What is Broca’s area
Broca’s area in the left inferior frontal gyrus is widely recognized to be important for speech production, but its specific role in the dynamics of cortical language networks is largely unknown 1. Spoken word production is fundamental to human communication, in the mid 18th century, a French physician Pierre Paul Broca was the first to link word production to a cortical region in the posterior inferior frontal gyrus, since referred to as “Broca’s area” 2. Paul Broca encountered two patients having impairments in language production. The inability to produce language is referred to as Broca’s aphasia. Pars opercularis (Brodmann area 44) and pars triangularis (Brodmann area 45) located in the inferior frontal gyrus today define Broca’s area (see Figure 2) 3. Paul Broca’s iconic findings are among the most influential in the field of cortical specialization, and Broca’s area is still considered to be critically involved in speech production 4.
Broca’s area is responsible for language production and comprehension. Patients with lesions in the Broca’s area experience poor grammar and slower speech production. In other words, these patients know what is being said to them but they cannot communicate fluently in return. Although patients with expressive aphasia know what they want to say, however, they experience problems in speaking it out. For instance, Leborgne who was one of Broca’s patients had the inability to produce neither words nor phrases. Interestingly, Leborgne was only able to say the word Tan and after his death, Broca discovered that Leborgne’s left frontal lobe was damaged. Another patient of Broca’s was named, Lelong. In Lelong’s case, he was only able to say yes, no, always, three, and lelo. Likewise, Broca also found lesions in the lateral frontal lobe. Therefore, Pierre Paul Broca concluded that speech production was somewhat localized in this region of the brain 2.
Broca’s aphasia is often seen in patient’s with head trauma or a stroke. While the individual has preserved comprehension, they have trouble speaking fluently. These patients often undergo speech therapy but because of their other illnesses are often looked after by nurses. Hence, nurses need to be aware of this speech disorder. Individuals with this disorder may be able to read, but their writing ability may be limited. However, it is important to appreciate the fact that in Broca’s aphasia, there is a preservation of intellectual and cognitive functions 5.
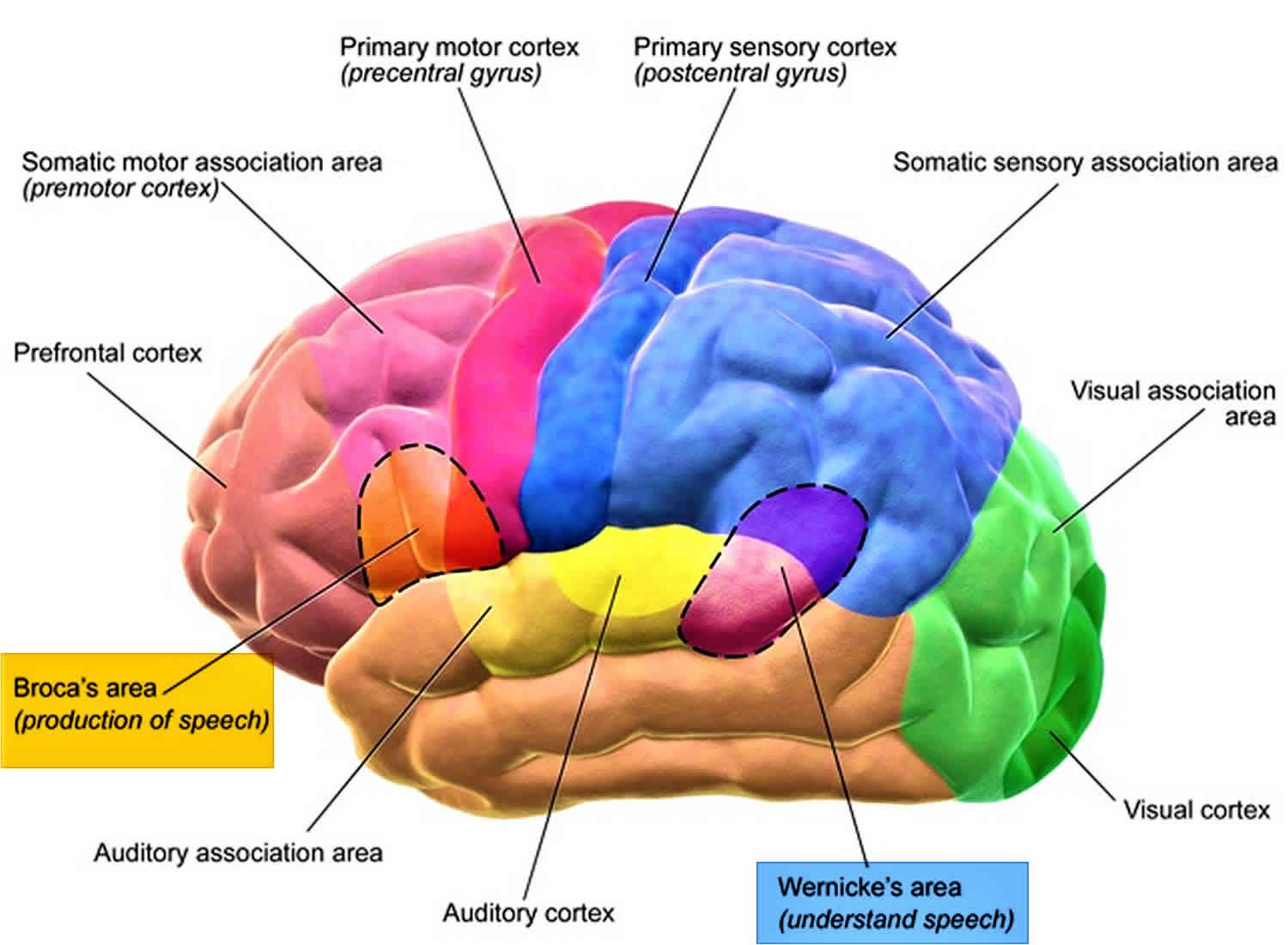
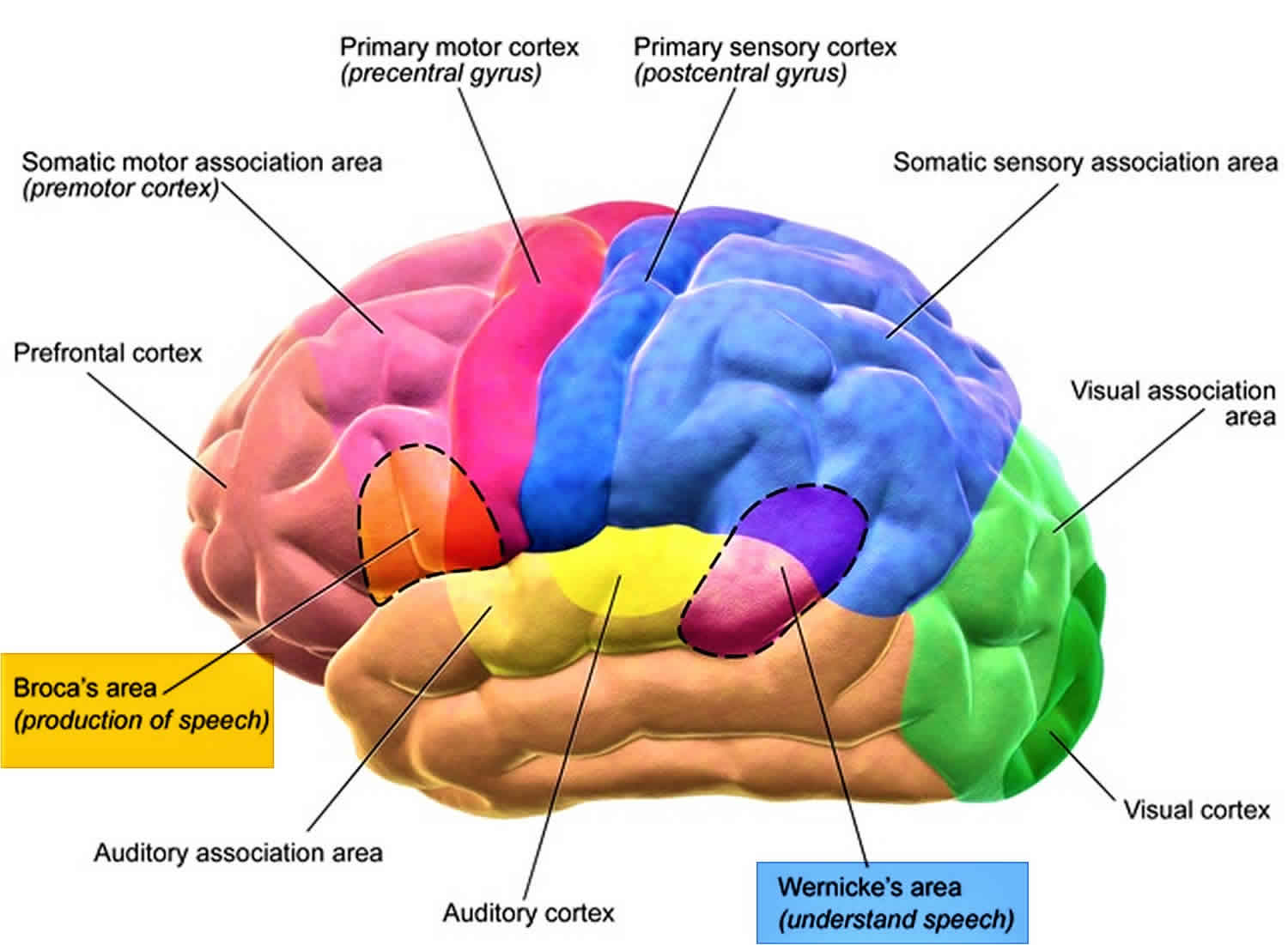
Figure 1. Broca’s area
 What is Wernicke’s area?
What is Wernicke’s area?
Wernicke’s area is also responsible for language processing. Carl Wernicke was a neurologist and his work involved brain injuries that led to aphasia. Strictly speaking, Wernicke’s aphasia is known today as patients who are able to produce speech but in a meaningless manner. In other words, patients may say many words but does not have any structural meaning to them. Wernicke’s area is also linked to the cerebral cortex. In addition, Wernicke’s area plays a role in the understanding of spoken and written comprehension.
Where is Broca’s area located?
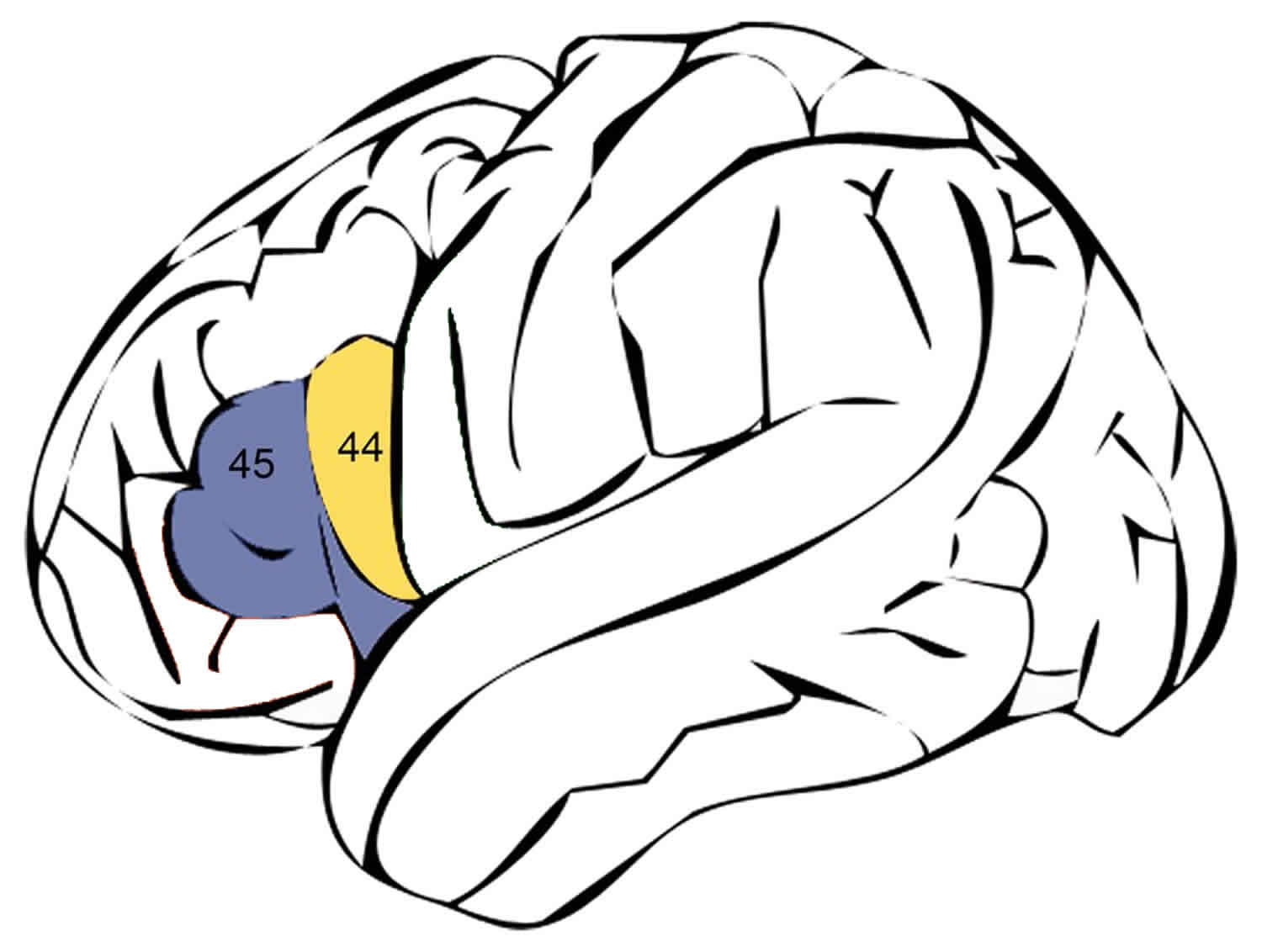
Broca’s area is located in a region in the inferior frontal lobe of the dominant hemisphere of the brain made up of Brodmann area 44 (pars opercularis) and Brodmann area 45 (pars triangularis).
Figure 2. Broca’s area location
What is the function of Broca’s area?
Broca’s area is responsible for speech production. Language function lateralized to the left hemisphere in 96% to 99% of right-handed people and 60% of left-handed people 6. Various pathways connect Broca’s area to the frontal lobe, basal ganglia, cerebellum, and contralateral hemisphere.
As a result of a lesion in Broca’s area, there is a breakdown between one’s thoughts and one’s language abilities. Thus, patients often feel that they know what they wish to say but are unable to produce the words. That is, they are unable to translate their mental images and representations to words. This affects the normal fluency of speech. The loss of language function may be because Broca’s area serves a role in ordering sounds into words, and words into sentences, and thus creates relationships between linguistic elements.
Broca’s area damage
Aphasia is a term used to describe a disturbance in the ability to use symbols (written or spoken) to communicate information and is categorized into two types: expressive aphasia or receptive aphasia. These two types of aphasia can occur together. Broca’s aphasia is also called expressive aphasia 6. A mild form of this condition is termed dysphasia. Aphasia/dysphasia should be distinguished from dysarthria which results from impaired articulation. Dysarthria, as opposed to aphasia, is a motor dysfunction due to disrupted innervation to the face, tongue or soft palate that results in slurred speech but intact fluency and comprehension. Aphasia is typically considered a cortical sign. Its presence suggests dysfunction of the dominant cerebral cortex 7.
The most common cause of Broca’s aphasia is a stroke involving the dominant inferior frontal lobe or Broca’s area (see Figures 1 and 2). A stroke in Broca’s area is usually due to thrombus or emboli in the middle cerebellar artery or internal carotid artery 6. Other causes of Broca’s aphasia include traumatic brain injury, tumors, and brain infections. Aphasia is a symptom of degenerative dementia such as Alzheimer disease. With dementia, patients develop gradual progressive language deficits as opposed to a sudden onset of loss of language function that is seen in an ischemic stroke 8.
Data on the incidence of Broca’s aphasia are limited. In the United States, approximately 170,000 new cases of aphasia related to stroke occur annually 9.
Broca’s aphasia is non-fluent aphasia. The output of spontaneous speech is markedly diminished. There is a loss of normal grammatical structure (agrammatic speech). Specifically, small linking words, conjunctions (and, or, but) and the use of prepositions are lost. As an example, a sentence like “I took the dog for a walk.” may become “I walk dog.” Patients can exhibit interjectional speech where there is a long latency, and the words that are expressed are produced as if under pressure. The ability to repeat phrases is also impaired. Despite these impairments, the words that are produced are often intelligible and contextually correct. In pure Broca’s aphasia, comprehension is intact.
Patients with Broca’s aphasia are often very upset about their difficulty communicating. This may be due to the deficit itself or may be due to damage to adjacent frontal lobe structures which control the inhibition of negative emotions. Broca’s aphasia can accompany other neurological deficits such as right facial weakness, hemiparesis or hemiplegia, and apraxia.
Broca’s area damage diagnosis
Your doctor will likely give you a physical and a neurological exam, test your strength, feeling and reflexes, and listen to your heart and the vessels in your neck. Your doctor will likely request an imaging test (CT, MRI, fMRI, PET or SPECT), usually an MRI, to quickly identify what’s causing the aphasia. Your doctor will also screen you for depression as this is also common in Broca’s aphasia 10.
You’ll also likely undergo tests and informal observations to assess your language skills, such as the ability to:
- Name common objects
- Engage in a conversation
- Understand and use words correctly
- Answer questions about something read or heard
- Repeat words and sentences
- Follow instructions
- Answer yes-no questions and respond to open-ended questions about common subjects
- Read and write
Broca’s area damage treatment
Broca’s aphasia often has a devastating effect on the ability of individuals to carry out their normal activities. It affects the patient’s ability to communicate and often leads to loss of productivity and vocation and can also lead to social isolation 11.
Currently, there is no standard treatment for Broca’s aphasia 6. Treatments should be tailored to each patient’s needs. Speech and language therapy is the mainstay of care for patients with aphasia. It is essential to provide aphasic patients a means to communicate their wants and needs, so these may be addressed. Often this is done by providing a board with various objects so that the patient can point to the object that they want. Involvement of a speech therapist, neuropsychologist, and neurologist in the development of a care plan for the patient with Broca’s aphasia is very helpful in obtaining a good outcome. One innovative treatment option for patients with Broca’s aphasia is melodic intonation. Melodic intonation relies on the fact that musical ability is often spared in Broca’s aphasia. Thus, the speech therapist encourages the patient with poor speech production to try to express their words with musical tones. This approach has shown promise in clinical trials.
Medical treatment of aphasia is currently under investigation in clinical trials. Drug therapies have included catecholaminergic agents (bromocriptine, levodopa, amantadine, dexamphetamine), piracetam and related compounds, acetylcholine esterase inhibitors, and neurotrophic factors. Previous studies have been small, and further studies are needed to determine the efficacy of these pharmacological agents. Also, transcranial magnetic stimulation and transcranial direct stimulation trials for aphasia are currently underway.
When the cause of Broca’s aphasia is a stroke, recovery of language function peaks within two to six months, after which time further progress is limited. However, patients should be encouraged to work on speech production, because cases of improvement have been seen long after a stroke. There are commercial software products available that claim to improve language function, but for the most part, these have not been rigorously tested in randomized clinical trials.
It is important to address issues of post-stroke depression and post-stroke cognitive impairment, as well as disorders of executive function, awareness, neglect, and hemiparesis during the rehabilitation process to optimize the outcome for an individual patient. Family and social support are extremely important to keep patients with language deficits engaged in social and leisure activities which can greatly influence the aphasic patient’s quality of life.
Some patients may recover functionally and be able to lead an independent life as long as they do not have other comorbidities or neurological deficits. The recovery after Broca’s aphasia is often many months or even years, especially if the cause was a stroke. Most people see mild improvement within the first six months, but full recovery can take years. The key is to educate the family members of caregivers who will be looking after the patients 12.
References- Flinker A, Korzeniewska A, Shestyuk AY, et al. Redefining the role of Broca’s area in speech. Proc Natl Acad Sci U S A. 2015;112(9):2871–2875. doi:10.1073/pnas.1414491112 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4352780
- Broca P. Remarques sur le siege de la faculté du langage articulé, suivies d’une observation d’aphémie (perte de la parole) [Remarks on the seat of the faculty of articulated language, following an observation of aphemia (loss of speech)] Bull Mem Soc Anat Paris. 1861;36:330–357
- Wikipedia contributors. “Broca’s area.” Wikipedia, The Free Encyclopedia. Wikipedia, The Free Encyclopedia, 3 Mar. 2013. Web. 2 Apr. 2013.
- Chronic apraxia of speech and Broca’s area. Trupe LA, Varma DD, Gomez Y, Race D, Leigh R, Hillis AE, Gottesman RF. Stroke. 2013 Mar; 44(3):740-4.
- Fridriksson J, Rorden C, Elm J, Sen S, George MS, Bonilha L. Transcranial Direct Current Stimulation vs Sham Stimulation to Treat Aphasia After Stroke: A Randomized Clinical Trial. JAMA Neurol. 2018 Dec 01;75(12):1470-1476.
- Acharya AB, Wroten M. Broca Aphasia. [Updated 2019 Jan 16]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK436010
- Ripamonti E, Frustaci M, Zonca G, Aggujaro S, Molteni F, Luzzatti C. Disentangling phonological and articulatory processing: A neuroanatomical study in aphasia. Neuropsychologia. 2018 Dec;121:175-185.
- Fridriksson J, Fillmore P, Guo D, Rorden C. Chronic Broca’s Aphasia Is Caused by Damage to Broca’s and Wernicke’s Areas. Cereb. Cortex. 2015 Dec;25(12):4689-96
- Ochfeld E, Newhart M, Molitoris J, Leigh R, Cloutman L, Davis C, Crinion J, Hillis AE. Ischemia in broca area is associated with broca aphasia more reliably in acute than in chronic stroke. Stroke. 2010 Feb;41(2):325-30.
- Des Roches CA, Vallila-Rohter S, Villard S, Tripodis Y, Caplan D, Kiran S. Evaluating Treatment and Generalization Patterns of Two Theoretically Motivated Sentence Comprehension Therapies. Am J Speech Lang Pathol. 2016 Dec 01;25(4S):S743-S757
- Ali N, Rafi MS, Ghayas Khan MS, Mahfooz U. The effectiveness of script training to restore lost communication in a patient with Broca’s aphasia. J Pak Med Assoc. 2018 Jul;68(7):1070-1075.
- Silverman ME. Community: the key to building and extending engagement for individuals with aphasia. Semin Speech Lang. 2011 Aug;32(3):256-67





{kind=link}