
What is ambiguous genitalia
Ambiguous genitalia encompasses a variety of disorders labeled as disorders of sex development or alternatively, differences in sex development 1. Ambiguous genitalia is a rare condition in which an infant’s external genitals don’t appear to be clearly either male or female. In a baby with ambiguous genitalia, the genitals may be incompletely developed or the baby may have characteristics of both sexes. The external sex organs may not match the internal sex organs or genetic sex.
Ambiguous genitalia isn’t a disease, it’s a disorder of sex development. Usually, ambiguous genitalia is obvious at or shortly after birth, and it can be very distressing for families. Your medical team will look for the cause of ambiguous genitalia and provide information and counseling that can help guide decisions about your baby’s gender and any necessary treatment.
Disorders of sex development have been defined as congenital conditions in which development of chromosomal, gonadal or anatomical sex is atypical 2, and comprise a wide set of metabolic and anatomic defects and variants that often can result in atypical genital appearance and may lead to emotional and psychological distress if not sensitively addressed.
Early in fetal development, the tissue that will become the gonads (ovaries or testes) is undifferentiated and has the potential to become either ovaries or testes. Gonadal development is the result of a complex interaction between chromosomes and hormones. Humans have 46 chromosomes in each cell of their bodies, or 23 pairs. The 23rd pair determines our gender; females usually have two X chromosomes, while males usually have one X and one Y chromosome. The chromosome complement (karyotype) in humans is usually written: 46 XX or 46 XY.
There is a gene located on the short arm (top half) of the Y chromosome, called “SRY,” which, if present, will cause the undifferentiated gonad to become testes around the sixth week of fetal life. At the same time, shrinkage of what would have been the female reproductive tract occurs. As the testes produce testosterone, the phallus (penis), scrotum and urethra form. Later, during the seventh to eighth month of the pregnancy, the testes will descend into the scrotum.
If there is no SRY gene, the gonad will usually differentiate into an ovary. Likewise, the female reproductive tract will continue to develop, forming the uterus and fallopian tubes. At the same time, shrinkage of what would have become the male reproductive organs occurs.
A variety of genetic, hormonal, and environmental factors may influence development and lead to ambiguous genitalia. There is great variability in how the genitals may appear.
In most cases, ambiguous genitalia in genetic females (babies with 2 X chromosomes) has the following features:
- An enlarged clitoris that looks like a small penis.
- The urethral opening (where urine comes out) can be anywhere along, above, or below the surface of the clitoris.
- The labia may be fused and look like a scrotum.
- The infant may be thought to be a male with undescended testicles.
- Sometimes a lump of tissue is felt within the fused labia, further making it look like a scrotum with testicles.
In a genetic male (1 X and 1 Y chromosome), ambiguous genitalia most often include the following features:
- A small penis (less than 2 to 3 centimeters, or 3/4 to 1 1/4 inches) that looks like an enlarged clitoris (the clitoris of a newborn female is normally somewhat enlarged at birth).
- The urethral opening may be anywhere along, above, or below the penis. It can be located as low as the perineum, further making the infant appear to be female.
- There may be a small scrotum that is separated and looks like labia.
- Undescended testicles commonly occur with ambiguous genitalia.
With a few exceptions, ambiguous genitalia is most often not life-threatening. However, it can create social problems for the child and family. For this reason, a team of experienced specialists, including neonatologists, geneticists, endocrinologists, and psychiatrists or social workers will be involved in the child’s care.
There are a few key terms that are frequently used in describing ambiguous genitalia and disorders of sex development 1:
- Micropenis is defined as penile length <2 standard deviations below the mean, and is based on age. For term infants, the commonly used cutoff is <2.0 cm for stretched penile length. References are available for different ages and gestational ages 3. Stretched penile length is measured along the dorsal surface of the penis, from pubic symphysis to the tip of the glans, with gentle traction. One method involves use of a firm, flat object, such as a tongue depressor, which is pressed against the pubic bone while the penis is gently stretched along the flat surface. A mark is made where the tip of the glans reaches and this length can then be directly measured.
- Clitoromegaly results from hypertrophy of the clitoris and is seen secondary to androgen exposure (virilization). A commonly used definition is a length >1 cm in term female infants, although width is often measured as well 4.
- Hypospadias is a ventral defect in the penile urethra, and is one of the most common genital defects. Incomplete fusion of the urethral folds will lead to hypospadias. This finding can be described by the location of the defect: penile, penoscrotal, scrotal, perineal, etc.
- Labioscrotal fusion describes the fusion or closure of the labioscrotal folds, and is also seen secondary to androgen exposure (virilization) in the fetus. This phenotype can vary as the fusion effect “zippers” up from posterior (inferior) to anterior (superior), reflecting the magnitude of androgen exposure.
- Bifid scrotum can be a more severe variant of labioscrotal fusion with a clear separation of left and right hemi-scrotum, on each side of the midline scrotal raphe.
- Cryptorchidism, also known as undescended testes, can be unilateral or bilateral, and along with hypospadias, are among the most common genital defects. There are two phases of descent: the first phase (intra-abdominal/inguinal, at 10–15 weeks gestation) is androgen-independent and the second phase (inguinoscrotal, at 26–40 weeks gestation) requires testosterone and dihydrotestosterone (DHT) 5. Bilaterality can be a clue to more severe hormonal defect or hypogonadism, though unilateral cryptorchidism can be seen in ovotesticular disorders of sex development or mixed gonadal dysgenesis and chromosomal mosaicism.
There are a number of different causes of ambiguous genitalia, with the most common described below. The cause, in many cases, is not known and the disorder appears to occur by chance.
Causes for ambiguous genitalia includes:
Children who are born with ambiguous genitalia may fall into one of the following groups:
46 XX (genetic females) – children who have:
Normal female internal structures (uterus, ovaries, fallopian tubes), but masculinized external genitalia. The most common cause of 46 XX DSD is congenital adrenal hyperplasia (CAH). Congenital adrenal hyperplasia (CAH) is a serious medical condition which can be associated with severe electrolyte (such as sodium) imbalances.
46 XX disorder of sex development can also result from exposure of the fetus to high levels of male hormones while in utero. This can occur if hormones enter the placenta, such as when the mother receives progesterone to prevent a miscarriage or has a hormone-producing tumor.
46 XY (genetic males) – children with a 46 XY karyotype and one of the following conditions:
- Testes with normal female external genitalia. This is called Androgen Insensitivity Syndrome (AIS) because the baby is not responsive to androgens (testosterone)
- Testes with ambiguous genitalia. This may be caused by a condition called 5-alpha-reductase deficiency. The enzyme 5-alpha reductase is deficient; therefore, it cannot carry out its task of converting testosterone into dihydrotestosterone (DHT), which is necessary for complete masculinization of a male fetus
Ovotesticular disorder of sex development – children who have:
- Both ovarian and testicular tissue
- External genitalia that are partially ambiguous
- Chromosomes that are either 46 XX, 46 XY, or a mixture (referred to as “mosaic”) of the two (46XX/46XY)
Gonadal dysgenesis – children who have:
- An undeveloped gonad
- Internal sex organs that are usually female
- External genitals that may vary between normal female and normal male, with the majority female
- Chromosomes that are 45 X, 46 XY, 46 XX, or a mosaic (such as 45X/46XX)
Figure 1. Ambiguous genitalia baby girl

Footnote: A 53-day-old, 27-weeks’premature female baby girl presents with genitalia that have become more noticeably ambiguous over the preceding several weeks.
[Source 6 ]Normal sex development
The genetic sex of a child is determined at conception. The mother’s egg cell contains an X chromosome, while the father’s sperm cell contains either an X or a Y chromosome. These X and Y chromosomes determine the child’s genetic sex.
Normally, an infant inherits 1 pair of sex chromosomes, 1 X from the mother and 1 X or one Y from the father. The father “determines” the genetic sex of the child. A baby who inherits the X chromosome from the father is a genetic female and has 2 X chromosomes. A baby who inherits the Y chromosome from the father is a genetic male and has 1 X and 1 Y chromosome.
The male and female reproductive organs and genitals both come from the same tissue in the fetus. Ambiguous genitalia can develop if the process that causes this fetal tissue to become “male” or “female” is disrupted. This makes it hard to easily identify the infant as male or female. The extent of the ambiguity varies. Very rarely, the physical appearance may be fully developed as the opposite of the genetic sex. For example, a genetic male may have developed the appearance of a normal female.
How sex organs form in the womb
A baby’s genetic sex is established at conception, based on the sex chromosomes. The mother’s egg contains an X chromosome, and the father’s sperm contains either an X or a Y chromosome. A baby who inherits the X chromosome from the father is a genetic female (two X chromosomes). A baby who inherits the Y chromosome from the father is a genetic male (one X and one Y chromosome).
Male and female sex organs develop from the same tissue. Whether this tissue becomes male organs or female organs depends on the chromosomes and the presence or absence of male hormones.
- In males, a region on the Y chromosome triggers the development of testicles, which produce male hormones. Male genitals develop in response to male hormones from the fetal testicles.
- In a fetus without a Y chromosome — without the effects of male hormones — the genitals develop as female.
Occasionally, a chromosomal abnormality may make determination of genetic sex complex.
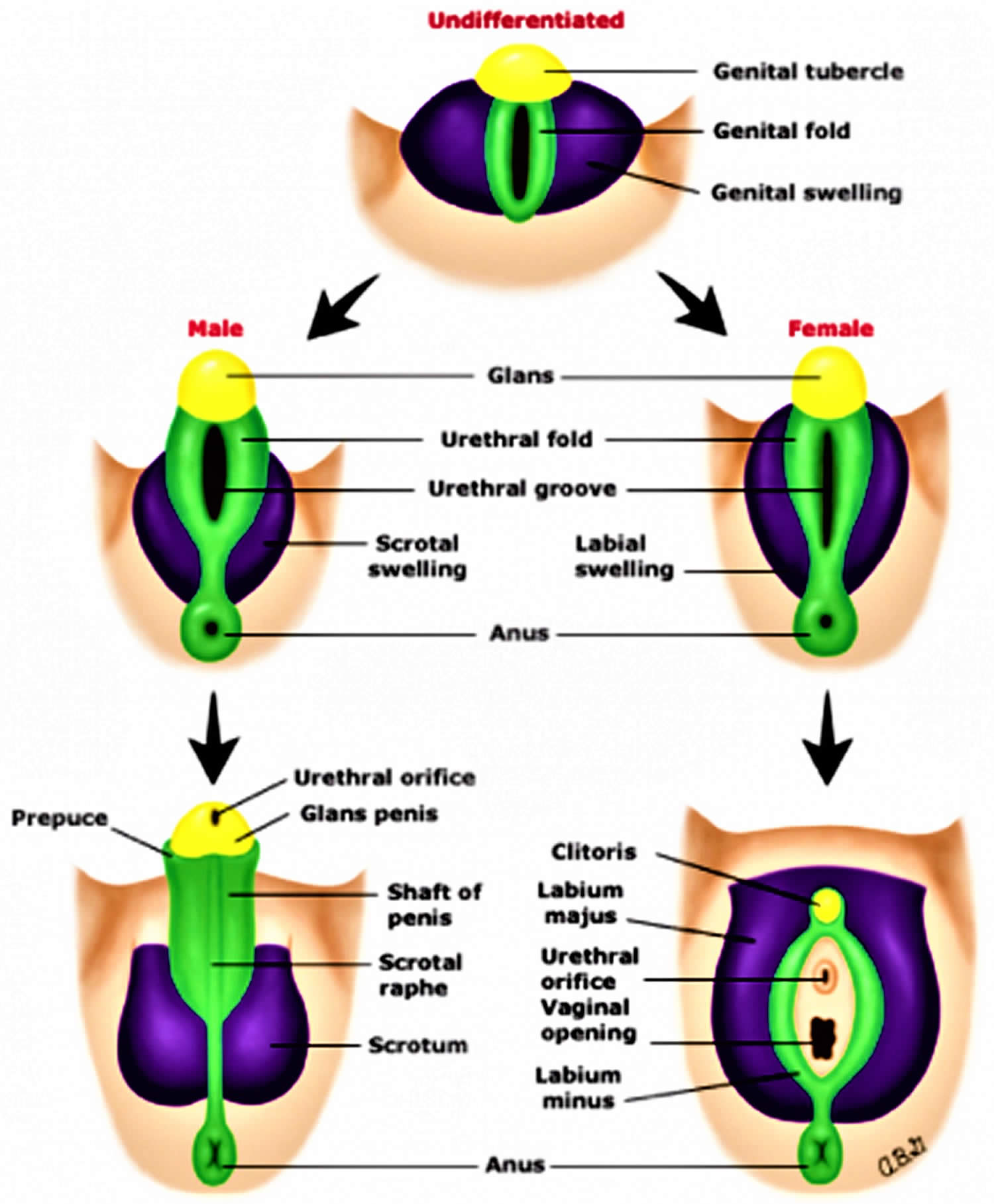
It is important to realize that the gonads (male testis or female ovaries) as well as internal and external genital structures all originate from the same bipotential embryologic tissues, and only through well-choreographed, well-coordinated and localized expression of genes and their gene products does normal sex differentiation and development progress.
The first migration of bipotential primordial germ cells from the yolk sac endoderm to the urogenital ridges leads to the undifferentiated gonad beginning at 4–6 weeks 4. The first 7 weeks of gestation have been considered the indifferent stage, as male and female fetuses would appear grossly indistinguishable from one another, though histologically, changes are well underway. A clear “switch” or decision point signaling the sex determination then occurs leading to the initiation of testicular or ovarian gonadal differentiation. The young bipotential gonad is able to differentiate towards a dedicated male or female pathway, either testis or ovary, respectively, based initially on factors that reside on the Y chromosome (the SRY gene is the prototypical example). Gonadal differentiation then triggers hormonal responses and along with precise and timely gene activation lead to normal/typical external and internal genital development. Scientists have learned about the role of timely and appropriate gene action in normal sex development through gene defects discovered along the pathways associated with disorders of sex development 7.
There is no true “default” pathway; however, androgen exposure determines the external genitalia phenotype. For example, androgen exposure from testosterone and its more potent metabolite dihydrotestosterone (DHT) leads to phallic enlargement and the formation of the penis and the fusion of the labioscrotal folds into a scrotum. The spectrum of phenotypes relating to androgen exposure is seen in many disorders of sex development with varying degrees of genital ambiguity. Different scales or scores have been developed to assess this spectrum, though the most commonly used is the Prader Scale 4, with some alternative scales being developed more recently 8.
With regard to the internal genitalia, the mesonephric duct develops into the Wollfian duct and the internal male genital organs, and the paramesonephric duct develops into the Müllerian duct and the internal female genital organs. In the presence of anti-Müllerian hormone (AMH) secreted by the Sertoli cells of the newly developed testes, the Müllerian structures regress, leaving only the Wollfian structures-epididymis, vas deferens, seminal vesicles, and ejaculatory ducts. Otherwise, the Müllerian structures persist, developing into the fallopian tubes, uterus, cervix, and upper vagina, while the Wollfian structures regress without testosterone trophic effect.
Figure 2. Development of external genitalia
Ambiguous genitalia causes
Ambiguous genitalia primarily occurs when hormone abnormalities during pregnancy interrupt or disturb the fetus’s developing sex organs.
A disruption of the steps that determine sex can result in a mismatch between the appearance of the external genitals and the internal sex organs or the genetic sex (XX or XY).
- A lack or deficiency of male hormones in a genetic male fetus can cause ambiguous genitalia, while exposure to male hormones during development results in ambiguous genitalia in a genetic female.
- Mutations in certain genes can influence fetal sex development and cause ambiguous genitalia.
- Chromosomal abnormalities, such as a missing sex chromosome or an extra one, also can cause ambiguous genitalia.
- In some cases, the cause of ambiguous genitalia may not be determined.
- Ambiguous genitalia can also be a feature of certain rare, complex syndromes that affect many organ systems.
The causes of ambiguous genitalia in newborn period are listed below. The most common cause of ambiguous genitalia is congenital adrenal hyperplasia (CAH). Congenital adrenal hyperplasia (CAH) comprises a collection of different adrenal steroid biosynthetic disorders which can result in wide-ranging signs and symptoms from salt-wasting adrenal crisis in the infant to virilization in young females, delayed puberty in adolescents and even polycystic ovary syndrome (PCOS)-like symptoms (i.e., acne, irregular menses, hirsutism, infertility) in young women. Congenital adrenal hyperplasia (CAH) should be the primary consideration in any virilized infant with non-palpable gonads. Adrenal crisis can lead to shock and death if this condition is not promptly recognized and treated.
In addition to congenital adrenal hyperplasia (CAH) being often recognized as the most common cause of ambiguous genitalia in infants and neonates, other notable causes include partial androgen insensitivity syndrome (Partial AIS or PAIS). Androgen insensitivity syndrome is caused by mutations in the androgen receptor (AR) gene on the X chromosome, and dictates response to androgen such as testosterone or DHT. Complete androgen insensitivity syndrome (CAIS) refers to a complete defect in androgen receptor (AR) and thus no response to androgen, whereas partial androgen insensitivity syndrome (PAIS) refers to a partial defect and thus partial activity in the androgen receptor (AR) and the androgen response. Complete androgen insensitivity syndrome (CAIS) often presents with primary amenorrhea in adolescent female, and since there is no androgen effect it does not lead to genital ambiguity. Complete androgen insensitivity syndrome (CAIS) cases are characterized by female external genitalia but with 46XY karyotype and elevated levels of testosterone, illustrating the complete androgen resistance resulting from the inactive androgen receptor (AR). Partial androgen insensitivity syndrome, being an intermediate and partial mutation, leads to some androgen effect and thus partial virilization. This phenotype then results in ambiguous genitalia in a 46XY infant.
Unfortunately, a great number of ambiguous genitalia cases do not have an identifiable cause, particularly among 46XY disorder of sex development, which highlights the importance of an experienced team with multidisciplinary focus 9. Please note that congenital malformations can also cause ambiguous genitalia, many of which have a primary genetic cause, and others which have a more structural or developmental cause and do not have any hormonal basis. These include VATER/VACTERL associations or cloacal exstrophy 10. VACTERL stands for vertebral defects, anal atresia, cardiac defects, tracheo-esophageal fistula, renal anomalies, and limb abnormalities. People diagnosed with VACTERL association typically have at least three of these characteristic features. Affected individuals may have additional abnormalities that are not among the characteristic features of VACTERL association.
(1) Virilization in 46XX infant
- Excess androgen production
- Congenital adrenal hyperplasia (CAH)
- 21 hydroxylase deficiency
- 11-beta hydroxylase deficiency
- 3-beta hydroxysteroid dehydrogenase (3βHSD) deficiency
- P450 oxidoreductase (POR) deficiency
- Defects in androgen metabolism or signaling
- Placental aromatase deficiency
- Exogenous: hyperandrogenism from maternal source
- Luteoma of pregnancy
- Uncontrolled maternal congenital adrenal hyperplasia (CAH)
- Adrenal virializing tumor
(2) Undervirilization in 46XY infant
- Defects in testosterone metabolism/synthesis
- Smith-Lemli-Opitz syndrome (7-dehydrocholesterol reductase deficiency)
- 5-alpha reductase deficiency
- Leydig cell hypoplasia/agenesis (LH-hCG Receptor defect)
- Congenital adrenal hyperplasia (CAH)
- 3-beta hydroxysteroid dehydrogenase (3βHSD) deficiency
- 17-alpha hydroxylase/17,20 lyase deficiency
- 17-beta hydroxysteroid dehydrogenase (ketosteroid reductase) deficiency
- Steroid acute regulatory (StAR) protein deficiency
- Defects in testosterone action
- Androgen insensitivity syndrome-partial (PAIS)
- Gonadal dysgenesis genetic syndromes (associated with developmental/skeletal anomalies)
- Denys-Drash Syndrome-Frasier syndrome spectrum (WT1)
- Campomelic dysplasia (SOX9)
- Others: SRY, SF1, DAX1, Wnt4
- Exogenous estrogen/progestin exposure
(3) Sex chromosome differences of sex development/other
- Partial and mixed gonadal dysgenesis (usually with mosaicism, such as 45X/46XY)
- Ovotesticular disorder of sex development (karyotype can vary, but most often 46XX)
- Congenital/complex urogenital abnormalities
- Incomplete development of sex anatomy (e.g., vaginal agenesis, gonadal agenesis, or aphallia)
- VATER/VACTERL
- Bladder/cloacal exstrophy
- Aphallia
- Others
(4) Transient
- Prematurity/persistent fetal adrenal
- Preterm ovarian hyperstimulation syndrome
- Genital swelling/edema
Possible causes in genetic females
Causes of ambiguous genitalia in a genetic female may include:
- Congenital adrenal hyperplasia (CAH). Certain forms of this genetic condition cause the adrenal glands to make excess male hormones (androgens).
- Prenatal exposure to male hormones. Certain drugs that contain male hormones or that stimulate production of male hormones in a pregnant woman can cause developing female genitals to become more masculine. A developing baby also may be exposed to excess male hormones if the mother has a disease or condition that causes hormone imbalance.
- Tumors. Rarely, a tumor in the mother can produce male hormones.
Possible causes in genetic males
Causes of ambiguous genitalia in a genetic male may include:
- Impaired testicle development. This may be due to genetic abnormalities or unknown causes.
- Androgen insensitivity syndrome (AIS). In this condition, developing genital tissues don’t respond normally to male hormones made by the testes.
- Abnormalities with testes or testosterone. Various abnormalities can interfere with the testes’ activity. This may include structural problems with the testes, problems with production of the male hormone testosterone or problems with cellular receptors that respond to testosterone.
- 5-alpha-reductase deficiency. This 5-alpha-reductase enzyme defect impairs normal male hormone production.
- Sex chromosome anomalies (e.g., Turner Syndrome, Klinefelter Syndrome, sex chromosome mosaicism)
Risk factors for developing ambiguous genitalia
Family history may play a role in the development of ambiguous genitalia, because many disorders of sex development result from genetic abnormalities that can be inherited. Possible risk factors for ambiguous genitalia include a family history of:
- Unexplained deaths in early infancy
- Infertility, absent menstrual periods or excess facial hair in females
- Genital abnormalities
- Abnormal physical development during puberty
- Congenital adrenal hyperplasia (CAH), a group of inherited genetic disorders that affect the adrenal glands
If your family has a history of these risk factors, consider seeking medical advice before trying to conceive. You may also benefit from genetic counseling.
Ambiguous genitalia symptoms
Your medical team will likely be the first to recognize ambiguous genitalia soon after your baby is born. Occasionally, ambiguous genitalia may be suspected before birth (prenatally). Characteristics can vary in severity, depending on when during genital development the problem occurred and the cause of the disorder.
Babies who are genetically female (with two X chromosomes) may have:
- An enlarged clitoris, which may resemble a penis
- Closed labia, or labia that include folds and resemble a scrotum
- Lumps that feel like testes in the fused labia
Babies who are genetically male (with one X and one Y chromosome) may have:
- A condition in which the narrow tube that carries urine and semen (urethra) doesn’t fully extend to the tip of the penis (hypospadias)
- An abnormally small penis with the urethral opening closer to the scrotum
- The absence of one or both testicles in what appears to be the scrotum
- Undescended testicles and an empty scrotum that has the appearance of a labia with or without a micropenis
Ambiguous genitalia complications
Complications of ambiguous genitalia may include:
- Infertility. Whether people with ambiguous genitalia can have children depends on the specific diagnosis. For example, genetic females with congenital adrenal hyperplasia usually can get pregnant if they so choose.
- Increased risk of certain cancers. Some disorders of sex development are associated with an increased risk of certain types of cancer.
Ambiguous genitalia diagnosis
Ambiguous genitalia is usually diagnosed at birth or shortly after. Doctors and nurses who help with delivery may notice the signs of ambiguous genitalia in your newborn.
History and physical exam assessment in infants with atypical genitalia
History
- Family history (other cases of atypical genitalia or sudden infant death; could point to genetic cause)
- Birth/maternal history (medications/exposures or maternal virilization)
Physical exam
- Overall appearance: vital signs, sick or well appearing (adrenal crisis?)
- Dysmorphic features (genetic syndromes)
- Skeletal malformations (campomelic dysplasia)
- Anatomic malformations (VATER/VACTERL, cloacal exstrophy)
Genital exam
- Phallic structure (micropenis vs. clitoromegaly)
- Gonads (bilateral, unilateral or non-palpable)
- Urethral orifice (hypospadias)
- Labioscrotal folds (symmetry, presence of gonads)
- Anogenital distance (androgen exposure)
- Skin exam: hyperpigmentation (possible ACTH elevation and adrenal failure)
Determining the cause
If your baby is born with ambiguous genitalia, the doctors will work to determine the underlying cause. The cause helps guide treatment and decisions about your baby’s gender. Your doctor will likely begin by asking questions about your family and medical history. He or she will do a physical exam to check for testes and evaluate your baby’s genitalia.
Diagnostic procedures may include a newborn screening test for CAH, hormonal studies and a biopsy of the reproductive organs.
Your medical team will likely recommend these tests:
- A pelvic ultrasound to check for the presence of female reproductive organs
- A genitourethrogram to look at the urethra and vagina if present
- A chromosomal analysis to help determine genetic sex: 46 XX or 46 XY
- Blood tests to measure hormone levels
- 17 hydroxy-progesterone
- Testosterone
- Gonadotropins (LH, FSH)
- Blood tests to analyze chromosomes and determine the genetic sex (XX or XY) or tests for single gene disorders
- Ultrasound of the pelvis and abdomen to check for undescended testes, uterus or vagina
- X-ray studies using a contrast dye to help clarify anatomy
In certain cases, minimally invasive surgery may be necessary to collect a tissue sample of your newborn’s reproductive organs.
Figure 3. Ambiguous genitalia ultrasound (hypospadias)
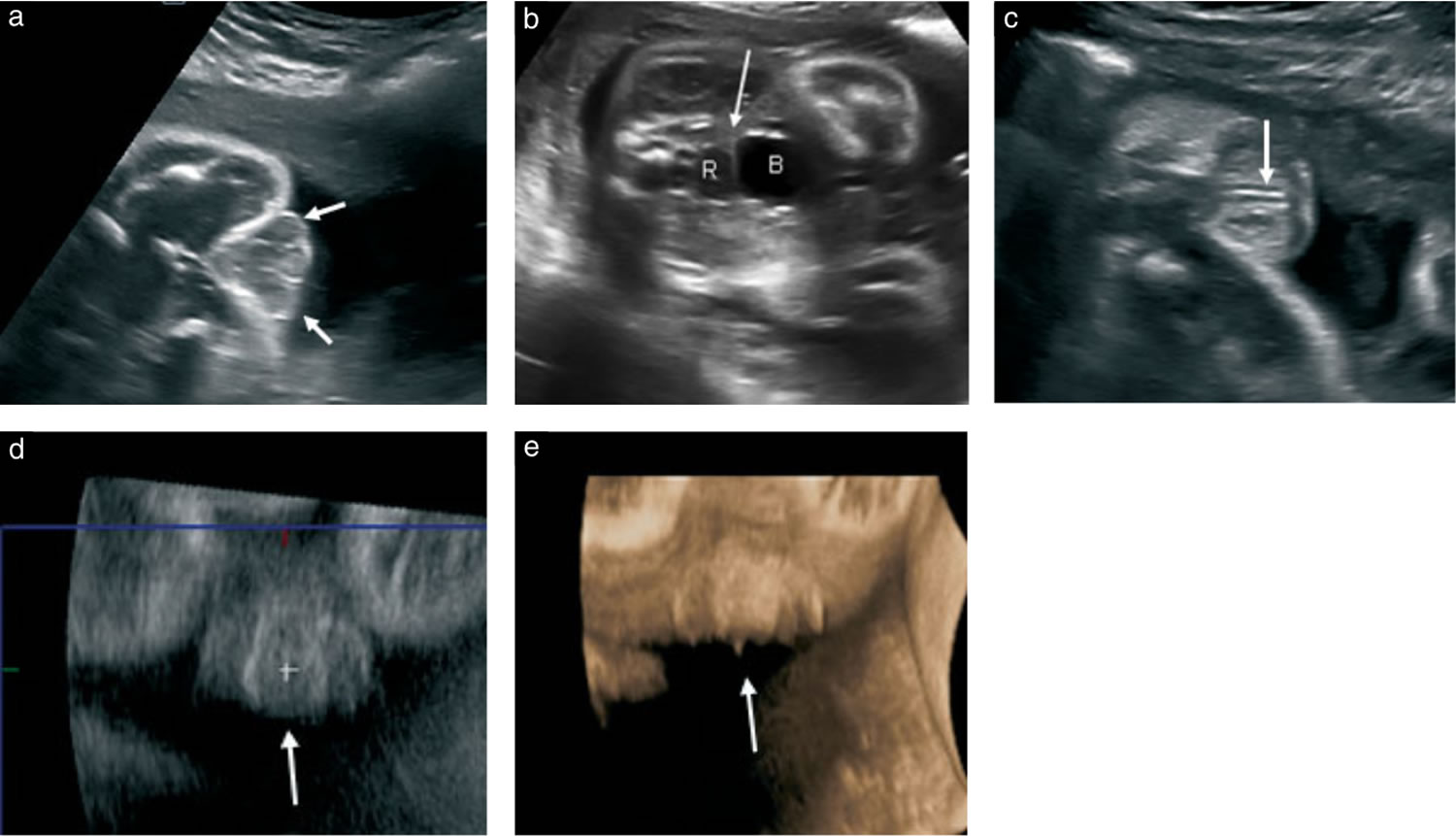
Footnote: Imaging in a case of hypospadias at 29 weeks’ gestation in a male fetus with severe early onset intrauterine growth restriction. Addition of an internal genitalia view in combination with the pregnancy history helped to confirm male gender. At delivery, micturitionoccurred at the penoscrotal junction, consistent with Grade 3 hypospadias with penoscrotal transposition. (a – c) Transverse ultrasoundimages demonstrating ambiguous genitalia. (a) Three structures create the ‘tulip’ sign, withthe short penile shaft nestled between the bifidscrotum (arrows). (b) The thin echogenic line (arrow) is the short rectovesical distance creatinga flat interface with the bladder (B) consistent with male internal genitalia. R, rectum. (c) The urethra is visualizedas an echogenic line (arrow) ending along the base/shaft of the shortpenis, consistent with hypospadias. (d) Coronal reconstruction image demonstrating the micropenis with bulbous ending and downward direction between the bifid scrotum (arrow). (e) Volume-rendered coronal image demonstrating downward direction of the micropenis between the bifid scrotum (arrow).
[Source 11 ]Determining your baby’s gender
Using the information gathered from these tests, your doctor may suggest a gender for your baby. The suggestion will be based on the cause, genetic sex, anatomy, future reproductive and sexual potential, probable adult gender identity, and discussion with you.
In some cases, a family may make a decision within a few days after the birth. However, it’s important that the family wait until test results are completed. Sometimes gender assignment can be complex and the long-term impact can be difficult to predict. Parents should be aware that as the child grows up, he or she may make a different decision about gender identification.
Be thoughtful with the sex assignment: do not rush!
Assigning a sex of rearing is a great responsibility and obligation and should not be rushed. Many factors must be taken into account, and thus it is essential to collect all relevant information while still being expeditious. This includes clinical information (genital appearance as reflecting androgen exposure and future sexual function), laboratory (and cytogenetic) data, as well as imaging, as discussed above. Note also that karyotype data alone is insufficient, and can lead the team astray if used in isolation. Parental views and possible cultural practices must also be respected. Additional considerations include prenatal androgen exposure effects, the future need for hormone replacement, surgical options and fertility potential, even if considered remote 12. Scientists now know that the brain should be considered a “sex organ”: early androgen exposure can have long-lasting effects, and the degree of androgen exposure in utero is believed to be predictive of future masculine behavior and gender identity, though evidence is limited 13. All of these factors named above must be collectively integrated to formulate the most accurate working diagnosis prior to assigning a sex and gender 14.
Ultimately, an individualized approach is essential since long term outcome data are still quite limited. And though uncertainty in the diagnosis is common, there are some general concepts that are widely accepted. For example, 46XX congenital adrenal hyperplasia (CAH) infants should generally be raised as female, unless markedly virilized, in which case the literature is not clear on outcomes. Also, in general 46XY infants with genital ambiguity should generally be assigned as male, especially if there is reasonable evidence of testicular function and androgen responsiveness. To assign such an individual as female constitutes risk 15. Evidence based guidelines are badly needed and future studies will help give better guidance for specific conditions and clinical scenarios, though multicenter networks are making progress 16.
Ambiguous genitalia treatment
Treatment for ambiguous genitalia depends on the type of condition and may include diagnostic, reconstructive surgery, hormone replacement therapy (HRT) or other treatments are used to treat conditions that can cause ambiguous genitalia.
Treatment is decided on a case-by-case basis through discussions with the family. Our team of providers will help each family decide what makes the most sense for their child.
Sometimes, the parents must choose whether to raise the child as male or female (regardless of the child’s chromosomes). This choice can have a big social and psychological impact on the child, so counseling is most often recommended.
In general, most individuals that are 46 XY disorder of sex development make up identify as males in adulthood, and should be raised as such. Exceptions include androgen insensitivity syndrome (AIS) and complete gonadal dysgenesis.
It is often technically easier to treat (and therefore raise) the child as female. This is because it is easier for a surgeon to make female genitalia than it is to make male genitalia. Therefore, sometimes this is recommended even if the child is genetically male. However, this is a difficult decision. You should discuss it with your family, your child’s provider, the surgeon, your child’s endocrinologist, and other health care team members.
For many children with disorder of sex development, long-term medical and surgical care may not be necessary. Common exceptions are children with congenital adrenal hyperplasia (CAH) who will require lifelong endocrine care and children who will require hormone replacement.
All children with disorder of sex development, however, may be at greater risk for psychosocial distress over time. For that reason doctors recommend ongoing, routine follow-up with your psychologist at least yearly to identify concerns early, address the child’s questions throughout childhood and adolescence, and provide needed support about body image, gender identity and peer interactions (e.g., dating), as appropriate.
With regard to psychosexual development, it is now becoming more understood that sex and gender, while having much overlap, is not the same. In addition, the concept of gender itself is being broadened, and reference has been made to a spectrum of gender expression and identity. The so-called “genderbread person”, an infographic and learning tool popularized on social media is one model to understand this wide phenotypic variation 17. While designed as a free online resource for understanding and conceptualizing differences and variations in gender identity, gender expression, and anatomical sex, it can also help facilitate a discussion of gender vs. sex either in the context of transgender medical care or in disorder of sex developments 17. Cases of either dissatisfaction with assigned gender or gender dysphoria are not rare, and these require the care of specialists experienced in managing gender dysphoria. Key points of advice for health care providers are summarized in Table 1.
Table 1. Top five key points in the early management of ambiguous genitalia or atypical genitalia
| (I) Exam: check for gonads; assess androgen effect |
| (II) Diagnostics: check labs for hormone/androgen levels, gonadotropins |
| ❖ The first several days of life are a critical time period for capturing hormone levels while they are still high yield. Delaying will miss this window |
| (III) Genetics: check chromosomes/karyotype |
| ❖ While not a perfectly specific test, chromosomes are still very helpful in working through the differential diagnosis |
| (IV) Assigning sex (sex of rearing): engage the family. Stay calm. Do not rush |
| ❖ Experts know that open, bidirectional discussion is of great value for families |
| ❖ First impressions matter: set a positive, respectful and sensitive tone |
| ❖ Allow enough time for discussion and questions |
| (V) Mobilize your multidisciplinary gender/disorder of sex development team* |
| ❖ A multidisciplinary care team can help minimize psychological trauma for families |
| ❖ Team should be comprised of various members with expertise and experience in disorder of sex development care, and may include the following disciplines: |
| ⬥ Core group |
| ⬥ Endocrinology |
| ⬥ Urology/surgery |
| ⬥ Psychology/psychiatry |
| ⬥ Social work |
| ⬥ Additional resources |
| ⬥ Genetics |
| ⬥ Gynecology |
| ⬥ Neonatology |
| ⬥ Medical ethics |
| ⬥ Nursing |
Footnote: *communication with primary care physician should be ongoing.
[Source 1 ]Once you and your doctor have chosen a gender for your baby, you may choose to begin treatment for ambiguous genitalia. The goal of treatment is long-term psychological and social well-being, as well as to enable sexual function and fertility to the greatest extent possible. When to begin treatment depends on your child’s specific situation.
Ambiguous genitalia is uncommon and complex, and it may require a team of experts. The team might include a pediatrician, neonatologist, pediatric urologist, pediatric general surgeon, endocrinologist, geneticist, and psychologist or social worker.
Medications
Hormone medications may help correct or compensate for the hormonal imbalance. For example, in a genetic female with a slightly enlarged clitoris caused by a minor to moderate case of congenital adrenal hyperplasia, proper levels of hormones may reduce the size of the tissue. Other children may take hormones around the time they would normally experience puberty.
Psychological issues
Optimizing psychosocial and psychosexual well-being
The need for broad and longitudinal psychological support cannot be overstated. Psychological issues can be dynamic along the age scale through infant, childhood, adolescent and adult developmental phases. Beginning in infancy, the confusion surrounding the diagnosis and sex assignment is long lasting and can be traumatic. Then later in childhood and progressing through adolescence and adulthood, themes of stigma, secrecy, and shame are common and intervention by experienced mental health providers for individual and family can provide much needed support.
Perhaps the ultimate goal of the sex assignment is that it eventually aligns with the individual’s gender identity, in order to foster a happy, productive and well-adjusted adult. Ideally this goal should also include optimized fertility potential and adult sexual function. Fertility prognosis has generally been dismal for many disorder of sex developments, though assisted reproductive technologies continue to improve and a recent study suggested that germ cells may be present in many infants with a variety of disorder of sex developments 12. Further, sexual function has often been compromised, sometimes thought to be related to surgical intervention. In addition to issues of stigmatization, these factors have contributed to high rates of dissatisfaction with medical and surgical care, leading to mistrust as well as increased depression and other mental health concerns. Parental stress has also been increasingly identified as a critical factor as well 18. For these reasons psychological support is crucial. In addition to resources within the multidisciplinary clinic team, there are many support groups available 18.
Ambiguous genitalia surgery
Though the history of surgery in disorder of sex development is filled with controversy and regret, surgical intervention has an important role in certain circumstances. The major indications for surgery in disorder of sex development are gonadectomy (generally to mitigate increased risk of malignancy) and genital reconstructive surgery, and both carry significant controversy. Additional goals of surgery, however, are to optimize future sexual function, facilitate options for future reproduction, minimize risk of urinary tract infection, and to avoid stigmatization related to atypical anatomy 19, though many of these points carry some controversy as well.
In children with ambiguous genitalia, surgery may be used to:
- Preserve normal sexual function
- Create genitals that appear more typical
The timing of surgery will depend on your child’s specific situation. Some doctors prefer to postpone surgery done solely for cosmetic reasons until the person with ambiguous genitalia is mature enough to participate in the decision about gender assignment.
For girls with ambiguous genitalia, the sex organs may work normally despite the ambiguous outward appearance. If a girl’s vagina is hidden under her skin, surgery in childhood can help with sexual function later. For boys, surgery to reconstruct an incomplete penis may normalize appearance and make erections possible. Surgery to reposition the testes into the scrotum may be required.
Results of surgery are often satisfying, but repeat surgeries may be needed later. Risks include a disappointing cosmetic result or sexual dysfunction, such as an impaired ability to achieve orgasm.
Gonadectomy
There is increased risk of neoplasm in dysgenetic gonads carrying Y chromosome material, and in sex chromosome disorder of sex developments such as mixed/partial gonadal dysgenesis. Malignant transformation can occur if resection is not pursued in a timely manner. While resection of the gonads to prevent the formation of these gonadal tumors (i.e., gonadoblastoma or dysgerminoma) is a reasonable consideration, there is believed to be time to deliberate since they usually do not occur in the first few years of life. In addition, potential function of that gonad (from a hormone production and fertility perspective) should be considered. In some cases, for example, waiting until adolescence can allow for spontaneous puberty to occur and avoid the need for pubertal induction hormone therapy. Importantly though, there may be future ethical or medicolegal implications, since it can be viewed as a sterilization procedure 20.
Reconstructive surgery
This type of surgery includes feminizing procedures for CAH, such as clitoral reduction and vaginoplasty, but also includes corrective repair in the male, for hypospadias and cryptorchidism. Previous guidelines (including the 2005 Chicago consensus) emphasized that feminizing reconstructive surgery should only be considered for more severe cases of virilization (Prader scores III, IV and V) 21. However, more recently some human rights groups have called for a moratorium on genital surgery 22, with the general recommendation to defer surgery until the individual is of age to decide for themselves. This complex topic will continue to foster controversy, since there is limited evidence for both sides of the debate, and this highlights the importance of open and transparent dialogue between the individual, family and team 23.
Prior to undergoing any procedure, it is important to have a thorough and open dialogue with the family (and patient, whenever possible) to avoid unnecessary and irreversible surgery. In addition, clear communication is needed to prevent unrealistic expectations regarding the timing of surgery and of anatomy following reconstruction 24.
Surgery for purely cosmetic reasons should be deferred until the individual has the knowledge to make an educated decision on their gender identity and external genitalia.
Vaginoplasty if the child is reared as female may be beneficial because of improved functional outcomes in adulthood if the surgery is performed early. Clitoroplasy can be delayed until the child can provide input, and often because the CAH improves as the child ages.
Coping and support
If your baby is diagnosed with ambiguous genitalia, you may worry about your child’s future. Mental health professionals can help you deal with this difficult and unexpected challenge. Ask your child’s doctor for a referral to a mental health professional who has experience helping people in your situation.
In addition to ongoing counseling for your family and your child, you may benefit from a support group, either in person or online. Your child can benefit from ongoing counseling by mental health professionals and participation in support groups into adulthood.
Not knowing the gender of your newborn immediately can turn a hoped-for celebration into a stressful crisis. Your medical team will provide you with updates and information as quickly as possible to help settle any questions about your child’s health.
Consider delaying a formal announcement of the birth until testing is complete and you’ve developed a plan with advice from your medical team. Give yourself some time to learn and think about the issue before answering difficult questions from family and friends.
References- Indyk JA. Disorders/differences of sex development (DSDs) for primary care: the approach to the infant with ambiguous genitalia. Transl Pediatr. 2017;6(4):323-334. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5682373/
- Lee PA, Houk CP, Ahmed SF, et al. Consensus statement on management of intersex disorders. Pediatrics 2006;118:e488-500. 10.1542/peds.2006-0738
- Feldman KW, Smith DW. Fetal phallic growth and penile standards for newborn male infants. J Pediatr 1975;86:395-8. 10.1016/S0022-3476(75)80969-3
- Sperling M. Pediatric Endocrinology. 4th ed. Philadelphia, Pennsylvania: Saunders Elsevier, 2014.
- Thorup J, McLachlan R, Cortes D, et al. What is new in cryptorchidism and hypospadias—a critical review on the testicular dysgenesis hypothesis. J Pediatr Surg 2010;45:2074-86. 10.1016/j.jpedsurg.2010.07.030
- Premature Baby Girl with Ambiguous Genitalia. Stephanie S. Crossen, Cheryl Hanna, JoDee M. Anderson. NeoReviews Jul 2013, 14 (7) e377-e382; DOI: 10.1542/neo.14-7-e377
- Yatsenko SA, Witchel SF. Genetic approach to ambiguous genitalia and disorders of sex development: What clinicians need to know. Semin Perinatol 2017;41:232-43. 10.1053/j.semperi.2017.03.016
- Ahmed SF, Khwaja O, Hughes IA. The role of a clinical score in the assessment of ambiguous genitalia. BJU Int 2000;85:120-4. 10.1046/j.1464-410x.2000.00354.x
- Parisi MA, Ramsdell LA, Burns MW, et al. A gender assessment team: Experience with 250 patients over a period of 25 years. Genet Med 2007;9:348-57. 10.1097/GIM.0b013e3180653c47
- Hutson JM, Grover SR, O’Connell M, et al. Malformation syndromes associated with disorders of sex development. Nat Rev Endocrinol 2014;10:476-87. 10.1038/nrendo.2014.83
- Diagnostic approach in prenatally detectedgenital abnormalities. Ultrasound Obstet Gynecol2010;35: 637 – 646 DOI:10.1002/uog.7679 https://obgyn.onlinelibrary.wiley.com/doi/pdf/10.1002/uog.7679
- Finlayson C, Fritsch MK, Johnson EK, et al. Presence of germ cells in disorders of sex development: Implications for fertility potential and preservation. J Urol 2017;197:937-43. 10.1016/j.juro.2016.08.108
- Arboleda VA, Sandberg DE, Vilain E. DSDs: genetics, underlying pathologies and psychosexual differentiation. Nat Rev Endocrinol 2014;10:603-15. 10.1038/nrendo.2014.130
- Meyer-Bahlburg HF, Baratz Dalke K, Berenbaum SA, et al. Gender assignment, reassignment and outcome in disorders of sex development: Update of the 2005 consensus conference. Horm Res Paediatr 2016;85:112-8. 10.1159/000442386
- Bangalore Krishna K, Houk CP, Lee PA. Pragmatic approach to intersex, including genital ambiguity, in the newborn. Semin Perinatol 2017;41:244-51. 10.1053/j.semperi.2017.03.013
- Lee PA, Wisniewski AB, Baskin L, et al. Advances in diagnosis and care of persons with DSD over the last decade. Int J Pediatr Endocrinol 2014;2014:19 10.1186/1687-9856-2014-19
- The Genderbread Person. https://www.genderbread.org/
- Wisniewski AB, Sandberg DE. Parenting Children with Disorders of Sex Development (DSD): A Developmental Perspective Beyond Gender. Horm Metab Res 2015;47:375-9. 10.1055/s-0034-1398561
- Mouriquand PD, Gorduza DB, Gay CL, et al. Surgery in disorders of sex development (DSD) with a gender issue: If (why), when, and how? J Pediatr Urol 2016;12:139-49. 10.1016/j.jpurol.2016.04.001
- Brain CE, Creighton SM, Mushtaq I, et al. Holistic management of DSD. Best Pract Res Clin Endocrinol Metab 2010;24:335-54. 10.1016/j.beem.2010.01.006
- Hughes IA, Houk C, Ahmed SF, et al. Consensus statement on management of intersex disorders. Arch Dis Child 2006;91:554-63. 10.1136/adc.2006.098319
- https://www.hrw.org/report/2017/07/25/i-want-be-nature-made-me/medically-unnecessary-surgeries-intersex-children-us
- Karkazis K, Rossi WC. Ethics for the Pediatrician: Disorders of Sex Development: Optimizing Care. Pediatr Rev 2010;31:e82-5. 10.1542/pir.31-11-e82
- Hughes IA, Houk C, Ahmed SF, et al. Consensus statement on management of intersex disorders. J Pediatr Urol 2006;2:148-62. 10.1016/j.jpurol.2006.03.004





{kind=link}