
Toe walking causes
Toe walking is a gait abnormality characterized by an absence of normal heel-to-floor contact (heel strike) by both feet during gait. It is defined as the inability to make heel contact with the floor during the initial stance phase of the gait cycle and the absence of full foot contact with the ground during the remainder of the gait cycle. The forefoot engages in the majority of floor contact throughout the gait cycle. Walking on the toes or the ball of the foot, also known as toe walking, is fairly common in children who are just beginning to walk. It is generally understood that toe walking involves the absence or limitation of heel strike in the contact phase of the gait cycle 1. Toe walking has been acknowledged as a symptom of disease processes, trauma and/or neurogenic influences, and when there is no identifiable medical cause of the gait pattern, it is labelled idiopathic toe walking 2. The most commonly observed type of toe walking is idiopathic toe walking. Most children outgrow toe walking. Kids who continue toe walking beyond the toddler years often do so out of habit. As long as your child is growing and developing normally, toe walking on its own is unlikely to be a cause for concern. In most patients, tiptoe walking is idiopathic (Idiopathic Toe Walking) and will resolve over time, but in some patients the behavior is a sign of neuromuscular problems, schizophrenia, learning disorders, cerebral palsy, muscular dystrophy or another generalized disease of nerve and muscle. Children with autism also may walk on their toes or the balls of their feet, but many do not. It is estimated that toe walking not associated with medical condition, physical injury or neurological condition occurs in 7 to 24 % of the childhood population 3. Critical to the management of toe walking is the exclusion of neurologic or muscular diseases as a cause of the perceived gait abnormality.
Table 1. Known conditions associated with or causing toe walking
| Accidents causing fractures/soft tissue injuries 4 |
|---|
| Angelman syndrome 5 |
| Anklyosing spondlyitis 6 |
| Autistic spectrum disorders 7 |
| Cerebral Palsy 8 |
| Charcot-Marie-Tooth 9/Hereditary motor sensory neuropathy type 1A 10 |
| Congenital talipes equinus (clubfoot) 11 |
| Developmental Coordination Disorder (Previously known as Clumsy Child Syndrome) 11 |
| Global developmental delay 12 |
| Leg length discrepancy 13 |
| Muscular Dystrophy 14 |
| Puncture wounds 15 |
| Scarring from accidents or burns 16 |
| Childhood Schizophrenia 17 |
| Spina Bifida 18 |
| Tethered cord syndrome 19 |
| Transient focal dystonia of the lower leg muscles 20 |
| Tumor within the belly of the gastrocnemius muscle 21 |
| Venous malformation of the gastrocnemius muscle 22 |
If your child is still toe walking after the age of 2 years, talk to your doctor about it 23. Make an appointment sooner if the toe walking is accompanied by tight leg muscles, stiffness in the ankle’s Achilles tendon or a lack of muscle coordination.
Unilateral tiptoe walking is usually a result of leg length discrepancy, spastic hemiparesis, or Achilles tendinitis. Less often, it is associated with calf hemangioma, linear scleroderma, or conversion reaction.
Bilateral tiptoe walking also is typically idiopathic, but can be associated with spastic diplegia. Less common causes are peripheral neuropathy, muscular dystrophy, psychosis, learning disorders, and spinal cord anomaly.
Idiopathic toe walking
Idiopathic toe walking can only be diagnosed in the absence of any orthopedic, medical condition, physical injury or neurological condition known to cause tiptoe walking 24. The idiopathic toe walking always affects both feet. In publications of pediatric gait development, children’s ability to walk on their toes during the development of gait has been described as a natural and non-compulsory part of gait development 25. Typically, children begin to walk at the age of 12–15 months. During the early stages of walking, children generally experiment with different foot positions, including walking on their toes, as a part of their motor experiences. By the third year of life, children are expected to walk with a heel–toe gait pattern 26. If walking on their toes persists, it is perceived as idiopathic toe walking, which is defined as toe walking in a child who has been evaluated by a physician and for whom no medical reason for idiopathic toe walking has been identified. idiopathic toe walking occurs in healthy and normally developing children, and it always occurs in both feet.
Idiopathic toe walking has been defined as the failure of the heel to make contact with the floor at the onset of stance 27 or as the absence of a heel rocker. In a normal gait, the term “heel rocker” refers to the progression of the limb with the heel as the pivotal area of support 28. The rear of the foot contacts the floor and rolls into ankle plantar flexion. Without a heel rocker phase, either the midfoot or forefoot touches the floor or the ankle moves toward ankle dorsiflexion.
Many authors have described the gait patterns of children with idiopathic toe walking based on a three-dimensional gait analysis. A classification system for the severity of idiopathic toe walking is based on ankle kinematic and kinetic data and comprises the presence of a first rocker, the presence of an early third rocker, and an early predominant first ankle moment 29. This classification includes three types: type 1 (mild), type 2 (moderate), and type 3 (severe) 29.
Idiopathic toe walking is not the result of initial Achilles’ tendon (heel cord) tightness; however, a tight Achilles’ tendon may sometimes develop as a child grows, in which case the phenomenon is called a contracture. When this type of contracture occurs, children can no longer drop their heels to the ground. This situation can lead to complications with their foot and leg positions and can contribute to flat arches and/or outward-rotated leg development when the child tries to maintain heel contact with the ground.
The cause of idiopathic toe walking is not fully known. However, among the factors that could lead to idiopathic toe walking, the following are noteworthy: tactile processing (an increased response to touch sensations), altered proprioceptive processing (sensing the body’s position in space), altered vestibular processing (maintaining balance), visual processing, decreased flexibility of the leg and foot muscles, reduced overall body strength, and family history (parents or siblings with a history of toe walking) 30.
The incidence of idiopathic toe walking has been reported to be present in up to 7% of the general pediatric population in some small studies 31, 32. However, owing to a small sample and variance in cultural influences, it may be presumed that there is no agreement on the true prevalence of idiopathic toe walking. The incidence of family members reporting an idiopathic toe walking history, according to a number of retrospective studies, is between 10-88% with the only prospective study reporting an incidence of 34.1% 33. It is also noted that having family members who have displayed idiopathic toe walking did not conclusively lead to further generations presenting with this gait type. There is strong agreement within the literature of a positive family history and no single sex dominance for children who have an idiopathic toe walking gait 32, 34. A link between speech delay, with or without a gross motor skill delay, and idiopathic toe walking has been identified in a number of studies 35, 36. There is an absence of research into the habitual nature of idiopathic toe walking or the social or familial influences of this gait style and no literature on any influential factors contributing to the initial development of this gait pattern.
Idiopathic toe walking and its relationship to equinus have been discussed in the literature. The suggestion that equinus is secondary to the development of this gait abnormality is common, yet unproven 37. Equinus is a condition in which the upward bending motion of the ankle joint is limited. Someone with equinus lacks the flexibility to bring the top of the foot toward the front of the leg. Equinus can occur in one or both feet. When it involves both feet, the limitation of motion is sometimes worse in one foot than in the other. The effectiveness of equinus treatment has been the focus of several studies in children with an idiopathic toe walking gait. The presence of idiopathic toe walking into adolescence and beyond has now been highlighted both in long-term case-controlled studies and within case reports leading to conflicting opinions on the necessity of treatment.7 8 The long-term effect idiopathic toe walking has on the foot and ankle has not been definitively established; however, there is prolific research of equinus and its negative impact on the foot and its function as well as changes in gait in adults and the elderly 38. There is limited research on many of the conservative treatment options for idiopathic toe walking including orthotics 39 and footwear 40. These treatment options have only been reported within case studies or author opinion pieces and it is not fully understood how these treatment options are thought to minimize the toe walking gait. Studies in normal gait and the pediatric foot have found that footwear provides a tactile input that may change the neurological input, which may in turn change the gait pattern. Footwear also has a mechanical influence at the foot which affects stride length 41 and motion of the subtala, midtarsal and ankle joint 42 and may also change the toe walking pattern. The full-length carbon fiber orthotic may have a mechanical and inhibitory action on the gait pattern, but this is yet to be established. Currently, serial casting 43, Botulinum toxin type A (BoNT-A) 44 and surgical Achilles tendon lengthening 45 have the best evidence for improved outcomes in the short-term and long-term.
Complications for surgical Achilles tendon lengthening procedures are not limited to, but can include, postoperative infection, tendon necrosis, deep vein thrombosis or sensory loss 46. While serial casting runs the risk of skin irritation, pressure wounds and permanent tissue damage 47, this is less likely to occur in healthy and normally sensate children. In recommended doses, botulinum neurotoxin-A (BoNT-A) is very safe with a very low complication rate. There have been reports of local complications, including pain at the injection site and local muscle weakness, which is a direct effect of the botulinum neurotoxin-A (BoNT-A) and when it occurs, it is always temporary, lasting up to a few weeks. Systemic complications may also include a short-lived ‘flu-like illness which may last 2–3 days. In larger doses, regional complications may occur such as bladder incontinence when upper leg injections are performed and swallowing difficulties when proximal upper limb or neck injections are performed. In children with severe cerebral palsy, there have been a small number of deaths worldwide associated with injections of large doses of botulinum neurotoxin-A (BoNT-A) given under general anesthetic. The cause of these deaths is not clear 48. Each of these treatments has a greater potential for complications that may impact the child’s function in the short-term or long-term compared with conservative measures such as a change in footwear and/or orthotic therapy.
Figure 1. Tone-inhibiting casts on a 5-year-old boy with severe idiopathic toe walking.

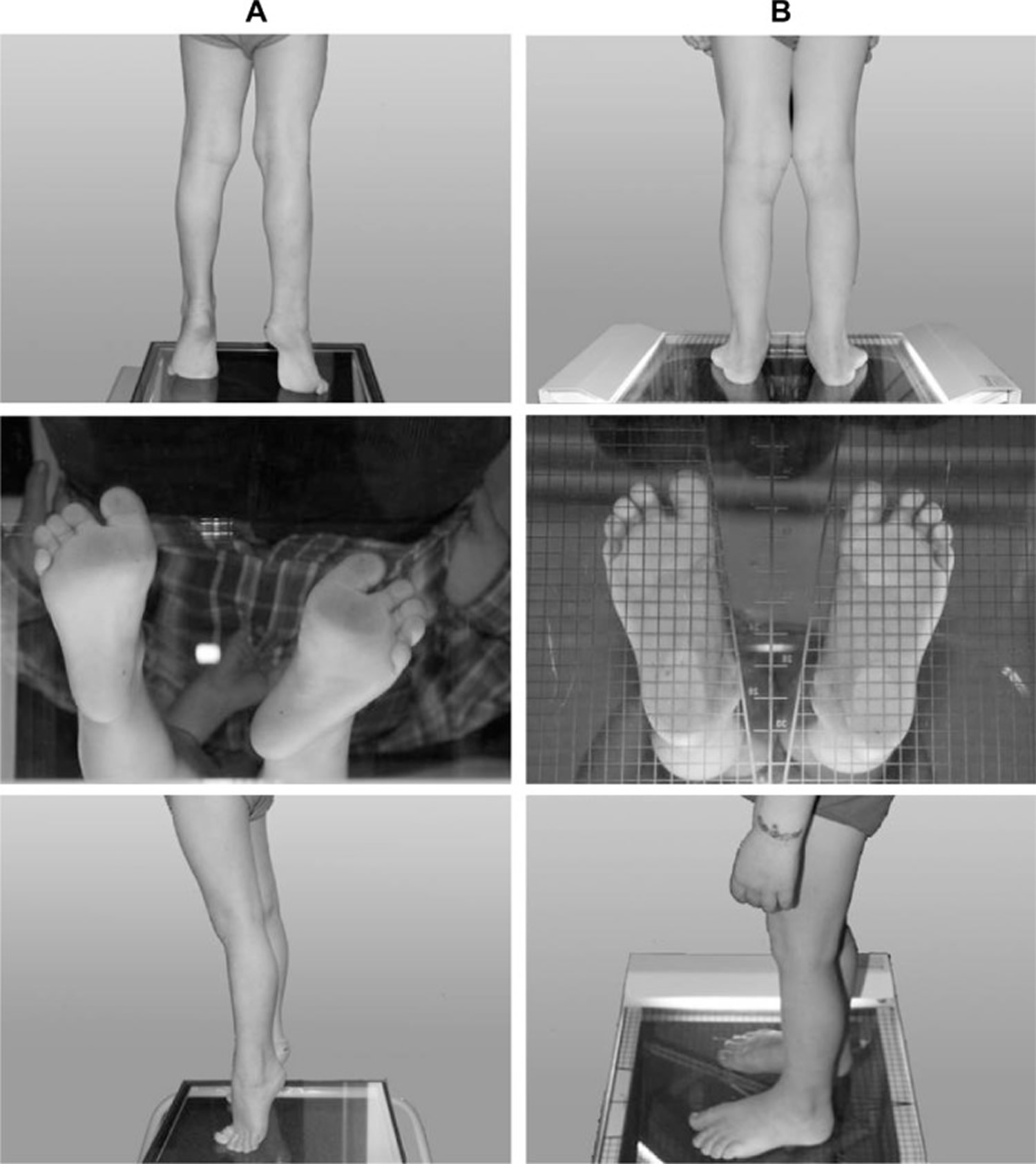
Figure 2. A 5-year-old boy with severe Idiopathic toe walking before tone-inhibiting cast treatment (A) and 3 months after cast removal (B).
There is limited evidence of conservative measures having a positive impact on idiopathic toe walking gait and no evidence to support the use of whole body vibration. Authors reporting the use of orthotics with or without specific footwear are anecdotal reports of author opinion 40 or have limited participant numbers within a case study8 of which has also not been published in peer reviewed media. Despite this, many clinicians report the use of full-length flat carbon devices or advise parents to purchase heavy shoes for their children.
The use of whole body vibration has been determined to have an immediate positive effect on gait in individuals with cerebral palsy 49. It is unknown what, if any, gait effect will be observed by the introduction of these external stimuli.
The treatment of idiopathic toe walking is complex due to the unknown etiology; therefore, it is necessary to have well-designed research investigating possible and feasible interventions.
There is no single treatment option proven to have a positive, long-term effect on idiopathic toe walking.
The natural history of idiopathic toe walking is not known. It appears clear that adults who were toe walkers do not continue to walk in the sever equinus (“ballet position”) that causes much of the concern in childhood. Anecdotally, adult toe walkers have a “bouncing” or “mincing” gait with less than normal heel contact during stance phase. Whether this results in any problems is unknown 50.
Toe walking causes
Typically, toe walking is simply a habit that develops when a child learns to walk – Idiopathic Toe Walking. In a few cases, toe walking is caused by an underlying condition, such as:
- A short Achilles tendon. This tendon links the lower leg muscles to the back of the heel bone. If it’s too short, it can prevent the heel from touching the ground.
- Cerebral palsy. Toe walking can be caused by cerebral palsy — a disorder of movement, muscle tone or posture that is caused by injury or abnormal development in the parts of the immature brain that control muscle function.
- Muscular dystrophy. Toe walking sometimes occurs in muscular dystrophy – such as Duchenne’s Muscular Dystrophy or Becker’s Muscular Dystrophy, a genetic disease in which muscle fibers are unusually susceptible to damage and weaken over time. This diagnosis may be more likely if your child initially walked normally before starting to toe walk.
- Autism. Toe walking has also been linked to autism, a complex spectrum of disorders that affect a child’s ability to communicate and interact with others.
- Pervasive Development Disorder.
- Peripheral neuropathy such as Charcot Marie Tooth
- Neuromuscular disorder such as Spinal Muscular Atrophy
- Tethered Spinal Cord Syndrome
- Congenital orthopedic condition such as Talipes Equinovarus (clubfoot)
Four basic questions can help in sorting out the differential diagnosis. These include:
When was the onset of tiptoe gait?
- Early onset tiptoe walking—defined as tiptoeing from initial ambulation or within 3 months of initial ambulation—usually is idiopathic or associated with spastic diplegic cerebral palsy.
- Late onset tiptoe walking—defined as tiptoeing which begins 4 or more months after a heel-toe gait has been established—usually indicates a neuromuscular problem such as Charcot-Marie-Tooth disease, Duchenne’s muscular dystrophy, or a spinal cord anomaly, and requires evaluation by a pediatric neurologist.
Is there a family history of toe walking?
Tiptoe walking is idiopathic in about 40% of children with a family history of tiptoe walkers, but it is important to obtain a family history because this can help in diagnosing Charcot-Marie-Tooth disease, Duchenne’s muscular dystrophy, or a psychiatric disorder. For example, if a parent has schizophrenia, a psychiatric evaluation of the child is warranted.
Is the neurologic examination abnormal?
An abnormal neurologic examination can help sort out the finer details of the cause of tiptoe walking in a child with a neuromuscular basis for the behavior.
Is there Achilles contracture?
A normal child should have 10 degrees of dorsal flexion. Proper measurement of dorsal flexion requires that the knee be extended, and the midfoot stabilized using the thumb (allowing midfoot pronation will falsely add 5-10 degrees of dorsal flexion). If you are unable to flex the ankle to neutral in this position, the Achilles tendon is tight.
Consider referring children older than age 2 years with tiptoe walking for evaluation by a neurologist, psychiatrist (particularly if there is a family history of psychiatric disorder), and orthopedist.
Risk factors for toe walking
Toe walking out of habit, also known as idiopathic toe walking, sometimes runs in families.
Toe walking complications
Persistent toe walking may increase a child’s risk of falling. It also can result in a social stigma if the child is perceived as “different” by peers.
Toe walking diagnosis
Toe walking can be observed during a physical exam. In some cases, the doctor may do an in-depth gait analysis or an exam known as electromyography (EMG). During an electromyography (EMG), a thin needle with an electrode is inserted into a muscle in the leg. The electrode measures the electrical activity in the affected nerve or muscle.
If the doctor suspects an underlying condition such as cerebral palsy or autism, he or she may recommend a neurological exam or testing for developmental delays.
How to stop toe walking
If your child is toe walking out of habit, treatment isn’t needed. He or she is likely to outgrow the habit. Your doctor may simply monitor your child’s gait during regular office visits.
If a physical problem is contributing to toe walking, treatment options may include:
- Physical therapy. Gentle stretching of the leg and foot muscles may improve your child’s gait.
- Leg braces or splints. Sometimes leg braces or splints help promote a normal gait.
- Serial casting. If physical therapy or leg braces aren’t helpful, your doctor may suggest trying a series of below-the-knee casts to progressively improve the ability to bring the toes toward the shin.
- Surgery. If conservative treatments fail, the doctor may recommend surgery to lengthen the muscles or tendons at the back of the lower leg.
If the toe walking is associated with cerebral palsy, autism or other problems, treatment focuses on the underlying condition.
Dynamic Achilles contracture
Dynamic Achilles Contracture is also known as overactive gastrocsoleus—might be managed with observation (idiopathic cases have been shown to resolve over time and to be clinically undetectable at 15-year follow-up); serial casting; botulinum toxin injections; gastroc recession (although studies have shown a 30% recurrence rate with this procedure); or bracing. This is true for both idiopathic cases and spastic diplegic cases with this type of contracture.
Static Achilles contracture
Static Achilles contracture is also known as tight gastrocsoleus—might be treated with gastroc recession or Achilles tendon lengthening in those with idiopathic and spastic diplegic tiptoe walking.
There are few data on treatment of psychiatric tiptoe walking, but generally this is treated the same as idiopathic tiptoe walking. Outcomes, however, are less predictable in these patients.
In those with Charcot-Marie-Tooth disease, treatments include ankle-foot orthosis splinting, plantar fasciotomy, tendon transfers, and foot osteotomies. In Duchenne’s muscular dystrophy, treatment may include ankle-foot orthosis splinting, or early surgery to lengthen the Achilles tendon or perform tendon transfer.
References- Williams CM, Tinley P, Curtin M. Idiopathic toe walking and sensory processing dysfunction. Journal of Foot and Ankle Research. 2010;3:16. doi:10.1186/1757-1146-3-16. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2933674/
- Williams CM, Michalitsis J, Murphy A, Rawicki B, Haines TP. Do external stimuli impact the gait of children with idiopathic toe walking? A study protocol for a within-subject randomised control trial. BMJ Open. 2013;3(3):e002389. doi:10.1136/bmjopen-2012-002389. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3612749/
- Sobel, E.; Caselli, M. A.; and Velez, Z.: Effect of persistent toe walking on ankle equinus. Analysis of 60 idiopathic toe walkers. J Am Podiatr Med Assoc, 87(1): 17-22, 1997, [4b]
- James A, Gilheany M. Paediatric Special Interest Group. Melbourne: Australian Podiatry Association; 2008. Case Study – Unilateral toe walking and talar dome lesions.
- Williams C, Philips RC, Wagstaff J. Facts about Angelman syndrome. Aurora, IL: Angelman Syndrom Foundation Inc. https://www.angelman.org/
- Reimer J, Altschuler EL. Unilateral predominant toe walking gait in a patient with ankylosing spondylitis. Am J Phys Med Rehabil. 2008;87:84. doi: 10.1097/PHM.0b013e31815e6b47. https://www.ncbi.nlm.nih.gov/pubmed/18158434
- Weber D. “Toe-walking” in children with early childhood autism. Acta Paedopsychiatr. 1978;43:73–83. https://www.ncbi.nlm.nih.gov/pubmed/345741
- Green LB, Hurvitz EA. Cerebral palsy. Phys Med Rehabil Clin N Am. 2007;18:859–882. https://www.ncbi.nlm.nih.gov/pubmed/17967366
- Newman CJ, Walsh M, O’Sullivan R, Jenkinson A, Bennett D, Lynch B, O’Brien T. The characteristics of gait in Charcot-Marie-Tooth disease types I and II. Gait Posture. 2007;26:120–127. doi: 10.1016/j.gaitpost.2006.08.006. https://www.ncbi.nlm.nih.gov/pubmed/17010610
- Herbertz S, Bernhard M, Heinritz W, C M, Syrbe S, A M. Toe walking and stumbling as first symptoms of a hereditary motor sensory neuropathy type 1A. Kinder- und Jugendmedizin. 2006;6:371–373
- Caselli MA, Rzonca EC, Lue BY. Habitual toe-walking: evaluation and approach to treatment. ClinPodiatr Med Surg. 1988;5:547–559. https://www.ncbi.nlm.nih.gov/pubmed/3293753
- Montgomery P, Gauger J. Sensory dysfunction in children that toe walk. Phys Ther. 1978;58:1195–1204. https://www.ncbi.nlm.nih.gov/pubmed/693578
- Song KM, Halliday SE, Little DG. The effect of limb-length discrepancy on gait. J Bone Joint Surg Am. 1997;79:1690–1698. doi: 10.1302/0301-620X.79B5.7615. https://www.ncbi.nlm.nih.gov/pubmed/9384429
- Emery AE. The muscular dystrophies. Lancet. 2002;359:687–695. doi: 10.1016/S0140-6736(02)07815-7. https://www.ncbi.nlm.nih.gov/pubmed/11879882
- Chudnofsky CR, Sebastian S. Special wounds. Nail bed, plantar puncture, and cartilage. Emerg Med Clin N Am. 1992;10:801–822. https://www.ncbi.nlm.nih.gov/pubmed/1358599
- Hahn SB, Park HJ, Park HW, Kang HJ, Cho JH. Treatment of severe equinus deformity associated with extensive scarring of the leg. Clin Orthop Relat R. 2001. pp. 250–257. https://www.ncbi.nlm.nih.gov/pubmed/11764356
- Colbert EG, Koegler RR. Toe walking in childhood schizophrenia. J Pediatr. 1958;53:219–220. doi: 10.1016/S0022-3476(58)80174-2. https://www.ncbi.nlm.nih.gov/pubmed/13564386
- Frischhut B, Stockl B, Landauer F, Krismer M, Menardi G. Foot deformities in adolescents and young adults with spina bifida. J Pediatr Orthop B. 2000;9:161–169. https://www.ncbi.nlm.nih.gov/pubmed/10904902
- Bachli H, Wasner M, Hefti F. [Intraspinal malformations. Tethered cord syndrome] Orthopade. 2002;31:44–50. doi: 10.1007/s132-002-8273-8. https://www.ncbi.nlm.nih.gov/pubmed/11963468
- Newman CJ, Ziegler AL, Jeannet PY, Roulet-Perez E, Deonna TW. Transient dystonic toe-walking: differentiation from cerebral palsy and a rare explanation for some unexplained cases of idiopathic toe-walking. Dev Med Child Neurol. 2006;48:96–102. doi: 10.1017/S0012162206000223. https://www.ncbi.nlm.nih.gov/pubmed/16417663
- Klemme WR, James P, Skinner SR. Latent onset unilateral toe-walking secondary to hemangioma of the gastrocnemius. J Pediatr Orthoped. 1994;14:773–775. https://www.ncbi.nlm.nih.gov/pubmed/7814593
- Domb BG, Khanna AJ, Mitchell SE, Frassica FJ. Toe-walking attributable to venous malformation of the calf muscle. Clin Orthop Relat R. 2004. pp. 225–229. https://www.ncbi.nlm.nih.gov/pubmed/15057102
- Pernet J, Billiaux A, Auvin S, Rakatovao D, Morin L, Presedo A. Early onset toe-walking in toddlers: a cause for concern?. J Pediatr. 2010 Sep. 157(3):496-8.
- Automated method to distinguish toe walking strides from normal strides in the gait of idiopathic toe walking children from heel accelerometry data. Gait & Posture March 2012, Volume 35, Issue 3, Pages 478–482
- Sutherland DH, Olshen RA, Biden EN, et al. The development of mature walking. Philadelphia: Mac Keith Press, 1988:151
- The development of mature gait. Sutherland DH, Olshen R, Cooper L, Woo SL.J Bone Joint Surg Am. 1980 Apr; 62(3):336-53. https://www.ncbi.nlm.nih.gov/pubmed/7364807/
- Perry J, Burnfield JM, Gronley JK, Mulroy SJ. Toe walking: muscular demands at the ankle and knee. Arch Phys Med Rehabil. 2003;84(1):7–16. https://www.ncbi.nlm.nih.gov/pubmed/12589614
- Perry J, Davids JR. Gait analysis normal and pathological function. J Pediatr Orthop. 1992;12(6):815.
- Armand S, Watelain E, Mercier M, Lensel G, Lepoutre FX. Identification and classification of toe-walkers based on ankle kinematics, using a data-mining method. Gait Posture. 2006;23(2):240–248. http://www.gaitposture.com/article/S0966-6362(05)00031-7/fulltext
- Williams CM, Tinley P, Curtin M. Idiopathic toe walking and sensory processing dysfunction. J Foot Ankle Res. 2010;3:16. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2933674/
- Bernhard MK, Merkenschlager A. Beeinflusst Barfußlaufen die Häufigkeit des idiopathischen Zehenspitzengangs? Unterschiede zwischen deutschen und bangalischen Kindern. Pädiatr Praxis 2008;72:301–5
- Fox A, Deakin S, Pettigrew G, et al. Serial casting in the treatment of idiopathic toe-walkers and review of the literature. Acta Orthop Belg 2006;72:722–30 https://www.ncbi.nlm.nih.gov/pubmed/17260610
- Fox A, Deakin S, Pettigrew G, Paton R. Serial casting in the treatment of idiopathic toe-walkers and review of the literature. Acta Orthop Belg. 2006;72:722–730. https://www.ncbi.nlm.nih.gov/pubmed/17260610
- Sobel E, Caselli MA, Velez Z. Effect of persistent toe walking on ankle equinus. Analysis of 60 idiopathic toe walkers. J Am Podiatr Med Assoc 1997;87:17–22 https://www.ncbi.nlm.nih.gov/pubmed/9009544
- Stricker SJ, Angulo JC. Idiopathic toe walking: a comparison of treatment methods. J Pediatr Orthoped. 1998;18:289–293. doi: 10.1097/00004694-199805000-00003. https://www.ncbi.nlm.nih.gov/pubmed/9600550
- Shulman LH, Sala DA, Chu MLY, McCaul PR, Sandler BJ. Developmental implications of idiopathic toe walking. J Pediatr. 1997;130:541–546. doi: 10.1016/S0022-3476(97)70236-1. https://www.ncbi.nlm.nih.gov/pubmed/9108850
- Stricker SJ, Angulo JC. Idiopathic toe walking: a comparison of treatment methods. J Pediatr Orthoped 1998;18:289–93 https://www.ncbi.nlm.nih.gov/pubmed/9600550
- Irving DB, Cook JL, Menz HB. Factors associated with chronic plantar heel pain: a systematic review. J Sci Med Sport 2006;9:11–22 https://www.ncbi.nlm.nih.gov/pubmed/16584917
- Pomarino D, Kuhl A, Kuhl F, et al. Case history and successful therapy of a toe walking 23-year old man. 2007;2008(12/12).
- Caselli MA. Habitual toe walking: learn to evaluate and treat this idiopathic childhood condition. Podiatry Manag 2002;Nov/Dec:163–74
- Lythgo N, Wilson C, Galea M. Basic gait and symmetry measures for primary school-aged children and young adults whilst walking barefoot and with shoes. Gait Posture 2009;30:502–6 https://www.ncbi.nlm.nih.gov/pubmed/19692245
- Wolf S, Simon J, Patikas D, et al. Foot motion in children shoes: a comparison of barefoot walking with shod walking in conventional and flexible shoes. Gait Posture 2008;27:51–9 https://www.ncbi.nlm.nih.gov/pubmed/17353125
- Brouwer B, Davidson LK, Olney SJ. Serial casting in idiopathic toe-walkers and children with spastic cerebral palsy. J Pediatr Orthop 2000;20:221–5 https://www.ncbi.nlm.nih.gov/pubmed/10739286
- Engstrom P, Gutierrez-Farewik EM, Bartonek A, et al. Does botulinum toxin A improve the walking pattern in children with idiopathic toe-walking? J Child Orth 2010;4:301–8 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2908341/
- Eastwood DM, Menelaus D, Dickens RV, et al. Idiopathic toe-walking: does treatment alter the natural history? J Pediatr Orthoped B 2000;9:47–9 https://www.ncbi.nlm.nih.gov/pubmed/10647110
- Lansdaal JR, Goslings JC, Reichart M, et al. The results of 163 Achilles tendon ruptures treated by a minimally invasive surgical technique and functional aftertreatment. Injury 2007;38:839–44 https://www.ncbi.nlm.nih.gov/pubmed/17316642
- Thornton H, Kilbride C. Physical management of abnormal tone and movement. In: Stokes M, editor. , eds. Physical management in neurological rehabilitation. 2nd edn London: Elsevier Health Sciences, 2004
- Davletov B, Bajohrs M, Binz T. Beyond BOTOX: advantages and limitations of individual botulinum neurotoxins. Trends Neurosci 2005;28:446–52
- Faust KA. The acute effect of whole body vibration on gait parameters in adults with cerebral palsy [Masters]. Indiana, IN: Ball State University, 2011 https://www.ncbi.nlm.nih.gov/pubmed/23445911
- Dietz F, Khunsree S. Idiopathic Toe Walking: To Treat or not to Treat, that is the Question. The Iowa Orthopaedic Journal. 2012;32:184-188. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3565400/





{kind=link}