What is shortness of breath Shortness of breath is also called dyspnea or breathlessness, is an intense tightening in your chest, air hunger, a feeling
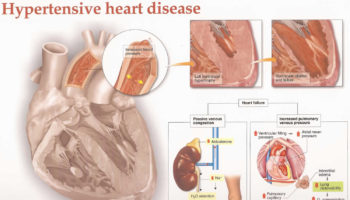
What is hypertensive heart disease Hypertensive heart disease refers to heart problems that occur because of high blood pressure that is present over a long
What is hypersensitivity pneumonitis Hypersensitivity pneumonitis also known as extrinsic allergic alveolitis, bird fancier’s lung, farmer’s lung, hot tub lung or humidifier lung, is a
What are granulocytes Granulocytes are mature infection-fighting white blood cells that have granules in their cytoplasm that show up as spots under the microscope. Granulocytes
What is Goodpasture syndrome Goodpasture syndrome also called pulmonary-renal syndrome, is a rare autoimmune disorder that involves your kidneys and lungs. Goodpasture syndrome is fatal unless
What is heat intolerance Heat intolerance is a feeling of being overheated when the temperature around you rises. Heat intolerance is also defined as the
{kind=link}









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}