
What is Blount’s disease
Blount’s disease is a growth disorder of the shin bone (tibia) in which the lower leg turns inward, making it look like a bowleg. Blount’s disease can affect people at any time during the growing process, but it’s more common in kids younger than 4 and in teens.
There are two types of Blount’s disease (early-onset and late-onset), based on whether symptoms begin before or after four years of age 1. Blount’s disease may occur in one or both legs and can lead to shortening of the affected leg and other changes within bones of the legs.
Infantile Blount disease or early-onset (occurring before 4 years of age) usually involves both legs. It is estimated that about 50-60% of individuals with infantile Blount disease have symptoms in both legs 2. Individuals with late-onset Blount disease are more likely to have only one affected leg 3.
The epidemiology of Blount’s disease is not well documented. Large series of patients with Blount disease indicates the estimated prevalence is less than 1% 4 in the United States. Predisposition for Blount’s disease has been attributed to race, genetics, age at walking, and obesity. Blount’s disease has increased prevalence in the overweight African American population and in the Scandinavian population. Increased occurrence has been seen in South Africa 5.
The cause of Blount’s disease is not well understood and remains controversial 6; however, a variety of hereditary and genetic factors are likely involved. The condition is more common among certain populations and is associated with obesity and early walking 6.
In Blount disease, a lot of pressure is put on the growth plate at the top of the tibia. This is called the physis and it’s made out of cartilage, which is weaker than bone. The job of the physis is to allow the bone to lengthen and grow.
But this excess pressure prevents the bone from growing normally. Instead, the lateral (outer) side of the tibia keeps growing but the medial (inner) side of the bone does not. This uneven bone growth causes the tibia to bend outward instead of grow straight.
Blount’s disease is very different from the bowlegs that babies and toddlers have. Their legs are naturally bowed and usually straighten out when they start walking.
But with Blount disease — whether it starts in early childhood or the teen years — the curve gets worse if it’s not treated. So early diagnosis is very important. Treatment may involve bracing and/or surgery 7.
In a child under the age of 2 years, it may be impossible to distinguish infantile Blount’s disease from physiologic genu varum. By the age of 3 years, however, the bowing will worsen and an obvious problem can often be seen in an x-ray.
Figure 1. Blount disease
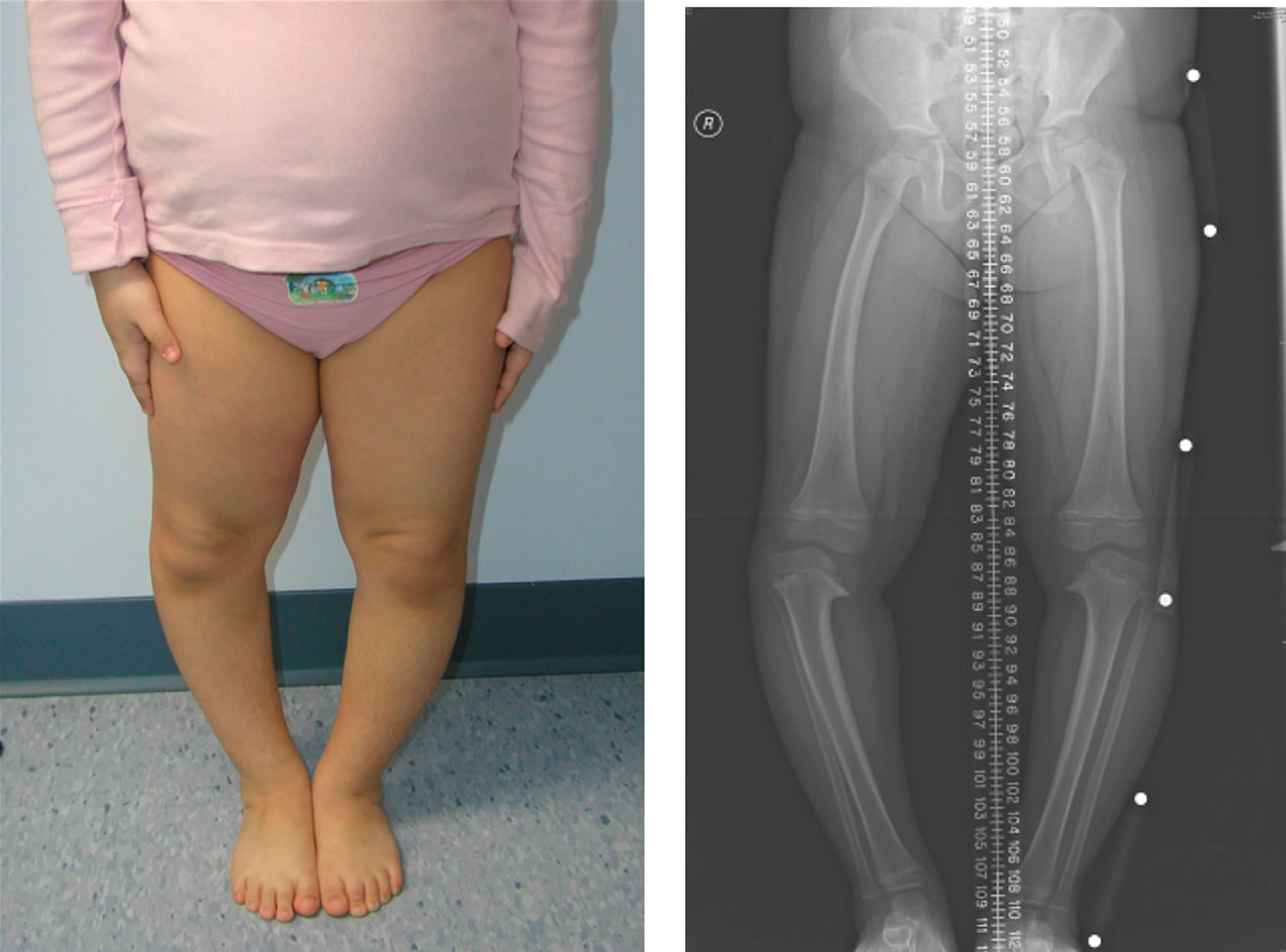
Footnote: 5 year old girl with bilateral early-onset Blount disease
[Source 8 ]Is Blount disease hereditary?
The cause of Blount disease remains controversial, but it is most likely secondary to a combination of hereditary and developmental factors 6.
Blount disease has an increased incidence in overweight children who walk at an early age 9. These findings have lead to theories that mechanical overload of the proximal tibia contribute to Blount disease. The mechanical overload of the physis is attributed to obesity and varus deformity 10. However, mechanical factors in isolation cannot cause Blount disease, given that the infantile form is often seen in children with normal weight 6.
Blount disease has a genetic component as well, but a direct pattern of inheritance has not been shown. Clearly, the cause of Blount disease is multifactorial and may differ in the early- and late-onset forms of Blount disease 6.
An association between vitamin D deficiency and Blount disease has been suggested 11, but an independent association between the two, without regard to obesity, has not been proved 12.
Blount’s disease causes
Blount’s disease occurs in young children and adolescents. The cause is unknown. It is thought to be due to the effects of weight on the growth plate 10. The inner part of the shin bone, just below the knee, fails to develop normally.
Most people who get Blount disease are overweight or gained weight very quickly.
Unlike bowlegs, which tend to straighten as the child develops, Blount disease slowly gets worse. It can cause severe bowing of one or both legs.
Blount’s disease is more common among African American children. Blount’s disease is also associated with obesity and walking at an early age 9 and those with a family member who had it.
Risks factors for Blount disease
Most kids who get Blount disease are overweight or gained weight very quickly. It’s also more common in people of African heritage, kids who started walking at an early age, and those with a family member who had it.
In Blount disease, a lot of pressure is put on the growth plate (an area of growing bone tissue) at the top of the tibia. As a result, the bone can’t grow normally. The lateral (outer) side of the tibia keeps growing but the medial (inner) side of the bone does not.
This uneven bone growth causes the tibia to bend outward instead of grow straight. One leg may also become slightly shorter than the other.
Blount’s disease signs and symptoms
The most obvious sign a person might have Blount disease is bowing of the leg below the knee. In young kids this is usually not painful, though it can affect the way they walk. For preteens and teens, Blount disease may cause knee pain that gets worse with activity (it may feel like a growing pain in the knee area). The pain may come and go. Most teens have already been taking over-the-counter pain relievers for it by the time they see a doctor.
The tibia can be rotated as well as bowed, causing a condition called in-toeing (when the feet point inward instead of straight out).
One or both of the lower legs turn inward. This is called “bowing.” It may:
- Look the same on both legs
- Occur just below the knee
- Rapidly get worse
It can cause other problems, too, mainly due to the way the lower leg bears the weight of the body. The tibia can be rotated as well as bowed, causing a condition called in-toeing (when the feet point inward instead of straight out).
Over time (usually decades), Blount disease can lead to arthritis of the knee joint and in severe cases, trouble walking. One leg may also become slightly shorter than the other.
Blount’s disease prognosis
In long-term follow-up of infantile Blount disease, Doyle et al 13 found that the outcome depends on the patient’s age and the severity of deformity at the time of intervention. An understanding of the natural history of Blount disease is important for treatment. The prognosis in the infantile form of Blount disease must be considered separately from that in the adolescent Blount disease. Infantile Blount disease has a good prognosis, and recurrence rates of deformity are low when treated at a young age and early stage.
Untreated infantile Blount disease is believed to be progressive. While partial or complete regression may occur in the early stages of Blount disease, later stages continue to progress and eventually lead to joint degeneration. In the late-onset form of Blount disease, regression does not occur and the varus deformity may worsen over time. These patients may eventually develop complications as a result of joint malalignment.
Data on long-term follow-up of Blount disease are limited, and further studies are needed to characterize the relationship between the deformity and the development of arthroses 13. Severity of deformity has been shown to correlate with severity proximal tibial deformity, and poor outcomes appear to be related to the degree of physeal damage 14. With advances in treatment, retrospective studies on different treatment groups may show whether progression to arthrosis is a significant concern.
If being overweight caused the Blount disease, it’s important for parents to help their child reach and maintain a healthy weight. This can reduce stress on the bones and joints and prevent other long-term problems from weight gain (like type 2 diabetes and heart disease).
If you need help getting your child to adopt a healthier lifestyle that includes a balanced diet and exercise, talk to your doctor. Most kids who are treated for Blount disease get better and have active lives.
Blount’s disease possible complications
Failure to treat Blount disease may lead to progressive deformity. The condition may lead to differences in leg lengths, which can result in disability if not treated.
Blount disease may come back after surgery, especially in younger children.
Blount disease diagnosis
If your child’s legs start bowing — especially if he/she also has knee pain that seems to be getting worse and can’t be traced to an injury — your doctor may consider Blount disease as a possibility. If so, your doctor will refer you to an orthopedic specialist (a doctor who treats bone problems).
Mild bone changes can be hard to spot in kids younger than 2 because their bowed legs might be normal and straighten out on their own. It’s easier for doctors to diagnose Blount disease in kids after age 2.
The orthopedic doctor will do a complete physical exam and also take X-rays of your child’s legs. These let the doc look for the abnormal bone growth patterns at the top of the tibia that are the telltale sign of Blount disease. They also help the doctor measure how severe the bowing is.
Blount disease treatment
Treatment of Blount disease depends on a child’s age and how curved the bone is.
Usually, doctors will just keep a close eye on the condition in children younger than 2. Kids 2 to 4 years old and those with severe bowing might need leg braces, called KAFOs (knee-ankle-foot orthotics). Knee-ankle-foot orthotics, which go from the thigh to the toes, are created for kids using a mold of their leg. The hope is that the braces gradually shift leg bones to a straighter position over time. However, doctors have differing opinions on KAFOs. If you have questions about them, talk to your doctor.
Older kids and teens, or kids who don’t get better wearing knee-ankle-foot orthotics, might need surgery:
- The surgeon can cut the bone, straighten it, and fasten it with plates and screws. This is called an osteotomy.
- Another procedure can slow or stop the growth of half of the growth plate to allow the other side to catch up and straighten the leg.
- A device called an external fixator can be put on the outside of the leg and attached to the bones after they are cut. It holds the bones in place while gradually straightening the leg.
If surgery is necessary, it will be done under general anesthesia. This means your child will be sedated and asleep and won’t feel anything. Afterward, your child might wear a cast or use crutches and a wheelchair for a while. Physical therapy also might be needed.
Blount disease surgery
Many different types of surgeries can correct Blount disease — some involve cutting the tibia, realigning it, and holding it in place with a plate and screws (this is called an osteotomy); some involve removing the damaged growth plate; and some use a device called an external fixator to hold the bones in place from the outside. If a person’s toes turn in, surgeons may correct the twist that’s causing that, too.
If surgery is necessary, it will be done under general anesthesia (you will be completely asleep and not feel anything). Afterward, you might wear a cast and use crutches for a while. You’ll also probably need physical therapy. The good news is that most teens make a complete recovery.
Recent studies have investigated individual aspects of the surgical management of Blount’s disease including closing wedge tibial osteotomies 15, fibular osteotomy 16, hemi-epiphyseal stapling 17 and different types of external fixators 18.
The medial tibial plateau elevation is performed acutely and there is ongoing debate on the relative merits of iliac crest graft or gradual correction as an alternative. A prospective randomised clinical trial by Zorzi et al 19 compared high tibial opening-wedge osteotomies with and without autologous iliac crest bone grafts. Blinded investigators concluded that all osteotomies had achieved bone union and that the difference in time to union was not statistically significant. The potential complications of bone grafting include infection, pain and failure 20. As patients requiring high degrees of correction often yield less than adequate bone 21, this method is not advocated 22.
Gradual correction has been reported to be a reliable and safe method of treating multi-planar deformities 23. Following a percutaneous osteotomy with progressive opening wedge correction using a modified Wagner monolateral fixator in ten patients (20 tibias) with late-onset Blount’s disease, de Pablos et al 24 noted, apart from one case of under-correction, no major complications. Similar results were noted when Coogan et al 23 reviewed their use of a circular external fixator in eight obese adolescents (12 tibias) undergoing gradual correction. A single case of premature consolidation was noted and this required a repeat osteotomy. The low incidence of neurovascular injury is likely to be due to the avoidance of acute intra-operative traction on the neurovascular structures.
Acute correction in Blount’s disease can be accomplished with a proximal tibial metaphyseal osteotomy 25. A variety of techniques have been suggested, including closing wedge 26, serrated 27, inclined 28, dome 29 and as was done in this study, an opening wedge osteotomy 30. Edwards et al 22 have used an acute opening wedge osteotomy without grafting and have observed uncomplicated union in all cases. Occasionally, this produced a medial metaphyseal prominence. This was not resected and it remodelled with time and did not produce a clinical or cosmetic abnormality 22.
Alternative methods of stabilization have been reported and include smooth pins and wires 31, cast immobilisation, plates and screws 30, inter-fragmentary screws32 and external fixators 32. Chotigavanichaya et al 33 conducted a retrospective review of osteotomies performed for late-onset Blount’s disease. Of these, 34 were cross-pinned while 14 were held with an external fixator. At six years follow-up, the recurrence of varus deformity was 94% in those who were pinned and 72% in those with an external fixator. Following external fixator use in this study, three of eight (37.5%) limbs had recurrence after initial complete correction. This is due to the effect of residual growth in the proximal tibial physis and the procedure has been modified to include formal drill epiphysiodesis at the time of fixator removal. An alternative approach would involve physeal ablation at the time of initial surgery, but this would potentially compromise the stability and viability of the epimetaphyseal fragment and is considered unwise, from a theoretical perspective alone.
Blount disease surgery risks
Regardless of the type of osteotomy and fixation device, there is a potential for serious adverse effects including compartment syndrome and focal neurological injury 34. In this report 22, one patient had mild paraesthesia lasting weeks, while one patient had a long episode of sensory and motor deficit of the peroneal nerve. A retrospective review of 116 children with 129 tibial osteotomies performed by Payman et al 35 noted 35 cases of delayed union, two cases with transient peroneal nerve palsy, one case of nonunion and one case of malunion. More recently, Wilson et al 36 reported a complication rate of 153% following 38 high tibial osteotomies with external fixation in patients with Blount’s disease; both studies highlighted Blount’s disease and obesity as factors increasing the complication rate.
The peroneal nerve is at risk at the time of fibular osteotomy and the recommendation is to perform the osteotomy through an incision that permits sub-periosteal exposure and osteotomy under direct vision. Paradoxically, this may increase the risk of neurapraxia due to a traction injury as seen in transient sensory loss in one patient 22. The site of the proximal fibular osteotomy is determined by the geometry of the tibial deformity and whilst a more distal division would be less likely to injure the peroneal nerve, it would produce a secondary fibular deformity that is frequently associated with local soft-tissue irritation. The fact that the complete peroneal nerve injury recovered without intervention indicates that this was also a traction injury, most likely at the time of fibular osteotomy.
References- Sanjeev Sabharwal. Blount disease. J Bone Joint Surg Am. Jul 01 2009; 91 (7):1758-1776. http://www.ncbi.nlm.nih.gov/pubmed/19571101
- Blount disease. J Am Acad Orthop Surg. 2013 Jul;21(7):408-18. doi: 10.5435/JAAOS-21-07-408. https://journals.lww.com/jaaos/Abstract/2013/07000/Blount_Disease.6.aspx
- Blount Disease. https://emedicine.medscape.com/article/1250420-overview
- Smith CF. Tibia vara (Blount’s disease). J Bone Joint Surg Am. 1982 Apr. 64(4):630-2.
- Bathfield CA, Beighton PH. Blount disease. A review of etiological factors in 110 patients. Clin Orthop Relat Res. 1978 Sep. (135):29-33.
- Blount disease. https://emedicine.medscape.com/article/1250420-overview
- Blount disease. https://medlineplus.gov/ency/article/001584.htm
- Blount disease. J Bone Joint Surg Am. 2009 Jul;91(7):1758-76. doi: 10.2106/JBJS.H.01348. https://www.ncbi.nlm.nih.gov/pubmed/19571101
- Scott AC, Kelly CH, Sullivan E. Body mass index as a prognostic factor in development of infantile Blount disease. J Pediatr Orthop. 2007 Dec. 27(8):921-5.
- Davids JR, Huskamp M, Bagley AM. A dynamic biomechanical analysis of the etiology of adolescent tibia vara. J Pediatr Orthop. 1996 Jul-Aug. 16(4):461-8.
- Montgomery CO, Young KL, Austen M, Jo CH, Blasier RD, Ilyas M. Increased risk of Blount disease in obese children and adolescents with vitamin D deficiency. J Pediatr Orthop. 2010 Dec. 30 (8):879-82.
- Lisenda L, Simmons D, Firth GB, Ramguthy Y, Kebashni T, Robertson AJ. Vitamin D Status in Blount Disease. J Pediatr Orthop. 2016 Jul-Aug. 36 (5):e59-62.
- Doyle BS, Volk AG, Smith CF. Infantile Blount disease: long-term follow-up of surgically treated patients at skeletal maturity. J Pediatr Orthop. 1996 Jul-Aug. 16(4):469-76.
- Hofmann A, Jones RE, Herring JA. Blount’s disease after skeletal maturity. J Bone Joint Surg Am. 1982 Sep. 64(7):1004-9.
- Burton A, Hennrikus W. Complete closing wedge osteotomy for correction of blount disease (tibia vara): A Technique. Am J Orthop 2016;45:16-18.
- Sachs O, Katzman A, Abu-Johar E, Eidelman M. Treatment of adolescent Blount disease using Taylor Spatial Frame with and without fibular osteotomy: Is there any difference? J Pediatr Orthop 2015;35:501-506.
- Schroerlucke S, Bertrand S, Clapp J, Bundy J, Gregg FO. Failure of Orthofix eight-Plate for the treatment of Blount disease. J Pediatr Orthop 2009;29:57-60.
- Mayer SW, Hubbard EW, Sun D, Lark RK, Fitch RD. Gradual Deformity Correction in Blount Disease. J Pediatr Orthop 2016;December 23; Epub ahead of print.
- Zorzi AR, da Silva HG, Muszkat C., et al. Opening-wedge high tibial osteotomy with and without bone graft. Artif Organs 2011;35:301-307.
- Goulet JA, Senunas LE, DeSilva GL, Greenfield ML. Autogenous iliac crest bone graft. Complications and functional assessment. Clin Orthop Relat Res 1997;339:76-81.
- Seagrave RA, Sojka J, Goodyear A, Munns SW. Utilizing reamer irrigator aspirator (RIA) autograft for opening wedge high tibial osteotomy: A new surgical technique and report of three cases. Int J Surg Case Rep 2014;5:37-42
- Edwards TA, Hughes R, Monsell F. The challenges of a comprehensive surgical approach to Blount’s disease. J Child Orthop. 2017;11(6):479-487. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5725776/
- Coogan PG, Fox JA, Fitch RD. Treatment of adolescent Blount disease with the circular external fixation device and distraction osteogenesis. J Pediatr Orthop 1996;16:450-454.
- de Pablos J, Azcárate J, Barrios C. Progressive opening-wedge osteotomy for angular long-bone deformities in adolescents. J Bone Joint Surg [Br] 1995;77-B:387-391.
- Sabharwal S. Blount disease. J Bone Joint Surg [Am] 2009;91-A:1758-1776.
- Schoenecker PL, Johnston R, Rich MM, Capelli AM. Elevation of the medical plateau of the tibia in the treatment of Blount disease. J Bone Joint Surg [Am] 1992;74-A:351-358.
- Hayek S, Segev E, Ezra E, Lokiec F, Wientroub S. Serrated W/M osteotomy. Results using a new technique for the correction of infantile tibia vara. J Bone Joint Surg (Br) 2000;82:1026-1029
- Rab GT. Oblique tibial osteotomy for Blount’s disease (tibia vara). J Pediatr Orthop 1988;8:715-720.
- Miller S, Radomisli T, Ulin R. Inverted arcuate osteotomy and external fixation for adolescent tibia vara. J Pediatr Orthop 2000;20:450-454.
- Martin SD, Moran MC, Martin TL, Burke SW. Proximal tibial osteotomy with compression plate fixation for tibia vara. J Pediatr Orthop 1994;14:619-622.
- Ferriter P, Shapiro F. Infantile tibia vara: factors affecting outcome following proximal tibial osteotomy. J Pediatr Orthop 1987;7:1-7.
- Smith SL, Beckish ML, Winters SC, Pugh LI, Bray EW. Treatment of late-onset tibia vara using afghan percutaneous osteotomy and orthofix external fixation. J Pediatr Orthop 2000;20:606-610.
- Chotigavanichaya C, Salinas G, Green T, Moseley CF, Otsuka NY. Recurrence of varus deformity after proximal tibial osteotomy in Blount disease: long-term follow-up. J Pediatr Orthop 2002;22:638-641.
- Loder RT, Johnston CE II. Infantile tibia vara. J Pediatr Orthop 1987;7: 639-646.
- Payman KR, Patenall V, Borden P, Green T, Otsuka NY. Complications of tibial osteotomies in children with comorbidities. J Pediatr Orthop 2002;22: 642-644.
- Wilson NA, Scherl SA, Cramer KE. Complications of high tibial osteotomy with external fixation in adolescent Blount’s disease. Orthopedics 2007;30: 848-852.





{kind=link}