
What is vulvodynia
Vulvodynia is chronic pain (lasting 3 months or longer) or discomfort of the vulva without an identifiable cause – not caused by an infection, skin disorder, or other medical condition 1, 2, 3. Vulvodynia is usually described as burning, stinging, irritation, or rawness. The location, constancy and severity of the pain vary among sufferers. Some women experience pain in only one area of the vulva, while others experience pain in multiple areas. The most commonly reported symptom is burning, but women’s descriptions of the pain vary. One woman reported her pain felt like “acid being poured on my skin,” while another described it as “constant knife-like pain.” Researchers and health care providers currently know little about why and how vulvodynia occurs—the condition and the pain have no known cause or cure 4. Therapies can help relieve symptoms of vulvodynia, but the condition can have some serious effects on women’s reproductive health and day-to-day life.
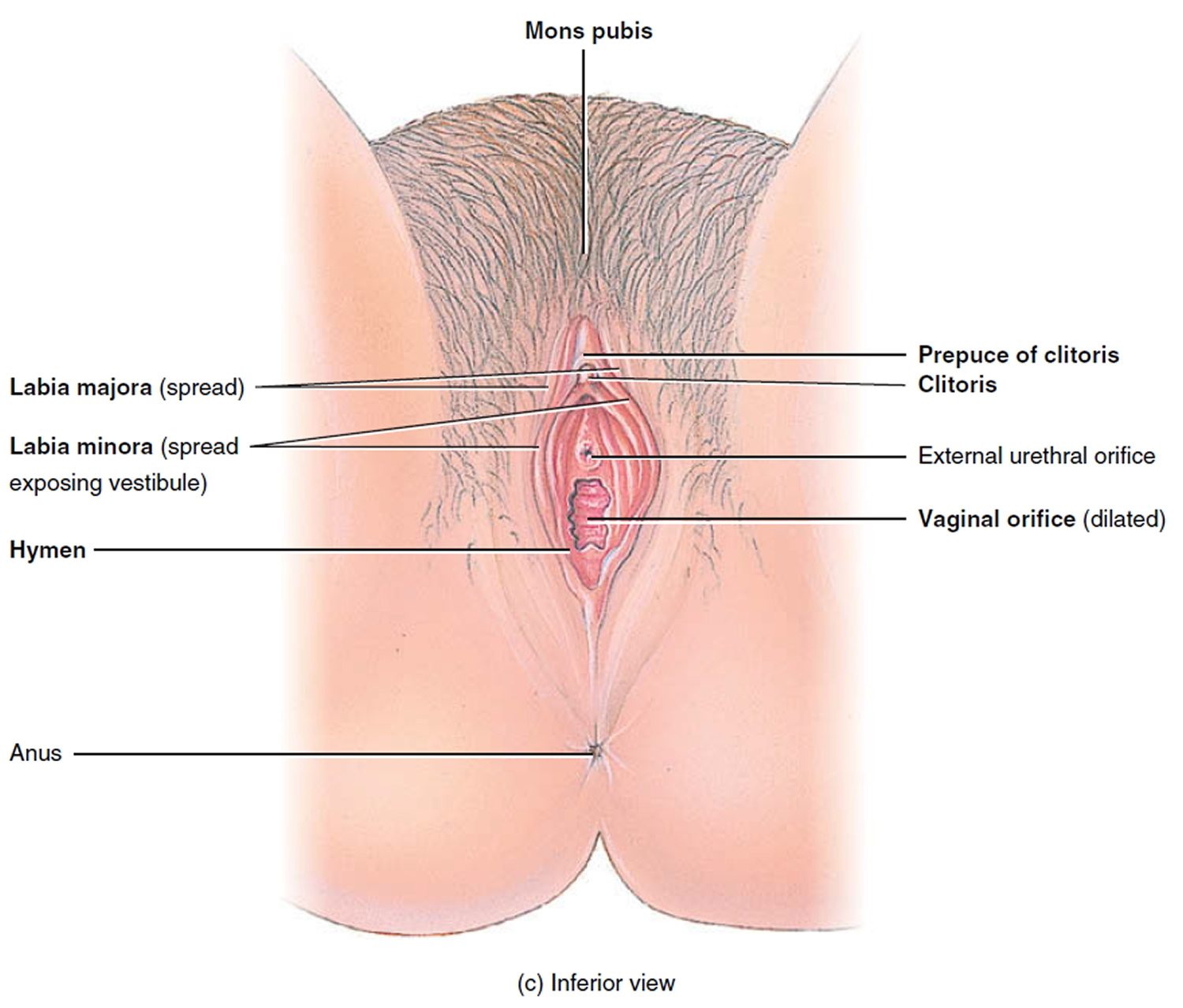
The vulva refers to the external female genitalia, including the labia (“lips” or folds of skin at the opening of the vagina), the clitoris, and the vaginal opening (see Figure 1).
The main vulvodynia symptom is pain in your genital area, which can be characterized as 5:
- Burning
- Soreness
- Stinging
- Rawness
- Painful intercourse (dyspareunia)
- Throbbing
- Itching
Your pain might be constant or occasional. It might occur only when the sensitive area is touched (provoked). You might feel the pain in your entire vulvar area (generalized), or the pain might be localized to a certain area, such as the opening of your vagina (vestibule).
Vulvar tissue might look slightly inflamed or swollen. More often, your vulva appears normal.
A similar condition, vestibulodynia also known as vulvar vestibulitis syndrome, causes pain only when pressure is applied to the area surrounding the entrance to your vagina (the vestibule, which is the tissue surrounding the vaginal opening).
Table 1. 2015 Consensus terminology and classification of Persistent Vulvar Pain and Vulvodynia
| Vulvar Pain Caused by a Specific Disorder | Vulvodynia |
|---|---|
| Infectious (e.g., recurrent candidiasis, herpes) | Vulvar pain of at least 3 months’ duration, without clear identifiable cause, which may have potential associated factors |
| Inflammatory (e.g., lichen sclerosus, lichen planus, immunobullous disorders) | Localized (e.g., vestibulodynia, clitorodynia) Generalized Mixed (localized and generalized) |
| Neoplastic (e.g., Paget disease, squamous cell carcinoma) | |
| Neurologic (e.g., postherpetic neuralgia, nerve compression, or injury, neuroma) | Provoked (e.g., insertional, contact) Spontaneous Mixed (provoked and spontaneous) |
| Trauma (e.g., female genital cutting, obstetrical) | |
| Iatrogenic (e.g., postoperative, chemotherapy, radiation) | Onset (primary or secondary) |
| Hormonal deficiencies (e.g., genitourinary syndrome of menopause, lactational amenorrhea) | Temporal pattern (intermittent, persistent, constant, immediate, delayed |
The exact number of women with vulvodynia is unknown. Researchers estimate that 9% to 18% of women between the ages of 18 and 64 may experience vulvar pain during their lifetimes 7, 8. In an epidemiological study carried out in the United States, researchers found that up to 16% of women experience vulvodynia throughout their lives 9 and that by age of 40, 7% to 8% of women would have experienced symptoms of vulvodynia at some point in their life 10. In Spain, a study published in 2019 has shown that vulvodynia prevalence throughout life reaches 13% of all women 11.
The evidence suggests that many women either do not seek help at all or go from doctor to doctor seeking a diagnosis and treatment without receiving answers 12.
Sometimes, vulvodynia is described with more specific terms:
- Generalized vulvodynia is pain or discomfort that can be felt in the entire vulvar area.
- Localized vulvodynia is felt in only one place on the vulva.
- Provoked vulvodynia is pain triggered by an activity or contact with the area, such as having sex, using a tampon, having a gynecological exam, or even wearing tight-fitting pants. Alternatively, spontaneous vulvodynia occurs when the pain is not initiated by any known trigger 13.
- Provoked vestibulodynia is vulvodynia with provoked pain that occurs in the vestibular region of the vulva, or the entry point to the vagina. This condition has formerly been called vulvar vestibulitis syndrome, focal vulvitis, vestibulodynia, or vulvar vestibulitis 13.
Although women often don’t mention vulvodynia to their doctors, vulvar pain is fairly common.
If you have pain in your genital area, discuss it with your doctor or ask for a referral to a gynecologist. It’s important to have your doctor rule out more easily treatable causes of vulvar pain — for instance, yeast or bacterial infections, herpes, precancerous skin conditions, genitourinary syndrome of menopause, and medical problems such as diabetes.
It’s also important not to repeatedly use over-the-counter treatments for yeast infections without seeing your doctor. Once your doctor has evaluated your symptoms, he or she can recommend treatments or ways to help you manage your pain.
Since vulvodynia is not simply a gynecological condition, many experts favor a multi-disciplinary approach to its management. Vulvodynia treatments focus on relieving symptoms.
Vulvodynia treatment may involve visiting a 14, 15:
- gynecologist or vulvovaginal specialist,
- dermatologist,
- neurologist,
- pain management specialist,
- urogynecologist, and/or
- physical therapist.
Also, because vulvodynia typically affects a woman’s sexual relationships and emotional well-being, your provider may recommend a psychologist or couples/sex therapist.
Many kinds of treatment are available. No one method works all the time for everyone and it may take time to find a treatment or combination of treatments, that alleviates your pain. It can take a few months after starting a treatment before any relief is noticed. Keeping a pain diary can help you track your symptoms and how they respond to different therapies. In some cases, your gynecologist or other health care professional may refer you to a pain specialist. A pain specialist may use techniques such as ultrasound and electrical stimulation to relieve pain.
Treatments are directed towards alleviating symptoms and usually provides moderate pain relief. Some women experience relief with a particular treatment, while others do not respond or experience unacceptable side effects.
Vulvar pain can have an emotional or psychological aspect, and some women benefit from psychological counseling, sex therapy, or both.
Women with provoked vestibulodynia may be candidates for surgery. Success rates for surgery vary from 60% – 90%.
Figure 1. The vulva – the outer part of the female genitalia
Localized Vulvodynia
Most women have pain at only one vulvar site. If the pain is in the vestibule, the tissue surrounding the vaginal opening, the diagnosis is vestibulodynia formerly known as vulvar vestibulitis syndrome (see Figure 2).
Figure 2. Localized vulvodynia
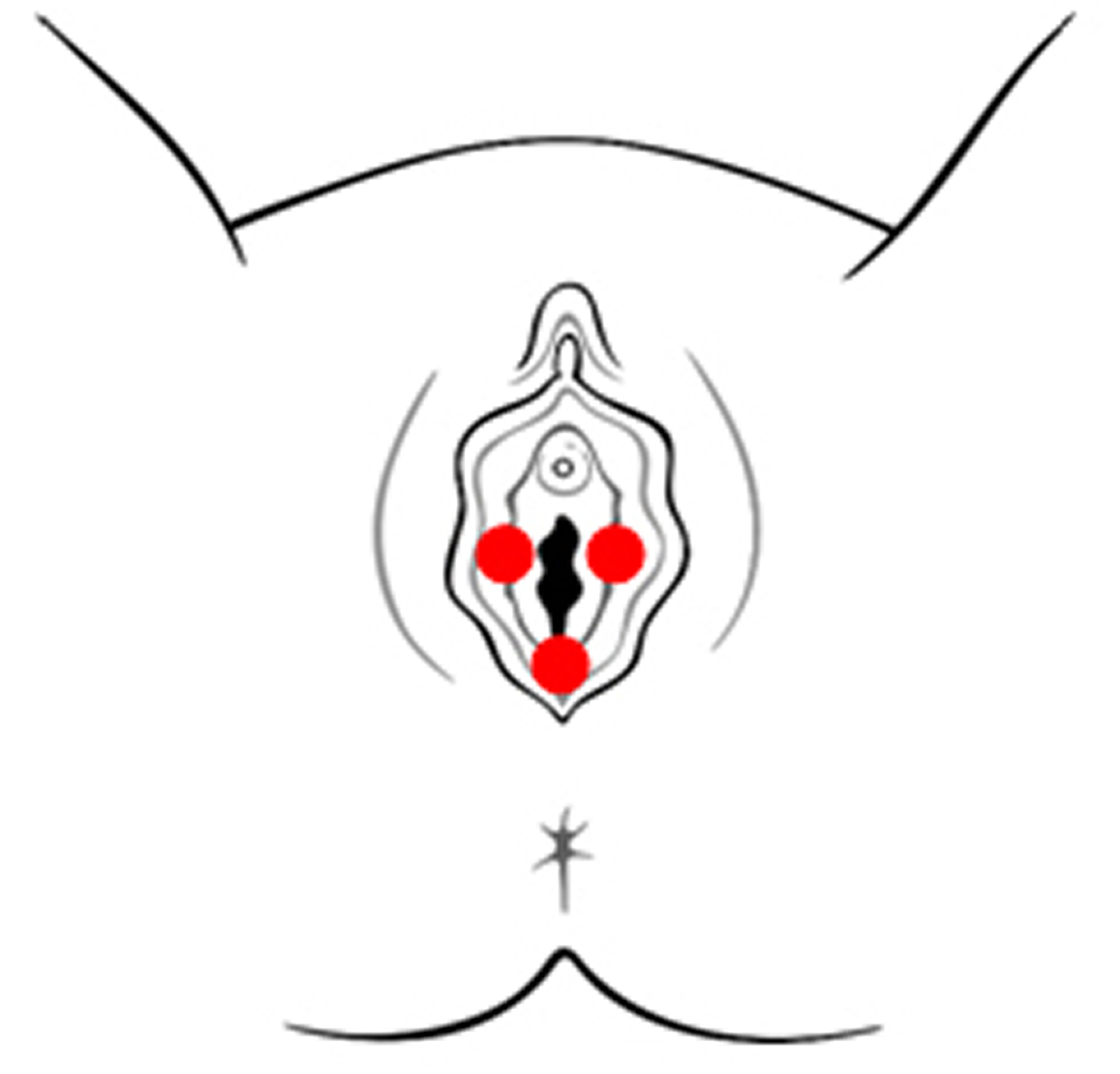
The majority of women with localized vulvodynia have provoked vestibulodynia, in which pain occurs during or after pressure is applied to the vestibule, e.g., with:
- sexual intercourse,
- tampon insertion,
- a gynecologic examination,
- prolonged sitting, and/or
- wearing fitted pants.
A less common form of localized vulvodynia, known as clitorodynia (pain in the clitoris), can be very painful.
Provoked vestibulodynia is further classified as primary or secondary.
Women with primary provoked vestibulodynia have experienced vestibular pain since the first attempt at vaginal penetration.
Women with secondary provoked vestibulodynia have experienced pain-free sexual intercourse prior to the development of vulvar pain.
Generalized Vulvodynia
For women with generalized vulvodynia (GV), pain occurs spontaneously and is relatively constant, but there can be some periods of symptom relief.
Activities that apply pressure to the vulva, such as prolonged sitting or sexual intercourse, typically exacerbate symptoms.
Vulva anatomy
The vulva is the outer part of the female genitals (Figure 1). The vulva includes the opening of the vagina sometimes called the vestibule. The vulva includes:
- Labia majora: two large, fleshy lips, or folds, of skin.
- Labia minora: small lips just inside the labia majora surrounding the openings to the urethra and vagina.
- Vestibule: space where the vagina opens
- Prepuce: a fold of skin formed by the labia minora that covers the clitoris
- Clitoris: a small protrusion of nerve tissue sensitive to stimulation
- Fourchette: area beneath the vaginal opening where the labia minora meet
- Perineum: area between the vagina and the anus
- Anus: opening at the end of the anal canal
- Urethra: connecting tube to the bladder
Around the opening of the vagina, there are 2 sets of skin folds. The inner set, called the labia minora, are small and hairless. The outer set, the labia majora, are larger, with hair on the outer surface. (Labia is Latin for lips.) The inner and outer labia meet, protecting the vaginal opening and, just above it, the opening of the urethra (the short tube that carries urine from the bladder). The Bartholin glands are found just inside the opening of the vagina — one on each side. These glands produce a mucus-like fluid that acts as a lubricant during sex.
At the front of the vagina, the labia minora meet to form a fold or small hood of skin called the prepuce. The clitoris is beneath the prepuce. The clitoris is an approximately ¾-inch structure of highly sensitive tissue that becomes swollen with blood during sexual stimulation. The labia minora also meet at a place just beneath the vaginal opening, at the fourchette. Beyond the fourchette is the anus, the opening to the rectum. This is where stool comes out of the body. The space between the vagina and the anus is called the perineum.
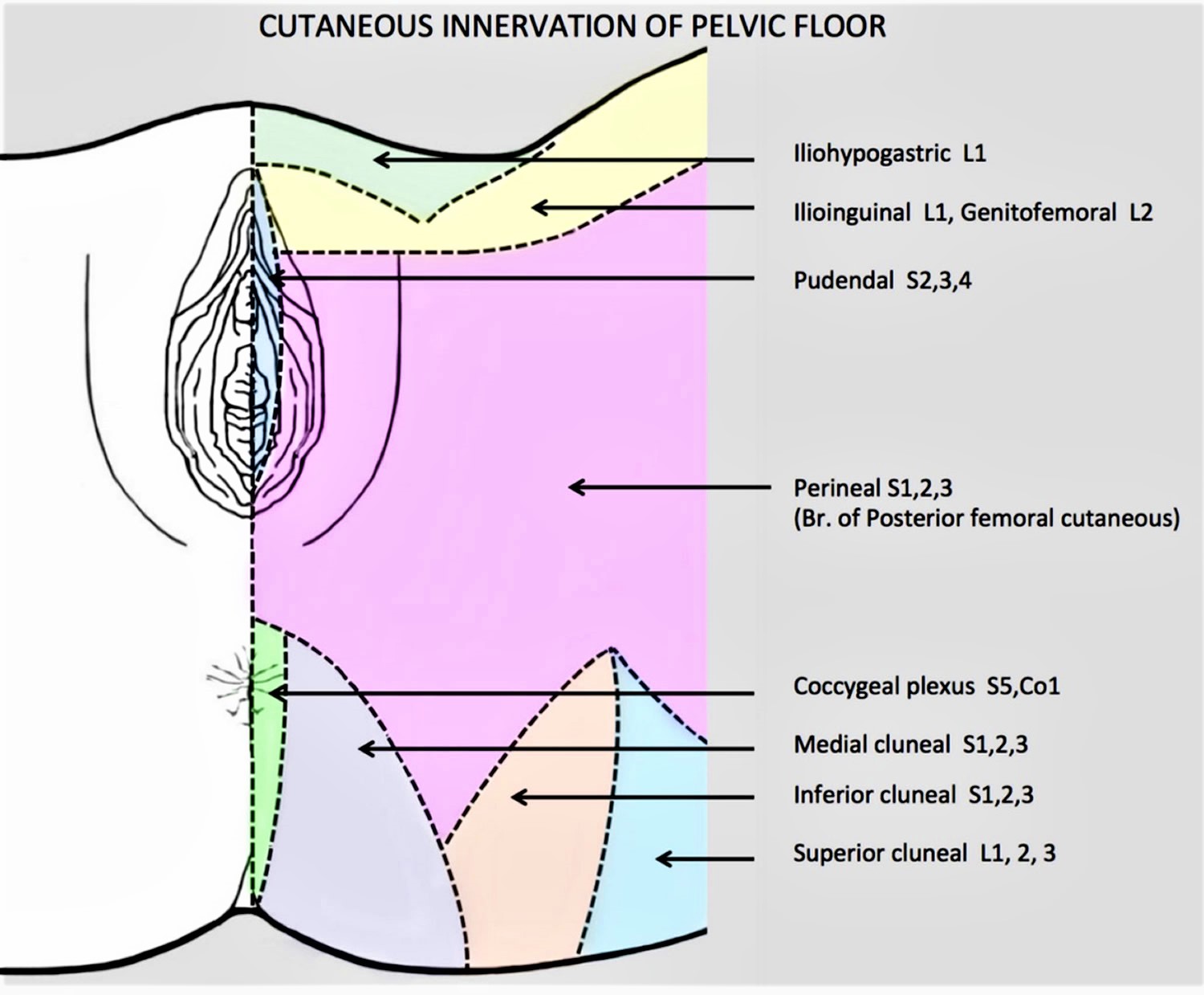
The pudendal nerve transmits pain messages and other sensations from the vulva (Figures 3 and 4). The pudendal nerve originates from the sacral spine, which is located directly below the low back area. The nerve passes through the pelvis and enters the vulvar region near the ischial spine, which is part of the hip bone. From there, it branches off into the inferior rectal nerve, perineal nerve and dorsal nerve of the clitoris. The pudendal nerve is responsible for proper functioning and control of urination, defecation and orgasm in both males and females.
Figure 3. Nerve supply of the vulva
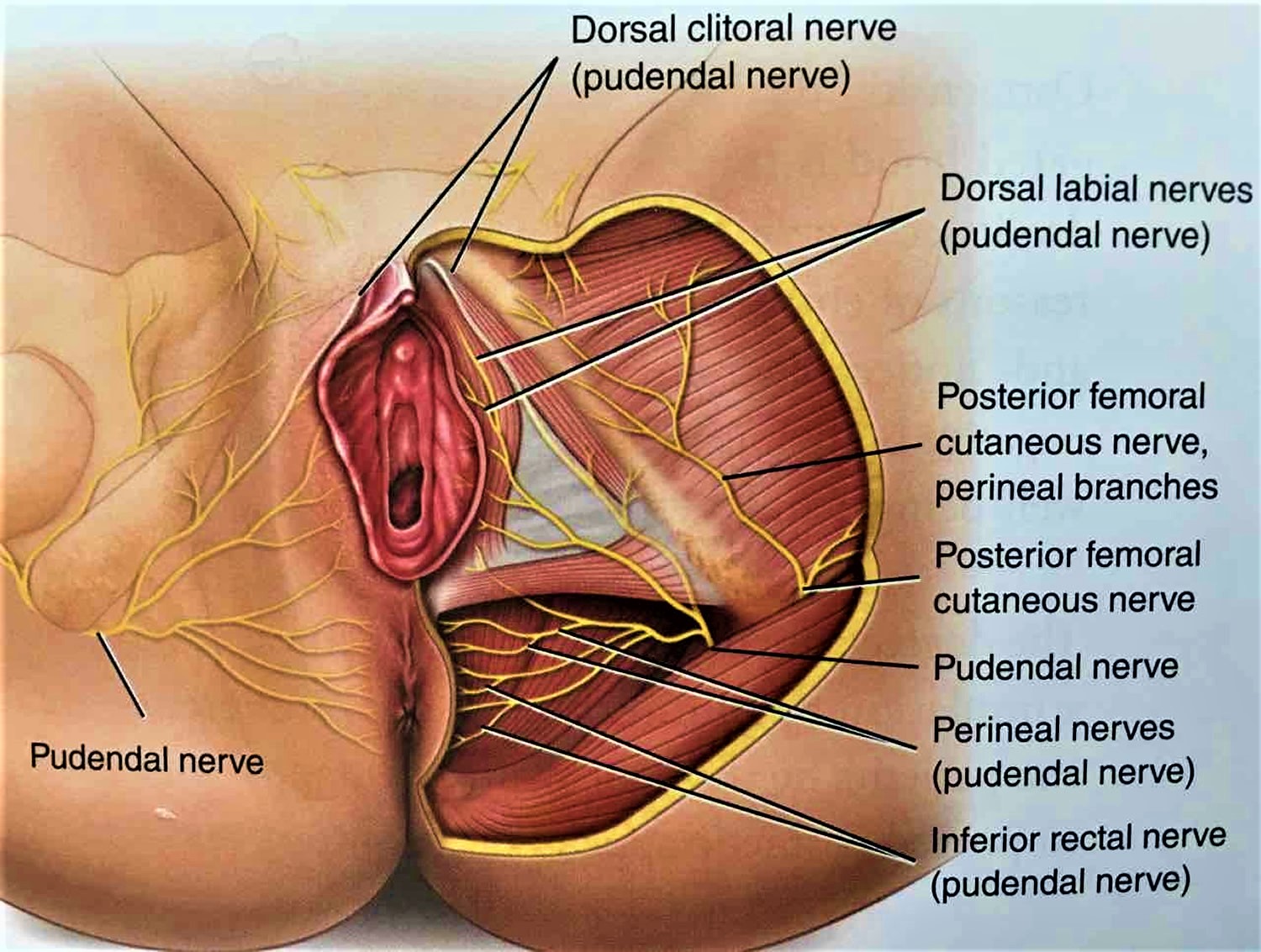
Figure 4. Nerve supply of the vulva
Vulvodynia causes
Vulvodynia is not caused by an active infection or a sexually transmitted disease. Vulvodynia tends to be diagnosed when other causes of vulvar pain, such as infection or skin diseases, are ruled out. Through continued research efforts, scientists move closer to discovering the underlying cause(s) of vulvodynia. Vulvodynia is likely caused by many factors working together.
Researchers speculate that one or more of the following may cause, or contribute to, vulvodynia 16:
- An injury to, or irritation of, the nerves that transmit pain from the vulva to the spinal cord
- Inflammation of the vulva
- Long-term reactions to certain infections
- Comorbidities and other pain syndromes (e.g., painful bladder syndrome, fibromyalgia, irritable bowel syndrome, temporomandibular disorder)
- Certain genetic disorders
- Sensitivity to certain foods
- Dysfunction of the muscles of the pelvic floor
- Conditions that affect nearby muscles or bones (e.g., pelvic muscle overactivity, myofascial, biomechanical)
- An increase in the number and sensitivity of pain-sensing nerve fibers in the vulva
- Elevated levels of inflammatory substances in the vulva
- An abnormal response of different types of vulvar cells to environmental factors such as infection or trauma
- Genetic factors such as susceptibility to chronic vestibular inflammation, chronic widespread pain and/or inability to combat vulvovaginal infection
- Pelvic floor muscle weakness, spasm or instability
- Injury to or irritation of the nerves that transmit pain and other sensations from the vulva
- Hormonal factors (e.g., pharmacologically induced)
- Altered hormone receptor expression in the vulvar tissue
- Psychosocial factors (e.g., mood, interpersonal, coping, role, sexual function)
- Localized hypersensitivity to Candida or other vulvovaginal organisms
- Recently it has been proposed an association between vulvodynia and the reported history of exposures to a number of household and work-related environmental toxins 17:
- Any exposure to spraying chemicals in or around the home
- Use of products that kill insects at home
- Use of products that kill insects on lawn
- Use of products that kill weeds or pest plants on lawn
- Use of products that kill mildew, blight, or fungus on law
- Use of insect repellant at least once a day for 5 days in a row
- Eesiding where insecticides were regularly sprayed
- Any exposure to rodent poison or mothballs at home
- Any exposure to pesticides, herbicides, or fumigants at work
- Exposure to pesticides for at least once a week for at least a month
Other causes of vulval pain
Pain in the vulva isn’t always vulvodynia. It can have a number of other causes, such as:
- persistent vaginal thrush or other vaginal infections
- sensitivity to something touching the vulva, such as soap, bubble bath or medicated creams (known as irritant contact dermatitis)
- a drop in the hormone oestrogen causing dryness of the vulva, particularly during the menopause
- a recurrent herpes infection
- lichen sclerosus or lichen planus (skin conditions that can cause intense irritation and soreness of the vulva)
- in rare cases, Behcet’s disease (a condition of the blood vessels that can cause genital ulcers) or Sjogren’s syndrome (a disorder of the immune system that can cause vaginal dryness)
Your doctor may want to rule out these conditions before treating you for vulvodynia. Some women can have a combination of problems, for example recurrent thrush and vulvodynia, with both needing proper treatment to reduce pain.
In summary, the relationship between genetic, inflammatory, infectious, hormonal, neuroproliferative, or muscular factors and vulvodynia has not been demonstrated 6. The International Association for the Study of Pain Interest Group on Neuropathic Pain (IASP NeuPSIG) states that the pain in vulvodynia should not be considered neuropathic and therefore it must fall into the category of dysfunctional pain 18.
Genetic factors
Some studies suggest that some women have a genetic predisposition to suffer from vulvodynia 6. This predisposition could be related to genetic polymorphisms that increase the risk of candidiasis or other vulvar infections, to genetic changes that favor an exaggerated inflammatory response, or to changes that increase hormonal susceptibility to oral contraceptives, or some polymorphisms involved in the modulation of endogenous pain 19, 20, 21. Polymorphism refers to the presence of two or more variant forms of a specific DNA sequence that can occur among different individuals or populations.
In some studies carried out in identical twins with chronic pelvic pain syndromes, a genetic component appears to be observed, but the contribution of this genetic predisposition does not reach a third of the total variation in the susceptibility to suffering from chronic pelvic pain syndromes 22, 23. Other studies have not found that the proposed genetic polymorphisms contribute to the development of vulvodynia 24, 25.
Inflammatory and infectious factors
It has been hypothesized an inflammatory pathogenesis for vulvodynia 26, 27, secondary to recurrent bacterial or candida infections 28 or, in some cases, following trauma to the vestibular mucosa 29. It has been suggested that there is a relationship between natural killer cell number deficiencies and recurrent yeast infections. Thus, vulvodynia would express a central sensitization condition that persists after the resolution of the acute local inflammation 30.
Several groups have proposed the study of vaginal or plasma pro-inflammatory cytokine profiles as possible biomarkers of vulvodynia 31, 32. An increase in the number of mast cells in the vestibular tissue has been found in women with vulvodynia 33, as well as a systemic reduction in the number of natural killer cells compared to controls 34.
However, the results of these studies are inconsistent. A recent systematic review was carried out by Chalmers et al. 33 has concluded that current evidence is limited and contradictory regarding the presence of local and systemic inflammation in women with vulvodynia, including levels of cytokines, prostaglandin E2, T cells, B cells, mast cells, natural killer cells, and macrophages.
Hormonal factors
Sexual responses, as well as genital pain, are modulated, in addition to neural pathways, by circulating levels of gonadal hormones 35. It has thus been theorized that low estrogen levels could lead to vulvodynia and dyspareunia. The decline in estrogen levels can occur naturally or iatrogenically. The most common cause of low estrogen levels in women is menopause. Other natural causes include anovulation secondary to lactation, anorexia, hypothalamic amenorrhea, hyperprolactinemia, and excessive physical activity or physiological stress 36.
As iatrogenic causes, decreased circulating estrogen after oophorectomy and hysterectomy and combined hormonal contraceptive drugs are cited 36. Combined hormonal contraceptives lead to a reduction in serum estradiol and free testosterone by decreasing ovarian production of estrogen and total testosterone. In addition, some combined hormonal contraceptives contain synthetic progestogens that act as antagonists of testosterone at the androgen receptor 36.
Combined hormonal contraceptives can cause changes in the vestibular mucosa, increasing its vulnerability to mechanical stress 37. It has been suggested that the use of combined hormonal contraceptives before the age of 17 increases the relative risk of developing vulvodynia 38. However, this association has not been found in population studies 39.
It has been shown that women with vulvar pain without an identifiable cause, but who started taking hormonal contraceptives may effectively be treated by discontinuing these contraceptives combined with the application of topical hormone therapy 40. Based on this therapeutic combination, our group proposes to distinguish persistent vulvar pain due to a genitourinary syndrome from menopause due to lack of estrogens from vulvodynia (pain syndrome), which may appear overlapping in menopause 41.
Peripheral neuropathic pain
One of the proposals on the cause of vulvodynia, mainly provoked vulvodynia, is a greater nerve fiber proliferation in the vulvar vestibule. For example, some studies have found an increase in the density of C nociceptor endings 29, 42. In these cases, the proposed treatment is vestibulectomy 43, 44. However, on the one hand, it has been shown that an increase in the density of nociceptors is not consistently correlated with allodynia in the vestibular mucosa, with no significant differences being observed between those points that patients perceive as sensitive and those that are not 45.
Pelvic floor muscle dysfunction
Vulvodynia has been associated with dysfunction of the pelvic floor muscles, such as hyperactivity, increased pelvic floor tone at rest, deficits in muscle control, and the presence of myofascial trigger points 46. The location of the pain is even related to the specific involvement of different muscles of the pelvic floor 47. However, there is no evidence for these claims 48 and to accurately assess pelvic floor muscle dysfunction in clinical practice, other more objective methods such as 4D transperineal ultrasound or dynamometric speculum should be further developed 49.
It is not clear whether the observed muscle hypertonicity is causally related to the cause of vulvodynia or is the result of pain 26, 27. The phenomenon of increased muscle tone of the pelvic floor muscles, frequently reported in women with provoked vulvodynia, is probably not the cause but the consequence of the pain 50. Women may also have spontaneous contraction of the pelvic floor muscles during attempted vaginal penetration. This pelvic floor muscle dysfunction may be the result of a protective reflex to prevent penetration or painful contact 27.
Psychological factors
Pain is a complex human experience in which many different factors interact, not only biological but also psychological, social, and cultural. Many women who suffer from vulvodynia also report more anxiety, fear of pain, hypervigilance, catastrophism, and depression 51. The association between anxiety and sexual problems and pelvic pain has been suggested by several studies 52, 53. Psychosexual evaluation combined with psychotherapy is recommended as a therapeutic approach to vulvodynia 51, 54.
Vulvodynia complications
Vulvodynia is one the most common causes of pain during sexual intercourse in premenopausal women 1. Because it can be painful and frustrating and can keep you from wanting sex, vulvodynia can cause emotional problems. For example, fear of having sex can cause spasms in the muscles around your vagina (vaginismus). Other complications might include:
- Anxiety
- Depression
- Sleep disturbances
- Sexual dysfunction
- Altered body image
- Relationship problems
- Decreased quality of life
Vulvodynia symptoms
The main symptom of vulvodynia is pain. The type of pain can be different for each woman.
Vulvodynia can cause burning, stinging, irritation, or rawness of the vulva. Some women may also have itching, aching, soreness, throbbing, or swelling. These symptoms may be caused by pressure on the vulvar area, such as during sex or when inserting a tampon. Symptoms may occur during exercise, after urinating, or even while sitting or resting 55.
Pain may move around or always be in the same place. It can be constant, or it can come and go.
Vulvodynia diagnosis
If you have vulvar pain, your gynecologist or other health care professional will try to rule out the most common causes of vulvar pain first. You may be asked questions about your symptoms, sexual history, and medical and surgical history. You may be asked when symptoms occur, what treatments you have tried, and whether you have any allergies, chronic infections, or skin problems.
Your gynecologist also will examine the vulva and vagina carefully. Your gynecologist may use a moist cotton swab to touch areas of the vulva (also known as cotton swab test). During the cotton-swab test, gentle pressure is applied to various vulvar sites and you’re asked to rate the severity of the pain. The goal is to find where the pain is and whether it is mild, moderate, or severe. If any areas of skin appear suspicious, your gynecologist may examine them with a magnifying instrument or take a biopsy of the area. Your gynecologist should carefully examine the vaginal secretions to rule out an active infection or skin disorder. Routine cultures for yeast and bacterial infections should be performed. Your gynecologist may also recommend that you have blood drawn to assess levels of estrogen, progesterone and testosterone.
You also may have a biopsy of the vulvar skin.
Vulvodynia treatment
Since vulvodynia is not simply a gynecological condition, many experts favor a multi-disciplinary approach to its management. Vulvodynia treatments focus on relieving symptoms.
Vulvodynia treatment may involve visiting a 14, 15:
- gynecologist or vulvovaginal specialist,
- dermatologist,
- neurologist,
- pain management specialist,
- urogynecologist, and/or
- physical therapist.
Also, because vulvodynia typically affects a woman’s sexual relationships and emotional well-being, your provider may recommend a psychologist or couples/sex therapist.
Many kinds of treatment are available. No one method works all the time for everyone and it may take time to find a treatment or combination of treatments, that alleviates your pain. It can take a few months after starting a treatment before any relief is noticed. Keeping a pain diary can help you track your symptoms and how they respond to different therapies. In some cases, your gynecologist or other health care professional may refer you to a pain specialist. A pain specialist may use techniques such as ultrasound and electrical stimulation to relieve pain.
Treatments are directed towards alleviating symptoms and usually provides moderate pain relief. Some women experience relief with a particular treatment, while others do not respond or experience unacceptable side effects.
Vulvar pain can have an emotional or psychological aspect, and some women benefit from psychological counseling, sex therapy, or both.
Women with provoked vestibulodynia may be candidates for surgery. Success rates for surgery vary from 60% – 90%.
Current vulvodynia treatments include:
- Discontinuation of Irritants
- Oral “Pain-Blocking” Medications
- Tricyclic Antidepressants
- Serotonin-Norepinephrine Reuptake Inhibitors
- Anticonvulsants
- Opioids
- Topical Medications
- Topical Hormonal Creams (e.g., estrogen, testosterone)
- Topical Anesthetics (e.g., lidocaine)
- Topical Compounded Formulations (e.g., anticonvulsant, antidepressant)
- Pelvic Floor Muscle Therapy
- Nerve Blocks
- Neurostimulation and Spinal Infusion Pump
- Biofeedback therapy. This therapy can help reduce pain by teaching you how to relax your pelvic muscles and control how your body responds to the symptoms.
- Surgery (for women with Provoked Vestibulodynia)
- Complementary or Alternative Medicine (including relaxation, massage, homeopathy, and acupuncture). But there is little evidence about the effectiveness of these approaches.
An expert panel, convened in 2016, recommended against the use of antidepressants or corticosteroids for vulvodynia 56.
Vulvodynia pain relief
Prescription medication
Several medications can be used to treat vulvodynia. Medications can be taken in pill form (oral), injected into the affected area, or applied to the skin (topical). The following medications have been found to be helpful in treating vulvodynia:
- Local anesthetics —These medications are applied to the skin. They may be used before sexual intercourse to provide short-term pain relief, or they can be used for extended periods. Topical lidocaine with 2–5% gel or cream is often tried in women with vulvodynia to reduce pain sensitivity of the skin and mucous membranes and for desensitization of vestibular nerves 57. This can be applied overnight or even several times a day depending on the patient’s needs. In a double-blind randomized controlled trial that compared topical lidocaine to placebo, no difference was found in pain response to the swab test in women with vulvodynia 58. Intermittent topical use of lidocaine may be useful for women with intense vestibular touch pain and may be used prior to vaginal penetration. Using lidocaine ointment can cause your partner to have temporary numbness after sexual contact.
- Antidepressants and antiseizure (anticonvulsants) drugs —Drugs used to treat depression and to prevent seizures also may help with the symptoms of vulvodynia. It may take a few weeks for these medications to work. Some types of antidepressants can be provided in the form of a cream that is applied to the skin.
- Tricyclic antidepressants (TCAs) are drugs considered first-line in the treatment of neuropathic pain 59. The exact anti-analgesic mechanism of tricyclic antidepressants is not completely clear but it appears to be due to repeated β2-adrenergic stimulation increasing concentration of norepinephrine at the level of the synaptic cleft 15. Amitriptyline is often used for generalized pain not necessarily associated with vulvodynia, however some efficacy has been observed when administered to patients reporting this painful condition 60. The only randomized controlled trial that evaluated tricyclic antidepressants in women with vulvodynia was conducted on low-dose oral desipramine that, however, did not find a superior effect compared to placebo 61. Other types of antidepressants used for neuropathic pain have not yet shown proven efficacy for vulvodynia.
- Anticonvulsants are often used in the treatment of vulvar pain but have been evaluated in a very small number of vulvodynia studies. Among the most used, gabapentine and cabergoline. Gabapentine is able to reduce the propagation of the painful signal by acting on voltage-dependent sodium channels and reducing the release of neurotransmitters at the presynaptic level. However, it was found that there are no differences in painful sensation by comparing two groups of women in which vulvar pain was evoked through rubbing with a vaginal swab on the vaginal fornixes, one group of which took gabapentine and the other of which is a control placebo group 62. In another case control study, on the other hand, gabapentin was able to reduce painful sensation compared to placebo 63. Further studies are needed to verify the potential role of anticonvulsant drugs in the treatment of painful vulvar pathologies, especially considering that this category of drugs could be exploited in all those overlap syndromes, in generalized vulvodynia or even in the case of comorbidities 64.
- Hormone creams —Estrogen cream applied to the vulva may help relieve vulvodynia in some cases.
- It was found that combining estrogen with testosterone and at the same time discontinuing the estrogen-progestogen pill, there was a reduction of vestibular pain in women with vulvodynia 65. It seems that hormone replacement therapy should not be recommended in the treatment of painful vulvar diseases, although future studies may show that there is a subgroup of patients who can improve with the cessation of hormonal contraceptives in combination with hormonal topical treatment 64.
- Neurotoxic agents. The use of botulinum toxin A (Botox) to reduce hypertonicity and pelvic pain in women in whom pelvic floor physical therapy has occurred does not improve symptom in patients who have tried this therapeutic strategy. However, the injection of botulinum toxin A (Botox) represents a simple and inexpensive outpatient procedure, furthermore favorable results have been reported with doses up to 100 Units 64. Randomized placebo-controlled studies on botulinum toxin A (Botox) are currently being carried out and it is hoped that the results obtained will help us to clarify which doses and above all which methods of injection are preferable and which subgroups of patients could benefit most from them 64.
Conventional painkillers such as acetaminophen (paracetamol) won’t usually relieve the pain of vulvodynia. But several medications available on prescription can help, including:
- antidepressants called amitriptyline and nortriptyline – possible side effects include drowsiness, weight gain and dry mouth
- anti-epilepsy medicines called gabapentin and pregabalin – possible side effects include dizziness, drowsiness and weight gain
Your doctor will probably start you on a low dose and gradually increase it until your pain subsides. You may need to take the medication for several months.
If you have pain in a specific area of your vulva, injections of local anesthetic and steroid medication into a nearby nerve may provide temporary pain relief.
Antihistamines might reduce itching.
Table 2 summarizes all the main drug classes used in the treatment of vulvodynia.
Table 3 shows the treatment strategy recommended by the Vulvodynia Nertwork study group 14. Interestingly, a multimodal intervention (consisting in the use of two or more types of therapy) was adopted in 74.3% of patients 14.
Table 2. Drugs used in the treatment of vulvodynia
| Drug Therapy | Regimen |
|---|---|
| Anti-nociceptive agents | |
| Lidocaine | Topical 5% ointment, every night for 7 weeks |
| Topical 2% lidocaine gel, 5 times per day for 12 weeks | |
| 5% cream, 4 times per day for 12 weeks | |
| Tricyclic | Oral desipramine, administered daily, increasing dose from 25 mg to 150 mg (6 weeks) for 12 weeks |
| Topical 2% amitriptyline cream, twice per day for 12 weeks | |
| Serotonin-norepinephrine reuptake inhibitors | Oral milnacipran, 50–200 mg per day for 12 weeks |
| Capsaicin | Topical 0.025% cream, 20 min application (then removed) per day for 8 weeks |
| Topical 0.05% cream, decreasing dose from twice per day to twice per week for 4 months | |
| Anti-convulsant agents | |
| 2–6% topical cream, 8 weeks | |
| Gabapentin | Highest tolerable oral dose between 1200 and 3000 mg per day for 8 weeks |
| Oral gabapentin, 1200–3000 mg per day for 8 weeks | |
| Anti-inflammatory agents | |
| Submucosal methylprednisolone (1, 0.5, 0.3 mL) once per week for 3 weeks | |
| Corticosteroids | 0.05% Clobetasol propionate or 0.5% topical hydrocortisone ointment for 28 nights |
| Topical 1% hydrocortisone cream, twice per day for 13 weeks | |
| Anti-neuroinflammatory agents | |
| 200 mg 3 times daily for four months | |
| Palmitoylethanolamide | 400 mg/40 mg 2 times daily for two months |
| 400 mg/40 mg two times daily for three months | |
| Antioxidant agents | |
| Alpha lipoic acid | 300–600 mg tablets for at least 3 weeks (600 mg for the acute phase, 300 mg for the maintenance phase) |
| 1800 mg intravenously per week | |
| Neurotoxic agents | |
| 20 U, single injection into the bulbocavernosus muscle | |
| Botulinum toxin A | 100 U, single injection into the bulbocavernosus muscle |
| 100 U, single injection into the levator ani muscle | |
| 50 U (single injection), 100 U (single injection, repeated after 3 months) |
Table 3. Recommended therapies for the treatment of vulvodynia by Vulvodynia Network Group
| Anticonvulsants (Neuromodulators) |
| -First-line treatment |
| -Amitriptyline oral: 1 drop = 2 mg; start with 26 mg and increase in steps of 5 mg, as tolerated, every 3–7 days up to 30 mg |
| -Second-line treatment |
| -Gabapentin (from 300 to 1500 mg/daily) or |
| -Pregabalin (from 50 to 150 mg/daily) or |
| -Duloxetine (from 30 to 60 mg/daily) * if the patient is among the non-responders, combined therapy is useful |
| Neuronal anti-inflammatory drugs |
| -Alpha-lipoic acid (600 mg/daily) |
| Non-pharmacological treatments: rehabilitation therapy of the pelvic floor |
| -Muscle rehabilitation exercises for the pelvic floor, such as internal stretching and hands-on massage, trigger point acupressure, external and internal tissue massage, electromyographic biofeedback |
| -Electrical nerve stimulation (TENS) |
| -Muscle relaxants: Diazepam, oral (2 mg to 10 mg/day) or Diazepam, vaginal 5 mg/day (off-label) |
| Anti-fungal |
| -Fluconazole 200 mg (3 times a day for 1 week then once a week for 4 weeks, then 1 tbl/15 days for 2 months, then 1 tbl/months for 3 months |
| -Itraconazole 100 mg (twice a day for 3 days, then 1 tbl/15 days for 3 months) * used in case of patient suffering from recurrent Candida infections |
Physical therapy
Physical therapy is another option for treating vulvodynia. This type of therapy can relax tissues in the pelvic floor and release tension in muscles and joints. Biofeedback is a form of physical therapy that trains you to strengthen the pelvic floor muscles. Strengthening these muscles may help lessen your pain.
A physiotherapist can teach you some pelvic floor exercises (such as squeezing and releasing your pelvic floor muscles) to help relax the muscles around your vagina.
Another technique to relax the muscles in the vagina and desensitize it involves using a set of vaginal trainers. These are smooth cones of gradually increasing size and length which can be inserted into your vagina in the privacy of your own home.
Some physiotherapists may also suggest trying TENS (transcutaneous electrical nerve stimulation) to reduce your pain. This is where a machine is used to deliver a mild electrical current to the painful area.
Trigger point therapy
Trigger point therapy is a form of massage therapy. A trigger point is a small area of tightly contracted muscle. Pain from a trigger point travels to nearby areas. Trigger point therapy involves soft tissue massage to relax the tight area of muscle. A combination of an anesthetic drug and a steroid also can be injected into the trigger point to provide relief.
Physical therapy and biofeedback also can be helpful for women with vulvodynia 66. Physical therapy for vulvodynia may include exercise, education, or manual therapies, such as massage, joint mobilization, or soft-tissue mobilization. Other forms of physical therapy can involve ultrasound, electrical stimulation, or biofeedback techniques.
Pelvic floor therapy
Many women with vulvodynia have tension in the muscles of the pelvic floor, which supports the uterus, bladder and bowel. Exercises to relax those muscles can help relieve vulvodynia pain.
Nerve block
A nerve block is a type of anesthesia in which an anesthetic drug is injected into the nerves that carry pain signals from the vulva to the spinal cord. This treatment interrupts the pain signals and can provide short-term and sometimes long-term pain relief. Injection of a drug called botulinum toxin A (also known as Botox) has been used to treat vulvodynia. This drug relaxes muscles of the pelvic floor. Current evidence regarding the efficacy of the botulinum toxin A treatment is mixed, and further clinical trials are needed.
Cognitive behavioral therapy
Cognitive behavioral therapy may be suggested if you have vulvodynia. A counselor can help you learn to cope with chronic pain. This may reduce stress and help you feel more in control of your symptoms. Sexual counseling can provide support and education about this condition for you and your partner. A randomized, controlled clinical trial found that women who had cognitive behavioral therapy reported a 30% decrease in vulvar pain that occurs with intercourse 56.
Surgery
Surgery is usually considered a last resort and may be an option for women with severe pain from vulvar vestibulitis who have not found relief through other treatment options 67. A vestibulectomy is the removal of the painful tissue from the part of the vulva called the vestibule and may help relieve pain and improve sexual comfort. It can be used for women who have vulvodynia specific to this area and for whom other treatments have not worked. It is not recommended for women with generalized vulvodynia that is not limited to the vestibule 66.
Vulvodynia home remedies
If you have vulvodynia, gentle care of the vulva can help provide some pain relief for some women 68. Avoid products and other items that may be irritating. The following may be helpful in relieving or reducing symptoms:
- Wear 100% cotton underwear to increase ventilation and dryness.
- Do not wear underwear while sleeping.
- Avoid tightfitting pantyhose and nylon underwear. Tight clothing restricts airflow to your genital area, often leading to increased temperature and moisture that can cause irritation.
- Soak in a sitz bath. Two to three times a day, sit in comfortable, lukewarm (not hot) or cool water with Epsom salts or colloidal oatmeal for five to 10 minutes.
- Avoid douching.
- Avoid irritants, such as perfumes, dyes, shampoos, detergents, and deodorants.
- Clean the vulva with water only.
- Wash gently. Scrubbing the affected area harshly or washing too often can increase irritation. Instead, use plain water to gently clean your vulva with your hand and pat the area dry. After bathing, apply a preservative-free emollient, such as plain petroleum jelly, to create a protective barrier.
- Switch to 100% cotton pads if regular pads are irritating.
- Use lubricants during sex, but avoid lubricants with flavor or cooling/warming sensation. Don’t use products that contain alcohol, flavor, or warming or cooling agents.
- Rinse and pat the vulva dry after urinating.
- After bathing, apply a thin layer of a preservative-free oil or petroleum jelly to hold in moisture and protect the skin.
- Avoid using a hair dryer to dry the vulvar area.
- Try cold compresses or gel packs on the vulva. Place them directly on your external genital area to ease pain and itching.
- Avoid exercises that put pressure directly on the vulva, such as bicycling or horseback riding.
Over-the-counter gels and lubricants
Applying the anesthetic gel lidocaine to your vulva about 10 minutes before sex may make it more comfortable. To stop the gel getting on your partner, either wipe it off just before having sex or ask your partner to wear a condom (if using condoms, use latex-free ones as latex condoms can be damaged by lidocaine).
If your pain is more constant, applying lidocaine regularly throughout the day may help. Lidocaine can also be used overnight. A tip is to put some on a cotton make-up removal pad and put it onto the sore area so it’s held in place by your underwear.
It’s very common to have some burning when the lidocaine is initially applied which can last several minutes before going numb. Try to give the lidocaine time it to work, but if the burning continues for 10 minutes, wash it off thoroughly.
Tubes of 5% lidocaine gel, cream or ointment can be bought over the counter from a pharmacy, although it’s a good idea to get a doctor’s advice before trying it.
Vaginal lubricants and aqueous cream (also available over the counter) may soothe the area and help moisturize the vulva if it’s dry. Speak to your pharmacist about these treatments.
Alternative medicine
Stress tends to worsen vulvodynia and having vulvodynia increases stress. Although there’s little evidence that alternative techniques work, some women get some relief from yoga, meditation, massage and other stress reducers.
Coping and support
You might find talking to other women who have vulvodynia helpful because it can provide information and make you feel less alone. If you don’t want to join a support group, your doctor might be able to recommend a counselor in your area who has experience helping women cope with vulvodynia.
Sex therapy or couples therapy might help you and your partner cope with vulvodynia’s affect on your relationship.
Vulvodynia diet
Some patients find that following a diet that is low in oxalates and taking calcium citrate supplements is helpful, although the evidence to support this approach is limited 69. Foods that are high in oxalates include greens, nuts, tea, chocolate, and soy products 70. Food high in oxalates may produce urine that is irritating, which contributes to the vulvar pain 71.
References- Brotto L.A., Sadownik L.A., Thomson S., Dayan M., Smith K.B., Seal B.N., Moses M., Zhang A. A Comparison of Demographic and Psychosexual Characteristics of Women With Primary Versus Secondary Provoked Vestibulodynia. Clin. J. Pain. 2014;30:428–435. doi: 10.1097/AJP.0b013e31829ea118
- Moyal-Barracco M, Lynch PJ. 2003 ISSVD terminology and classification of vulvodynia: a historical perspective. J Reprod Med. 2004 Oct;49(10):772-7.
- Bornstein J, Goldstein AT, Stockdale CK, Bergeron S, Pukall C, Zolnoun D, Coady D; consensus vulvar pain terminology committee of the International Society for the Study of Vulvovaginal Disease (ISSVD), the International Society for the Study of Women’s Sexual Health (ISSWSH), and the International Pelvic Pain Society (IPPS). 2015 ISSVD, ISSWSH and IPPS Consensus Terminology and Classification of Persistent Vulvar Pain and Vulvodynia. Obstet Gynecol. 2016 Apr;127(4):745-751. doi: 10.1097/AOG.0000000000001359
- National Vulvodynia Association. (2016). Vulvodynia: A common and under-recognized pain disorder in women and female adolescents – Integrating current knowledge into clinical practice. https://cme.dannemiller.com/articles/activity?id=570&f=1
- Vulvodynia. https://www.mayoclinic.org/diseases-conditions/vulvodynia/symptoms-causes/syc-20353423
- Torres-Cueco R, Nohales-Alfonso F. Vulvodynia-It Is Time to Accept a New Understanding from a Neurobiological Perspective. Int J Environ Res Public Health. 2021 Jun 21;18(12):6639. doi: 10.3390/ijerph18126639
- Arnold, L. D., Bachmann, G. A., Rosen, R., & Rhoads, G. G. (2007). Assessment of vulvodynia symptoms in a sample of U.S. women: A prevalence survey with a nested case control study. American Journal of Obstetrics and Gynecology, 196(2), 128e1-128e6
- Bergeron S, Reed BD, Wesselmann U, Bohm-Starke N. Vulvodynia. Nat Rev Dis Primers. 2020 Apr 30;6(1):36. doi: 10.1038/s41572-020-0164-2
- Harlow BL, Stewart EG. A population-based assessment of chronic unexplained vulvar pain: have we underestimated the prevalence of vulvodynia? J Am Med Womens Assoc (1972). 2003 Spring;58(2):82-8.
- Harlow B.L., Kunitz C.G., Nguyen R.H., Rydell S.A., Turner R.M., MacLehose R.F. Prevalence of symptoms consistent with a diagnosis of vulvodynia: Population-based estimates from 2 geographic regions. Am. J. Obstet. Gynecol. 2014;210:40.e1–40.e8. doi: 10.1016/j.ajog.2013.09.033
- Gómez I., Coronado P.J., Martín C.M., Alonso R., Guisasola-Campa F.J. Study on the prevalence and factors associated to vulvodynia in Spain. Eur. J. Obstet. Gynecol. Reprod. Biol. 2019;240:121–124. doi: 10.1016/j.ejogrb.2019.06.005
- Harlow, B. L., Kunitz, C. G., Nguyen, R. H. N., Rydell, S. A., Turner, R. M., & MacLehose, R. F. (2014). Prevalence of symptoms consistent with a diagnosis of vulvodynia: Population-based estimates from two geographical regions. American Journal of Obstetrics and Gynecology, 210(1), 40.e1–40.e8.
- National Vulvodynia Association. (2012). What is vulvodynia? https://www.nva.org/what-is-vulvodynia/
- LePage K, Selk A. What Do Patients Want? A Needs Assessment of Vulvodynia Patients Attending a Vulvar Diseases Clinic. Sex Med. 2016 Dec;4(4):e242-e248. doi: 10.1016/j.esxm.2016.06.003
- Zolnoun, D.A.; Hartmann, K.E.; Steege, J.F. Overnight 5% lidocaine ointment for treatment of vulvar vestibulitis. Obstet. Gynecol. 2003, 102, 84–87.
- Bornstein J., Goldstein A.T., Stockdale C.K., Bergeron S., Pukall C., Zolnoun D., Coady D., consensus vulvar pain terminology committee of the International Society for the Study of Vulvovaginal Disease (ISSVD) International Society for the Study of Women’s Sexual Health (ISSWSH) International Pelvic Pain Society (IPPS) 2015 ISSVD, ISSWSH, and IPPS Consensus Terminology and Classification of Persistent Vulvar Pain and Vulvodynia. J. Sex. Med. 2016;13:607–612. doi: 10.1016/j.jsxm.2016.02.167
- Reed B.D., McKee K.S., Plegue M.A., Park S.K., Haefner H.K., Harlow S.D. Environmental Exposure History and Vulvodynia Risk: A Population-Based Study. J. Women’s Health. 2019;28:69–76. doi: 10.1089/jwh.2018.7188
- Jensen T.S., Baron R., Haanpää M., Kalso E., Loeser J.D., Rice A.S., Treede R.-D. A new definition of neuropathic pain. Pain. 2011;152:2204–2205. doi: 10.1016/j.pain.2011.06.017
- Babula O., Danielsson I., Sjoberg I., Ledger W.J., Witkin S.S. Altered distribution of mannose-binding lectin alleles at exon I codon 54 in women with vulvar vestibulitis syndrome. Am. J. Obstet. Gynecol. 2004;191:762–766. doi: 10.1016/j.ajog.2004.03.073
- Lev-Sagie A., Prus D., Linhares I.M., Lavy Y., Ledger W.J., Witkin S.S. Polymorphism in a gene coding for the inflammasome component NALP3 and recurrent vulvovaginal candidiasis in women with vulvar vestibulitis syndrome. Am. J. Obstet. Gynecol. 2009;200:303.e1–303.e6. doi: 10.1016/j.ajog.2008.10.039
- Goldstein A., Belkin Z.R., Krapf J.M., Song W., Khera M., Jutrzonka S.L., Kim N.N., Burrows L.J., Goldstein I. Polymorphisms of the Androgen Receptor Gene and Hormonal Contraceptive Induced Provoked Vestibulodynia. J. Sex. Med. 2014;11:2764–2771. doi: 10.1111/jsm.12668
- Vehof J., Zavos H.M.S., Lachance G., Hammond C.J., Williams F.M.K. Shared genetic factors underlie chronic pain syndromes. Pain. 2014;155:1562–1568. doi: 10.1016/j.pain.2014.05.002
- Tunitsky E., Barber M., Jeppson P., Nutter B., Jelovsek J., Ridgeway B. Bladder Pain Syndrome/Interstitial Cystitis in Twin Sisters. J. Urol. 2012;187:148–152. doi: 10.1016/j.juro.2011.09.051
- Heddini U., Bohm-Starke N., Grönbladh A., Nyberg F., Nilsson K.W., Johannesson U. GCH1-Polymorphism and Pain Sensitivity among Women with Provoked Vestibulodynia. Mol. Pain. 2012;8:68. doi: 10.1186/1744-8069-8-68
- Patanwala I.Y., Lamvu G., Ledger W.J., Witzeman K., Marvel R., Rapkin A., Bongiovanni A.M., Feranec J., Witkin S.S. Catechol-O-methyltransferase gene polymorphism and vulvar pain in women with vulvodynia. Am. J. Obstet. Gynecol. 2017;216:395.e1–395.e6. doi: 10.1016/j.ajog.2016.10.020
- Pukall C.F., Goldstein A., Bergeron S., Foster D., Stein A., Kellogg-Spadt S., Bachmann G. Vulvodynia: Definition, Prevalence, Impact, and Pathophysiological Factors. J. Sex. Med. 2016;13:291–304. doi: 10.1016/j.jsxm.2015.12.021
- Wesselmann U., Bonham A., Foster D. Vulvodynia: Current state of the biological science. Pain. 2014;155:1696–1701. doi: 10.1016/j.pain.2014.05.010
- Harlow B.L., Caron R.E., Parker S.E., Chatterjea D., Fox M.P., Nguyen R.H. Recurrent Yeast Infections and Vulvodynia: Can We Believe Associations Based on Self-Reported Data? J. Women’s Health. 2017;26:1069–1076. doi: 10.1089/jwh.2016.5777
- Bohm-Starke N. Medical and physical predictors of localized provoked vulvodynia. Acta Obstet. Gynecol. Scand. 2010;89:1504–1510. doi: 10.3109/00016349.2010.528368
- Ji R.-R., Xu Z.-Z., Gao Y.-J. Emerging targets in neuroinflammation-driven chronic pain. Nat. Rev. Drug Discov. 2014;13:533–548. doi: 10.1038/nrd4334
- Reed B.D., Plegue M.A., Sen A., Haefner H.K., Siddiqui J., Remick D.G. Nerve Growth Factor and Selected Cytokines in Women With and Without Vulvodynia. J. Low. Genit. Tract Dis. 2018;22:139–146. doi: 10.1097/LGT.0000000000000377
- Zanotta N., Campisciano G., Scrimin F., Ura B., Marcuzzi A., Vincenti E., Crovella S., Comar M. Cytokine profiles of women with vulvodynia: Identification of a panel of pro-inflammatory molecular targets. Eur. J. Obstet. Gynecol. Reprod. Biol. 2018;226:66–70. doi: 10.1016/j.ejogrb.2018.05.035
- Chalmers K.J., Madden V.J., Hutchinson M.R., Moseley G.L. Local and Systemic Inflammation in Localized, Provoked Vestibulodynia: A Systematic Review. Obstet. Gynecol. 2016;128:337–347. doi: 10.1097/AOG.0000000000001510
- Masterson BJ, Galask RP, Ballas ZK. Natural killer cell function in women with vestibulitis. J Reprod Med. 1996 Aug;41(8):562-8.
- Ting A.Y., Blacklock A.D., Smith P.G. Estrogen Regulates Vaginal Sensory and Autonomic Nerve Density in the Rat1. Biol. Reprod. 2004;71:1397–1404. doi: 10.1095/biolreprod.104.030023
- Rowen T., Goldstein A. Nosology and epidemiology of dyspareunia and vulvodynia. In: Goldstein I., Clayton A., Goldstein A., Kim N., Kingsberg S., editors. Textbook of Female Sexual Function and Dysfunction. WILEY Blackwell; Hoboken, NJ, USA: 2018. pp. 247–256.
- Burrows L.J., Basha M., Goldstein A.T. The effects of hormonal contraceptives on female sexuality: A review. J. Sex. Med. 2012;9:2213–2223. doi: 10.1111/j.1743-6109.2012.02848.x
- Bazin S., Bouchard C., Brisson J., Morin C., Meisels A., Fortier M. Vulvar vestibulitis syndrome: An exploratory case-control study. Obstet. Gynecol. 1994;83:47–50.
- Reed B.D., Harlow S.D., Legocki L.J., Helmuth M., Haefner H.K., Gillespie B.W., Sen A. Oral contraceptive use and risk of vulvodynia: A population-based longitudinal study. BJOG Int. J. Obstet. Gynaecol. 2013;120:1678–1684. doi: 10.1111/1471-0528.12407
- Burrows L.J., Goldstein A.T. The Treatment of Vestibulodynia with Topical Estradiol and Testosterone. Sex. Med. 2013;1:30–33. doi: 10.1002/sm2.4
- Nohales-Alfonso F., Duarte-Pérez M., Vazquez-Rodriguez S., García-Gamón M., Bas-Esteve E. Eficacia de la combinacion de estrogenos y androgenos locales en el tratamiento del dolor vulvar asociado al sindrome genitourinario de la menopausia. Datos preliminares. Toko-Gin Pract. 2020;79:120–125.
- Weström L.V., Willén R. Vestibular Nerve Fiber Proliferation in Vulvar Vestibulitis Syndrome. Obstet. Gynecol. 1998;91:572–576. doi: 10.1097/00006250-199804000-00017
- King M., Rubin R., Goldstein A.T. Current Uses of Surgery in the Treatment of Genital Pain. Curr. Sex. Heal. Rep. 2014;6:252–258. doi: 10.1007/s11930-014-0032-8
- Kliethermes C.J., Shah M., Hoffstetter S., Gavard J.A., Steele A. Effect of Vestibulectomy for Intractable Vulvodynia. J. Minim. Invasive Gynecol. 2016;23:1152–1157. doi: 10.1016/j.jmig.2016.08.822
- Tympanidis P., Terenghi G., Dowd P. Increased innervation of the vulval vestibule in patients with vulvodynia. Br. J. Dermatol. 2003;148:1021–1027. doi: 10.1046/j.1365-2133.2003.05308.x
- Morin M., Bergeron S., Khalifé S., Mayrand M., Binik Y.M. Morphometry of the Pelvic Floor Muscles in Women With and Without Provoked Vestibulodynia Using 4D Ultrasound. J. Sex. Med. 2014;11:776–785. doi: 10.1111/jsm.12367
- Shafik A. The Role of the Levator Ani Muscle in Evacuation, Sexual Performance and Pelvic Floor Disorders. Int. Urogynecol. J. 2000;11:361–376. doi: 10.1007/PL00004028
- Witzeman K., Nguyen R.H., Eanes A., As-Sanie S., Zolnoun D. Mucosal versus muscle pain sensitivity in provoked vestibulodynia. J. Pain Res. 2015;8:549–555. doi: 10.2147/JPR.S85705
- Fontaine F., Dumoulin C., Bergeron S., Mayrand M.-H., Khalifé S., Wadell G., Morin M. Pelvic Floor Muscle Morphometry and Function in Women With Primary and Secondary Provoked Vestibulodynia. J. Sex. Med. 2018;15:1149–1157. doi: 10.1016/j.jsxm.2018.06.001
- Micheletti L., Radici G., Lynch P.J. Is the 2003 ISSVD terminology and classification of vulvodynia up-to-date? A neurobiological perspective. J. Obstet. Gynaecol. 2015;35:788–792. doi: 10.3109/01443615.2015.1019437
- Mascherpa F, Bogliatto F, Lynch PJ, Micheletti L, Benedetto C. Vulvodynia as a possible somatization disorder. More than just an opinion. J Reprod Med. 2007 Feb;52(2):107-10. https://iris.unito.it/retrieve/e27ce426-ae8e-2581-e053-d805fe0acbaa/Vulvodynia%20as%20a%20Possible%20Somatization%20Disorder.%20More%20Than%20Just%20an%20Opinion%202007.pdf
- Alappattu M.J., George S., Robinson M.E., Fillingim R., Moawad N., LeBrun E.W., Bishop M.D. Painful Intercourse Is Significantly Associated with Evoked Pain Perception and Cognitive Aspects of Pain in Women with Pelvic Pain. Sex. Med. 2015;3:14–23. doi: 10.1002/sm2.52
- Sutton K., Pukall C., Wild C., Johnsrude I., Chamberlain S. Cognitive, Psychophysical, and Neural Correlates of Vulvar Pain in Primary and Secondary Provoked Vestibulodynia: A Pilot Study. J. Sex. Med. 2015;12:1283–1297. doi: 10.1111/jsm.12863
- Alappattu M.J., Bishop M.D. Psychological Factors in Chronic Pelvic Pain in Women: Relevance and Application of the Fear-Avoidance Model of Pain. Phys. Ther. 2011;91:1542–1550. doi: 10.2522/ptj.20100368
- American College of Obstetricians and Gynecologists. (2014). Vulvodynia. Frequently Asked Questions (FAQ 127). https://www.acog.org/Patients/FAQs/Vulvodynia
- Bergeron, S., Binik, Y. M., Khalifé, S., Pagidas, K., Glazer, H. I., Meana, M., & Amsel, R. (2001). A randomized comparison of group cognitive-behavioral therapy, surface electromyographic biofeedback, and vestibulectomy in the treatment of dyspareunia resulting from vulvar vestibulitis. Pain, 91, 297–306.
- Foster DC, Kotok MB, Huang LS, Watts A, Oakes D, Howard FM, Poleshuck EL, Stodgell CJ, Dworkin RH. Oral desipramine and topical lidocaine for vulvodynia: a randomized controlled trial. Obstet Gynecol. 2010 Sep;116(3):583-593. doi: 10.1097/AOG.0b013e3181e9e0ab
- Leo, R.J. A systematic review of the utility of anticonvulsant pharmacotherapy in the treatment of vulvodynia pain. J. Sex. Med. 2013, 10, 2000–2008.
- Leo RJ. A systematic review of the utility of anticonvulsant pharmacotherapy in the treatment of vulvodynia pain. J Sex Med. 2013 Aug;10(8):2000-8. doi: 10.1111/jsm.12200
- Brown, C.S.; Bachmann, G.A.; Wan, J.; Foster, D.C.; Gabapentin (GABA) Study Group. Gabapentin for the treatment of vulvodynia: A randomized controlled trial. Obstet. Gynecol. 2018, 131, 1000–1007.
- Bachmann, G.A.; Brown, C.S.; Phillips, N.A.; Rawlinson, L.A.; Yu, X.; Wood, R.; Foster, D.C. Effect of gabapentin on sexual function in vulvodynia: A randomized, placebo-controlled trial. Am. J. Obstet. Gynecol. 2019, 220, 89.e1–89.e8.
- Bergeron, S.; Khalifé, S.; Dupuis, M.-J.; McDuff, P. A randomized clinical trial comparing group cognitivebehavioral therapy and a topical steroid for women with dyspareunia. J. Consult. Clin. Psychol. 2016, 84, 259–268.
- Falsetta, M.L.; Foster, D.C.; Woeller, C.F.; Pollock, S.J.; Bonham, A.D.; Piekna-Przybylska, D.; Maggirwar, S.B.; Haidaris, C.G.; Phipps, R.P. Toll-like receptor signaling contributes to proinflammatory mediator production in localized provoked vulvodynia. J. Low. Genit. Tract Dis. 2018, 22, 52–57.
- Merlino L, Titi L, Pugliese F, D’Ovidio G, Senatori R, Rocca CD, Piccioni MG. Vulvodynia: Pain Management Strategies. Pharmaceuticals. 2022; 15(12):1514. https://doi.org/10.3390/ph15121514
- Lua LL, Hollette Y, Parm P, Allenback G, Dandolu V. Current practice patterns for management of vulvodynia in the United States. Arch Gynecol Obstet. 2017 Mar;295(3):669-674. doi: 10.1007/s00404-016-4272-x
- Reed, B. D. (2006). Vulvodynia: Diagnosis and management. American Family Physician, 73, 1231–1238. https://www.aafp.org/afp/2006/0401/p1231.html
- American College of Obstetricians and Gynecologists. (2011). Vulvodynia. Frequently Asked Questions (FAQ 127). Washington, DC: American College of Obstetricians and Gynecologists. https://www.acog.org/-/media/For-Patients/faq127.pdf?dmc=1&ts=20160817T1318087562
- Haefner, H. K., Collins, M. E., Davis, G. D., Edwards, L., Foster, D. C., Hartmann, E. H., et al. (2005). The vulvodynia guideline. Journal of Lower Genital Tract Disease, 9, 40–51
- Reed, B.D. (2006). Vulvodynia: Diagnosis and management. American Family Physician, 73, 1231–1238.
- Mayo Clinic. Kidney stones: Prevention. https://www.mayoclinic.org/diseases-conditions/kidney-stones/symptoms-causes/syc-20355755
- American College of Obstetricians and Gynecologists. (2011). Vulvodynia. Frequently Asked Questions (FAQ 127). Washington, DC: American College of Obstetricians and Gynecologists. https://www.acog.org/-/media/For-Patients/faq127.pdf?dmc=1&ts=20160817T1318087562





{kind=link}