplasia means that your child’s thumb is missing altogether. Thumb hypoplasia is a congenital condition, which means your child is born with this condition. Thumb hypoplasia is a rare congenital deformity that constitutes 3.5% of all upper limb congenital deformities 1. Thumb hypoplasia is a rare condition and occurs in about 1 in 100,000 infants. It is equally common in males and females. In approximately 60 percent of patients with thumb hypoplasia, both thumbs are affected. In some cases, a child’s other fingers may also be missing or underdeveloped.
The degree to which your child’s thumb is underdeveloped can vary; it may only be slightly smaller in size than normal, or missing entirely (a condition known as thumb aplasia).
Thumb hypoplasia key points:
- Your child’s thumb is slightly smaller than normal, but all of its structures — the bones, tendons, ligaments, muscles, and joints — are normal.
- Your child’s thumb is small and there are often minor abnormalities in the tendons and muscles within the thumb.
- The middle joint of the thumb is unstable, causing the thumb to wobble. The web space between the thumb and index finger is tight and restricts movement.
- The bones of your child’s thumb are abnormally small.
- There are abnormalities in many of the thumb’s muscles along with a range of problems in the joints of the thumb and an abnormal tight web space between the thumb and index finger.
- Your child’s thumb is “floating” with no bony support and is attached to the hand by only skin and soft tissue.
- Your child’s thumb is missing.
- Thumb hypoplasia is rare, occurring in about 1 out of every 100,000 babies.
- Thumb hypoplasia can occur by itself or may be associated with other conditions where the radial side (thumb side) of the forearm does not develop properly. These include Holt-Oram and Fanconi syndromes. And also routinely seen with radial longitudinal deficiency.
Thumb hypoplasia classification
Thumb hypoplasia was originally classified by Blauth 2 and subsequently modified by Buck-Gramko 3 and Manske et al 4 (see Table 1 below) and finally by Tonkin in 2013 (Figure 1) who added subgrades such as 2C 5. Thumb hypoplasia classification system is dependent on the degree of hypoplasia, ranging from a slightly smaller thumb to a completely absent thumb. The modification proposed by Manske et al 4 divides grade 3 based on the stability of the thumb carpometacarpal (CMC) joint. The modified classification provides surgeons guidance with regards to treatment of these underdeveloped thumbs. While some surgeons may choose to reconstruct all forms of hypoplastic thumbs, most Western surgeons utilize the classification and reconstruct thumbs type 2 and 3A, and choose pollicization for grades 3B, 4, and 5 thumbs.
Figure 1. Thumb hypoplasia classification (Tonkin classification)
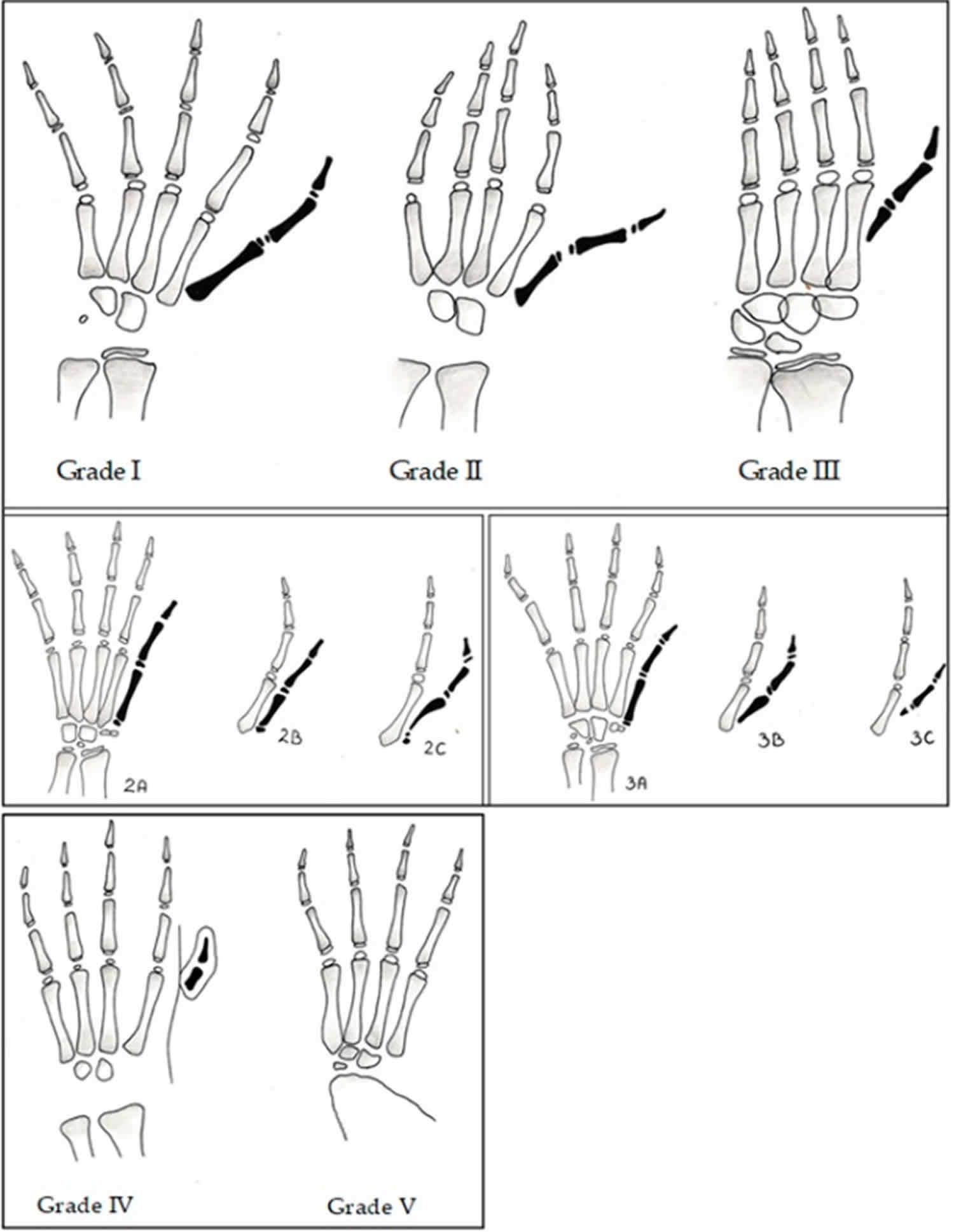
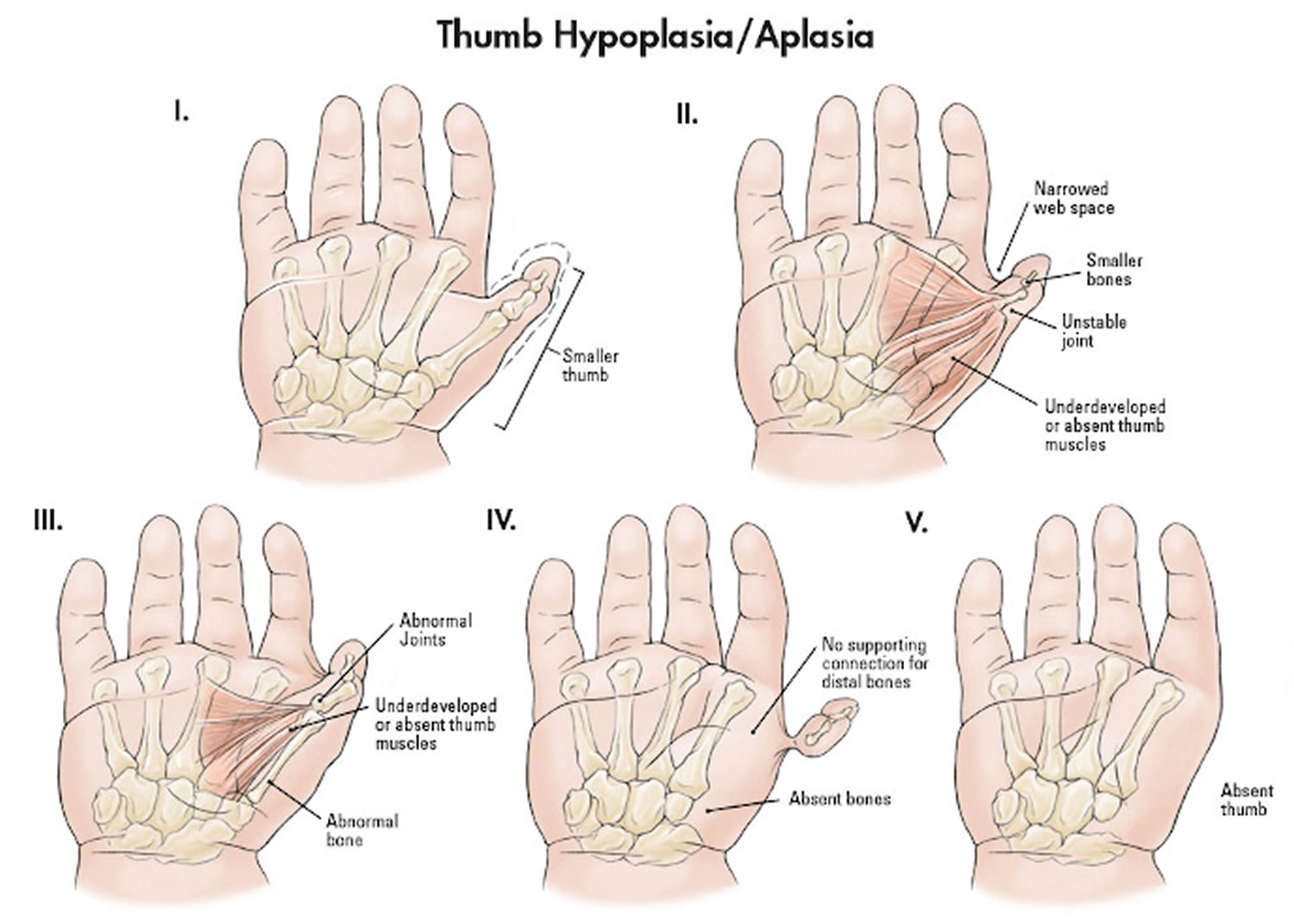
Table 1. Thumb hypoplasia classification of Blauth as modified by Manske
| Thumb hypoplasia classification | |
|---|---|
| Type 1 | Slightly small thumb |
| Type 2 | Small thumb with Narrow first web space Unstable carpometacarpal joint Deficient thenar musculature |
| Type 3a | Type 2 with Extrinsic tendon abnormalities Metacarpal hypoplasia Stable carpometacarpal joint |
| Type 3b | Type 2 with Extrinsic tendon abnormalities Absent metacarpal base/ carpometacarpal instability |
| Type 4 | Floating thumb |
| Type 5 | Absent thumb |
Thumb hypoplasia causes
The cause of thumb hypoplasia is unknown, but the condition has been associated with several genetic syndromes and conditions including:
- VATER syndrome, a group of birth defects that affect five different areas in which a child may have abnormalities: vertebrae, anus, trachea, esophagus and renal (kidneys)
- TAR syndrome, which is characterized by the absence of the radius bone in the forearm and extremely reduced platelet count
- Holt-Oram syndrome, often called hand-heart syndrome, which includes abnormalities of hands and arms, as well as cardiac defects
- Fanconi’s anemia, which is a rare blood disorder that affects many parts of the body.
Thumb hypoplasia symptoms
Because of the reduced functionality of your child’s thumb, they may have some problems with using their hand.
Children will adapt and can function without a missing finger. Children who have no use of a thumb will learn to rely on a lateral pinch between the long and index fingers. However, they may have problems with fine motor activities such as pinching and grasping. It is these children who may require surgery to correct the problem.
Thumb hypoplasia diagnosis
In most cases, thumb hypoplasia is identified after birth. In some cases, thumb hypoplasia is diagnosed before birth during an ultrasound.
In order to determine the best course of treatment for your child’s thumb hypoplasia, doctors may:
- Conduct a thorough physical exam of your child and take a family medical history
- Use imaging techniques like X-rays to look at the underlying structure of your child’s hands
- Recommend genetic testing and imaging of other parts of the body to identify related genetic syndromes and conditions
- Recommend a cardiac echocardiogram if a heart murmur is detected
- Recommend a renal ultrasound if a genetic anomaly is suspected
Thumb hypoplasia treatment
The thumb is a very important part of the hand: it accounts for about 40 percent of the hand’s function. This is why surgery to reconstruct a small thumb or create a thumb if one is missing entirely is usually the recommended treatment for thumb hypoplasia.
Your child will be examined by one of our pediatric hand and arm specialists to determine which surgery is best suited to her condition.
Thumb hypoplasia surgery
Surgical treatment is required for grade 2 to 5 deformities.
When considering reconstruction for types 2 and 3A, there are 3 specific components to be considered:
- There is hypoplasia of the thumb muscles, intrinsics only in type 2 and extrinsic with intrinsic muscles in type 3.
- There is instability of the thumb metacarpophalangeal joint. The metacarpophalangeal joint instability must be addressed in order to provide stability for use and function of the thumb specifically with regards to pinch and grasp. This can be isolated to laxity of the ulnar collateral ligament or can be a global instability.
- The first webspace may be narrowed, requiring widening with a Z-plasty or dorsal transposition flap. This can be challenging to recognize in small hands and as a guide, in a normal hand the distance between the thumb and index metacarpal head should be the same as that of the index to small metacarpal head.
There are two commonly utilized tendon transfers to augment thumb function and strength in opposition, the Huber opposition transfer 6 and the flexor digitorum superficialis opposition transfer 7. Both techniques are effective in improving thumb function and each has specific advantages.
The Huber opposition transfer involves transfer of the abductor digiti minimi muscle from the ulnar border of the hand to the thumb. This muscle is a reliable transfer candidate; it is always present in radial longitudinal deficiency and there is little (if any) notable deficit once transferred. The abductor digiti minimi is rotated across the palm and augments thumb opposition and increases bulk in the thenar region, improving cosmesis of the hand. Also the transfer does not require the use of a pulley, which the flexor digitorum superficialis transfer necessitates. Unfortunately the muscle is short and has a very small tendon insertion. As a result, this muscle cannot be used to help stabilize the thumb metacarpophalangeal joint. Additional steps, such as imbrication of the ulnar collateral ligament and capsule of the metacarpophalangeal joint, must be performed to create stability of this joint. This is important because the pull of the Huber transfer on the abductor pollicis brevis insertion adds a further deforming force to the UCL and can worsen UCL instability if this is not addressed.
The flexor digitorum superficialis opposition transfer is the alternative to the Huber to improve hypoplastic thumb strength and function. This technique utilizes a flexor tendon from one of the ulnar digits, typically the ring finger or long finger, as a transfer to augment thumb strength. As with the abductor digiti minimi, the flexor digitorum superficialis is present in the ring finger and can be reliably harvested. There has been no documentation of decreased strength in the hand with this transfer. The flexor digitorum superficialis passes across the palm to the thumb. This technique does not augment the thenar eminence cosmetically, but the tendon length is beneficial because it allows for simultaneous reconstruction of the collateral ligament of the thumb metacarpophalangeal joint.
Reconstructive surgery for hypoplastic thumb
If your child’s hand has a carpometacarpal joint, which stabilizes the base of the thumb, your child may benefit from a surgery to rebuild the ligaments and fix the tendons of the thumb. This will allow the reconstructed thumb to function more normally.
Thumb reconstruction is typically performed as an outpatient procedure when your child is about a year old. Your child will go home the same day as the procedure. She will have a long arm cast for two weeks after surgery, then be in a splint for another two weeks. She may need to work with one of our hand therapists to maximize functionality of the reconstructed thumb.
Pollicization
If your child does not have a carpometacarpal joint, a surgeon will perform a pollicization. This surgery includes the amputation of the non-functional, unstable thumb and the construction of a useable thumb by moving the index finger to the thumb position.
This procedure is typically performed as an inpatient procedure when your child is about a year old. Your child will be spend one night in the hospital after this surgery and will be in a long arm cast for two weeks following the surgery.
After the cast is removed, your child’s hand will be placed in a splint and hand therapy will be started. In most cases, your child will need several months of hand therapy after surgery. The newly constructed thumb will never be as strong or have as much range of motion as a normal thumb, but this surgery will significantly increase the functionality of your child’s hand.
Pollicization may be followed by subsequent procedures to deepen the web space between the fingers or improve motion.
Figure 2. Thumb hypoplasia treated with pollicization
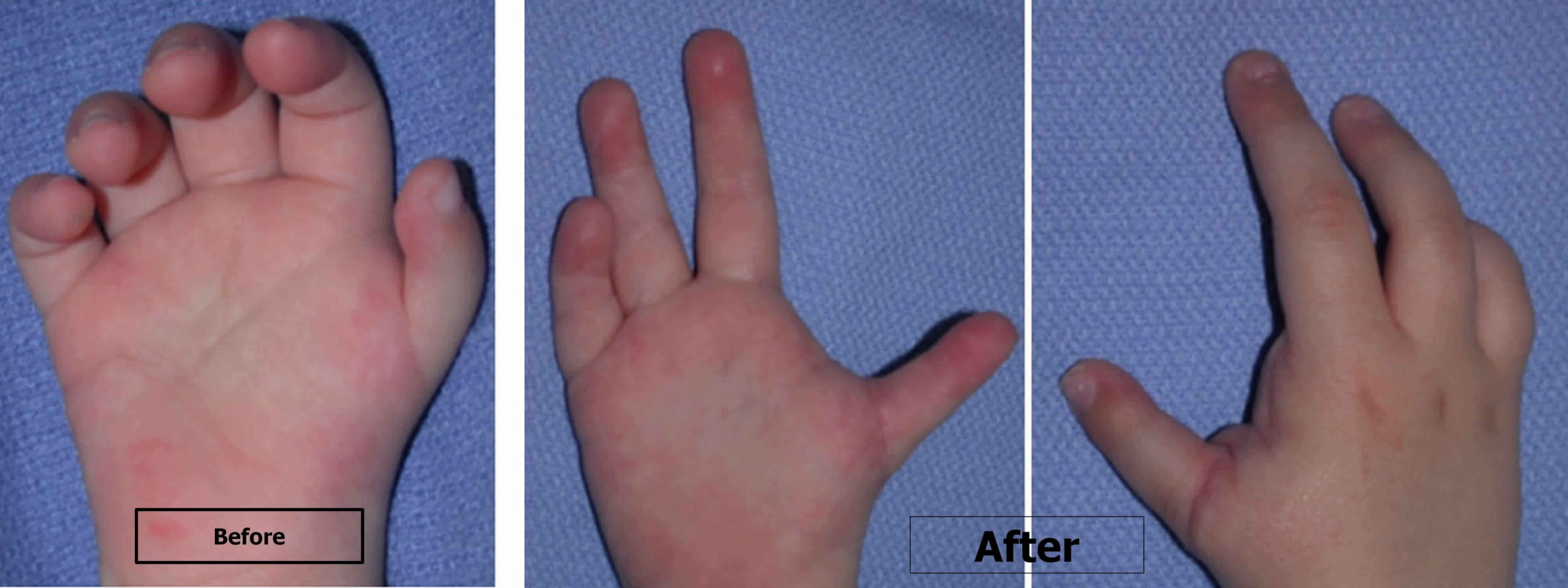
Footnote: Thumb hypoplasia before (left) and after (right) being treated with pollicization.
Follow-up care
Your child will need to be examined by the hand surgeon two weeks after surgery, and again at six weeks and three months postoperatively.
Your child will need hand therapy after surgery. The duration of therapy will depend on which surgery was performed and how much normal hand function your child has.
You can also expect to return to the hand surgeon for several annual visits throughout early childhood to ensure that your child is developing appropriate hand function as she develops skills such as writing and playing sports.
References- Ozols D, Butnere MM, Petersons A. Methods for Congenital Thumb Hypoplasia Reconstruction. A Review of the Outcomes for Ten Years of Surgical Treatment. Medicina (Kaunas). 2019;55(10):610. Published 2019 Sep 20. doi:10.3390/medicina55100610 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6843639
- Blauth W. Numerical variations. In: Schneider-Sickert F, editor. Congential Variations of the Hand. Springer Science & Business Media; Berlin, Germany: 1981. pp. 120–121.
- Buck-Gramcko D. Congenital malformations of the hand and forearm. Chir Main. 2002;21(2):70–101.
- Manske PR, McCarroll HR, Jr, James M. Type III—a hypoplastic thumb. J Hand Surg Am. 1995;20(2):246–253.
- Tonkin M.A. On the classification of congenital thumb hypoplasia. J. Hand Surg. 2014;39:948–955. doi: 10.1177/1753193413516246
- de Roode CP, James MA, McCarroll HR., Jr Abductor digit minimi opponensplasty: Technique, modifications, and measurement of opposition. Tech Hand Up Extrem Surg. 2010;14(1):51–3.
- Christen T, Dautel G. Type II and IIIA thumb hypoplasia reconstruction. J Hand Surg Am. 2013;38(10):2009–2015.





{kind=link}