What is alkaptonuria Alkaptonuria is a rare genetic metabolic disorder characterized by the accumulation of homogentisic acid in the body. Affected individuals lack enough functional
What is ambiguous genitalia Ambiguous genitalia encompasses a variety of disorders labeled as disorders of sex development or alternatively, differences in sex development ((Indyk JA.
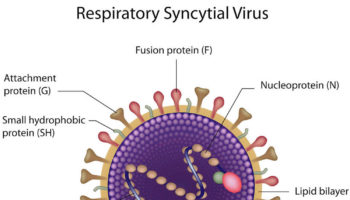
What is respiratory syncytial virus Respiratory syncytial virus (RSV) is a common respiratory virus that infects your airways and lungs that usually causes mild, cold-like
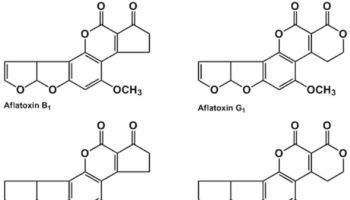
What is aflatoxin Aflatoxins are toxins produced by a Aspergillus flavus and and the closely related species Aspergillus parasiticus fungus, one of the most abundant soil-borne
What is SHBG SHBG is short for sex hormone binding globulin is also called Testosterone-Estradiol Binding Globulin, SHBG is a glycoprotein that is produced by
What does crystals in urine mean Crystals in urine is also called crystalluria, is a frequent finding in the routine examination of urine sediments. Your urine
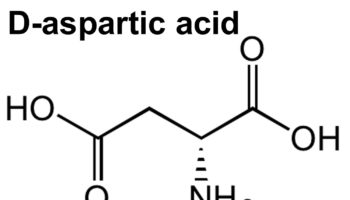
What does d aspartic acid do D-Aspartic acid is an non-essential amino acid that plays an important role in tuning testosterone production in the gonads
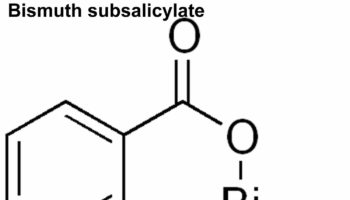
What is bismuth subsalicylate Bismuth subsalicylate is an antacid and anti-diarrhea medication that is used to treat diarrhea, heartburn, nausea, indigestion and upset stomach in adults
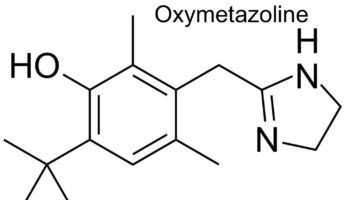
Oxymetazoline nasal spray Oxymetazoline is a a direct acting sympathomimetic vasoconstrictor that works by narrowing swollen blood vessels. Oxymetazoline works by narrowing the blood vessels in
{kind=link}





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}