Bounding pulse
Bounding pulse also known as water hammer pulse, is a forceful pulse with a rapid upstroke and descent or strong throbbing felt over one of the arteries in your body. Bounding pulse is due to a forceful heartbeat. Bounding pulse is seen in many physiological and pathological conditions but is most often associated with aortic regurgitation 1. According to the Framingham study, the prevalence of aortic regurgitation was 4.9%, with moderate or severe regurgitation occurring in 0.5%. Aortic regurgitation is more common in men than in women. Clinical manifestations of the disease peak between the fourth and sixth decades of life 2.
In 1833, Dr. Dominic John Corrigan first described bounding pulse or the water hammer pulse when he saw the visible sudden distention and collapse of the carotid arteries in patients with aortic regurgitation. Dr. Thomas Watson further investigated this palpable pulse in 1844. He compared the findings to the pulse felt when playing with a water hammer toy. During the Victorian era, a water hammer was a toy in which a tube was filled halfway with fluid, and the rest would be a vacuum. The tube could be continuously inverted, and the sound of the impact would sound like a hammer blow 3.
A bounding pulse and rapid heart rate both occur in the following conditions or events:
- Abnormal or rapid heart rhythms
- Anemia
- Anxiety
- Long-term (chronic) kidney disease
- Heart failure
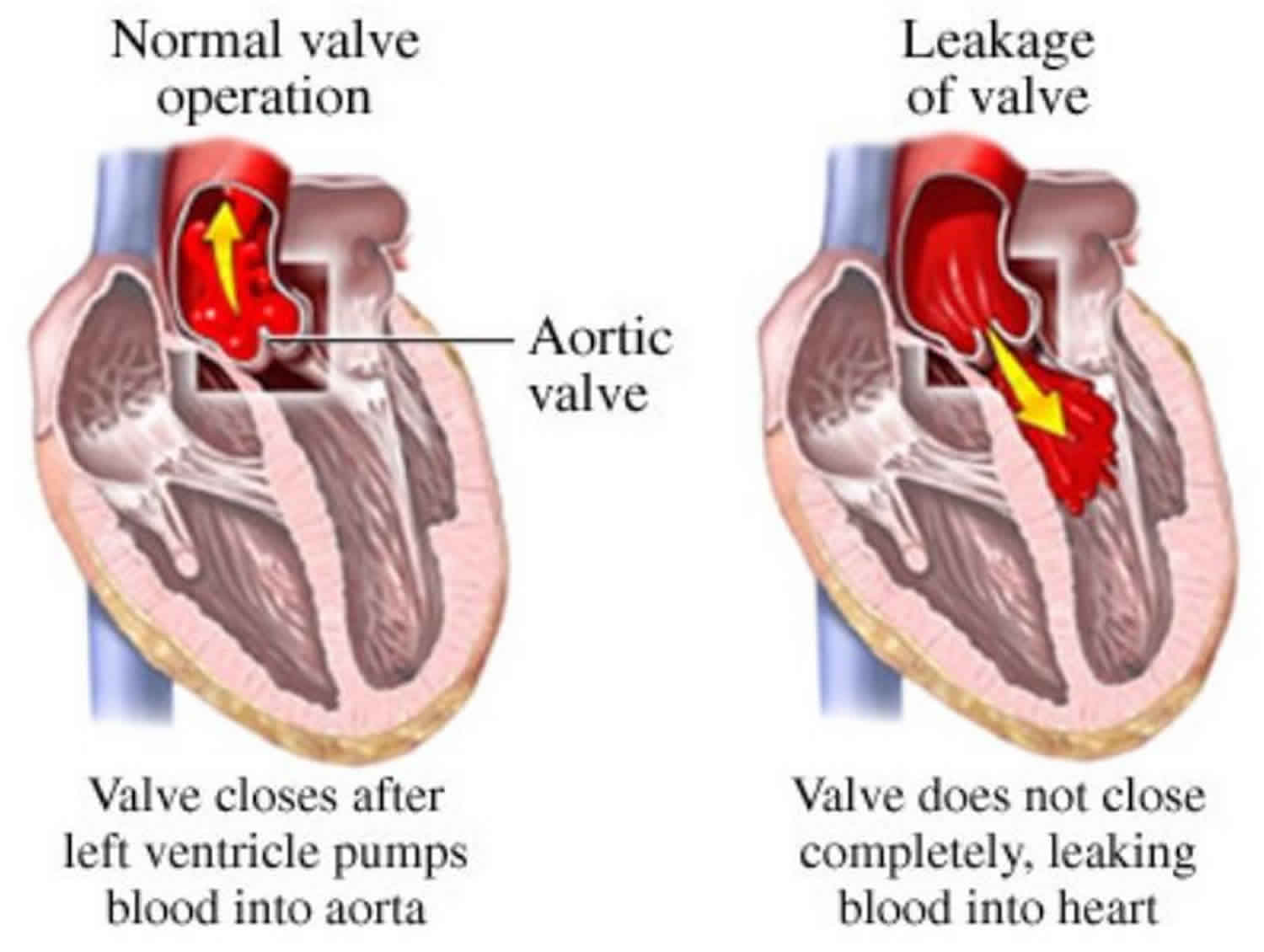
- Heart valve problem called aortic regurgitation
- Heavy exercise
- Fever
- Pregnancy, because of increased fluid and blood in the body
- Overactive thyroid (hyperthyroidism)
See your health care provider if the intensity or rate of your pulse increases suddenly and does not go away. This is very important when:
- You have other symptoms along with increased pulse.
- The change in your pulse does not go away when you rest for a few minutes.
- You already have been diagnosed with a heart problem.
Bounding pulse causes
A bounding pulse can be physiological or related to hyperdynamic circulatory states or cardiac lesions. Prominent bounding pulses are classically associated with moderate or severe aortic regurgitation because of low diastolic pressure and wide pulse pressure 4. A similar pattern can be present in other lesions that provide aortopulmonary connections (patent ductus arteriosus, aortopulmonary window, truncus arteriosus) or arteriovenous connections (arteriovenous malformation) 4.
Physiological causes include:
- Exercise
- Fever
- Pregnancy, because of increased fluid and blood in the body
- Anxiety
Hyperdynamic circulatory states include:
- Thyrotoxicosis or overactive thyroid (hyperthyroidism)
- Anemia
- Paget disease
- Liver cirrhosis
- Long-term (chronic) kidney disease
- Thiamine deficiency or beriberi
- Systolic hypertension
- Arteriovenous fistula
- Cor pulmonale
Cardiac lesions include:
- Aortic regurgitation
- Patent ductus arteriosus
- Aortopulmonary window
- Sinus of Valsalva rupture
- Leaking aortic valve prosthesis
- A ventricular septal defect with aortic regurgitation
- Truncus arteriosus
- Mitral regurgitation
- Heart failure
- Complete heart block
- Abnormal or rapid heart rhythms.
Bounding pulse pathophysiology
In physiological and hyperdynamic circulatory states, the fall in systemic vascular resistance and increased cardiac output causes bounding pulse or water hammer pulse.
The pathophysiology in patients with aortic regurgitation is different. An increased stroke volume filling the relatively empty arterial vessels causes the rapid upstroke when feeling the water hammer pulse. This increased stroke volume is secondary to an increase in end-diastolic volume from the retrograde blood flow from the aorta into the left ventricle during ventricular diastole, or relaxation. The rapid downstroke is partly due to two causes. The first cause is the sudden fall in diastolic pressure in the aorta, which is due to regurgitation of blood from the aorta, or “aortic run-off,” into the left ventricle through the leaky valve. The second cause is the rapid emptying of the arterial system.
The decrease in diastolic pressure from the regurgitant flow also causes an increase in pulse pressure. Pulse pressure is the difference between the systolic and diastolic pressure. Compensation for the decrease in diastolic pressure occurs in two ways. First, due to the regurgitant fraction of blood flow, the heart undergoes chamber dilation and eccentric hypertrophy. These effects increase the stroke volume and therefore the systolic pressure. Secondly, the sympathetic nervous system releases catecholamines and the renin-angiotensin-aldosterone axis works to increase cardiac output to try to maintain a normal mean arterial pressure. As aortic regurgitation continues to progress and worsen, the systolic pressure and pulse pressure continue to rise. Increasing these pressures accentuates the water hammer pulse. However, as the left ventricle continues to stretch, and with the resultant cardiac remodeling, systolic heart failure eventually develops. Systolic heart failure results in stroke volume decrease and forward blood flow 3.
Bounding pulse diagnosis
Your medical history will be vital in determining the cause of the bounding pulse. For example, alcohol abuse in a patient with bounding pulse sign could lead to the diagnosis of cirrhosis. Getting a detailed extracardiac history can help diagnose conditions such as anemia, thyrotoxicosis, fever, pregnancy, cirrhosis, Marfan, rheumatological disorders, and syphilis. A detailed cardiac history, especially regarding congenital heart diseases, will be necessary when suspecting long-term valvular or septal defects 3.
Your doctor will ask questions such as:
- Is this the first time you have felt a bounding pulse?
- Did it develop suddenly or gradually?
- Is it always present, or does it come and go?
- Does it only happen along with other symptoms, such as palpitations?
- What other symptoms do you have?
- Does it get better if you rest?
- Are you pregnant?
- Have you had a fever?
- Have you been very anxious or stressed?
- Do you have other heart problems, such as heart valve disease, high blood pressure, or congestive heart failure?
- Do you have kidney failure?
Your doctor will do a physical exam that includes checking your temperature, pulse, rate of breathing, and blood pressure. Your heart and circulation will also be checked.
The fundamental principle of eliciting bounding pulse is to elevate the patient’s arm above the heart and to palpate the patient’s forearm with the examiner’s palm. The first step is to place the patient in a supine position at a slight recline. With the examiner’s hand wrapped around the patient’s wrist, the radial pulse is palpated. The patient’s arm is then raised above the patient’s head. The water hammer pulse will feel like a tapping impulse through the patient’s forearm due to the rapid emptying of blood from the arm during diastole, with the help of gravity’s effects.
The following diagnostic tests may be performed:
- Blood studies (CBC or complete blood count) for anemia
- Testing thyroid-stimulating hormone or T4 in a patient with suspected thyrotoxicosis
- A urine pregnancy test in a woman of childbearing age
- Genetic testing for Marfan
- Rheumatological blood work for collagen vascular diseases
- Abdominal ultrasound for cirrhosis
- Chest x-ray
- ECG (electrocardiogram)
- Echocardiogram
Chronic aortic regurgitation is one of the more common causes of the water hammer pulse. Therefore, echocardiography such as a transesophageal echocardiogram may be necessary. Examination of the anatomy of the valve, quantifying the amount of aortic regurgitation, defining aortic morphology and size, and evaluating the mechanism of regurgitation between types 1 to 3 will be essential. These actions are particularly helpful to determine whether surgery or valve repair is necessary.
Bounding pulse treatment
Treatment for bounding pulse is dependent on the underlying cause.
Chronic aortic regurgitation is one of the common causes of bounding pulse. Thus, knowing the most up-to-date recommendations on aortic valve repair or replacement will be crucial. The 2017 European Society of Cardiology/European Association for Cardio-Thoracic Surgery guidelines for the management of valvular heart disease outline the indications for intervention in chronic aortic regurgitation. These guidelines depend on the size of the ascending aorta, the severity of the regurgitation, patient symptomology, and the left ventricular function. For patients with severe aortic regurgitation, surgery is indicated in certain patients of classes 1B and 1C. These class 1B patients include symptomatic patients and those with a resting left ventricular ejection fraction less than or equal to 50%. Candidates from class 1C include patients undergoing a coronary artery bypass graft or surgery of the ascending aorta or another valve. In individuals who are asymptomatic with normal left ventricular function, regular evaluation of left ventricular function with serial echocardiograms and changes in patient exercise tolerance will be essential to identify the necessity for surgery 5.
References- Pabba K, Boudi FB. Water Hammer Pulse. [Updated 2019 Jun 26]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK526118
- Maurer G. Aortic regurgitation. Heart. 2006 Jul;92(7):994-1000.
- Suvarna JC. Watson’s water hammer pulse. J Postgrad Med. 2008 Apr-Jun;54(2):163-5.
- Comprehensive Pediatric Hospital Medicine 2007. ISBN: 978-0-323-03004-5 https://doi.org/10.1016/B978-0-323-03004-5.X5001-7
- Baumgartner H, Falk V, Bax JJ, De Bonis M, Hamm C, Holm PJ, Iung B, Lancellotti P, Lansac E, Muñoz DR, Rosenhek R, Sjögren J, Mas PT, Vahanian A, Walther T, Wendler O, Windecker S, Zamorano JL. 2017 ESC/EACTS Guidelines for the Management of Valvular Heart Disease. Rev Esp Cardiol (Engl Ed). 2018 Feb;71(2):110.





{kind=link}