How to Build Lean Muscle
Caloric Intake
In its simplest form, Calories In vs Calories Out (CICO) is an acronym for the idea that weight loss or gain is determined by a caloric deficit or surplus, regardless of diet composition. Both voluntary and involuntary factors govern the “calories out” side of the equation, beginning with the varying metabolic cost of processing the macronutrients. As reported by Jéquier, the thermic effect of protein (expressed as a percentage of energy content) is 25–30%, carbohydrate is 6–8%, and fat is 2–3% 1. However, Halton and Hu 2 reported greater variability, with the thermic effect of protein being 20–35%, carbohydrate at 5–15%, and fat being subject to debate since some investigators found a lower thermic effect than carbohydrate while others found no difference.
The thermic effect of food (TEF), also called diet-induced thermogenesis, is one of several components of energy expenditure (EE). The thermic effect of food (TEF) represents approximately 8–15% of total daily energy expenditure (TEE) 3. The largest component of total daily energy expenditure (TEE), at least among individuals not involved in extremely high volumes of exercise, is resting energy expenditure (REE), which is often mentioned interchangeably with resting metabolic rate (RMR) or basal metabolic rate (BMR). Basal metabolic rate is the energetic cost of the biological processes required for survival at rest. As a matter of technical trivia, basal metabolic rate (BMR) is measured in an overnight fasted state, lying supine at complete rest, in the postabsorptive state (the condition in which the gastrointestinal tract is empty of nutrients and body stores must supply required energy). Resting energy expenditure (REE) or resting metabolic rate (RMR) represents fasted-state energy expenditure at rest at any time of the day, and can range 3–10% higher than BMR due to the residual influence of thermic effect of food (TEF) and physical activity 4.
Basal metabolic rate typically amounts to 60–70% of total daily energy expenditure (TEE). The other main component of total daily energy expenditure (TEE) is non-resting energy expenditure, which is comprised of 3 subcomponents: non-exercise activity thermogenesis (NEAT), exercise activity thermogenesis (ExEE), and finally, thermic effect of food (TEF). Non-exercise activity thermogenesis (NEAT) encompasses the energy expenditure of occupation, leisure, basic activities of daily living, and unconscious/spontaneous activity such as fidgeting. While resting metabolic rate (RMR) and thermic effect of food (TEF) are relatively static, Non-exercise activity thermogenesis (NEAT) and exercise activity thermogenesis (ExEE) vary widely within and across individuals. Exercise activity thermogenesis (ExEE) has been reported to range from 15 to 30% of total daily energy expenditure (TEE) 3, but the role of non-exercise activity thermogenesis (NEAT) is more easily overlooked. Non-exercise activity thermogenesis (NEAT) comprises ~15% of total daily energy expenditure (TEE) in sedentary individuals and perhaps 50% or more in highly active individuals 5. The impact of non-exercise activity thermogenesis (NEAT) can be substantial since it can vary by as much as 2000 kcals between individuals of similar size 6. Table 4 outlines the components of total daily energy expenditure (TEE), with examples of low, moderate, and high total daily energy expenditure (TEE) 5.
Humans have a remarkable ability to maintain a relatively constant body weight through adult life despite wide variations in daily energy intake and expenditure. This indicates a highly sophisticated integration of systems that tirelessly auto-regulate homeostasis. In the case of hypocaloric conditions, the body up-regulates hunger and down-regulates energy expenditure. The integration of physiological factors regulating the body’s defense against weight loss (and also weight gain) is symphonic. The central nervous system ‘communicates’ with the adipose tissue, gastrointestinal tract and other organs in an effort to defend against homeostatic changes. This regulatory system is influenced by nutritional, behavioral, autonomic, and endocrine factors 7.
The degree of processing or refinement of foods can influence their thermic effect. Barr and Wright 8 found a diet-induced thermogenesis of 137 kcal for a ‘whole food’ meal, and 73 kcal for the processed food meal. The ‘whole food’ meal had 5% more protein, and 2.5 g more fiber, but these factors are too small to account for the substantial difference in postprandial energy expenditure. The authors speculated that the greater mechanized preparation of the processed food caused less peristalsis and a greater loss of bioactive compounds, resulting in fewer metabolites, thus requiring less enzyme activity. This would lead to more energetically efficient absorption and metabolism. It is important to note that this was not a comparison of a highly processed food versus a whole food. Both of the meals in the comparison were cheese sandwiches. One just happened to have less mechanical refinement, and slightly more fiber and protein. The results of this study imply that processed foods are more fattening or less effective for weight management. However, the contrary has been demonstrated. Meal replacement products (powders, shakes, and bars) have matched or outperformed the effectiveness of whole food-based diets for weight loss and weight loss maintenance 9.
Table 1. Components of total daily energy expenditure (TEE)
| Component of TEE | Percent of TEE | Example: 1600 kcal TEE | Example: 2600 kcal TEE | Example: 3600 kcal TEE |
|---|---|---|---|---|
| Thermic effect of food (TEF) | 8–15% | 128–240 | 208–390 | 288–540 |
| Exercise activity thermogenesis (ExEE) | 15–30% | 240–480 | 390–780 | 540–1080 |
| Non-exercise activity thermogenesis (NEAT) | 15–50% | 240–800 | 390–1300 | 540–1800 |
| Basal metabolic rate (BMR) | 60–70% | 960–1120 | 1560–1820 | 2160–2520 |
An awareness of tissue-specific metabolism can be helpful in understanding the resting metabolic benefits of improving body composition. It can also serve to clarify the widely misunderstood and often overestimated contribution of muscle to REE. McClave and Snider 11 reported that the greatest contributors to resting metabolic rate (RMR), per unit of mass, are the heart and kidneys, each spending approximately 400 kcal/kg/day. Next in the hierarchy are the brain and the liver, at 240 and 200 kcal/kg/day, respectively. These four organs constitute up to 70–80% of resting energy expenditure (REE). In contrast, muscle and adipose tissue expend 13 and 4.5 kcal/kg/day, respectively. A relatively significant muscular gain of 5 kg would increase resting energy expenditure (REE) by only ~65 kcal/day. However, on a net basis (accounting for the total mass of each tissue in the body), muscle, brain, and liver are the top-3 contributors to overall resting metabolic rate (RMR). Thus, substantial losses in lean mass – including muscle – can meaningfully impact resting metabolic rate (RMR). Finally, it should be noted that tissue-specific energy expenditure can vary according to obese vs. non-obese status, advanced age, and to a lesser degree, sex 12. Table 5 outlines the contribution of organs and tissues to REE in healthy adult humans 11.
Table 2. Energy Expenditure of Different Tissues/Organs
| Organ or tissue | Metabolic rate (kcal/kg/day) | % Overall REE | Weight (kg) | % of Total body weight |
|---|---|---|---|---|
| Adipose | 4.5 | 4 | 15 | 21.4 |
| Other (bone, skin, intestine, glands) | 12 | 16 | 23.2 | 33.1 |
| Muscle | 13 | 22 | 28 | 40.0 |
| Liver | 200 | 21 | 1.8 | 2.6 |
| Brain | 240 | 22 | 1.4 | 2.0 |
| Heart | 400 | 9 | 0.3 | 0.5 |
| Kidneys | 400 | 8 | 0.3 | 0.5 |
In determining an appropriate caloric intake, it should be noted that the tissue lost during the course of an energy deficit is influenced by the size of the energy deficit. While greater deficits yield faster weight loss, the percentage of weight loss coming from lean body mass (LBM) tends to increase as the size of the deficit increases 13, 14, 15. In studies of weight loss rates, weekly losses of 1 kg compared to 0.5 kg over 4 weeks resulted in a 5% decrease in bench press strength and a 30% greater reduction in testosterone levels in strength training women 16. Weekly weight loss rates of 1.4% of bodyweight compared to 0.7% in athletes during caloric restriction lasting four to eleven weeks resulted in reductions of fat mass of 21% in the faster weight loss group and 31% in the slower loss group. In addition, LBM increased on average by 2.1% in the slower loss group while remaining unchanged in the faster loss group. Worthy of note, small amounts of LBM were lost among leaner subjects in the faster loss group 14.
Therefore, weight loss rates that are more gradual may be superior for LBM retention. At a loss rate of 0.5 kg per week (assuming a majority of weight lost is fat mass), a 70 kg athlete at 13% body fat would need to be no more than 6 kg to 7 kg over their contest weight in order to achieve the lowest body fat percentages recorded in competitive bodybuilders following a traditional three month preparation 17, 18. If a competitor is not this lean at the start of the preparation, faster weight loss will be required which may carry a greater risk for LBM loss.
In a study of bodybuilders during the twelve weeks before competition, male competitors reduced their caloric intake significantly during the latter half and subsequently lost the greatest amount of lean body mass (LBM) in the final three weeks 19. Therefore, diets longer than two to four months yielding weight loss of approximately 0.5 to 1% of bodyweight weekly may be superior for LBM retention compared to shorter or more aggressive diets. Ample time should be allotted to lose body fat to avoid an aggressive deficit and the length of preparation should be tailored to the competitor; those leaner dieting for shorter periods than those with higher body fat percentages. It must also be taken into consideration that the leaner the competitor becomes the greater the risk for LBM loss 20, 15. As the availability of adipose tissue declines the likelihood of muscle loss increases, thus it may be best to pursue a more gradual approach to weight loss towards the end of the preparation diet compared to the beginning to avoid LBM loss.
- Diets focused primarily on gaining lean mass are driven by a sustained caloric surplus to facilitate anabolic processes and support increasing resistance-training demands 10. The composition and magnitude of the surplus, as well as training status of the subjects can influence the nature of the gains.
- A wide range of dietary approaches (low-fat to low-carbohydrate/ketogenic diets and all points between) can be similarly effective for improving body composition.
- Bodybuilders typically employ a higher meal frequency in an attempt to optimize fat loss and muscle preservation. However, the majority of chronic experimental studies have failed to show that different meal frequencies have different influences on bodyweight or body composition 21, 22, 23. Despite this limitation, the available research has consistently refuted the popular belief that a grazing pattern (smaller, more frequent meals) raises energy expenditure compared to a gorging pattern (larger, less frequent meals). Disparate feeding patterns ranging from two to seven meals per day have been compared in tightly controlled studies using metabolic chambers, and no significant differences in 24-hour thermogenesis have been detected 24, 25. Along these lines, Stote et al. [113] found that compared to three meals per day, one meal per day caused slightly more weight and fat loss. Curiously, the one meal per day group also showed a slight gain in lean mass, but this could have been due to the inherent error in the use of bioelectrical impedance analysis (BIA) to measure body composition for body composition assessment 26.
- Increasing dietary protein to levels significantly beyond current recommendations for athletic populations may result in improved body composition. The International Society of Sports Nutrition’s original 2007 position stand on protein intake (1.4–2.0 g/kg) 27 has gained further support from subsequent investigations arriving at similar requirements in athletic populations 28, 29, 30, 31, 32, 33.
- Higher protein intakes (2.3–3.1 g/kg lean mass) may be required to maximize muscle retention in lean, resistance-trained subjects under hypocaloric conditions. Emerging research on very high protein intakes (>3 g/kg) has demonstrated that the known thermic, satiating, and lean-mass-preserving effects of dietary protein might be amplified in resistance-training subjects.
- The collective body of intermittent caloric restriction (intermittent fasting) research demonstrates no significant advantage over daily caloric restriction for improving body composition. Time-restricted feeding typically involves a fasting period of 16–20 hours and a feeding period of 4–8 hours daily. Unsurprisingly, significant weight loss occurs, and this includes a reduction in lean mass as well as fat mass 34, 35. An 8-week trial by Tinsley et al. 36 examined the effect of a 20-hour fasting/4-hour feeding protocol (20/4) done 4 days per week on recreationally active, but untrained subjects. No limitations were placed on the amounts and types of food consumed in the 4-hour eating window. A standardized resistance training program was administered 3 days per week. The time-restricted feeding group lost body weight, due to a significantly lower energy intake (667 kcal less on fasting compared to non-fasting days). Cross sectional area of the biceps brachii and rectus femoris increased similarly in both the time-restricted feeding and normal diet group. No significant changes in body composition (via DXA) were seen between groups. Despite a lack of statistical significance, there were notable effect size differences in lean soft tissue (normal diet gained 2.3 kg, while time-restricted feeding lost 0.2 kg). Although both groups increased strength without significant between-group differences, effect sizes were greater in the time-restricted feeding group for bench press endurance, hip sled endurance, and maximal hip sled strength. This finding should be viewed cautiously given the potential for greater and more variable neurological gains in untrained subjects. A subsequent study by Moro et al. 37 found that in resistance-trained subjects on a standardized training protocol, a 16-hour fasting/8-hour feeding cycle (16/8) resulted in significantly greater fat loss in time-restricted feeding vs. normal diet control group (ND) (1.62 vs. 0.31 kg), with no significant changes in lean mass in either group. Time-restricted feeding’s meals were consumed at 1 pm, 4 pm, and 8 pm. Normal diet’s meals were consumed at 8 am, 1 pm, and 8 pm. Macronutrient intake between the time-restricted feeding and normal diet groups was matched, unlike the aforementioned Tinsley et al. study 36 whereby protein intake was disparate and sub-optimal (1.0 g/kg in the time-restricted feeding group and 1.4 g/kg in the normal diet control group). Subjects in the present study’s time-restricted feeding and normal diet group consumed 1.93 and 1.89 g/kg, respectively. The mechanisms underlying these results are not clear. The authors speculated that increased adiponectin levels in the time-restricted feeding group could have stimulated mitochondrial biogenesis via interacting with PPAR-gamma, in addition to adiponectin acting centrally to increase energy expenditure. However, the time-restricted feeding group also experienced unfavorable changes such as decreased testosterone and triiodothyronine levels.
- Seimon et al. 38 recently published the largest systematic review of intermittent fasting research to date, comparing the effects of intermittent energy restriction (IER) to continuous energy restriction (CER) on body weight, body composition, and other clinical parameters. Their review included 40 studies in total, 12 of which directly compared an intermittent energy restriction (IER) with a continuous energy restriction (CER) condition. They found that overall, the two diet types resulted in “apparently equivalent outcomes” in terms of body weight reduction and body composition change. Interestingly, intermittent energy restriction (IER) was found to be superior at suppressing hunger. The authors speculated that this might be attributable to ketone production in the fasting phases. However, this effect was immaterial since on the whole, intermittent fasting failed to result in superior improvements in body composition or greater weight loss compared to continuous energy restriction (CER). Table 3 outlines the characteristics of the major diet archetypes.
- Dehydration: In an attempt to enhance muscle size and definition by reducing extracellular water content, many bodybuilders engage in fluid, electrolyte, and carbohydrate manipulation in the final days and hours before competing 39, 40. The effect of electrolyte manipulation and dehydration on visual appearance has not been studied, however it may be a dangerous practice 41. Furthermore, dehydration could plausibly degrade appearance considering that extracellular water is not only present in the subcutaneous layer. A significant amount is located in the vascular system. Thus, the common practice of “pumping up” to increase muscle size and definition by increasing blood flow to the muscle with light, repetitive weight lifting prior to stepping on stage 42 could be compromised by dehydration or electrolyte imbalance. Furthermore, dehydration reduces total body hydration. A large percentage of muscle tissue mass is water and dehydration results in decreases in muscle water content 43 and therefore muscle size, which may negatively impact the appearance of muscularity. At this time it is unknown whether dehydration or electrolyte manipulation improves physique appearance. What is known is that these practices are dangerous and have the potential to worsen it. It is unclear if carbohydrate loading has an impact on appearance and if so, how significant the effect is. However, the recommended muscle-sparing practice by some researchers to increase the carbohydrate content of the diet in the final weeks of preparation 44 might achieve any proposed theoretical benefits of carbohydrate loading. If carbohydrate loading is utilized, a trial run before competition once the competitor has reached or nearly reached competition leanness should be attempted to develop an individualized strategy. However, a week spent on a trial run consuming increased carbohydrates and calories may slow fat loss, thus ample time in the diet would be required.
- Carbohydrate Loading: In the final days before competing, bodybuilders commonly practice carbohydrate loading similar to endurance athletes in an attempt to raise muscle-glycogen levels and increase muscle size 45, 46, 47, 42. In the only direct study of this practice, no significant quantitative change in muscle girth was found to occur [208]. However, an isocaloric diet was used, with only a change in the percentage of carbohydrate contributing to the diet. If total calories had also been increased, greater levels of glycogen might have been stored which could have changed the outcome of this study. Additionally, unlike the subjects in this study bodybuilders prior to carbohydrate loading have reduced glycogen levels from a long calorically restricted diet and it is possible in this state that carbohydrate loading might effect a visual change. Furthermore, bodybuilding performance is measured subjectively, thus analysis of girth alone may not discern subtle visual changes which impact competitive success. Lastly, some bodybuilders alter the amount of carbohydrate loaded based on the visual outcome, increasing the amount if the desired visual change does not occur 47. Thus, an analysis of a static carbohydrate load may not accurately represent the dynamic nature of actual carbohydrate loading practices.In fact, in an observational study of competitive bodybuilders in the days before competition who loaded carbohydrates, subjects showed a 4.9% increase in biceps thickness the final day before competition compared to six weeks prior 45. Although it is unknown if this was caused by increased muscle glycogen, it is unlikely it was due to muscle mass accrual since the final weeks of preparation are often marked by decreases not increases in lean mass 44. Future studies of this practice should include a qualitative analysis of visual changes and analyze the effects of concurrent increases in percentage of carbohydrates as well as total calories.
- The long-term success of a diet depends upon compliance and suppression or circumvention of mitigating factors such as adaptive thermogenesis. Joosen and Westerterp 48 examined the literature (11 studies) to see if “adaptive thermogenesis” existed in overeating experiments. No evidence beyond the theoretical costs of increased body size and thermic effect of food were found. Nevertheless, there is substantial interindividual variability in the energetic response to overfeeding. They found in overfeeding experiments, weight gain is often less than expected from the energy excess intake. In part this is the result of an obligatory increase in energy expenditure associated with the increased body weight and lean mass 49 and the larger amount of food to be digested and absorbed 50. However, evidence for adaptive thermogenesis as a mechanism to explain interindividual differences in weight gain on the same overeating regimen is still inconsistent and hard to prove 51
- There is a paucity of research on women and older populations, as well as a wide range of untapped permutations of feeding frequency and macronutrient distribution at various energetic balances combined with training. Behavioral and lifestyle modification strategies are still poorly researched areas of weight management.
Low-Calorie Diets
Low-calorie diets (LCD) and very-low-calorie diets (VLCD) are characterized by their provision of 800–1200 kcal/day and 400–800 kcal/day, respectively 52. Note that Low-calorie diets (LCD) have also been given a more liberal definition of providing 800–1800 kcal 53. Very-low-calorie diets (VLCD) are typically in liquid form and commercially prepared. The aim of the diet is to induce rapid weight loss (1.0–2.5 kg/week) while preserving as much lean mass as possible. Very-low-calorie diets (VLCD) are designed to replace all regular food consumption, and therefore should not be confused with meal replacement products intended to replace one or two meals per day. As such, very-low-calorie diets (VLCD) are fortified with the full spectrum of essential micronutrients. The macronutrient content of very-low-calorie diets (VLCD) is approximately protein 70–100 g/day, fat 15 g/day and carbohydrate 30–80 g/day. A protein-sparing modified fast can be considered the higher-protein variant of a VLCD, with protein intakes of approximately 1.2–1.5 g/kg/d 54. However, even at protein intakes as low as 50 g/day, the proportion of lean mass loss from VLCD has been reported to be 25% of total weight loss, with 75% as fat loss 55.
Resistance training has shown an impressive ability to augment the preservation of muscle and even increase it during VLCD – at least in untrained/obese subjects. A 12-week trial by Bryner et al. 56 found that resistance training while consuming 800 kcal resulted in the preservation of lean mass in untrained obese subjects. There was actually a slight gain, but it did not reach statistical significance. Resting metabolic rate (RMR) significantly increased in the training group, but it decreased in the control group. Donnelly et al. 57 reported a significant increase in cross-sectional area of both slow- and fast-twitch muscle fibers in untrained obese subjects after 12 weeks on an 800 kcal diet with resistance training. While these results cannot necessarily be extrapolated to lean, trained subjects, they are nevertheless intriguing.
In obese populations, aggressive caloric restriction is a potentially powerful intervention since a greater initial weight loss is associated with greater long-term success in weight loss maintenance 58. However, a meta-analysis by Tsai and Wadden 53 found that VLCD did not result in greater long-term (1 year or more) weight loss than LCD. Eight to 12 week VLCD are common in clinical practice before transitioning to less severe caloric restriction; however, there is an ongoing debate regarding the duration that can be safely sustained for VLCD. Multiple deaths have been reported due to low-quality protein intake, excessive loss of lean mass, and inadequate medical supervision 59. Adverse effects of VLCD include cold intolerance, fatigue, headache, dizziness, muscle cramps, and constipation. Hair loss was reported to be the most common complaint of extended VLCD use 53. It should be noted that VLCD use has limited relevance to healthy and athletic populations.
Low-Fat diets
Low-fat diets (LFD) have been defined as providing 20–35% fat 60. This is based on the Acceptable Macronutrient Distribution Ranges (AMDR) for adults, set by the Food and Nutrition Board of the Institute of Medicine 61. The AMDR set protein at 10–35%, carbohydrate at 45–65%, and fat at 20–35% of total energy. Although the classification of low-fat diets (LFD) is based on the AMDR, it might be more accurate to call them high-carbohydrate diets, given the dominance of this macronutrient in the ranges. As such, the definition of low-fat diets (LFD) is inherently subjective.
Scientists and physicians have promoted decreased fat intake since the 1950s 62. The 1977 publication of the Dietary Goals for the United States, and the 1980 publication of the inaugural Dietary Guidelines for Americans (DGA) reinforced a reduction in total fat intake with the aim of improving public health 63. Although the AMDR were published in 2005, their staying power is apparent since the recently updated Dietary Guidelines for Americans adheres to these ranges 64, as do major health organizations such as the American Heart Association, American Diabetes Association and Academy of Nutrition and Dietetics.
A recent systematic review by Hooper et al. 65 analyzed 32 randomized controlled trials (RCTs) containing ~54,000 subjects, with a minimum duration of 6 months. Reducing the proportion of dietary fat compared to usual intake modestly but consistently reduced body weight, body fat, and waist circumference. Excluded from the analysis were RCTs where subjects in either the control or experimental groups had the intention to reduce weight. The implication of these findings is that reducing the proportion of dietary fat can cause a de facto reduction of total energy intake, thereby reducing body fat over time.
The premise of dietary fat reduction for weight loss is to target the most energy-dense macronutrient to impose hypocaloric conditions. Tightly controlled experiments have covertly manipulated the fat content of diets similar in appearance and palatability, and the higher energy density of the higher-fat diets resulted in greater weight gain and/or less weight loss 66, 67. However, over the long-term, diets with lower energy density have not consistently yielded greater weight loss than energy restriction alone 68, 69. Reasons for the disparity between short- and long-term effects of energy density reduction include speculation that learned compensation is occurring. In addition, postprandial factors may increase sensory-specific satiety that over time can reduce the initial palatability of energy-dense foods 70.
Very-low-fat diets (VLFD) have been defined as providing 10–20% fat 60. Diets fitting this profile have a limited amount of research. The body of controlled intervention data on VLFD mainly consists of trials examining the health effects of vegetarian and vegan diets that aggressively minimize fat intake. These diets have shown consistently positive effects on weight loss 71, but this literature lacks body composition data. Among the few studies that did, the A TO Z Weight Loss Study by Gardner et al. 72, did not show any significant between-group differences in body fat reduction among the diets (Atkins, Zone, LEARN, and Ornish). However, despite the Ornish group’s assigned fat intake of ≤10% of total calories, actual intake progressed from 21.1 to 29.8% by the end of the 12-month trial. Similar results were seen by de Souza et al. 73 in the POUNDS LOST trial. Four groups were assigned high-protein (25%) and average-protein (15%) versions of high-fat (40%) and low-fat (20%) diets. No significant between-group differences were seen in the loss of total abdominal, subcutaneous, or visceral fat at either six months or two years. A mean loss of 2.1 kg lean mass and 4.2 kg fat mass occurred in both groups at 6 months. No lean mass-retentive advantage was seen in the higher-protein diets, but this could have been due to both protein intake levels being sub-optimal (1.1 and 0.7 g/kg). As seen in previous low fat diet research, the targeted restriction to 20% fat was apparently difficult to attain since actual intakes ranged 26–28%.
Low-Carbohydrate diets
Similar to low fat diets, low-carbohydrate diets (LCD) are a broad category lacking an objective definition. There is no universal agreement on what quantitatively characterizes an low-carbohydrate diets (LCD). The Dietary Guidelines for Americans lists 45–65% of total energy as the appropriate carbohydrate intake for adults 74. Therefore, diets with intakes below 45% fall short of the ‘official’ guidelines and can be viewed as LCD. However, other published definitions of low-carbohydrate diets (LCD) disregard the limits set in the Dietary Guidelines for Americans. Low-carbohydrate diets (LCD) have been defined as having an upper limit of 40% of total energy from carbohydrate 75, 76. In absolute rather than proportional terms, LCD have been defined as having less than 200 g of carbohydrate 75. Some investigators have taken issue with this liberal definition of LCD, preferring to delineate non-ketogenic LCD as containing 50–150 g, and ketogenic diet as having a maximum of 50 g 77.
Meta-analyses comparing the effects of low fat diets with low-carbohydrate diets have yielded mixed results across a wide range of parameters. Liberal operational definitions of low-carbohydrate diets (e.g., ≤45%) have led to a lack of significant differences in body weight and waist circumference 78, while lower carbohydrate classification thresholds (<20%) have favored low-carbohydrate diets for weight loss and other cardiovascular risk factors 79. Recently, Hashimoto et al. 80 conducted the first-ever meta-analysis on the effect of low-carbohydrate diets on fat mass (FM) and body weight. The analysis, limited to trials involving overweight/obese subjects, had a total of 1416 subjects, stratifying the diets as “mild low-carbohydrate diets” (~40% carbohydrate) or “very low-carbohydrate diets” (~50 g carbohydrate or 10% of total energy). Eight randomised clinical trials (RCTs) included a very low-carbohydrate diets treatment, and 7 RCTs included a mild low-carbohydrate diets treatment. With all groups considered, fat mass decrease was significantly greater in the low-carbohydrate diets than the control diets. However, sub-analysis showed that fat mass decrease in very low-carbohydrate diets was greater than the controls, while the difference in fat mass decrease between mild low-carbohydrate diets and controls was not significant. A separate sub-analysis of short- versus long-term effects found that both types of low-carbohydrate diets yielded significantly greater fat loss than controls in trials less than, as well as longer than 12 months. A further sub-analysis of found that BIA failed to detect significant between-group differences in fat mass reduction, while DXA showed significantly greater decreases in low-carbohydrate diets than controls. It should be noted that despite reaching statistical significance, mean differences in fat mass reduction between low-carbohydrate diets and control groups were small (range = 0.57–1.46 kg). Practical relevance is questionable given the obese nature of the subjects. The authors speculated that the advantage of the low-carbohydrate diets over the control diets could have been due to their higher protein content.
Ketogenic diets
Despite being a subtype of low-carbohydrate diets, the ketogenic diet (KD) deserves a separate discussion. Whereas non-ketogenic low-carbohydrate diets is subjectively defined, ketogenic diet (KD) is objectively defined by its ability to elevate circulating ketone bodies measurably – a state called ketosis, also known as physiological or nutritional ketosis. Aside from completely fasting, this condition is attained by restricting carbohydrate to a maximum of ~50 g or ~10% of total energy 77, while keeping protein moderate (1.2–1.5 g/kg/day) 81, with the remaining predominance of energy intake from fat (~60–80% or more, depending on degree protein and carbohydrate displacement). Ketosis is a relatively benign state not to be confused with ketoacidosis, which is a pathological state seen in type 1 diabetics, where a dangerous overproduction of ketones occurs in the absence of exogenous insulin. The primary ketone produced hepatically is acetoacetate, and the primary circulating ketone is β-hydroxybutyrate 82. Under normal, non-dieting conditions, circulating ketone levels are low (<3 mmol/l). Depending on the degree of restriction of carbohydrate or total energy, ketogenic diet (KD) can raise circulating ketone levels to a range of ~0.5–3 mmol/l, with physiological ketosis levels reaching a maximum of 7–8 mmol/l 81.
The proposed fat loss advantage of carbohydrate reduction beyond a mere reduction in total energy is based largely on insulin-mediated inhibition of lipolysis and presumably enhanced fat oxidation. However, a single-arm study by Hall et al. 83 examined the effect of 4 weeks on a low fat diet (300 g carbohydrate) followed by 4 weeks on a ketogenic diet (KD) (31 g carbohydrate). Blood ketone levels plateaued at ~1.5 mmol/l within two weeks into the ketogenic diet (KD). A transient increase in energy expenditure (~100 kcal/day) lasting a little over a week occurred upon switching to the ketogenic diet (KD). This was accompanied by a transient increase in nitrogen loss, potentially suggesting a stress response including the ramping up of gluconeogenesis. Although insulin levels dropped rapidly and substantially during the ketogenic diet (KD) (consisting of 80% fat, 5% carbohydrate), an actual slowing of body fat loss was seen during the first half of the ketogenic diet (KD) phase.
It has been postulated that the production and utilization of ketone bodies impart a unique metabolic state that, in theory, should outperform non-ketogenic conditions for the goal of fat loss 77. However, this claim is largely based on research involving higher protein intakes in the low-carbohydrate diets/ketogenic diet groups. Even small differences in protein can result in significant advantages to the higher intake. A meta-analysis by Clifton et al. 84 found that a 5% or greater protein intake difference between diets at 12 months was associated with a threefold greater effect size for fat loss. Soenen et al. 85 systematically demonstrated that the higher protein content of low-carbohydrate diets, rather than their lower carbohydrate content, was the crucial factor in promoting greater weight loss during controlled hypocaloric conditions. This is not too surprising, considering that protein is known to be the most satiating macronutrient 86. A prime example of protein’s satiating effect is a study by Weigle et al. 87 showing that in ad libitum conditions, increasing protein intake from 15 to 30% of total energy resulted in a spontaneous drop in energy intake by 441 kcal/day. This led to a body weight decrease of 4.9 kg in 12 weeks.
With scant exception 88, all controlled interventions to date that matched protein and energy intake between ketogenic diet (KD) and non-ketogenic diet conditions have failed to show a fat loss advantage of the ketogenic diet (KD) 89, 90, 91. A recent review by Hall 92 states, “There has never been an inpatient controlled feeding study testing the effects of isocaloric diets with equal protein that has reported significantly increased energy expenditure or greater loss of body fat with lower carbohydrate diets.” In light of this and the previously discussed research, the ‘special effects’ of low-carbohydrate diets and ketogenic diets are not due to their alleged metabolic advantage, but their higher protein content. Perhaps the strongest evidence against the alleged metabolic advantage of carbohydrate restriction is a recent pair of meta-analyses by Hall and Guo 91, which included only isocaloric, protein-matched controlled feeding studies where all food intake was provided to the subjects (as opposed to self-selected and self-reported intake). A total of 32 studies were included in the analysis. Carbohydrate ranged from 1 to 83% and dietary fat ranged from 4 to 84% of total energy. No thermic or fat loss advantage was seen in the lower-carbohydrate conditions. In fact, the opposite was revealed. Both energy expenditure (EE) and fat loss were slightly greater in the higher-CHO/lower-fat conditions (EE by 26 kcal/day, fat loss by 16 g/d); however, the authors conceded that these differences were too small to be considered practically meaningful 91.
If there is any advantage to ketogenic diet (KD) over non-KD for fat loss, it is potentially in the realm of appetite regulation. Under non-calorically restricted conditions, ketogenic diet (KD) has consistently resulted in body fat and/or body weight reduction 93, 94. This occurs via spontaneous energy intake reduction, which could be due to increased satiety through a suppression of ghrelin production 95. Moreover, ketogenic diet has demonstrated hunger-suppressive effects independent of protein content. In a 4-week crossover design, Johnstone et al. 96 found that a ketogenic diet consumed ad libitum (without purposeful caloric restriction) resulted in an energy intake reduction of 294 kcal/day. The latter results were seen despite a relatively high protein intake (30% of energy) matched between ketogenic diet (4% CHO) and non-KD (35% CHO) conditions. In further support of this idea, a meta-analysis by Gibson et al. 97 found that ketogenic diet suppresses appetite more than VLCD. However, it remains unclear whether the appetite suppression is due to ketosis or other factors such as an increased protein or fat intake, or restriction of carbohydrate.
An area of growing interest is the effect of ketogenic diet on athletic performance. Since training capacity has the potential to affect body composition, the effect of ketogenic diet on exercise performance warrants discussion. Carbohydrate restriction combined with high fat intake to become fat-adapted (or ketoadapted) is a tactic that attempts to improve performance by increasing the body’s reliance on fat as fuel, thereby sparing/decreasing glycogen use, which ostensibly could improve athletic performance. However, in contrast to the proposed benefits of fat-adaptation on performance, Havemann et al. 98 found that 7 days of a high-fat diet (68%) followed by 1 day of high-carbohydrate diet (90%) expectedly increased fat oxidation, but decreased 1-km sprint power output in well-trained cyclists. Stellingwerff et al. 99 compared substrate utilization, glycogenolysis, and enzymatic activity from either 5 days of a high-fat diet (67%) or high-carbohydrate (70%) followed by one day of high-carbohydrate with no training, followed by experimental trials on the seventh day. The high-fat diet increased fat oxidation, but also lowered pyruvate dehydrogenase activity and decreased glycogenolysis. These results provide a mechanistic explanation for the impairment in high-intensity work output as a result of high-fat, carbohydrate-restricted diets 100, 101, 102. Recently, an performance impairment effect from ketoadaptation has been observed at lower intensities as well. Burke et al. 103 reported that after 3 weeks on a ketogenic diet at a slight energy deficit, elite race walkers showed increased fat oxidation and aerobic capacity. However, this was accompanied by a reduction in exercise economy (increased oxygen demand for a given speed). The linear and non-linear high-carbohydrate diets in the comparison both caused significant performance improvements, while no significant improvement was seen in the ketogenic diet (there was a nonsignificant performance decrease). It is notable that Paoli et al. 104 found no decrease in bodyweight-based strength performance in elite artistic gymnasts during 30 days of ketogenic diet. Furthermore, the ketogenic diet resulted in significant loss of fat mass (1.9 kg) and non-significant gain of lean mass (0.3 kg). However, unlike Burke et al.’s study, which equated protein between groups (~2.2 g/kg), Paoli et al.’s protein intakes were skewed in favor of the ketogenic diet (2.9 vs. 1.2 g/kg). Wilson et al. 88 recently reported similar increases in strength and power in a protein and calorie-matched comparison of a ketogenic diet and a Western diet model, suggesting that ketogenic diet might have less ergolytic potential for strength training than it does for endurance training.
High-Protein diets
A common thread among high-protein diets (HPD) is that they have their various and subjective definitions. High-protein diets have been more generally defined as intakes reaching 105 or exceeding 25% of total energy 60. High-protein diets have also been identified as ranging from 1.2–1.6 g/kg 86. Classic work by Lemon et al. showed that protein consumed at double the Recommended Dietary Allowance (RDA) (1.6 g/kg) repeatedly outperformed the Recommended Dietary Allowance (0.8 g/kg) for preserving lean mass and reducing fat mass 106, 107. However, Pasiakos et al. 108 found that triple the Recommended Dietary Allowance (RDA) (2.4 g/kg) did not preserve lean mass to a significantly greater extent than double the Recommended Dietary Allowance (RDA). More recently, Longland et al. 109 found that in dieting conditions involving high-intensity interval sprints and resistance training, protein intake at 2.4 g/kg caused lean mass gains (1.2 kg) and fat loss (4.8 kg), while 1.2 g/kg resulted in preservation of lean mass (0.1 kg), and less fat loss (3.5 kg). A unique methodological strength in Longland et al.’s design was the use of the 4C model to assess body composition. Subjects were also provided all food and beverage intake, which added an extra layer of control and strengthened the findings. Augmenting this body of literature is Arciero et al.’s work on “protein-pacing” (4–6 meals/day, >30% protein per meal resulting in >1.4 g/kg/d), which has demonstrated this method’s superiority over conventional, lower-protein/lower-frequency diets for improving body composition in hypocaloric conditions 110, 111.
Of the macronutrients, protein has the highest thermic effect and is the most metabolically expensive. Given this, it is not surprising that higher protein intakes have been seen to preserve resting energy expenditure while dieting. Also, protein is the most satiating macronutrient, followed by carbohydrate, and fat being the least 112. A succession of recent meta-analyses 113, 114, 115 supports the benefit of higher protein intakes for reducing body weight, fat mass, and waist circumference, and preserving lean mass in an energy deficit. A systematic review by Helms et al. 28 suggested that protein intakes of 2.3–3.1 g/kg lean mass was appropriate for lean, resistance trained athletes in hypocaloric conditions. This is one of the rare pieces of literature that report protein requirements on the basis of lean mass rather than total body weight.
Antonio et al. 116 recently began a series of investigations of which can be considered super-high-protein diets. First in the series, the addition of dietary protein amounting to 4.4 g/kg for eight weeks in resistance-trained subjects did not significantly change body composition compared to control conditions of maintenance intake with habitual protein at 1.8 g/kg. Remarkably, the additional protein amounted to an ~800 kcal/day increase, and did not result in additional weight gain. A subsequent 8-week investigation involved resistance-trained subjects on a formally administered, periodized resistance training protocol 117. The high-protein group (HP) consumed 3.4 g/kg, while the normal-protein group (NP) consumed 2.3 g/kg. High-protein group (HP) and normal-protein group (NP) showed significant gains in lean mass (1.5 kg in both groups). A significantly greater fat mass decrease occurred in HP compared to NP (1.6 and 0.3 kg, respectively). This is intriguing, since high-protein group (HP) reported a significant increase caloric intake compared to baseline (374 kcal), while NP’s caloric increase was not statistically significant (103 kcal). A subsequent 8-week crossover trial 118 in resistance-trained subjects compared protein intakes of 3.3 versus 2.6 g/kg/d. A lack of significant differences in body composition and strength performance were seen despite a significantly higher caloric intake in HP vs. NP (an increase of 450 vs. 81 kcal above baseline). Antonio et al.’s most recent investigation 116 was a 1-year crossover trial using resistance-trained subjects, comparing protein intakes of 3.3 vs. 2.5 g/kg. In agreement with previous findings, there were no differences in body composition (importantly, no significant increase in fat mass), despite a significantly higher caloric intake in HP vs. NP (an increase of 450 vs. 81 kcal above baseline). This study also addressed health concerns about long-term high protein intakes (3–4 times the RDA) by demonstrating no adverse effects on a comprehensive list of measured clinical markers, including a complete metabolic panel and blood lipid profile 116.
An in-patient, metabolic ward study by Bray et al. 105 compared 8 weeks of hypercaloric conditions with protein at 5 (low protein), 15 (normal protein), and 25% of total energy (high protein). All three groups gained total body weight, but low protein lost 0.7 kg lean mass. Moreover, the normal protein and high protein groups gained 2.87 and 3.98 kg lean mass, respectively. All three groups gained body fat (3.51 kg) with no significant difference between groups. These results are seemingly at odds with Antonio et al.’s observations116. However, aside from the tighter control and surveillance inherent with metabolic ward conditions, Bray et al.’s subjects were untrained and remained sedentary throughout the study. Antonio et al.’s well-trained subjects were undergoing intensive resistance training and could have had an advantage regarding fuel oxidation and preferential nutrient partitioning toward lean body mass.
Speculation over the fate of the extra protein consumed in the Antonio et al. studies 116 may include a higher thermic effect of feeding, increased non-exercise activity thermogenesis (NEAT), increased thermic effect of exercise (ExEE), increased fecal energy excretion, reduced intake of the other macronutrients via increased satiety and suppressed hepatic lipogenesis. It should be noted as well that there might have been a misreporting of energy intake. Antonio et al.’s findings collectively suggest that the known thermic, satiating, and lean mass-preserving effects of dietary protein might be amplified in trained subjects undergoing progressive resistance exercise.
Intermittent Fasting
Intermittent fasting (IF) can be divided into three subclasses: alternate-day fasting (ADF), whole-day fasting (WDF), and time-restricted feeding (TRF) 119. The most extensively studied Intermittent fasting (IF) variant is alternate-day fasting (ADF), which typically involves a 24-hour fasting period alternated with a 24-hour feeding period. Complete compensatory intake on the feeding days (to offset the fasting days’ deficit) does not occur, and thus total weight loss and fat loss occurs on alternate-day fasting (ADF). Lean mass retention has been a surprisingly positive effect of alternate-day fasting (ADF) 120. However, lean mass loss in alternate-day fasting (ADF) conditions has also been observed by other investigators 121. The latter effect might be attributable to more severe energy deficits. The more lean mass-friendly is an energy-restricted period (~25% of maintenance requirements, typically in the form of a single meal at lunchtime) alternated with a 24-hour ad libitum (as desired) feeding period. Recently, Catenacci et al. 120 reported that alternate-day fasting (ADF) with zero caloric intake on the fasting days alternated with as desired feeding days showed similar results to daily caloric restriction on body composition, and slightly outperformed daily caloric restriction after 6-months of unsupervised weight loss maintenance. On the note of alternating fasting and feeding periods of the same length, alternate-week energy restriction (1 week on ~1300 kcal/day, one week on the usual diet) has only a single study to date, but is worth mentioning since it was as effective as continuous energy restriction for reducing body weight and waist girth at 8 weeks and 1 year 122.
Whole-day fasting (WDF) involves one to two 24-hour fasting periods throughout the week of otherwise maintenance intake to achieve an energy deficit. Of note, not all whole-day fasting (WDF) studies involve zero energy intake during the ‘fasting’ days. Although whole-day fasting (WDF) has been consistently effective for weight loss, Harvie et al. 123 saw no difference in body weight or body fat reduction between the whole-day fasting (2 ‘fasting’ days of ~647 kcal) group and controls when the weekly energy deficit was equated over a 6-month period. A subsequent study by Harvie et al. 124 compared daily energy restriction with two separate all whole-day fasting diets: one with two structured energy-restricted ‘fasting’ days per week, and one whose 2 ‘fasting’ days consisted of ad libitum protein and unsaturated fat. Both all whole-day fasting diets caused greater 3-month fat loss than daily energy restriction (3.7 vs. 2.0 kg). An important detail here is that at 3 months, 70% of the fasting days were completed in the all whole-day fasting groups while the daily energy restriction group achieved their targeted caloric deficit only 39% of the trial.
Time-restricted feeding (TRF) typically involves a fasting period of 16–20 hours and a feeding period of 4–8 hours daily. The most widely studied form of time-restricted feeding (TRF) is Ramadan fasting, which involves approximately 1 month of complete fasting (both food and fluid) from sunrise to sunset. Unsurprisingly, significant weight loss occurs, and this includes a reduction in lean mass as well as fat mass 35. Aside from Ramadan fasting studies, dedicated time-restricted feeding (TRF) research has been scarce until recently. An 8-week trial by Tinsley et al. 125 examined the effect of a 20-hour fasting/4-hour feeding protocol (20/4) done 4 days per week on recreationally active, but untrained subjects. No limitations were placed on the amounts and types of food consumed in the 4-hour eating window. A standardized resistance training program was administered 3 days per week. The time-restricted feeding (TRF) group lost body weight, due to a significantly lower energy intake (667 kcal less on fasting compared to non-fasting days). Cross sectional area of the biceps brachii and rectus femoris increased similarly in both the time-restricted feeding (TRF) and normal diet (ND) group. No significant changes in body composition (via DXA) were seen between groups. Despite a lack of statistical significance, there were notable effect size differences in lean soft tissue (ND gained 2.3 kg, while time-restricted feeding lost 0.2 kg). Although both groups increased strength without significant between-group differences, effect sizes were greater in the time-restricted feeding (TRF) group for bench press endurance, hip sled endurance, and maximal hip sled strength. This finding should be viewed cautiously given the potential for greater and more variable neurological gains in untrained subjects.
A subsequent study by Moro et al. 126 found that in resistance-trained subjects on a standardized training protocol, a 16-hour fasting/8-hour feeding cycle (16/8) resulted in significantly greater fat mass loss in time-restricted feeding vs. normal diet control group (ND) (1.62 vs. 0.31 kg), with no significant changes in lean mass in either group. Time-restricted feeding (TRF)’s meals were consumed at 1 pm, 4 pm, and 8 pm. ND’s meals were consumed at 8 am, 1 pm, and 8 pm. Macronutrient intake between the time-restricted feeding and ND groups was matched, unlike the aforementioned Tinsley et al. study 125 whereby protein intake was disparate and sub-optimal (1.0 g/kg in the time-restricted feeding group and 1.4 g/kg in the ND control group). Subjects in the present study’s time-restricted feedingand ND group consumed 1.93 and 1.89 g/kg, respectively. The mechanisms underlying these results are not clear. The authors speculated that increased adiponectin levels in the time-restricted feeding group could have stimulated mitochondrial biogenesis via interacting with PPAR-gamma, in addition to adiponectin acting centrally to increase energy expenditure. However, the time-restricted feeding group also experienced unfavorable changes such as decreased testosterone and triiodothyronine levels.
Seimon et al. 127 recently published the largest systematic review of IF research to date, comparing the effects of intermittent energy restriction (IER) to continuous energy restriction (CER) on body weight, body composition, and other clinical parameters. Their review included 40 studies in total, 12 of which directly compared an intermittent energy restriction with a continuous energy restriction condition. They found that overall, the two diet types resulted in “apparently equivalent outcomes” in terms of body weight reduction and body composition change. Interestingly, intermittent energy restriction was found to be superior at suppressing hunger. The authors speculated that this might be attributable to ketone production in the fasting phases. However, this effect was immaterial since on the whole, Intermittent Fasting (IF) failed to result in superior improvements in body composition or greater weight loss compared to continuous energy restriction.
Table 3. Diet categories
| Diet | Composition | Strengths | Limitations |
|---|---|---|---|
| Low-calorie diets (LCD) | LCD: 800–1200 kcal/day VLCD: 400–800 kcal/day | Rapid weight loss (1.0–2.5 kg/week, diets involve premade products that eliminate or minimize the need for cooking and planning. | VLCD have a higher risk for more severe side-effects, but do not necessary outperform LCD in the long-term |
| Low-fat diets (LFD) | LFD: 25–30% fat VLFD: 10–20% fat | LFD have the support of the major health organizations due to their large evidence basis in the literature on health effects. Flexible macronutrient range. Does not indiscriminately vilify foods based on carbohydrate content. | Upper limits of fat allowance may falsely convey the message that dietary fat is inherently antagonistic to body fat reduction. VLFD have a scarce evidence basis in terms of comparative effects on body composition, and extremes can challenge adherence. |
| Low-carbohydrate diets | 50–150 g carbohydrate, or up to 40% of kcals from carbohydrate | Defaults to higher protein intake. Large amount of flexibility in macronutrient proportion, and by extension, flexibility in food choices. Does not indiscriminately prohibit foods based on fat content. | Upper limits of carbohydrate allowance may falsely convey the message that carbohydrate is inherently antagonistic to body fat reduction. |
| Ketogenic diets (KD) | Maximum of ~50 g carbohydrate Maximum of ~10% carbohydrate | Defaults to higher protein intake. Suppresses appetite/controls hunger, causes spontaneous reductions in kcal intake under non-calorically restricted conditions. Simplifies the diet planning and decision-making process. | Excludes/minimizes high-carbohydrate foods which can be nutrient dense and disease-preventive. Can compromise high-intensity training output. Has not shown superior effects on body composition compared to non-KD when protein and kcals are matched. Dietary extremes can challenge long-term adherence. |
| High-protein diets (HPD) | HPD: ≥ 25% of total kcals, or 1.2–1.6 g/kg (or more) Super HPD: > 3 g/kg | HPD have a substantial evidence basis for improving body composition compared to RDA levels (0.8 g/kg), especially when combined with training. Super-HPD have an emerging evidence basis for use in trained subjects seeking to maximize intake with minimal-to-positive impacts on body composition. | May cause spontaneous reductions in total energy intake that can antagonize the goal of weight gain. Potentially an economical challenge, depending on the sources. High protein intakes could potentially displace intake of other macronutrients, leading to sub-optimal intakes (especially carbohydrate) for athletic performance goals. |
| Intermittent fasting (IF) | Alternate-day fasting (ADF): alternating 24-h fast, 24-h feed. Whole-day fasting (WDF): 1–2 complete days of fasting per week. Time-restricted feeding (TRF): 16–20-h fast, 4–8-h feed, daily. | ADF, WDF, and TRF have a relatively strong evidence basis for performing equally and sometimes outperforming daily caloric restriction for improving body composition. ADF and WDF have ad libitum feeding cycles and thus do not involve precise tracking of intake. TRF combined with training has an emerging evidence basis for the fat loss while maintaining strength. | Questions remain about whether IF could outperform daily linear or evenly distributed intakes for the goal of maximizing muscle strength and hypertrophy. IF warrants caution and careful planning in programs that require optimal athletic performance. |
Muscle Action
Most resistance training programs primarily include dynamic repetitions with both concentric (CON; muscle shortening) and eccentric (ECC; muscle lengthening) muscle actions, whereas isometric (ISOM; no net change in muscle length) actions play a secondary role (e.g., during nonagonist muscle stabilization, core strength, grip strength, pauses between eccentric (ECC) and concentric (CON) actions, or specific agonist ISOM exercises). Greater force per unit of muscle size is produced during eccentric (ECC) actions 129 than either CON or ISOM actions. Moreover, eccentric (ECC) actions require less motor unit activation per specific load 129, are less metabolically demanding 130, and are conducive to promoting hypertrophic adaptation 131 yet result in more pronounced delayed onset muscle soreness 132 as compared with concentric (CON) actions. Dynamic concentric (CON) muscular strength improvement is greatest when ECC actions are included with CON actions 133, and independently, ECC isokinetic training has been shown to produce greater muscle action-specific strength gains than CON training 134. The role of muscle action manipulation during resistance training is minimal with respect to overall progression because most programs include both CON and ECC actions in a given repetition. However, the inclusion of additional ISOM exercise may be beneficial. In some programs, the use of different forms of ISOM training, for example, functional ISOM 135 and supramaximal ECC actions (Keogh JWL, Wilson GJ, Weatherby RP. A cross-sectional comparison of different resistance training techniques in the bench press. J Strength Cond Res. 1999;13:247-58.)), has been reported to produce additional benefit. Specifically, certain ISOM actions have been recommended for promoting low back health and have been demonstrated effective for the selective recruitment of postural, spinal-stabilization musculature 136.
Repetition Speed
Less is known concerning the effect of repetition velocity on hypertrophy. In untrained individuals, fast (1:1) and moderate to slow (3:3) velocities of training produced similar changes in elbow flexor girth after 6 wk of training 137. However, 8 wk of fast (210°·s−1) ECC isokinetic training produced larger increases in Type II muscle fiber CSA than slow (20°/second) training 138, and 8 wk of fast ECC (180°·s−1) isokinetic training produced greater hypertrophy than slow ECC (30°/second), fast and slow CON training 134. For dynamic constant external resistance training, it has been suggested that higher velocities of movement pose less of a stimulus for hypertrophy than slow and moderate velocities. However, intentional slow velocities require significant reductions in loading and result in less of a blood lactate response and less metabolic response when total training time is equated 139. It does appear that the use of different velocities is warranted for long-term improvements in hypertrophy for advanced training.
It is recommended that slow to moderate velocities be used by novice- and intermediate-trained individuals. For advanced training, it is recommended that slow, moderate, and fast repetition velocities be used depending on the load, the repetition number, and the goals of the particular exercise 140, 141.
Exercise Selection
Both single- and multiple-joint exercises have been shown to be effective for increasing muscular strength in the targeted muscle groups using multiple modalities, for example, free weights, machines, cords, etc. 142, 143. Multiple-joint exercises, such as bench press and squat, require complex neural responses 144 and have generally been regarded more effective for increasing overall muscular strength because they enable a greater magnitude of weight to be lifted 145. Single-joint exercises, such as knee extensions and knee curls, have been used to target-specific muscle groups and pose a reduced level of skill and technical involvement. It is important to note that alterations in body posture, grip, and hand width/foot stance and position change muscle activation and alter the exercise. Thus, many variations or progressions of single- and multiple-joint exercises can be performed. Another way to vary exercise selection is to include unilateral as well as bilateral exercises. The level of muscle activation differs when an exercise is performed bilaterally versus unilaterally. Unilateral training may increase bilateral strength (in addition to unilateral strength), and bilateral training may increase unilateral strength 146. Unilateral training has been shown to improve some aspects of sports performance, such as single-leg jumping ability to a greater extent than bilateral training 146. Of interest has been the performance of single- and multiple-joint exercises in unstable environments, for example, with stability balls, wobble boards, and BOSU balls 147. These exercises have been shown to increase the activity of lower torso musculature and other stabilizer muscles (compared with stable environments); however, the magnitude of agonist force production is considerably lower resulting in lighter weights lifted 148. There are a multitude of exercises that can be performed in a variety of conditions that leaves many options for resistance training variation.
Adding High-Intensity Interval Training (HIIT) Workout To Your Weight Training Program
Traditionally, resistance training often is performed separately from aerobic training — typically on two or three nonconsecutive days each week. The American College of Sports Medicine recommends 8 to 12 repetitions of a resistance training exercise for each major muscle group at an intensity of 40% to 80% of a one-repetition max (1RM) depending on the training level of the participant. Two to three minutes of rest is recommended between exercise sets to allow for proper recovery. Two to four sets are recommended for each muscle group 149.
Standard guidelines for aerobic training recommend 150 minutes per week of moderate-intensity exercise (46% to 63% of maximal oxygen uptake, VO2max) for 30 to 60 minutes per session and/or 75 minutes per week of vigorous-intensity exercise (64% to 90% V˙O2max) for 20 to 60 minutes per session 149.
To address the limitations of traditional exercise protocols and provide an effective and efficient program for you, one of the exercise strategies to use is high intensity interval training (HIIT) using body weight as resistance. The approach combines aerobic and resistance training into a single exercise bout lasting approximately 7 minutes. Participants can repeat the 7-minute bout 2 to 3 times, depending on the amount of time you have. As body weight provides the only form of resistance, the program can be done anywhere.
High intensity interval training programs include short bursts of high-intensity activity performed at maximal effort (80-95 percent peak oxygen intake or VO2 max), separated by short periods of low-intensity work that allow partial recovery. The recovery periods may last equally as long as the work periods and are usually performed at 40% to 50% of a person’s estimated maximal heart rate. The workout continues with the alternating work and relief periods totaling 20 to 60 minutes. Two HIIT sessions a week is plenty, in addition to your other weight training workouts.
High-intensity interval training involves repeated short (<45 seconds) to long (2-4 minutes) bouts of rather high-intensity exercise interspersed with recovery periods. A typical high-intensity interval training session might include a three-minute warmup, four to six repetitions of a 30-second sprint followed by a 60-second active recovery, and a three-minute cool-down 150. High intensity interval training is not as complicated as you might think. Interval training is simply alternating bursts of intense activity with intervals of lighter activity. For instance, if your exercise is walking — if you’re in good shape, you might incorporate short bursts of jogging into your regular brisk walks. If you’re less fit, you might alternate leisurely walking with periods of faster walking. For example, if you’re walking outdoors, you could walk faster between certain mailboxes, trees or other landmarks.
High-Intensity Interval Resistance Training (HIRT) can be a fast and efficient way to lose excess body weight and body fat 151, 152, 153, 154. It has been proposed that short period resistance training could play a role in weight control by increasing resting energy expenditure but the effects of different kinds of resistance training has not been widely reported. The incorporated resistance training contributes significantly to the amount of fat burned during a workout 155. When resistance training exercises using multiple large muscles are used with very little rest between sets, they can elicit aerobic and metabolic benefits 156, 157, 152. Research has found that these metabolic benefits can be present for up to 72 hours after a high-intensity exercise bout has been completed 158.
There also may be a greater impact on subcutaneous fat loss with high-intensity intermittent circuit-style resistance training protocols than with traditional steady state sustained-effort aerobic work or traditional resistance training. This is thought to be from the increased level of catecholamines and growth hormone found in the blood both during and after high-intensity resistance training exercise with shortened rest periods (<30 seconds) 159, 152.
Shorter rest periods result in a shorter total exercise time. This is attractive to individuals who are trying to maximize the impact of an exercise program in minimal time.
In a small study involving 17 men doing resistance training, who were separated into doing the High-Intensity Interval Resistance Training (HIRT) consisting of: 6 repetitions, 20 seconds rest, 2/3 repetitions, 20 secs rest, 2/3 repetitions with 2 mins 30 seconds rest between sets, three exercises for a total of 7 sets. And the Traditional Resistance Training consisted of eight exercises of 4 sets of 8–12 repetitions with one/two minutes rest with a total amount of 32 sets. The researchers measured basal resting energy expenditure before the exercise and at 22 hours after the training session.
This data 160 suggest that shorter high-intensity interval resistance training sessions may increase resting energy expenditure at 22 hours after exercise to a greater extent than traditional resistance training and improving fat oxidation. The shorter exercise time commitment may help to reduce one major barrier to exercise.
Free Weights and Machines
Weight machines have been regarded as safer to use, easy to learn, and allow performance of some exercises that may be difficult with free weights, for example, knee extension. Machines help stabilize the body and limit movement about specific joints involved in synergistic force production, and machine exercises have demonstrated less neural activation when matched for intensity for most comparisons to free-weight exercises 161. Unlike machines, free weights may result in a pattern of intra- and intermuscular coordination that mimics the movement requirements of a specific task. Both free weights and machines are effective for increasing strength. Research shows that free-weight training leads to greater improvements in free-weight tests and machine training results in greater performance on machine tests 162. When a neutral testing device is used, strength improvement from free weights and machines appears similar 163. The choice to incorporate free weights or machines should be based on level of training status and familiarity with specific exercise movements as well as the primary training objective.
Exercise Order
The sequencing of exercises significantly affects the acute expression of muscular strength 164. This also applies when exercises are sequenced based on agonist/antagonist muscle group relationships. Muscle force and power may be potentiated when opposing exercises (antagonist movements) are performed 165; however, force and power may be reduced if the exercises are performed consecutively 166. Studies show that multiple-joint exercise (bench press, squat, leg press, and shoulder press) performance declines significantly when these exercises are performed later (after several exercises stressing similar muscle groups) rather than early in a workout 167. Considering that these multiple-joint exercises have been shown to be effective for increasing strength, maximizing performance of these exercises by performing them early in a workout may be necessary for optimal strength gains 168.
Recommendations for sequencing exercises for novice, intermediate, and advanced strength training for total body (all muscle groups trained in the workout), upper/lower body split (upper-body musculature trained 1 d and lower-body musculature trained another day), and muscle group split (individual muscle groups trained during a workout) workouts include large muscle group exercises before small muscle group exercises, multiple-joint exercises before single-joint exercises, higher-intensity exercises before lower-intensity exercises, or rotation of upper and lower body or agonist-antagonist exercises, that is, exercise performed for a muscle group followed by an exercise for the opposing muscle group 169.
Rest Periods
The amount of rest between sets and exercises significantly affects metabolic, hormonal and cardiovascular responses to an acute bout during resistance exercise as well as performance of subsequent sets and training adaptations. Acute resistance exercise performance may be compromised with one versus 3-min rest periods 170, and strength recovery may not be complete within 3 min 171. Several studies have shown that the number of repetitions performed may be compromised with short rest intervals, and 3- to 5-min rest intervals produce less performance decrements than 30 s to 2 min 172. In untrained individuals, circuit RT programs (using minimal rest in between exercises) have been shown to produce modest increases in strength 173. However, most longitudinal training studies have shown greater strength increases with long versus short rest periods (e.g., 2-5 min vs 30-40 s [3,213,230]), and one study has shown a lack of strength increase with 40-s rest periods 174. It is important to note that rest period length will vary based on the complexity of a given exercise (e.g., Olympic lifts and variations require longer rest periods) and the primary objective for incorporating the exercise into the training program (i.e., not every exercise will use the same rest interval).
For novice, intermediate, and advanced training, it is recommended that rest periods of at least 2-3 min be used for core exercises using heavier loads (those exercises included specifically to improve maximal strength such as the squat and bench press).
For assistance exercises (those exercises complimentary to core exercises), a shorter rest period length of 1-2 min may suffice 175.
Muscular Loading
The load is the amount of weight lifted in a given set, which is based on a percentage of the 1-repetition maximum (1RM). The volume is the total number of exercises, repetitions, and sets that are performed in a given exercise session. Rest period is the time period between each set and exercise. Frequency refers to the number of exercise sessions per week. How to manipulate each of these for the optimal enhancement of strength, power, hypertrophy, or muscular endurance is described below.
Altering the training load affects the acute metabolic, hormonal, neural, and cardiovascular responses to resistance exercise. Depending on an individual’s training experience and current level of fitness, proper loading during resistance training encompasses one or more of the following loading schemes:
- Increasing load based on a percentage of 1 RM,
- Increasing absolute load based on a targeted repetition number, or
- Increasing loading within a prescribed zone (e.g., 8-12 RM).
The load required to increase maximal strength in untrained individuals is fairly low. Loads of 45-50% of 1 RM (and less) have been shown to increase dynamic muscular strength in previously untrained individuals 176. Light loads that can be lifted a maximum of 15-25 repetitions have been shown to increase strength in moderately trained individuals 177. It appears greater loading is needed with progression. At least 80% of 1 RM is needed to produce further neural adaptations and strength during resistance training in experienced lifters 178. Several pioneering studies indicated that training with loads corresponding to 1-6 RM (mostly 5-6 RM) was most conducive to increasing maximal dynamic strength 179. Strength increases have been shown to be greater using heavy weights for 3-5 RM compared with 9-11 and 20-28 RM 180. Although significant strength increases have been reported using loads corresponding to 8-12 RM and lighter (33,149,250), this loading range may be inferior for maximizing strength in advanced lifters 178. Research examining periodized resistance training has demonstrated a need for variable-intensity loading schemes 181. Contrary to early suggestions of 6 RM loading, it appears that using a variety of training loads is most conducive to maximizing muscular strength 181. Meta-analytical data have shown that 60% of 1 RM produced the largest effect sizes for strength increases in novice individuals whereas 80% of 1 RM produced the largest effect sizes for strength increases in trained individuals 182 and 85% of 1 RM was most effective in athletes 183. For novice individuals, it has been suggested that moderate loading (50-60% of 1 RM or less) be used initially as learning proper form, and technique is paramount. These dose-response data refer to average training dosages, that is, mean loads used for all exercises. Further, using a variety of loads appears to be most effective for long-term progression in muscular strength 143. Recent studies have shown that self-selected resistance training intensities are lower than what is recommended, for example, 38-58% of 1 RM 184. Thus, intensity needs to be prescribed above one’s threshold (based on targeted repetition number) for progression in experienced populations.
Training Volume
Training volume is a summation of the total number of repetitions performed during a training session multiplied by the resistance used (kg) and is reflective of the duration of which muscles are being stressed 185. Training volume has been shown to affect neural, hypertrophic, metabolic and hormonal responses and subsequent adaptations to resistance training. Altering training volume can be accomplished by changing the number of exercises performed per session, the number of repetitions performed per set, or the number of sets per exercise. Low-volume programs, for example, high load, low repetitions, moderate to high number of sets, have been characteristic of resistance training. Studies using two 186, 187, three 170, 188, four to five 133, 189, and six or more 190, 191 sets per exercise have all produced significant increases in muscular strength in both trained and untrained individuals. In direct comparison, studies have reported similar strength increases in novice individuals between two and three sets 192 and two and four sets 193, whereas three sets have been reported superior to one and two 194. Although little is known concerning the optimal number of sets performed per muscle group per session, a meta-analysis of 37 studies has shown that approximately eight sets per muscle group produced the largest effect size in athletes 195, 196.
Another aspect that has received considerable attention is the comparison of single- and multiple-set programs. In many of these studies, one set per exercise performed for 8-12 repetitions at a relatively slow velocity has been compared with both periodized and nonperiodized multiple-set programs. A common criticism of these investigations is that the number of sets per exercise was not controlled from other variables such as intensity, frequency, and repetition velocity. Notwithstanding this concern, most research investigations comparing single- versus multiple-set training for muscular fitness have examined the effects of a standard single-set training program relative to that of any number of possible multiple-set programs of varying intensity. This design has made the process of identifying a clear-cut prescription recommendation very difficult because these studies have yielded conflicting results. Several studies have reported similar strength increases between single- and multiple-set programs 197, 198, whereas others reported multiple-set programs superior 199, 200 in previously untrained individuals. Since 2002, six studies have shown multiple-set superiority for 33-100% of the dynamic strength assessments used, whereas the remaining dynamic strength assessments showed similar increases. These data have prompted the notion that untrained individuals respond favorably to both single- and multiple-set programs and formed the basis for the popularity of single-set training among general fitness enthusiasts 201. In resistance-trained individuals, multiple-set programs have been shown to be superior for strength enhancement 202, 170, 203 in all but one study 204. Among resistance-trained postmenopausal women, multiple-set training led to 3.5-5.5% strength increases, whereas single-set training led to −1% to 2% strength reductions 202. No comparative study has shown single-set training superior to multiple-set training in trained or untrained individuals.
The results of meta-analytical studies have shown multiple-set resistance training superior to single sets for strength enhancement in untrained 205, 182 and trained populations 206 and superior for strength increases for programs lasting 17-40 wk 206. These studies have shown that performing three to four sets per exercise produced the most substantial effect sizes 205, 182. Thus, it appears that both program types are effective for increasing strength in untrained to moderately trained individuals during relatively short-term training periods. Long-term studies support the contention that a moderate increase in training volume is needed for further improvement. However, there is a point where further increase in volume may be counterproductive. In weightlifters, a moderate volume was shown to be more effective for increasing strength than low or high volumes of training with similar intensity 207. The key factor may be variation of training volume (and its interaction with intensity) rather than absolute number of sets.
Muscular Strength
The ability to generate force is necessary for all types of movement. Muscle fiber cross-sectional area (CSA) is positively related to maximal force production 208. The arrangement of fibers according to their angle of pennation, muscle length, joint angle, and contraction velocity can alter the expression of muscular strength 209. Force generation is further dependent upon motor unit activation, and motor units are recruited according to their recruitment threshold that typically involves the activation of the slower (lower force-producing) motor units before the faster (higher force-producing) units, that is, size principle 210. Adaptations to resistance training enable greater force generation through numerous neuromuscular mechanisms. Muscle strength may increase significantly within the first week of training 211, and long-term strength enhancement manifests itself through enhanced neural function (e.g., greater recruitment, rate of discharge), increased muscle fiber cross-sectional are, changes in muscle architecture and possible adaptations to increased metabolites, for example, H+, for increased strength. The magnitude of strength enhancement is dependent on the type of program used and the careful prescription of muscle actions, intensity, volume, exercise selection and order, rest periods between sets, and frequency.
Muscular strength is the ability of a muscle or muscle group to exert a maximal external force.
- Load: 60-70% 1RM for novice to intermediate; 80-100% for advanced
- Volume: 1-3 sets of 8-12 repetitions for novice to intermediate; 2-6 sets of 1-8 repetitions for advanced
- Rest period: 2-3 min for higher intense exercises that use heavier loads; 1-2 minutes between the lower intense exercises with light load.
Muscular Power
Power is defined as the optimal amount of work performed in a given time period. Muscular power is the highest power output attainable during a particular movement, and is required in activities of daily living, sport, and work. For optimal improvements in muscular power, a light load of 0 to 60% of 1RM should be used for 3-6 repetitions over one to three sets per exercise.
- Load: 30-60% 1RM for upper body exercises; 0-60% 1RM for lower body exercises
- Volume: 1-3 sets of 3-6 repetitions per exercise
- Rest period: 2-3 min for higher intense exercises that use heavier loads; 1-2 minutes between the lower intense exercises with light load.
Muscular Hypertrophy
Muscular hypertrophy is the enhancement of muscle size.
- Load: 70-85% 1RM for novice to intermediate; 70-100% for advanced
- Volume: 1-3 sets of 8-12 repetitions for novice to intermediate; 3-6 sets of 1-12 repetitions for advanced
- Rest period: 2-3 min for higher intense exercises that use heavier loads; 1-2 minutes between the lower intense exercises with light loads.
Muscular Endurance
Local muscular endurance is the ability of a muscle or a muscle group to repeatedly exert a submaximal resistance.
- Load: lower than 70% of 1RM
- Volume: 2-4 sets of 10-25 repetitions
- Rest period: 30 seconds to 1-minute between each set.
Frequency
For all the above, it is recommended that novice individuals train the entire body 2-3 days per week. Intermediate individuals should train 3 days if using a total-body workouts or 4 days if using an upper/lower body split routine, training each major muscle group twice per week. Advanced lifters can train 4-6 days per week, training each major muscle group once to twice per week. At this level, muscle group split routines of one to three muscle groups trained per workout are common since this would allow a higher volume per muscle group. Elite weightlifters and bodybuilders may benefit from using very high frequencies such as, two workouts per day for 4-5 days per week.
Optimal resistance training frequency (the number of workouts per week) depends upon several factors such as volume, intensity, exercise selection, level of conditioning, recovery ability, and number of muscle groups trained per workout session. Numerous studies have used frequencies of two to three alternating days per week in previously untrained individuals 212. This frequency has been shown to be an effective initial frequency, whereas 1-2 days per week appears to be an effective maintenance frequency for those individuals already engaged in resistance training 213. In several studies comparing strength gains, 1) 3 d of training per week was superior to 1 day 214 and 2 days 215, 2) 3 days produced similar strength increases to 2 days per week when volume was equated 212, 3) 4 days per week was superior to three 216, 4) 2 days per week was superior to 1 day 217, and 5) 3-5 days per week was superior to 1 and 2 d 218. Meta-analytical data have shown that strength gains in untrained individuals were highest with a frequency of 3 days per week 182.
Optimal progression of frequency during advanced training varies considerably. It has been shown that football players training 4-5 days per week achieved better results than those who trained either 3 or 6 days per week 219. Advanced and elite weightlifters and bodybuilders use high-frequency training, for example, four to six sessions per week or more. Double-split routines (two training sessions per day with emphasis on different muscle groups) are common during training 220, which may result in 8-12 training sessions per week. Frequencies as high as 18 sessions per week have been reported in elite Olympic weightlifters 221. The rationale for high-frequency training is that frequent short sessions followed by periods of recovery, nutrition supplementation, and food intake allow for high-intensity training and performance (reduced fatigue). Häkkinen and Kallinen 222 reported greater increases in muscle cross-sectional area (CSA) and strength when training volume was divided into two sessions per day as opposed to one. Elite power lifters train 4-6 days per week 223. It is important to note that not all muscle groups are trained per workout during a high-frequency model of training. Meta-analytical data have shown that training a muscle group two times per week in advanced individuals yielded the highest effect size 224 and two to three times per week yielded similar effect sizes in athletes 195.
It is recommended that advanced lifters train 4-6 days per week. Elite weightlifters and bodybuilders may benefit from using very high frequency, for example, two workouts in 1 day for 4-5 days per week.
Overtraining
To reduce the risk of overtraining, a dramatic increase in volume should be avoided. It is recommended that a 2-10% increase in the load be applied when the individual can comfortably perform the current workload for one to two repetitions over the desired number on two consecutive training sessions.
Build Lean Muscle Workout
The American College of Sports Medicine (ACSM) recommends that a strength training program should be performed a minimum of two non-consecutive days each week, with one set of 8 to 12 repetitions for healthy adults or 10 to 15 repetitions for older and frail individuals 149. Eight to 10 exercises should be performed that target the major muscle groups 149. Examples of typical resistance exercises that can be performed using free-weights, machines, or body weight for the major muscle groups are:
Table 4. RESISTANCE TRAINING GUIDELINES AND EXERCISES
Free-Weight | Machine-Based | Body Weight | |
| Chest | Supine Bench Press | Seated Chest Press | Push-ups |
| Back | Bent-over Barbell Rows | Lat Pulldown | Pull-ups |
| Shoulders | Dumbell Lateral Raise | Shoulder Press | Arm Circles |
| Biceps | Barbell/Dumbell Curls | Cable Curls | Reverse Grip Pull-ups |
| Triceps | Dumbell Kickbacks | Pressdowns | Dips |
| Abdomen | Weighted Crunches | Seated “Abs” Machine | Crunches, Prone Planks |
| Quadriceps | Back Squats | Leg Extenstion | Body weight lunges |
| Hamstrings | Stiff-leg Deadlifts | Leg Curls | Hip-ups |
The American College of Sports Medicine (ACSM) stresses the importance of progressing resistance training programs to meet specific resistance training goals. Progression in resistance training may be defined as “the act of moving forward or advancing toward a specific goal over time until the target goal has been achieved,” whereas maintenance resistance training refers to programs designed to maintain the current level of muscular fitness 149. This can occur with specific trainable characteristics of muscular fitness, such as strength, power, muscle hypertrophy and local muscular endurance. These four factors will improve with almost any properly designed resistance training program, but will be fully enhanced by properly modifying the load, volume, rest period between sets, and the frequency of each workout.
Countless resistance training models can be effective if these principles are incorporated and manipulated into the design. The magnitude of improvement depends upon the individual’s training status and genetic predisposition 225. Progressive overload is the gradual increase of stress placed upon the body during exercise training. Among untrained or novice populations, physiological adaptations to an resistance training program may occur in a short period. Systematically increasing the demands placed upon the body is necessary for further improvement and may be accomplished through altering one or more of the following variables:
- Exercise intensity (i.e., absolute or relative resistance/load for a given exercise/movement) may be increased;
- Total repetitions performed at the current intensity may be increased;
- Repetition speed/tempo with submaximal loads may be altered according to goals;
- Rest periods may be shortened for endurance improvements or lengthened for strength and power training; and
- Training volume (total work represented as the product of the total number of repetitions performed and the resistance) may be gradually increased (e.g., 2.5-5% 75) (Table 2).
Table 5. Muscle Building Workout Plan
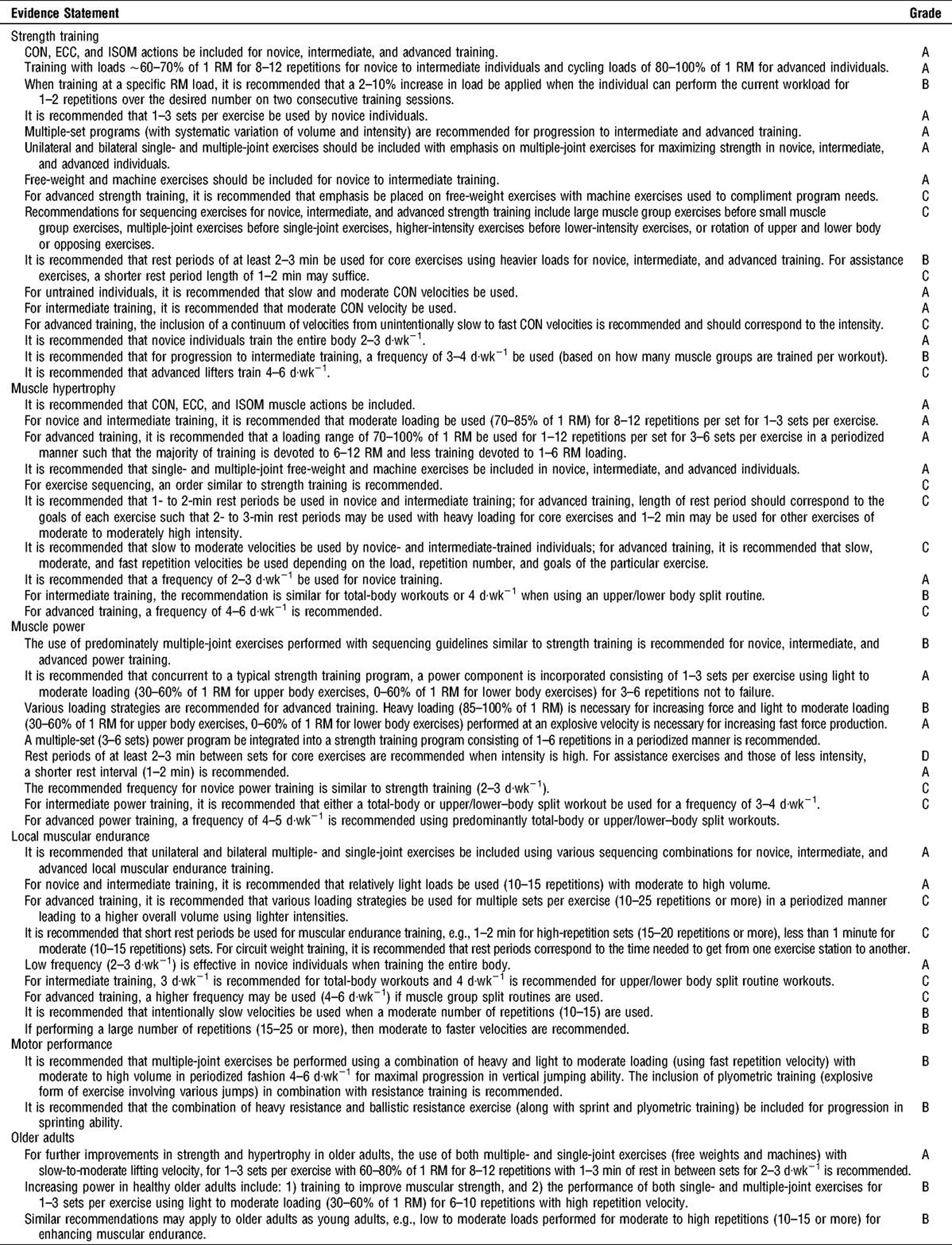
Note: CON = the motion of an active muscle while it is shortening under load (contracting) ; ECC = the motion of an active muscle while it is lengthening under load; ISOM = static strength training, involve muscular actions in which the length of the muscle does not change and there is no visible movement at the joint (no movement).

How to Build Lean Muscle for Females
Participation in sports is highly encouraged for girls – involvement in these organized activities has been proven to help improve girls’ social lives and prevent teen pregnancies. And exercise has been shown to boost mood and decrease depression in women and is an important part of leading a healthy lifestyle.
An important source of physical activity, which is often overlooked in young females due to social and cultural stigmas, is sport participation. Sport participation is great for building confidence and self-esteem while decreasing levels of depression. In addition, sport participation provides a means to build important life skills, such as teamwork and goal-setting, while having fun and staying in shape. Research has shown that young female athletes generally have higher academic test scores and are more likely to graduate from college.
There are also important health benefits obtained from participating in sports and physical activity. Young female athletes are generally healthier and have a lower prevalence of overweight and obesity throughout life, reducing their risk for other diseases, such as diabetes and heart disease. Sport participation is also an important component to building strong bones, which will decrease the risk of osteoporosis as they age.
Muscular strength and endurance is a component of fitness that is necessary for optimal well-being and quality of life. Unfortunately, the cost of joining a health club or gym is a major barrier for many people who want to do resistance training. Membership costs vary depending on the city and facility’s services, but fees generally range from $25 to $100 per month. Additional initiation fees may run into the hundreds. In addition, the inconvenience of traveling to a facility and working out with strangers is not appealing to everyone.
A cost-effective and convenient alternative to a gym membership is turning your living room or basement into your own personal training facility. Of course your home gym will not have expensive strength training machines, such as hip sleds or assisted pull-up machines. However, with a moderate investment and a good imagination, you can get a great workout in the comfort of your own home.
What You Need
- Space. You’ll need an open space that allows freedom of movement and is void of hazards that you might step on, bump into or trip over. A rearranged living room or an open garage stall with adequate traction will work well. You will need about 100 square feet (10′ x 10′).
- Equipment. Invest in a few dumbbells (new about $0.50 per pound) or resistance bands and a stability ball. Most strength training exercises can be performed with this basic equipment. An adjustable bench that changes angles for your upper body is not necessary, but it would offer additional variety.
- Plan. Don’t begin resistance training until you have developed a plan. It is important that you have a structured program that includes 8-10 exercises to target the major muscle groups of the body. It is always wise to consult a local fitness expert and follow the American College of Sports Medicine (ACSM) guidelines above for strength training. If you are a novice, a fitness professional will be able to give you advice beyond what is described here. Perform 1-3 sets of 8-12 repetitions at least twice a week. Make sure to do a brief warm-up before starting your session.
Tips for Strength Training
- Control the weight. It is important to perform each exercise in a controlled manner. Lower the weight slowly since you are working the same muscles as when you are lifting. To control speed of movement, try using a one-two-three count. The up phase (concentric or lifting) is completed quickly to a count of “one,” and the down phase (eccentric or lowering) is completed slowly to a count of “two-three.” To maintain sport performance and prevent injury throughout the whole range of motion, strengthening both phases of muscle contraction is important. Resistance exercise programs are therefore recommended for muscle health and strength across the age span. Eccentric strength is especially important for balance, mobility and physical functions such as walking down stairs or lowering objects to the ground. Traditional strength training eccentric programs typically involve lifting a weight in the concentric phase for 2 seconds and lower a weight in the eccentric phase for ~4-6 seconds to maximize strength gain. Because the muscle forces that are generated during slow eccentric overloading are high compared to traditional concentric resistance exercise, 3-5 days of rest should be provided between days of exercise. This recovery time allows the muscle to repair, adapt and prepare for the next exercise session.
- Breathe. Ideally, you should exhale when the weight is being raised and inhale when the weight is being lowered. Don’t ever hold your breath. It might help to count out loud the one-two-three count during the movement.
- Go to failure. An estimated 70 percent of strength gains can occur in the first set of training if performed to failure, otherwise called “rep out.” Failure or “repping out” means doing as many reps as possible for whatever resistance selected. Going to failure is challenging, but it will maximize your fitness response in a minimal amount of time. The takeaway is that you can get away with doing only one set if you perform that set to failure. Ideally, you should select a weight so that you fail between 8-12 repetitions. As you get stronger, you will need to increase the weight or the repetitions to elicit more gains.
- Progress slowly. The famous saying “Rome wasn’t built in a day” applies here. Don’t expect miraculous results immediately. Rather, work toward your goals slowly, and appreciate the process of being active. During your first few workouts, use a light resistance, focus on your form and don’t go to failure just yet. Also, be sure to allow time for recovery between sets (30-120 seconds) and between workouts (1-2 days). Your first few workouts might only last 15-20 minutes.
- Include variation. It is not unusual for workouts to become stale and for fitness gains to level off. These plateaus are expected and indicate that you are becoming more trained. Don’t get discouraged. If your workout gets old and boring, try different exercises and vary the number of repetitions, the weight or resistance, and the amount of rest between sets. These changes are likely to stimulate muscle adaptation and promote greater enjoyment of exercise.
Although it is impossible to improve at the same rate over long-term periods (e.g., >6 months), the proper manipulation of program variables (choice of resistance, exercise selection and order, number of sets and repetitions, frequency, and rest period length) can limit training plateaus and increase the ability to achieve a higher level of muscular fitness. Trainable characteristics include muscular strength, power, hypertrophy, and local muscular endurance. Variables such as speed and agility, balance, coordination, jumping ability, flexibility, and other measures of motor performance may be enhanced by resistance training. Resistance training, when incorporated into a comprehensive fitness program, improves cardiovascular function 227, reduces the risk factors associated with coronary heart disease 228 and non-insulin-dependent diabetes 229, prevents osteoporosis 230, may reduce the risk of colon cancer 231, promotes weight loss and maintenance 232, improves dynamic stability and preserves functional capacity 232, and fosters psychological well-being 233.
- Add on. Creating your own home gym is not a massive financial obligation and will not take much space. Over time, add more equipment to your collection, and continue to expand the possibilities of your home training center. For example, build on to your collection with a medicine ball, Bosu® ball or additional free weights.
- Do something. When it comes to strength training—and exercise in general—doing something is truly better than continuing to be sedentary. Of course, more is better than some, and it’s possible to train too much. It is not necessary to join a gym to enjoy the benefits of strength training. You can definitely do some in the comfort of your own home.
Full Body—A Sample Home Workout Plan
Squat—for hips, thighs and buttocks
- From the sitting position with your feet shoulder-width apart and your toes in front of your knees, lean forward slightly and stand up without locking your knees.
- Slowly lower your body back to a seated position where your upper legs are approximately parallel to the floor.
- Alternative—Place a stability ball between your middle-back and a wall, and lean back into the ball while performing these same movements.
Figure 1. Squat

Chest Press—for chest muscles and triceps
- Lie on your back with your feet flat and knees bent.
- Grip dumbbells and extend upward but don’t lock the elbows. Slowly lower to the starting position.
- Alternatives—Sit on a stability ball and perform same movement. Simple pushups also work these muscles. A variation in push-ups could be putting your feet on a chair simulating an incline chest press.
Figure 2. Chest Press

Back Extension—for buttocks (gluteals) and low back
- Lie face down on the floor.
- Raise left arm and right leg off the floor with head and neck in line with the arm. Hold for 1-2 seconds, and then slowly lower the arm and leg back to the starting position. Repeat this movement for the right arm and left leg.
- Alternative—Perform the movement on all fours or lying face down on a stability ball.
Figure 3. Back Extension

Standing Lunges—for front of thighs (quadriceps) and buttocks
- With one leg, step backward until the thigh of the forward leg is parallel to the ground or as far as feels comfortable. Your back knee should come close to the floor but not touch it.
- Push with the front leg, driving your heel into the floor, to return to the starting position.
- Alternative—Using a regular-height chair, do bench step-ups from the floor in an “up-up-down-down” pattern. To increase resistance in this exercise, hold dumbbells in your hands.
Figure 4. Standing Lunges
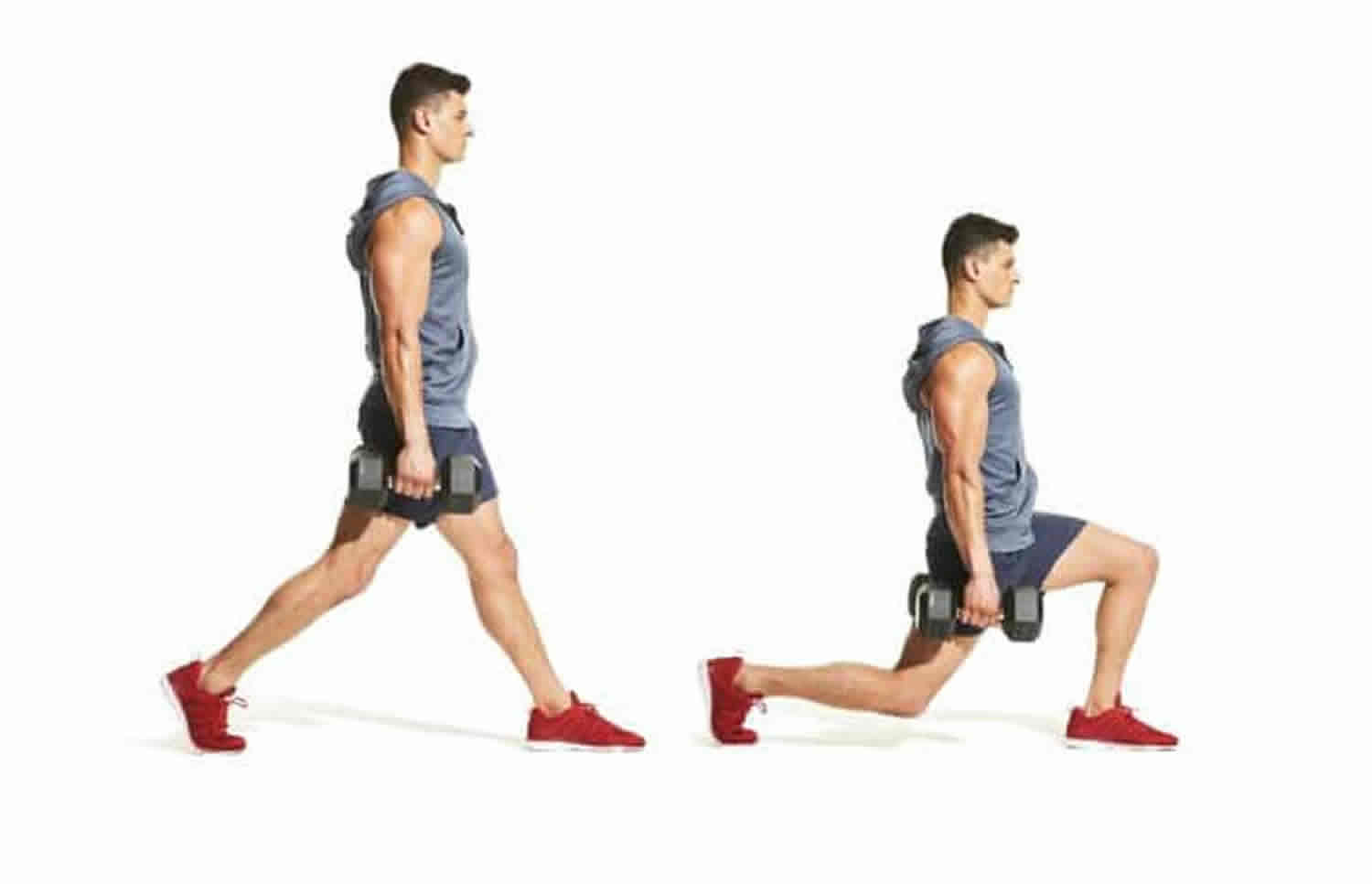
Dumbell Shoulder Press—for shoulders
- Perform this movement sitting in a regular chair, standing or sitting on a stability ball. Hold a dumbbell in each hand with an overhand grip. Make a 90-degree angle with your arms by raising the dumbbells so they are level with your ears.
- Slowly raise dumbbells over your head until arms are fully extended, but do not lock your elbows. Slowly lower the dumbbells to the starting position.
- Alternative—Perform a lateral raise by lifting the arms to the sides with a slight bend in the elbows. Keep the weights and arms below shoulder height. You will likely need lower weight for this exercise compared to shoulder press.
Figure 5. Dumbell Shoulder Press

Pelvic Tilt—for abdominals and buttocks
- Lie on the floor with feet flat on the ground and knees bent. Keep arms at your sides with palms facing the floor.
- Raise your pelvis so your buttocks and lower back are off the floor. Pause, and then slowly lower your pelvis to the floor.
- Alternatives—Perform a standard crunch while sitting on a stability ball or on the floor. Try a reverse curl by lying on your back and place arms to the side with the palms face down and knees bent. Raise the knees to the chest lifting the hips off the floor.
Figure 6. Pelvic Tilt

Leg Curl—for back of thighs (hamstrings)
- Stand behind a chair, and with your foot flexed, slowly bend one leg at the knee, raising your heel up toward your buttocks. Keep your support leg slightly bent.
- Slowly lower your foot back to the ground. Add ankle weights to increase resistance or use a resistance band.
- Alternative—Perform a hamstring roll using a stability ball. Lie on your back with your knees bent and your heels on the ball. Raise your hips off the floor and roll the ball away from you until your legs are straight. Roll the ball inward and outward.
Figure 7. Leg Curl
Dumbbell Row—for back musculature and biceps
- Stand with feet shoulder-width apart. Hold a dumbbell in each hand with elbows slightly bent. Bend forward at the waist and keep a slight bend in the knees.
- Pull dumbbells up to your sides until your upper arms are almost parallel to the ground. Slowly return the dumbbells to the starting position.
- Alternative—With resistance bands, stand on the band in its most middle section while holding the ends of the resistance band with your hands.
Figure 8. Dumbell Row
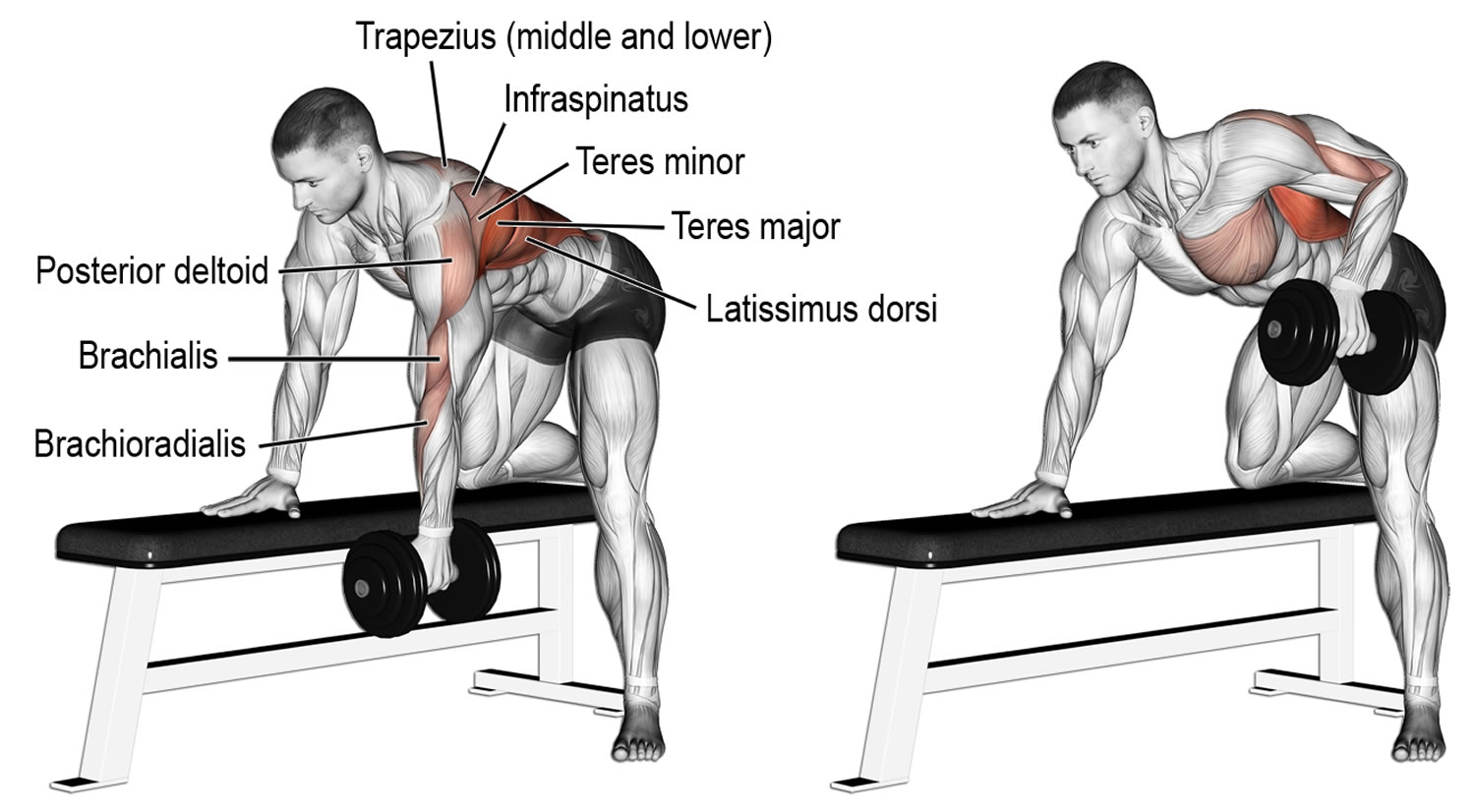
Biceps Curl—for biceps
- Stand with a dumbbell in each hand and your palms facing your thighs.
- Slowly lift the weights and rotate your forearm so that your palms end up facing your shoulders at the top of the movement. Slowly lower to the starting position so that your palms are facing your thighs.
- Alternative—With resistance bands, stand on the band in its most middle location while holding the ends of the resistance band with your hands while performing the movement.
Figure 9. Biceps Curl
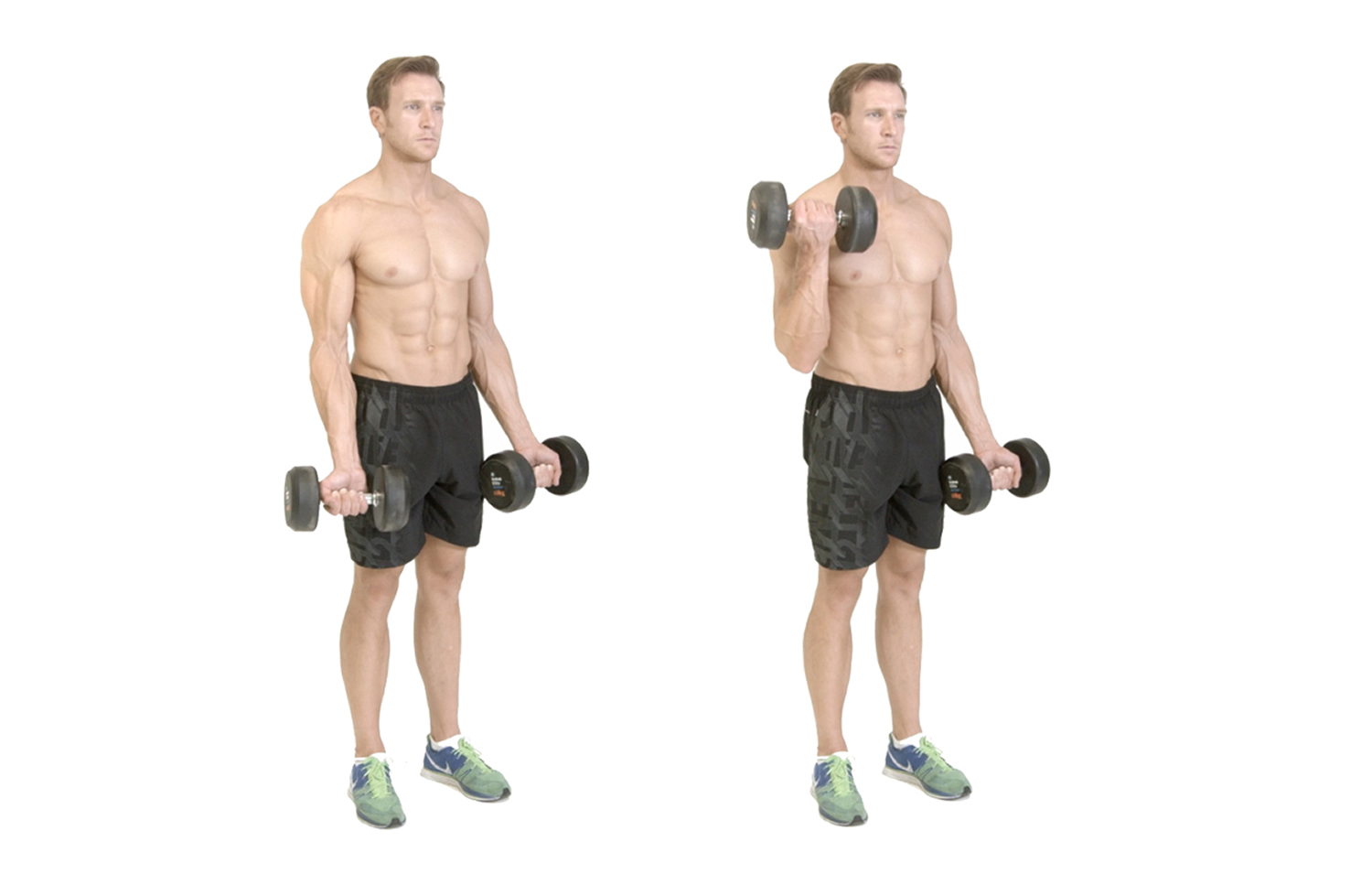
Side Plank—for core
- Lie on your side with left leg on top of the right. Raise upper body and place right elbow beneath the right shoulder.
- Your elbow should be bent at a 90-degree angle and resting on the ground. Hold for up to 60 seconds.
- Alternative—Perform a standard plank by lying face down resting on the forearms with your palms flat on the floor. Rise up onto your toes and rest on your elbows, keeping your back straight and flat.
Figure 10. Side Plank

Female Athlete Triad Syndrome
Over the past decade, more and more opportunities for females to become involved in sports have arisen and female sport participation is higher than ever. Girls who begin sports younger in life are more likely to continue being active as they get older; therefore, young females should be encouraged to find activities and sports that interest them so they can learn how to be physically active early in life and carry those habits with them as they get older. But with increasing pressure in today’s society to be extremely thin, some females take involvement in athletics or exercise too far. Fear of becoming overweight or out of shape can lead to the “Female Athlete Triad,” a condition that can lead to bone loss, stoppage of menstrual periods, and eating disorders. The actual prevalence is unknown. However, prevention of decreased energy availability aids the prevention of other health risks, including amenorrhea, low BMD, and fractures. Female athletes who suffer from disordered eating have been found to have a twofold to fourfold increased risk of developing a sports-related injury 234, 235.
The Female Athlete Triad 236 is a health concern for active women and girls who are driven to excel in sports. It involves three distinct and interrelated conditions:
- Disordered eating (a range of poor nutritional behaviors),
- Amenorrhea (irregular or absent menstrual periods) and
- Osteoporosis (low bone mass and microarchitectural deterioration, which leads to weak bones and risk of fracture).
Girls who participate in sports that emphasize thinness, such swimming or gymnastics, are especially at risk. Parents and coaches should not encourage weight loss, and should monitor young athletes’ eating habits to ensure they are not skipping meals or eating very little.
Any woman who may be experiencing the Triad should seek advice from a qualified sports medicine or exercise science professional, counselor, or dietician.
Causes of Female Athlete Triad
Exercise alone does not put someone at risk for developing the Triad; however, an energy deficit, in which caloric intake doesn’t match energy expenditure, is a risk factor. All women face societal pressure that “thin is in.” A young woman or girl who is determined to achieve a lean appearance or athletic success may attempt to excel through compulsive dieting and exercise. Such athletes are typically goal-oriented perfectionists. This misguided approach may lead to disordered eating, menstrual dysfunction and lower-than-normal bone mass formation.
Who is affected by the Female Athlete Triad
Females who participate in a sport where being thin or lean is considered ideal are at increased risk of sub-optimal energy availability or disordered eating, as defined by the original description of the female athlete triad. Athlete education about proper nutrition and energy status is crucial to prevent the negative consequences associated with the triad, particularly those involving bone and reproductive health.
Anyone may be affected, but women and girls participating in activities which emphasize leanness are at especially high risk. These activities can include:
- Bodybuilders
- Gymnastics
- Ballet
- Diving
- Figure skating
- Aerobics
- Running
Weight class sports associated with disordered eating in athletes, including males, are:
- Wrestling
- Rowing
- Martial arts.
DISORDERED EATING
In response to pressure to lose weight, women and girls may practice unhealthy weight-control methods, including restricted food intake, self-induced vomiting, consumption of appetite suppressants and diet pills, and use of laxatives and compounds to increase urination. Specific eating disorders are anorexia nervosa and bulimia. Many girls and women hide or deny their eating disorders due to embarrassment, shame, fear of losing control of their dieting and a mistaken believe that excessive weight loss enhances performance.
WARNING SIGNS OF EATING DISORDERS
- Excessive leanness or rapid weight loss;
- Preoccupation with weight, food, mealtime rituals and body image;
- Avoiding team meals, or secretive eating;
- Wide fluctuations in weight;
- Daily vigorous exercise in addition to regular training sessions;
- Stress fractures (i.e. microfractures of bones that may progress to complete fractures);
- Yellowing of the skin;
- Soft baby hair on the skin;
- Frequent sore throats despite no other signs of respiratory illness (self-induced vomiting);
- Chipmunk-like cheeks from swollen parotid glands (self-induced vomiting);
- Many dental cavities and/or foul breath (self-induced vomiting);
- Fatigue, light-headedness or dizziness; and
- Depression or low self-esteem.
EATING DISORDERS CAN BE FATAL
Eating disorders are serious, chronic medical and psychological illnesses. Individuals with untreated chronic anorexia or bulimia may die prematurely from heart
problems, blood electrolyte (i.e., salt) disorders, suicide or other health problems. If these disorders are recognized early, however, treatment may be effective.
Amenorrhea
An unbalanced diet, inadequate caloric intake relative to exercise level and excessive training may predispose females to menstrual abnormalities. Any female who hasn’t started menstruating by age 16, misses three consecutive periods or has periods that occur at intervals of greater than 35 days should be evaluated by a physician. Before attributing menstrual abnormalities to exercise, other conditions – such as pregnancy, abnormalities of the reproductive organs or thyroid disease – must be ruled out.
Osteoporosis
Osteoporosis refers to low bone mass and fragility of the skeleton. Low estrogen levels and other hormonal changes, which accompany irregular or absent menstrual periods, may predispose females to osteoporosis, especially in their teens and twenties when bone mass is accumulating. A 20-year-old woman without menses during her critical teenage growth period may have bone mass typical of a 70-year-old woman, predisposing her to stress fractures and fractures later in life. Adequate nutrition fosters good bone formation. Calcium requirements for teenage girls and young women with normal menses is 1,200 mg per day. Females with irregular or absent menses require 1,500 mg of calcium and 400 mg of Vitamin D per day.
How to prevent the Female Athlete Triad
Emphasis or pressure to achieve unrealistically low body weight should be avoided by coaches, parents, athletic administrators and health professionals. Out-of-competition “weigh-ins” should be discouraged. Rules governing sports should be examined, and rules encouraging excessive leanness should be eliminated or revised. Athletes and coaches should be encouraged to look for warning signs of eating disorders. Although the female athlete triad poses a great health risk, the benefits of participation in sports significantly outweigh the risks 237.
Any athlete who falls under the so-called umbrella of the triad should be questioned and educated regarding all of the components and potential health risks of this condition. By preventing premature bone loss in young female athletes, we can prevent future fragility fractures. Education of athletes is crucial to prevention. If athletes can understand the importance of optimal energy availability and how it directly affects bone and reproductive health, the pathology associated with the components of the triad may be avoided.
Early recognition and treatment of the Female Athlete Triad
Although individuals with disordered eating or amenorrhea may deny nutritional or health problems and are reluctant to seek care, medical attention is mandatory. An athlete should be reminded that medical care and proper nutrition may enhance performance. If an eating disorder or amenorrhea is suspected, the involved individual should be strongly encouraged or required to seek medical attention. If the individual refuses, the concerned coach, friend or parents should consult with a physician directly. Treatment and management of the Female Athlete Triad often requires a multidisciplinary approach, especially in patients with an eating disorder. A registered dietician, a primary care physician with expertise in treating athletes with the triad, psychologist and the support of family, friends, teammates and coaches are important members of the treatment team. In athletes diagnosed with an eating disorder (anorexia nervosa or bulimia) or low self-esteem, a psychiatrist or primary care physician may opt to prescribe antidepressants. However, the use of pharmacologic therapy has fallen
out of favor, and the current mainstay of treatment is to increase calorie intake, which leads to the resumption of menses and halts additional bone loss.
Build Lean Muscle Diet
Amino acids are major nutrient regulators of muscle protein turnover. After protein ingestion, hyperaminoacidemia stimulates increased rates of skeletal muscle protein synthesis, suppresses muscle protein breakdown and promotes net muscle protein gain for several hours 238. These acute observations form the basis for strategized protein intake to promote lean mass gain, or prevent lean mass loss over the long term. However, factors such as protein dose, protein source, and timing of intake are important in mediating the anabolic effects of amino acids on skeletal muscle and must be considered within the context of evaluating the reported efficacy of long-term studies investigating protein supplementation as part of a dietary strategy to promote lean mass accretion and/or prevent lean mass loss. Current research suggests that dietary protein supplementation can augment resistance exercise-mediated gains in skeletal muscle mass and strength and can preserve skeletal muscle mass during periods of diet-induced energy restriction 238. Perhaps less appreciated, protein supplementation can augment resistance training-mediated gains in skeletal muscle mass even in individuals habitually consuming ‘adequate’ (i.e., >0.8 g kg/day) protein. Additionally, overfeeding energy with moderate to high-protein intake (15–25 % protein or 1.8–3.0 g kg/day) is associated with lean, but not fat mass accretion, when compared to overfeeding energy with low protein intake (5 % protein or ~0.68 g kg/day) 238. Amino acids represent primary nutrient regulators of skeletal muscle anabolism, capable of enhancing lean mass accretion with resistance exercise and attenuating the loss of lean mass during periods of energy deficit, although factors such as protein dose, protein source, and timing of intake are likely important in mediating these effects.
Adequate Protein Consumption
In a review by Phillips and Van Loon 239, it is suggested that a protein intake of 1.8-2.7 g/kg for athletes training in hypocaloric conditions may be optimal. While this is one of the only recommendations existing that targets athletes during caloric restriction, this recommendation is not given with consideration to bodybuilders performing concurrent endurance and resistance training at very low levels of body fat. The collective agreement among reviewers is that a protein intake of 1.2-2.2 g/kg is sufficient to allow adaptation to training for athletes whom are at or above their energy needs 239, 240. However, bodybuilders during their contest preparation period typically perform resistance and cardiovascular training, restrict calories and achieve very lean conditions 241, 19. Each of these factors increases protein requirements and when compounded may further increase protein needs 242. Therefore, optimal protein intakes for bodybuilders during contest preparation may be significantly higher than existing recommendations. However, the recently published systematic review by Helms et al. 242 on protein intakes in resistance-trained, lean athletes during caloric restriction suggests a range of 2.3-3.1 g/kg of LBM, which may be more appropriate for bodybuilding. Moreover, the authors suggest that the lower the body fat of the individual, the greater the imposed caloric deficit and when the primary goal is to retain LBM, the higher the protein intake (within the range of 2.3-3.1 g/kg of LBM) should be.
Carbohydrate Intake
While it is true that resistance training utilizes glycogen as its main fuel source 243, total caloric expenditure of strength athletes is less than that of mixed sport and endurance athletes. Thus, authors of a recent review recommend that carbohydrate intakes for strength sports, including bodybuilding, be between 4–7 g/kg depending on the phase of training 244. However, in the specific case of a bodybuilder in contest preparation, achieving the necessary caloric deficit while consuming adequate protein and fat would likely not allow consumption at the higher end of this recommendation.
Satiety and fat loss generally improve with lower carbohydrate diets; specifically with higher protein to carbohydrate ratios 245, 246. In terms of performance and health, low carbohydrate diets are not necessarily as detrimental as typically espoused 247. In a recent review, it was recommended for strength athletes training in a calorically restricted state to reduce carbohydrate content while increasing protein to maximize fat oxidation and preserve LBM 239. However, the optimal reduction of carbohydrate and point at which carbohydrate reduction becomes detrimental likely needs to be determined individually.
While it appears low carbohydrate, high protein diets can be effective for weight loss, a practical carbohydrate threshold appears to exist where further reductions negatively impact performance and put one at risk for LBM losses. In support of this notion, researchers studying bodybuilders during the final 11 weeks of contest preparation concluded that had they increased carbohydrate during the final weeks of their diet they may have mitigated metabolic and hormonal adaptations that were associated with reductions in LBM 248.
Therefore, once a competitor has reached or has nearly reached the desired level of leanness, it may be a viable strategy to reduce the caloric deficit by an increase in carbohydrate. For example, if a competitor has reached competition body fat levels (lacking any visible subcutaneous fat) and is losing half a kilogram per week (approximately a 500 kcals caloric deficit), carbohydrate could be increased by 25-50 g, thereby reducing the caloric deficit by 100-200 kcals in an effort to maintain performance and LBM. However, it should be noted that like losses of lean body mass, decrements in performance may not affect the competitive outcome for a bodybuilder. It is possible that competitors who reach the leanest condition may experience unavoidable drops in performance.
Fat Intake
Body composition and caloric restriction may play greater roles in influencing testosterone levels that fat intake. During starvation, a reduction in testosterone occurs in normal weight, but not obese, males 249. In addition, rate of weight loss may influence testosterone levels. Weekly target weight loss rates of 1 kg resulted in a 30% reduction in testosterone compared to target weight loss rates of 0.5 kg per week in resistance trained women of normal weight 250.
Reductions in the percentage of dietary fat in isocaloric diets from approximately 40% to 20% has resulted in modest, but significant, reductions in testosterone levels 251. However, distinguishing the effects of reducing total dietary fat on hormonal levels from changes in caloric intake and percentages of saturated and unsaturated fatty acids in the diet is difficult 252. However, a drop in testosterone does not equate to a reduction in LBM. In direct studies of resistance trained athletes undergoing calorically restricted high protein diets, low fat interventions that maintain carbohydrate levels appear to be more effective at preventing LBM loses than lower carbohydrate, higher fat approaches. These results might indicate that attempting to maintain resistance training performance with higher carbohydrate intakes is more effective for LBM retention than attempting to maintain testosterone levels with higher fat intakes.
While cogent arguments for fat intakes between 20 to 30% of calories have been made to optimize testosterone levels in strength athletes 253, in some cases this intake may be unrealistic in the context of caloric restriction without compromising sufficient protein or carbohydrate intakes. While dieting, low carbohydrate diets may degrade performance 254 and lead to lowered insulin and IGF-1 which appear to be more closely correlated to LBM preservation than testosterone 248. Thus, a lower end fat intake between 15-20% of calories, which has been previously recommended for bodybuilders 255, can be deemed appropriate if higher percentages would reduce carbohydrate or protein below ideal ranges.
Table 6. Dietary recommendations for bodybuilding contest preparation
| Diet component | Recommendation |
|---|---|
| Protein (g/kg of LBM) | 2.3-3.1 |
| Fat (% of total calories) | 15-30% |
| Carbohydrate (% of total calories) | remaining |
| Weekly weight loss (% of body weight) | 0.5-1% |
Note: It must be noted that there is a high degree of variability in the way that individuals respond to diets. If training performance degrades it may prove beneficial to decrease the percentage of calories from dietary fat within these ranges in favor of a greater proportion of carbohydrate. Finally, while outside of the norm, some competitors may find that they respond better to diets that are higher in fat and lower in carbohydrate than recommended in this review. Therefore, monitoring of individual response over a competitive career is suggested. There is no evidence of any relationships with bone structure or regional subcutaneous fat distribution with any response to specific macronutrient ratios in bodybuilders or athletic populations. Bodybuilders, like others athletes, most likely operate best on balanced macronutrient intakes tailored to the energy demands of their sport 256. While the majority of competitors will respond best to the fat and carbohydrate guidelines proposed, the occasional competitor will undoubtedly respond better to a diet that falls outside of these suggested ranges. Careful monitoring over the course of a competitive career is required to determine the optimal macronutrient ratio for pre-contest dieting.
Timing and consumption of protein and/or carbohydrate during workouts
Questions remain about the utility of consuming protein and/or carbohydrate during bodybuilding-oriented training bouts. Since these bouts typically do not resemble endurance bouts lasting 2 hours or more, nutrient consumption during training is not likely to yield any additional performance-enhancing or muscle -sparing benefits if proper pre-workout nutrition is in place. In the exceptional case of resistance training sessions that approach or exceed two hours of exhaustive, continuous work, it might be prudent to employ tactics that maximize endurance capacity while minimizing muscle damage. This would involve approximately 8–15 g protein co-ingested with 30–60 g carbohydrate in a 6-8% solution per hour of training 257. Nutrient timing is an intriguing area of study that focuses on what might clinch the competitive edge. In terms of practical application to resistance training bouts of typical length, Aragon and Schoenfeld 258 recently suggested a protein dose corresponding with 0.4-0.5 g/kg bodyweight consumed at both the pre- and post-exercise periods. However, for objectives relevant to bodybuilding, the current evidence indicates that the global macronutrient composition of the diet is likely the most important nutritional variable related to chronic training adaptations. Table 7 below provides a continuum of importance with bodybuilding-specific context for nutrient timing.
Table 7. Continuum of nutrient & supplement timing importance
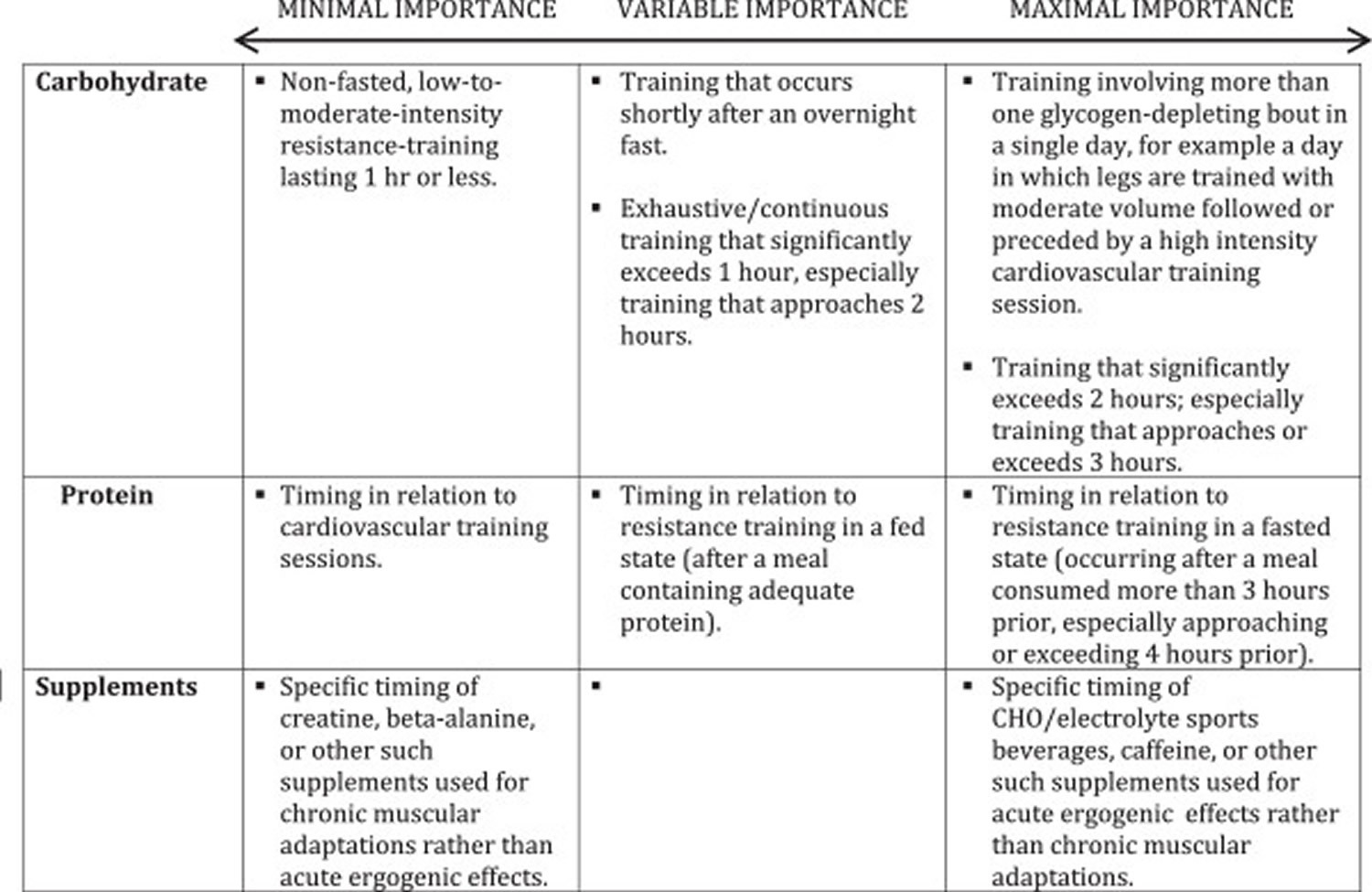
- Jéquier E. Pathways to obesity. Int J Obes Relat Metab Disord. 2002;26(Suppl 2):S12–7. doi: 10.1038/sj.ijo.0802123. https://www.ncbi.nlm.nih.gov/pubmed/12174324
- Halton T, Hu F. The effects of high protein diets on thermogenesis, satiety and weight loss: a critical review. J Am Coll Nutr. 2004;23(5):373–85. doi: 10.1080/07315724.2004.10719381. https://www.ncbi.nlm.nih.gov/pubmed/15466943
- von Loeffelholzn C. The Role of Non-exercise Activity Thermogenesis in Human Obesity. Updated 2014 Jun 5. In: De Groot LJ, Chrousos G, Dungan K, et al, editors Endotext . South Dartmouth (MA): MDText.com, Inc. Available from: https://www.ncbi.nlm.nih.gov/books/NBK279077/
- Pinheiro Volp A, Esteves de Oliveira F, Duarte Moreira Alves R, Esteves E, Bressan J. Energy expenditure: components and evaluation methods. Nutr Hosp. 2011;26(3):430–40. https://www.ncbi.nlm.nih.gov/pubmed/21892558
- Levine J. Nonexercise activity thermogenesis (NEAT): environment and biology. Am J Physiol Endocrinol Metab. 2004;286(5):E675–85. doi: 10.1152/ajpendo.00562.2003. https://www.ncbi.nlm.nih.gov/pubmed/15102614
- Levine J. Nonexercise activity thermogenesis–liberating the life-force. J Intern Med. 2007;262(3):273–87. doi: 10.1111/j.1365-2796.2007.01842.x. https://www.ncbi.nlm.nih.gov/pubmed/17697152
- Boguszewski C, Paz-Filho G, Velloso L. Neuroendocrine body weight regulation: integration between fat tissue, gastrointestinal tract, and the brain. Endokrynol Pol. 2010;61(2):194–206. https://www.ncbi.nlm.nih.gov/pubmed/20464707
- Barr S, Wright J. Postprandial energy expenditure in whole-food and processed-food meals: implications for daily energy expenditure. Food Nutr Res. 2010;54. doi: 10.3402/fnr.v54i0.5144. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2897733/
- Davis L, Coleman C, Kiel J, Rampolla J, Hutchisen T, Ford L, et al. Efficacy of a meal replacement diet plan compared to a food-based diet plan after a period of weight loss and weight maintenance: a randomized controlled trial. Nutr J. 2010;9:11. doi: 10.1186/1475-2891-9-11. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2851659/
- Aragon AA, Schoenfeld BJ, Wildman R, et al. International society of sports nutrition position stand: diets and body composition. Journal of the International Society of Sports Nutrition. 2017;14:16. doi:10.1186/s12970-017-0174-y. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5470183/
- McClave S, Snider H. Dissecting the energy needs of the body. Curr Opin Clin Nutr Metab Care. 2001;4(2):143–7. doi: 10.1097/00075197-200103000-00011. https://www.ncbi.nlm.nih.gov/pubmed/11224660
- Müller M, Wang Z, Heymsfield S, Schautz B, Bosy-Westphal A. Advances in the understanding of specific metabolic rates of major organs and tissues in humans. Curr Opin Clin Nutr Metab Care. 2013;16(5):501–8. https://www.ncbi.nlm.nih.gov/pubmed/23924948
- Hall KD. What is the required energy deficit per unit weight loss? Int J Obes. 2007;32:573–576. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2376744/
- Garthe I, Raastad T, Refsnes PE, Koivisto A, Sundgot-Borgen J. Effect of two different weight-loss rates on body composition and strength and power-related performance in elite athletes. Int J Sport Nutr Exerc Metab. 2011;21:97–104. https://www.ncbi.nlm.nih.gov/pubmed/21558571
- Hall KD. Body fat and fat-free mass inter-relationships: Forbes’s theory revisited. Br J Nutr. 2007;97:1059–1063. doi: 10.1017/S0007114507691946. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2376748/
- Mero AA, Huovinen H, Matintupa O, Hulmi JJ, Puurtinen R, Hohtari H, Karila T. Moderate energy restriction with high protein diet results in healthier outcome in women. J Int Soc Sports Nutr. 2010;7:4. doi: 10.1186/1550-2783-7-4. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2822830/
- Withers RT, Noell CJ, Whittingham NO, Chatterton BE, Schultz CG, Keeves JP. Body composition changes in elite male bodybuilders during preparation for competition. Aust J Sci Med Sport. 1997;29:11–16. https://www.ncbi.nlm.nih.gov/pubmed/9127683
- van der Ploeg GE, Brooks AG, Withers RT, Dollman J, Leaney F, Chatterton BE. Body composition changes in female bodybuilders during preparation for competition. Eur J Clin Nutr. 2001;55:268–277. doi: 10.1038/sj.ejcn.1601154. https://www.ncbi.nlm.nih.gov/pubmed/11360131
- Newton LE, Hunter GR, Bammon M, Roney RK. Changes in psychological state and self-reported diet during various phases of training in competitive bodybuilders. J Strength Cond Res. 1993;7:153–158.
- Forbes GB. Body fat content influences the body composition response to nutrition and exercise. Ann N Y Acad Sci. 2000;904:359–365. https://www.ncbi.nlm.nih.gov/pubmed/10865771
- Harvie MN, Pegington M, Mattson MP, Frystyk J, Dillon B, Evans G, Cuzick J, Jebb SA, Martin B, Cutler RG, Son TG, Maudsley S, Carlson OD, Egan JM, Flyvbjerg A, Howell A. The effects of intermittent or continuous energy restriction on weight loss and metabolic disease risk markers: a randomized trial in young overweight women. Int J Obes. 2011;35:714–727. doi: 10.1038/ijo.2010.171. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3017674/
- Soeters MR, Lammers NM, Dubbelhuis PF, Ackermans M, Jonkers-Schuitema CF, Fliers E, Sauerwein HP, Aerts JM, Serlie MJ. Intermittent fasting does not affect whole-body glucose, lipid, or protein metabolism. Am J Clin Nutr. 2009;90:1244–1251. doi: 10.3945/ajcn.2008.27327. https://www.ncbi.nlm.nih.gov/pubmed/19776143
- La Bounty PM, Campbell BI, Wilson J, Galvan E, Berardi J, Kleiner SM, Kreider RB, Stout JR, Ziegenfuss T, Spano M, Smith A, Antonio J. International Society of Sports Nutrition position stand: meal frequency. J Int Soc Sports Nutr. 2011;8:4. doi: 10.1186/1550-2783-8-4. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3070624/
- Compared with nibbling, neither gorging nor a morning fast affect short-term energy balance in obese patients in a chamber calorimeter. Taylor MA, Garrow JS. Int J Obes Relat Metab Disord. 2001 Apr; 25(4):519-28. https://www.ncbi.nlm.nih.gov/pubmed/11319656/
- Influence of the feeding frequency on nutrient utilization in man: consequences for energy metabolism. Verboeket-van de Venne WP, Westerterp KR. Eur J Clin Nutr. 1991 Mar; 45(3):161-9. https://www.ncbi.nlm.nih.gov/pubmed/1905998/
- Helms ER, Aragon AA, Fitschen PJ. Evidence-based recommendations for natural bodybuilding contest preparation: nutrition and supplementation. Journal of the International Society of Sports Nutrition. 2014;11:20. doi:10.1186/1550-2783-11-20. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4033492/
- Campbell B, Kreider R, Ziegenfuss T, La Bounty P, Roberts M, Burke D, et al. International Society of Sports Nutrition position stand: protein and exercise. J Int Soc Sports Nutr. 2007;4:8. doi: 10.1186/1550-2783-4-8. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2117006/
- Helms E, Zinn C, Rowlands D, Brown S. A systematic review of dietary protein during caloric restriction in resistance trained lean athletes: a case for higher intakes. Int J Sport Nutr Exerc Metab. 2014;24(2):127–38. doi: 10.1123/ijsnem.2013-0054. https://www.ncbi.nlm.nih.gov/pubmed/24092765
- Helms E, Aragon A, Fitschen P. Evidence-based recommendations for natural bodybuilding contest preparation: nutrition and supplementation. J Int Soc Sports Nutr. 2014;11:20. doi: 10.1186/1550-2783-11-20. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4033492/
- Bandegan A, Courtney-Martin G, Rafii M, Pencharz P, Lemon P. Indicator amino acid–derived estimate of dietary protein requirement for male bodybuilders on a non training day is several-fold greater than the current recommended dietary allowance. J Nutr. 2017;147(5):850-7. https://www.ncbi.nlm.nih.gov/pubmed/28179492
- Cermak NR, de PT, Groot LC S, WH van Loon LJ. Protein supplementation augments the adaptive response of skeletal muscle to resistance-type exercise training: a meta-analysis. Am J Clin Nutr. 2012;96(6):1454–64. doi: 10.3945/ajcn.112.037556. http://ajcn.nutrition.org/content/96/6/1454.long
- Phillips S, Van Loon L. Dietary protein for athletes: from requirements to optimum adaptation. J Sports Sci. 2011;29(Suppl 1):S29–38. doi: 10.1080/02640414.2011.619204. https://www.ncbi.nlm.nih.gov/pubmed/22150425
- Churchward-Venne T, Murphy C, Longland T, Phillips S. Role of protein and amino acids in promoting lean mass accretion with resistance exercise and attenuating lean mass loss during energy deficit in humans. Amino Acids. 2013;45(2):231–40. doi: 10.1007/s00726-013-1506-0. https://www.ncbi.nlm.nih.gov/pubmed/23645387
- Attarzadeh Hosseini S, Sardar M, Hejazi K, Farahati S. The effect of ramadan fasting and physical activity on body composition, serum osmolarity levels and some parameters of electrolytes in females. Int J Endocrinol Metab. 2013;11(2):88–94. doi: 10.5812/ijem.9602. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3693661/
- Norouzy A, Salehi M, Philippou E, Arabi H, Shiva F, Mehrnoosh S, Mohajeri SMR, Reza Mohajeri SA, Motaghedi Larijani A, Nematy M. Effect of fasting in Ramadan on body composition and nutritional intake: a prospective study. J Hum Nutr Diet. 2013;26(Suppl. 1):97–104. https://www.ncbi.nlm.nih.gov/pubmed/23679071
- Time-restricted feeding in young men performing resistance training: A randomized controlled trial. Tinsley GM, Forsse JS, Butler NK, Paoli A, Bane AA, La Bounty PM, Morgan GB, Grandjean PW. Eur J Sport Sci. 2017 Mar; 17(2):200-207. https://www.ncbi.nlm.nih.gov/pubmed/27550719/
- Effects of eight weeks of time-restricted feeding (16/8) on basal metabolism, maximal strength, body composition, inflammation, and cardiovascular risk factors in resistance-trained males. Moro T, Tinsley G, Bianco A, Marcolin G, Pacelli QF, Battaglia G, Palma A, Gentil P, Neri M, Paoli A. J Transl Med. 2016 Oct 13; 14(1):290. https://www.ncbi.nlm.nih.gov/pubmed/27737674/
- Do intermittent diets provide physiological benefits over continuous diets for weight loss? A systematic review of clinical trials. Seimon RV, Roekenes JA, Zibellini J, Zhu B, Gibson AA, Hills AP, Wood RE, King NA, Byrne NM, Sainsbury A. Mol Cell Endocrinol. 2015 Dec 15; 418 Pt 2():153-72. https://www.ncbi.nlm.nih.gov/pubmed/26384657/
- Kleiner SM, Bazzarre TL, Litchford MD. Metabolic profiles, diet, and health practices of championship male and female bodybuilders. J Am Diet Assoc. 1990;90:962–967. https://www.ncbi.nlm.nih.gov/pubmed/2365938
- Hickson JF Jr, Johnson TE, Lee W, Sidor RJ. Nutrition and the precontest preparations of a male bodybuilder. J Am Diet Assoc. 1990;90:264–267. https://www.ncbi.nlm.nih.gov/pubmed/2303663
- Andersen RE, Barlett SJ, Morgan GD, Brownell KD. Weight loss, psychological, and nutritional patterns in competitive male body builders. Int J Eat Disord. 1995 Jul;18(1):49-57. https://www.ncbi.nlm.nih.gov/pubmed/7670443
- Balon TW, Horowitz JF, Fitzsimmons KM. Effects of carbohydrate loading and weight-lifting on muscle girth. Int J Sport Nutr. 1992;2:328–334. https://www.ncbi.nlm.nih.gov/pubmed/1299502
- Costill DL, Cote R, Fink W. Muscle water and electrolytes following varied levels of dehydration in man. J Appl Physiol. 1976;40:6–11. https://www.ncbi.nlm.nih.gov/pubmed/1248983
- Maestu J, Eliakim A, Jurimae J, Valter I, Jurimae T. Anabolic and catabolic hormones and energy balance of the male bodybuilders during the preparation for the competition. J Strength Cond Res. 2010;24:1074–1081. doi: 10.1519/JSC.0b013e3181cb6fd3. https://www.ncbi.nlm.nih.gov/pubmed/20300017
- Bamman MM, Hunter GR, Newton LE, Roney RK, Khaled MA. Changes in body composition, diet, and strength of bodybuilders during the 12 weeks prior to competition. J Sports Med Phys Fitness. 1993;33:383–391. https://www.ncbi.nlm.nih.gov/pubmed/8035587
- Walberg-Rankin J, Edmonds CE, Gwazdauskas FC. Diet and weight changes of female bodybuilders before and after competition. Int J Sport Nutr. 1993;3:87–102. https://www.ncbi.nlm.nih.gov/pubmed/8499941
- Shephard RJ. Electrolyte manipulation in female body-builders. Br J Sports Med. 1994;28:60–61. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1332163/
- Joosen A, Westerterp K. Energy expenditure during overfeeding. Nutr Metab (Lond) 2006;3:25. doi: 10.1186/1743-7075-3-25. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1543621/
- Changes in energy expenditure resulting from altered body weight. Leibel RL, Rosenbaum M, Hirsch J. N Engl J Med. 1995 Mar 9; 332(10):621-8. https://www.ncbi.nlm.nih.gov/pubmed/7632212/
- Determinants of 24-hour energy expenditure in man. Methods and results using a respiratory chamber. Ravussin E, Lillioja S, Anderson TE, Christin L, Bogardus C. J Clin Invest. 1986 Dec; 78(6):1568-78. https://www.ncbi.nlm.nih.gov/pubmed/3782471/
- Joosen AM, Westerterp KR. Energy expenditure during overfeeding. Nutrition & Metabolism. 2006;3:25. doi:10.1186/1743-7075-3-25. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1543621/
- Ar L. Formula food-reducing diets:a new evidence-based addition to the weight management tool box. Nutr Bull. 2014;39(3):238–46. doi: 10.1111/nbu.12098. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4314695/
- Tsai A, Wadden T. The evolution of very-low-calorie diets: an update and meta-analysis. Obesity (Silver Spring) 2006;14(8):1283–93. doi: 10.1038/oby.2006.146. https://www.ncbi.nlm.nih.gov/pubmed/16988070
- Chang J, Kashyap S. The protein-sparing modified fast for obese patients with type 2 diabetes: what to expect. Cleve Clin J Med. 2014;81(9):557–65. doi: 10.3949/ccjm.81a.13128. https://www.ncbi.nlm.nih.gov/pubmed/25183847
- Saris W. Very-low-calorie diets and sustained weight loss. Obes Res. 2001;9(Suppl 4):295S–301S. doi: 10.1038/oby.2001.134. https://www.ncbi.nlm.nih.gov/pubmed/11707557
- Bryner R, Ullrich I, Sauers J, Donley D, Hornsby G, Kolar M, et al. Effects of resistance vs. aerobic training combined with an 800 calorie liquid diet on lean body mass and resting metabolic rate. J Am Coll Nutr. 1999;18(2):115–21. doi: 10.1080/07315724.1999.10718838. https://www.ncbi.nlm.nih.gov/pubmed/10204826
- Donnelly J, Sharp T, Houmard J, Carlson M, Hill J, Whatley J, et al. Muscle hypertrophy with large-scale weight loss and resistance training. Am J Clin Nutr. 1993;58(4):561–5. https://www.ncbi.nlm.nih.gov/pubmed/8379514
- Nackers L, Ross K, Perri M. The association between rate of initial weight loss and long-term success in obesity treatment: does slow and steady win the race? Int J Behav Med. 2010;17(3):161–7. doi: 10.1007/s12529-010-9092-y. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3780395/
- JE D, J J, S G. Diet and body composition. Effect of very low calorie diets and exercise. Sports Med. 1991;12(4):237–49. doi: 10.2165/00007256-199112040-00003. https://www.ncbi.nlm.nih.gov/pubmed/1784876
- Makris A, Foster G. Dietary approaches to the treatment of obesity. Psychiatr Clin North Am. 2011;34(4):813–27. doi: 10.1016/j.psc.2011.08.004. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3222874/
- Manore M. Exercise and the institute of medicine recommendations for nutrition. Curr Sports Med Rep. 2005;4(4):193–8. doi: 10.1097/01.CSMR.0000306206.72186.00. https://www.ncbi.nlm.nih.gov/pubmed/16004827
- La Berge A. How the ideology of low fat conquered America. J Hist Med Allied Sci. 2008;63(2):139–77. doi: 10.1093/jhmas/jrn001. https://www.ncbi.nlm.nih.gov/pubmed/18296750
- 2015 Dietary Guidelines Advisory Committee DGAC MEETING 1: Materials and Presentations. History of Dietary Guidance Development in the United States and the Dietary Guidelines for Americans. https://health.gov/dietaryguidelines/2015-binder/meeting1/docs/Minutes_DGAC_Mtg_1_508.pdf
- USDA, USDHHS. 2015 – 2020 Dietary Guidelines for Americans, 8th Edition: U.S. Government Printing Office; 2015. Available from: https://www.cnpp.usda.gov/2015-2020-dietary-guidelines-americans
- Hooper LAA, Bunn D, Brown T, Summerbell CD, Skeaff CM. Effects of total fat intake on body weight. Cochrane Database Syst Rev. 2015;7(8):CD011834. https://www.ncbi.nlm.nih.gov/pubmed/26250104
- Lissner L, Levitsky D, Strupp B, Kalkwarf H, Roe D. Dietary fat and the regulation of energy intake in human subjects. Am J Clin Nutr. 1987;46(6):886–92. https://www.ncbi.nlm.nih.gov/pubmed/3687822
- Kendall A, Levitsky D, Strupp B, Lissner L. Weight loss on a low-fat diet: consequence of the imprecision of the control of food intake in humans. Am J Clin Nutr. 1991;53(5):1124–9. https://www.ncbi.nlm.nih.gov/pubmed/2021123
- Karl J, Roberts S. Energy density, energy intake, and body weight regulation in adults. Adv Nutr. 2014;5(6):835–50. doi: 10.3945/an.114.007112. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4224224/
- Saquib N, Natarajan L, Rock C, Flatt S, Madlensky L, Kealey S, et al. The impact of a long-term reduction in dietary energy density on body weight within a randomized diet trial. Nutr Cancer. 2008;60(1):31–8. doi: 10.1080/01635580701621320. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2575113/
- Stubbs R, Whybrow S. Energy density, diet composition and palatability: influences on overall food energy intake in humans. Physiol Behav. 2004;81(5):755–64. doi: 10.1016/j.physbeh.2004.04.027. https://www.ncbi.nlm.nih.gov/pubmed/15234181
- Huang R, Huang C, Hu F, Chavarro J. Vegetarian diets and weight reduction: a meta-analysis of randomized controlled trials. J Gen Intern Med. 2016;31(1):109–16. doi: 10.1007/s11606-015-3390-7. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4699995/
- Gardner C, Kiazand A, Alhassan S, Kim S, Stafford R, Balise R, et al. Comparison of the Atkins, Zone, Ornish, and LEARN diets for change in weight and related risk factors among overweight premenopausal women: the A TO Z Weight Loss Study: a randomized trial. JAMA. 2007;297(9):969–77. doi: 10.1001/jama.297.9.969. https://www.ncbi.nlm.nih.gov/pubmed/17341711
- de Souza R, Bray G, Carey V, Hall K, LeBoff M, Loria C, et al. Effects of 4 weight-loss diets differing in fat, protein, and carbohydrate on fat mass, lean mass, visceral adipose tissue, and hepatic fat: results from the POUNDS LOST trial. Am J Clin Nutr. 2012;95(3):614–25. doi: 10.3945/ajcn.111.026328. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3278241/
- USDA, USDHHS. 2015 – 2020 Dietary Guidelines for Americans, 8th Edition: U.S. Government Printing Office; 2015. Available from: https://health.gov/dietaryguidelines
- Frigolet M, Ramos Barragán V, Tamez GM. Low-carbohydrate diets: a matter of love or hate. Ann Nutr Metab. 2011;58(4):320–34. doi: 10.1159/000331994. https://www.ncbi.nlm.nih.gov/pubmed/21985780
- Lara-Castro C, Garvey W. Diet, insulin resistance, and obesity: zoning in on data for Atkins dieters living in South Beach. J Clin Endocrinol Metab. 2004;89(9):4197–205. doi: 10.1210/jc.2004-0683. https://www.ncbi.nlm.nih.gov/pubmed/15356006
- Westman E, Feinman R, Mavropoulos J, Vernon M, Volek J, Wortman J, et al. Low-carbohydrate nutrition and metabolism. Am J Clin Nutr. 2007;86(2):276–84. https://www.ncbi.nlm.nih.gov/pubmed/17684196
- Hu T, Mills K, Yao L, Demanelis K, Eloustaz M, Yancy WJ, et al. Effects of low-carbohydrate diets versus low-fat diets on metabolic risk factors: a meta-analysis of randomized controlled clinical trials. Am J Epidemiol. 2012;176(Suppl 7):S44–54. doi: 10.1093/aje/kws264. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3530364/
- Mansoor N, Vinknes K, Veierød M, Retterstøl K. Effects of low-carbohydrate diets v. low-fat diets on body weight and cardiovascular risk factors: a meta-analysis of randomised controlled trials. Br J Nutr. 2016;115(3):466–79. doi: 10.1017/S0007114515004699. https://www.ncbi.nlm.nih.gov/pubmed/26768850
- Hashimoto Y, Fukuda T, Oyabu C, Tanaka M, Asano M, Yamazaki M, et al. Impact of low-carbohydrate diet on body composition: meta-analysis of randomized controlled studies. Obes Rev. 2016;17(6):499–509. doi: 10.1111/obr.12405. https://www.ncbi.nlm.nih.gov/pubmed/27059106
- Paoli A. Ketogenic diet for obesity: friend or foe? Int J Environ Res Public Health. 2014;11(2):2092–107. doi: 10.3390/ijerph110202092. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3945587/
- Paoli A, Rubini A, Volek J, Grimaldi K. Beyond weight loss: a review of the therapeutic uses of very-low-carbohydrate (ketogenic) diets. Eur J Clin Nutr. 2013;67(8):789–96. doi: 10.1038/ejcn.2013.116. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3826507/
- Hall K, Chen K, Guo J, Lam Y, Leibel R, Mayer L, et al. Energy expenditure and body composition changes after an isocaloric ketogenic diet in overweight and obese men. Am J Clin Nutr. 2016;104(2):324–33. doi: 10.3945/ajcn.116.133561. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4962163/
- Clifton P, Condo D, Keogh J. Long term weight maintenance after advice to consume low carbohydrate, higher protein diets–a systematic review and meta analysis. Nutr Metab Cardiovasc Dis. 2014;24(3):224–35. doi: 10.1016/j.numecd.2013.11.006. https://www.ncbi.nlm.nih.gov/pubmed/24472635
- Soenen S, Bonomi A, Lemmens S, Scholte J, Thijssen M, van Berkum F, et al. Relatively high-protein or ‘low-carb’ energy-restricted diets for body weight loss and body weight maintenance? Physiol Behav. 2012;107(3):374–80. doi: 10.1016/j.physbeh.2012.08.004. https://www.ncbi.nlm.nih.gov/pubmed/22935440
- Leidy H, Clifton P, Astrup A, Wycherley T, Westerterp-Plantenga M, Luscombe-Marsh N, et al. The role of protein in weight loss and maintenance. Am J Clin Nutr. 2015.
- Weigle D, Breen P, Matthys C, Callahan H, Meeuws K, Burden V, et al. A high-protein diet induces sustained reductions in appetite, ad libitum caloric intake, and body weight despite compensatory changes in diurnal plasma leptin and ghrelin concentrations. Am J Clin Nutr. 2005;82(1):41–8. https://www.ncbi.nlm.nih.gov/pubmed/16002798
- Wilson J, Lowery R, Roberts M, Sharp M, Joy J, Shields K, et al. The effects of ketogenic dieting on body composition, strength, power, and hormonal profiles in resistance training males. J Strength Cond Res. 2017. doi: 10.1519/JSC.0000000000001935. https://www.ncbi.nlm.nih.gov/pubmed/28399015
- Veum V, Laupsa-Borge J, Eng Ø, Rostrup E, Larsen T, Nordrehaug J, et al. Visceral adiposity and metabolic syndrome after very high-fat and low-fat isocaloric diets: a randomized controlled trial. Am J Clin Nutr. 2017;105(1):85–99. doi: 10.3945/ajcn.115.123463. https://www.ncbi.nlm.nih.gov/pubmed/27903520
- Stimson R, Johnstone A, Homer N, Wake D, Morton N, Andrew R, et al. Dietary macronutrient content alters cortisol metabolism independently of body weight changes in obese men. J Clin Endocrinol Metab. 2007;92(11):4480–4. doi: 10.1210/jc.2007-0692. https://www.ncbi.nlm.nih.gov/pubmed/17785367
- Hall K, Guo J. Obesity Energetics: Body Weight Regulation and the Effects of Diet Composition. Gastroenterology. Gastroenterology. 2017;152(7):1718-27. https://www.ncbi.nlm.nih.gov/pubmed/28193517
- Hall K. A review of the carbohydrate-insulin model of obesity. Eur J Clin Nutr. 2017;71(3):323–6. doi: 10.1038/ejcn.2016.260. https://www.ncbi.nlm.nih.gov/pubmed/28074888
- Jabekk P, Moe I, Meen H, Tomten S, Høstmark A. Resistance training in overweight women on a ketogenic diet conserved lean body mass while reducing body fat. Nutr Metab (Lond) 2010;7:17. doi: 10.1186/1743-7075-7-17. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2845587/
- Wood R, Volek J, Davis S, Dell’Ova C, Fernandez M. Effects of a carbohydrate-restricted diet on emerging plasma markers for cardiovascular disease. Nutr Metab (Lond) 2006;3:19. doi: 10.1186/1743-7075-3-19. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1481590/
- Sumithran P, Prendergast L, Delbridge E, Purcell K, Shulkes A, Kriketos A, et al. Ketosis and appetite-mediating nutrients and hormones after weight loss. Eur J Clin Nutr. 2013;67(7):759–64. doi: 10.1038/ejcn.2013.90. https://www.ncbi.nlm.nih.gov/pubmed/23632752
- Johnstone A, Horgan G, Murison S, Bremner D, Lobley G. Effects of a high-protein ketogenic diet on hunger, appetite, and weight loss in obese men feeding ad libitum. Am J Clin Nutr. 2008;87(1):44–55. https://www.ncbi.nlm.nih.gov/pubmed/18175736
- Gibson A, Seimon R, Lee C, Ayre J, Franklin J, Markovic T, et al. Do ketogenic diets really suppress appetite? a systematic review and meta-analysis. Obes Rev. 2015;16(1):64–76. doi: 10.1111/obr.12230. https://www.ncbi.nlm.nih.gov/pubmed/25402637
- Havemann L, West S, Goedecke J, Macdonald I, St Clair Gibson A, Noakes T, et al. Fat adaptation followed by carbohydrate loading compromises high-intensity sprint performance. J Appl Physiol. 2006;100(1):194–202. doi: 10.1152/japplphysiol.00813.2005. https://www.ncbi.nlm.nih.gov/pubmed/16141377
- Stellingwerff T, Spriet L, Watt M, Kimber N, Hargreaves M, Hawley J, et al. Decreased PDH activation and glycogenolysis during exercise following fat adaptation with carbohydrate restoration. Am J Physiol Endocrinol Metab. 2006;290(2):E380–8. doi: 10.1152/ajpendo.00268.2005. https://www.ncbi.nlm.nih.gov/pubmed/16188909
- Burke L. Re-examining high-fat diets for sports performance: Did we call the ‘nail in the coffin’ too soon? Sports Med. 2015;45(Suppl 1):S33–49. doi: 10.1007/s40279-015-0393-9. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4672014/
- Urbain P, Strom L, Morawski L, Wehrle A, Deibert P, Bertz H. Impact of a 6-week non-energy-restricted ketogenic diet on physical fitness, body composition and biochemical parameters in healthy adults. Nutr Metab (Lond). 2017;14. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5319032/
- Zajac A, Poprzecki S, Maszczyk A, Czuba M, Michalczyk M, Zydek G. The effects of a ketogenic diet on exercise metabolism and physical performance in off-road cyclists. Nutrients. 2014;6(7):2493–508. doi: 10.3390/nu6072493. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4113752/
- Burke L, Ross M, Garvican-Lewis L, Welvaert M, Heikura I, Forbes S, et al. Low carbohydrate, high fat diet impairs exercise economy and negates the performance benefit from intensified training in elite race walkers. 2016. doi: 10.1113/JP273230. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5407976/
- Paoli A, Grimaldi K, D’Agostino D, Cenci L, Moro T, Bianco A, et al. Ketogenic diet does not affect strength performance in elite artistic gymnasts. J Int Soc Sports Nutr. 2012;9(1):34. doi: 10.1186/1550-2783-9-34. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3411406/
- Bray G, Smith S, de Jonge L, Xie H, Rood J, Martin C, et al. Effect of dietary protein content on weight gain, energy expenditure, and body composition during overeating: a randomized controlled trial. JAMA. 2012;307(1):47–55. doi: 10.1001/jama.2011.1918. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3777747/
- Layman D, Evans E, Erickson D, Seyler J, Weber J, Bagshaw D, et al. A moderate-protein diet produces sustained weight loss and long-term changes in body composition and blood lipids in obese adults. J Nutr. 2009;139(3):514–21. doi: 10.3945/jn.108.099440. https://www.ncbi.nlm.nih.gov/pubmed/19158228
- Layman D, Evans E, Baum J, Seyler J, Erickson D, Boileau R. Dietary protein and exercise have additive effects on body composition during weight loss in adult women. J Nutr. 2005;135(8):1903–10. https://www.ncbi.nlm.nih.gov/pubmed/16046715
- Pasiakos S, Cao J, Margolis L, Sauter E, Whigham L, McClung J, et al. Effects of high-protein diets on fat-free mass and muscle protein synthesis followingweight loss: a randomized controlled trial. FASEB J. 2013;27(9):3837–47. doi: 10.1096/fj.13-230227. https://www.ncbi.nlm.nih.gov/pubmed/23739654
- Longland T, Oikawa S, Mitchell C, Devries M, Phillips S. Higher compared with lower dietary protein during an energy deficit combined with intense exercise promotes greater lean mass gain and fat mass loss: a randomized trial. Am J Clin Nutr. 2016;103(3):738–46. doi: 10.3945/ajcn.115.119339. https://www.ncbi.nlm.nih.gov/pubmed/26817506
- Arciero P, Ormsbee M, Gentile C, Nindl B, Brestoff J, Ruby M. Increased protein intake and meal frequency reduces abdominal fat during energy balance and energy deficit. Obesity (Silver Spring) 2013;21(7):1357–66. doi: 10.1002/oby.20296. https://www.ncbi.nlm.nih.gov/pubmed/23703835
- Arciero PE RC, Bunsawat K, Gentile C, Ketcham C, Darin C, Renna M, et al. Protein-pacing from food or supplementation improves physical performance in overweight men and women: the PRISE 2 study. Nutrients. 2016;8(5):E288. doi: 10.3390/nu8050288. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4882701/
- Pesta D, Samuel V. A high-protein diet for reducing body fat: mechanisms and possible caveats. Nutr Metab (Lond) 2014;11(1):53. doi: 10.1186/1743-7075-11-53. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4258944/
- Wycherley T, Moran L, Clifton P, Noakes M, Brinkworth G. Effects of energy-restricted high-protein, low-fat compared with standard-protein, low-fat diets: a meta-analysis of randomized controlled trials. Am J Clin Nutr. 2012;96(6):1281–98. doi: 10.3945/ajcn.112.044321. https://www.ncbi.nlm.nih.gov/pubmed/23097268
- Dong J, Zhang Z, Wang P, Qin L. Effects of high-protein diets on body weight, glycaemic control, blood lipids and blood pressure in type 2 diabetes: meta-analysis of randomised controlled trials. Br J Nutr. 2013;10(5):781–9. doi: 10.1017/S0007114513002055. https://www.ncbi.nlm.nih.gov/pubmed/23829939
- Santesso N, Akl E, Bianchi M, Mente A, Mustafa R, Heels-Ansdell D, et al. Effects of higher- versus lower-protein diets on health outcomes: a systematic review and meta-analysis. Eur J Clin Nutr. 2012;66(7):780–8. doi: 10.1038/ejcn.2012.37. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3392894/
- Antonio J, Ellerbroek A, Silver T, Vargas L, Tamayo A, Buehn R, et al. A high protein diet has no harmful effects: a one-year crossover study in resistance-trained males. J Nutr Metab. 2016;2016:9104792. doi: 10.1155/2016/9104792. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5078648/
- Antonio J, Ellerbroek A, Silver T, Orris S, Scheiner M, Gonzalez A, et al. A high protein diet (3.4 g/kg/d) combined with a heavy resistance training program improves body composition in healthy trained men and women–a follow-up investigation. J Int Soc Sports Nutr. 2015;12:39. doi: 10.1186/s12970-015-0100-0. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4617900/
- Antonio J, Ellerbroek A, Silver T, Vargas L, Peacock C. The effects of a high protein diet on indices of health and body composition–a crossover trial in resistance-trained men. J Int Soc Sports Nutr. 2016;13:3. doi: 10.1186/s12970-016-0114-2. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4715299/
- Tinsley G, La Bounty P. Effects of intermittent fasting on body composition and clinical health markers in humans. Nutr Rev. 2015;73(10):661–74. doi: 10.1093/nutrit/nuv041. https://www.ncbi.nlm.nih.gov/pubmed/26374764
- Catenacci V, Pan Z, Ostendorf D, Brannon S, Gozansky W, Mattson M, et al. A randomized pilot study comparing zero-calorie alternate-day fasting to daily caloric restriction in adults with obesity. Obesity (Silver Spring) 2016;24(9):1874–83. doi: 10.1002/oby.21581. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5042570/
- Hill J, Schlundt D, Sbrocco T, Sharp T, Pope-Cordle J, Stetson B, et al. Evaluation of an alternating-calorie diet with and without exercise in the treatment of obesity. Am J Clin Nutr. 1989;50(2):248–54. https://www.ncbi.nlm.nih.gov/pubmed/2667313
- Keogh J, Pedersen E, Petersen K, Clifton P. Effects of intermittent compared to continuous energy restriction on short-term weight loss and long-term weight loss maintenance. Clin Obes. 2014;4(3):150–6. doi: 10.1111/cob.12052. https://www.ncbi.nlm.nih.gov/pubmed/25826770
- Harvie M, Pegington M, Mattson M, Frystyk J, Dillon B, Evans G, et al. The effects of intermittent or continuous energy restriction on weight loss and metabolic disease risk markers: a randomized trial in young overweight women. Int J Obes (Lond) 2011;35(5):714–27. doi: 10.1038/ijo.2010.171. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3017674/
- Harvie M, Wright C, Pegington M, McMullan D, Mitchell E, et al. The effect of intermittent energy and carbohydrate restriction v. daily energy restriction on weight loss and metabolic disease risk markers in overweight women. Br J Nutr. 2013;110(8):1534–47. doi: 10.1017/S0007114513000792. https://www.ncbi.nlm.nih.gov/pubmed/23591120
- Tinsley G, Forsse J, Butler N, Paoli A, Bane A, La Bounty P, et al. Time-restricted feeding in young men performing resistance training: A randomized controlled trial. Eur J Sport Sci. 2017;17(2):200–7. doi: 10.1080/17461391.2016.1223173. https://www.ncbi.nlm.nih.gov/pubmed/27550719
- Moro T, Tinsley G, Bianco A, Marcolin G, Pacelli Q, Battaglia G, et al. Effects of eight weeks of time-restricted feeding (16/8) on basal metabolism, maximal strength, body composition, inflammation, and cardiovascular risk factors in resistance-trained males. J Transl Med. 2016;14(1):290. doi: 10.1186/s12967-016-1044-0. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5064803/
- Seimon R, Roekenes J, Zibellini J, Zhu B, Gibson A, Hills A, et al. Do intermittent diets provide physiological benefits over continuous diets for weight loss? A systematic review of clinical trials. Mol Cell Endocrinol. 2015;418(Pt 2):153–72. doi: 10.1016/j.mce.2015.09.014. https://www.ncbi.nlm.nih.gov/pubmed/26384657
- Aragon AA, Schoenfeld BJ, Wildman R, et al. International society of sports nutrition position stand: diets and body composition. Journal of the International Society of Sports Nutrition. 2017;14:16. doi:10.1186/s12970-017-0174-y. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5470183
- Komi PV, Kaneko M, Aura O. EMG activity of leg extensor muscles with special reference to mechanical efficiency in concentric and eccentric exercise. Int J Sports Med. 1987;8(Suppl):22-9. https://www.ncbi.nlm.nih.gov/pubmed/3583516
- Bonde-Peterson F, Knuttgen HG, Henriksson J. Muscle metabolism during exercise with concentric and eccentric contractions. J Appl Physiol. 1972;33:792-5. https://www.ncbi.nlm.nih.gov/pubmed/4643859
- Hather BM, Tesch PA, Buchanan P, Dudley GA. Influence of eccentric actions on skeletal muscle adaptations to resistance training. Acta Physiol Scand. 1991;143:177-85. https://www.ncbi.nlm.nih.gov/pubmed/1835816
- Ebbeling CB, Clarkson PM. Exercise-induced muscle damage and adaptation. Sports Med. 1989;7:207-34. https://www.ncbi.nlm.nih.gov/pubmed/2657962
- Dudley GA, Tesch PA, Miller BJ, Buchanan MD. Importance of eccentric actions in performance adaptations to resistance training. Aviat Space Environ Med. 1991;62:543-50. https://www.ncbi.nlm.nih.gov/pubmed/1859341
- Farthing JP, Chilibeck PD. The effects of eccentric and concentric training at different velocities on muscle hypertrophy. Eur J Appl Physiol. 2003;89:578-86.
- Jackson A, Jackson T, Hnatek J, West J. Strength development: using functional isometrics in an isotonic strength training program. Res Q Exerc Sport. 1985;56:234-7.
- McGill SM. Low back stability: from formal description to issues for performance and rehabilitation. Exerc Sports Sci Rev. 2001;29:26-31. https://www.ncbi.nlm.nih.gov/pubmed/11210443
- Munn J, Herbert RD, Hancock MJ, Gandevia SC. Resistance training for strength: effect of number of sets and contraction speed. Med Sci Sports Exerc. 2005;37:1622-6. www.ncbi.nlm.nih.gov/pubmed/16177617
- Shepstone TN, Tang JE, Dallaire S, et al. Short-term high- vs. low-velocity isokinetic lengthening training results in greater hypertrophy of the elbow flexors in young men. J Appl Physiol. 2005;98:1768-76.
- Hunter GR, Seelhorst D, Snyder S. Comparison of metabolic and heart rate responses to super slow vs. traditional resistance training. J Strength Cond Res. 2003;17:76-81. www.ncbi.nlm.nih.gov/pubmed/12580660
- Farthing JP, Chilibeck PD. The effects of eccentric and concentric training at different velocities on muscle hypertrophy. Eur J Appl Physiol. 2003;89:578-86.
- Munn J, Herbert RD, Hancock MJ, Gandevia SC. Resistance training for strength: effect of number of sets and contraction speed. Med Sci Sports Exerc. 2005;37:1622-6. https://www.ncbi.nlm.nih.gov/pubmed/16177617
- Cronin J, McNair PJ, Marshall RN. The effects of bungy weight training on muscle function and functional performance. J Sports Sci. 2003;21:59-71. www.ncbi.nlm.nih.gov/pubmed/12587892
- Kraemer WJ, RatamessNA. Fundamentals of resistance training: progression and exercise prescription. Med Sci Sport Exerc. 2004;36:674-8. https://www.ncbi.nlm.nih.gov/pubmed/15064596
- Chilibeck PD, Calder AW, Sale DG, Webber CE. A comparison of strength and muscle mass increases during resistance training in young women. Eur J Appl Physiol. 1998;77:170-5. https://www.ncbi.nlm.nih.gov/pubmed/9459538
- Stone MH, Plisk SS, Stone ME, et al. Athletic performance development: volume load-1 set vs. multiple sets, training velocity and training variation. NSCA J. 1998;20:22-31.
- McCurdy KW, Langford GA, Doscher MW, Wiley LP, Mallard KG. The effects of short-term unilateral and bilateral lower-body resistance training on measures of strength and power. J Strength Cond Res. 2005;19:9-15. www.ncbi.nlm.nih.gov/pubmed/15705051
- Kibler WB, Press J, Sciascia A. The role of core stability in athletic function. Sports Med. 2006;36:189-98. https://www.ncbi.nlm.nih.gov/pubmed/16526831
- Anderson K, Behm DG. Trunk muscle activity increases with unstable squat movements. Can J Appl Physiol. 2005;30:33-45. https://www.ncbi.nlm.nih.gov/pubmed/15855681
- The American College of Sports Medicine. Resistance Training for Health and Fitness. https://www.acsm.org/docs/brochures/resistance-training.pdf
- Mayo Foundation for Medical Education and Research. Sprint, rest, repeat: Exploring the benefits of high-intensity interval training. http://www.mayoclinic.org/medical-professionals/clinical-updates/physical-medicine-rehabilitation/sprint-rest-repeat-exploring-the-benefits-of-high-intensity-interval-training
- Gibala MJ, Little JP, Essen MV, et al.. Short-term sprint interval versus traditional endurance training: similar initial adaptations in human skeletal muscle and exercise performance. J Physiol. 2006; 575 (3): 901–11.
- Murphy E, Schwarzkopf R. Effects of standard set and circuit weight training on excess post-exercise oxygen consumption. J Strength Cond Res. 1992;6(2):66–124.
- Trapp EG, Chisholm DJ, Fruend J, Bouthcher SH. The effects of high-intensity intermittent exercise training on fat loss and fasting insulin levels of young women. Int J Obes. 2008;32(4):684–91.
- Wernbom M, Augustsson J, Thomee R. The influence of frequency, intensity, volume and mode of strength training on whole muscle cross-sectional area in humans. Sports Med. 2007;37(3):225–64. https://www.ncbi.nlm.nih.gov/pubmed/17326698
- Scott CB, Leighton BH, Ahearn KJ, McManus JJ. Aerobic, anaerobic, and excess postexercise oxygen consumption energy expenditure of muscular endurance and strength: 1-set of bench press to muscular fatigue. J Strength Cond Res. 2011;25(4):903–8. https://www.ncbi.nlm.nih.gov/pubmed/20703175
- Elliot DL, Goldberg L, Kuehl KS. Effects of resistance training on excess post-exercise O2 consumption. J Appl Sports Sci Res. 1992; 6: 77–81.
- Haltom R, Kraemer RR, Sloan RA, Frank K, Tryniecki JL. Circuit weight training and its effects on excess postexercise oxygen consumption. Med Sci Sports Exerc. 1999; 31: 1202–7.
- Heden L, Lox C, Rose P, Reid S, Kirk EP. One set resistance training elevates energy expenditure for 72 hours similar to three sets. Eur J Appl Physiol. 2011; 111 (3): 477–84.
- Moller N, Schmitz O, Porksen N, Moller J, Jorgenson JO. Dose-response studies on the metabolic effects of a growth hormone pulse in humans. Metabolism. 1992;41(2):172–5. https://www.ncbi.nlm.nih.gov/pubmed/1736039
- J Transl Med. 2012; 10: 237. High-Intensity Interval Resistance Training (HIRT) influences resting energy expenditure and respiratory ratio in non-dieting individuals. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3551736/
- McCaw ST, Friday JJ. A comparison of muscle activity between a free weight and machine bench press. J Strength Cond Res. 1994;8:259-64.
- Boyer BT. A comparison of the effects of three strength training programs on women. J Appl Sports Sci Res. 1990;4:88-94.
- Willoughby DSGillespie JW. A comparison of isotonic free weights and omnikinetic exercise machines on strength. J Human Mov Stud. 1990;19:93-100.
- Sforzo GA, Touey PR. Manipulating exercise order affects muscular performance during a resistance exercise training session. J Strength Cond Res. 1996;10:20-4.
- Baker D, Newton RU. Acute effect on power output of alternating an agonist and antagonist muscle exercise during complex training. J Strength Cond Res. 2005;19:202-5. www.ncbi.nlm.nih.gov/pubmed/15705035
- Maynard J, Ebben WP. The effects of antagonist prefatigue on agonist torque and electromyography. J Strength Cond Res. 2003;17:469-74.
- Simao R, Farinatti PTV, Polito MD, Viveiros L, Fleck SJ. Influence of exercise order on the number of repetitions performed and perceived exertion during resistance exercise in women. J Strength Cond Res. 2007;21:23-8. www.ncbi.nlm.nih.gov/pubmed/17313265
- Spreuwenberg LP, Kraemer WJ, Spiering BA, et al. Influence of exercise order in a resistance-training exercise session. J Strength Cond Res. 2006;20:141-4. www.ncbi.nlm.nih.gov/pubmed/16503673
- Simao R, Farinatti PTV, Polito MD, Maior AS, Fleck SJ. Influence of exercise order on the number of repetitions performed and perceived exertion during resistive exercises. J Strength Cond Res. 2005;19:152-6. www.ncbi.nlm.nih.gov/pubmed/15705026
- Kraemer WJ. A series of studies-the physiological basis for strength training in American football: fact over philosophy. J Strength Cond Res. 1997;11:131-42.
- Behm DG, Reardon G, Fitzgerald J, Drinkwater E. The effect of 5, 10, and 20 repetition maximums on the recovery of voluntary and evoked contractile properties. J Strength Cond Res. 2002; 16:209-18. www.ncbi.nlm.nih.gov/pubmed/11991772
- Ratamess NA, Falvo MJ, Mangine GT, et al. The effect of rest interval length on metabolic responses to the bench press exercise. Eur J Appl Physiol. 2007;100:1-17. www.ncbi.nlm.nih.gov/pubmed/17237951
- Harber MP, Fry AC, Rubin MR, Smith JC, Weiss LW. Skeletal muscle and hormonal adaptations to circuit weight training in untrained men. Scand J Med Sci Sports. 2004;14:176-85. www.ncbi.nlm.nih.gov/pubmed/15144358
- Pincivero DM, Lephart SM, Karunakara RG. Effects of rest interval on isokinetic strength and functional performance after short term high intensity training. Br J Sports Med. 1997;31:229-34. www.ncbi.nlm.nih.gov/pubmed/9298559
- Robinson JM, Stone MH, Johnson RL, et al. Effects of different weight training exercise/rest intervals on strength, power, and high intensity exercise endurance. J Strength Cond Res. 1995;9:216-21.
- Weiss LW, Coney HD, Clark FC. Differential functional adaptations to short-term low- moderate-, and high-repetition weight training. J Strength Cond Res. 1999;13:236-41.
- Rhea MR, Phillips WT, Burkett LN, et al. A comparison of linear and daily undulating periodized programs with equated volume and intensity for local muscular endurance. J Strength Cond Res. 2003;17:82-7. https://www.ncbi.nlm.nih.gov/pubmed/12580661
- Häkkinen K, Alen M, Komi PV. Changes in isometric force-and relaxation-time, electromyographic and muscle fibre characteristics of human skeletal muscle during strength training and detraining. Acta Physiol Scand. 1985;125:573-85. https://www.ncbi.nlm.nih.gov/pubmed/4091001
- O’Shea P. Effects of selected weight training programs on the development of strength and muscle hypertrophy. Res Q. 1966;37:95-102.
- Campos GE, Luecke TJ, Wendeln HK, et al. Muscular adaptations in response to three different resistance-training regimens: specificity of repetition maximum training zones. Eur J Appl Physiol. 2002;88:50-60.
- Fleck SJ. Periodized strength training: a critical review. J Strength Cond Res. 1999;13:82-9.
- Rhea MR, Alvar BA, Burkett LN, Ball SD. A meta-analysis to determine the dose response for strength development. Med Sci Sports Exerc. 2003;35:456-64. https://www.ncbi.nlm.nih.gov/pubmed/12618576
- Peterson MD, Rhea MR, Alvar BA. Maximizing strength development in athletes: a meta-analysis to determine the dose-response relationship. J Strength Cond Res. 2004;18:377-82. https://www.ncbi.nlm.nih.gov/pubmed/15142003
- Ratamess NA, Faigenbaum AD, Hoffman JR, Kang J. Self-selected resistance training intensity in healthy women: the influence of a personal trainer. J Strength Cond Res. 2008;22:103-11.
- Tran QT, Docherty D, Behm D. The effects of varying time under tension and volume load on acute neuromuscular responses. Eur J Appl Physiol. 2006;98:402-10. https://www.ncbi.nlm.nih.gov/pubmed/16969639
- Dudley GA, Djamil R. Incompatibility of endurance- and strength-training modes of exercise. J Appl Physiol. 1985;59:1446-51. https://www.ncbi.nlm.nih.gov/pubmed/4066574
- Mayhew JL, Gross PM. Body composition changes in young women with high resistance training. Res Q. 1974;45:433-40.
- Staron RS, Karapondo DL, Kraemer WJ, et al. Skeletal muscle adaptations during early phase of heavy-resistance training in men and women. J Appl Physiol. 1994;76:1247-55.
- Hortobagyi T, Barrier J, Beard D, et al. Greater initial adaptations to submaximal muscle lengthening than maximal shortening. J Appl Physiol. 1996;81:1677-82. https://www.ncbi.nlm.nih.gov/pubmed/8904586
- Housh DJ, Housh TJ, Johnson GO, Chu WK. Hypertrophic response to unilateral concentric isokinetic resistance training. J Appl Physiol. 1992;73:65-70. https://www.ncbi.nlm.nih.gov/pubmed/1506400
- Sale DG, Jacobs I, MacDougall JD, Garner S. Comparisons of two regimens of concurrent strength and endurance training. Med Sci Sports Exerc. 1990;22:348-56.
- Capen EK. Study of four programs of heavy resistance exercises for development of muscular strength. Res Q. 1956;27:132-42.
- Ostrowski KJ, Wilson GJ, Weatherby R, Murphy PW, Lyttle AD. The effect of weight training volume on hormonal output and muscular size and function. J Strength Cond Res. 1997;11:148-54.
- Berger RA. Effect of varied weight training programs on strength. Res Q. 1962;33:168-81.
- Peterson MD, Rhea MR, Alvar BA. Maximizing strength development in athletes: a meta-analysis to determine the dose-response relationship. J Strength Cond Res. 2004;18:377-82. www.ncbi.nlm.nih.gov/pubmed/15142003
- Peterson MD, Rhea MR, Alvar BA. Applications of the dose-response for muscular strength development: a review of meta-analytic efficacy and reliability for designing training prescription. J Strength Cond Res. 2005;19:950-8. https://www.ncbi.nlm.nih.gov/pubmed/16287373
- Coleman AE. Nautilus vs universal gym strength training in adult males. Am Correct Ther J. 1977;31:103-7. https://www.ncbi.nlm.nih.gov/pubmed/899994
- Jacobson BH. A comparison of two progressive weight training techniques on knee extensor strength. J Athl Train. 1986;21:315-9.
- Sanborn K, Boros R, Hruby J, et al. Short-term performance effects of weight training with multiple sets not to failure vs a single set to failure in women. J Strength Cond Res. 2000;14:328-31.
- Takeshima N, Rogers M, Watanabe E, et al. Water-based exercise improves health-related aspects of fitness in older women. Med Sci Sports Exerc. 2002;33:544-51. Takeshima N, Rogers M, Watanabe E, et al. Water-based exercise improves health-related aspects of fitness in older women. Med Sci Sports Exerc. 2002;33:544-51.
- Feigenbaum MS, Pollock ML. Prescription of resistance training for health and disease. Med Sci Sports Exerc. 1999;31:38-45. https://www.ncbi.nlm.nih.gov/pubmed/9927008
- Kemmler WK, Lauber D, Engelke K, Weineck J. Effects of single- vs. multiple-set resistance training on maximum strength and body composition in trained postmenopausal women. J Strength Cond Res. 2004;18:689-94. https://www.ncbi.nlm.nih.gov/pubmed/15574068
- Kraemer WJ, Ratamess N, Fry AC, et al. Influence of resistance training volume and periodization on physiological and performance adaptations in college women tennis players. Am J Sports Med. 2000;28:626-33. https://www.ncbi.nlm.nih.gov/pubmed/11032216
- Hass CJ, Garzarella L, Dehoyos D, Pollock ML. Single versus multiple sets and long-term recreational weightlifters. Med Sci Sports Exerc. 2000;32:235-42. https://www.ncbi.nlm.nih.gov/pubmed/10647555
- Rhea MR, Alvar BA, Burkett LN. Single versus multiple sets for strength: a meta-analysis to address the controversy. Res Q Sport Exerc. 2002;73:485-8.
- Wolfe BL, Lemura LM, Cole PJ. Quantitative analysis of single- vs. multiple-set programs in resistance training. J Strength Cond Res. 2004;18:35-47. https://www.ncbi.nlm.nih.gov/pubmed/14971985
- Gonzalez-Badillo JJ, Gorostiaga EM, Arellano R, Izquierdo M. Moderate resistance training volume produces more favorable strength gains than high or low volumes during a short-term training cycle. J Strength Cond Res. 2005;19:689-97.
- Finer JT, Simmons RM, Spudich JA. Single myosin molecule mechanics: piconewton forces and nanometre steps. Nature. 1994;368:113-9. https://www.ncbi.nlm.nih.gov/pubmed/8139653
- Knapik JJ, Mawdsley RH, Ramos MU. Angular specificity and test mode specificity of isometric and isokinetic strength training. J Orthop Sports Phys Ther. 1983;5:58-65. https://www.ncbi.nlm.nih.gov/pubmed/18806429
- Henneman E, Somjen G, Carpenter D. Functional significance of cell size in spinal motoneurons. J Neurophysiol. 1965; 28:560-80. https://www.ncbi.nlm.nih.gov/pubmed/14328454
- Coburn JW, Housh TJ, Malek MH, et al. Neuromuscular responses to three days of velocity-specific isokinetic training. J Strength Cond Res. 2006;20:892-8.
- Candow DG, Burke DG. Effect of short-term equal-volume resistance training with different workout frequency on muscle mass and strength in untrained men and women. J Strength Cond Res. 2007;21:204-7. https://www.ncbi.nlm.nih.gov/pubmed/17313289
- Graves JE, Pollock ML, Leggett SH, et al. Effect of reduced training frequency on muscular strength. Int J Sports Med. 1988;9:316-9. https://www.ncbi.nlm.nih.gov/pubmed/3246465
- McLester JR, Bishop P, Guilliams ME. Comparison of 1 day and 3 days per week of equal-volume resistance training in experienced subjects. J Strength Cond Res. 2000;14:273-81.
- Graves JE, Pollock ML, Jones AE, Colvin AB, Leggett SH. Specificity of limited range of motion variable resistance training. Med Sci Sports Exerc. 1989;21:84-9. www.ncbi.nlm.nih.gov/pubmed/2927306
- Hunter GR. Changes in body composition, body build, and performance associated with different weight training frequencies in males and females. NSCA J. 1985;7:26-8.
- Pollock ML, Graves JE, Bamman MM, et al. Frequency and volume of resistance training: effect of cervical extension strength. Arch Phys Med Rehabil. 1993;74:1080-6. www.ncbi.nlm.nih.gov/pubmed/8215860
- Gillam GM. Effects of frequency of weight training on muscle strength enhancement. J Sports Med. 1981;21:432-6.
- Hoffman JR, Kraemer WJ, Fry AC, Deschenes M, Kemp DM. The effect of self-selection for frequency of training in a winter conditioning program for football. J Appl Sport Sci Res. 1990;3:76-82.
- Häkkinen K, Pakarinen A, Alen M, Kauhanen H, Komi PV. Neuromuscular and hormonal responses in elite athletes to two successive strength training sessions in one day. Eur J Appl Physiol. 1988;57:133-9. www.ncbi.nlm.nih.gov/pubmed/3349977
- Zatsiorsky V, Kraemer WJ. Science and Practice of Strength Training. 2nd ed. Champaign (IL): Human Kinetics; 2006.
- Häkkinen K, Kallinen M. Distribution of strength training volume into one or two daily sessions and neuromuscular adaptations in female athletes. Electromyogr Clin Neurophysiol. 1994;34:117-24. www.ncbi.nlm.nih.gov/pubmed/8187678
- Fleck SJ, Kraemer WJ. Designing Resistance Training Programs. 2nd ed. Champaign (IL): Human Kinetics Books; 1997. p. 1-115.
- Rhea MR, Alvar BA, Burkett LN, Ball SD. A meta-analysis to determine the dose response for strength development. Med Sci Sports Exerc. 2003;35:456-64. www.ncbi.nlm.nih.gov/pubmed/12618576
- American College of Sports Medicine. Progression models in resistance training for healthy adults. Med Sci Sports Exerc. 2002;34:364-80.
- Medicine & Science in Sports & Exercise. 41(3):687-708, March 2009.
- Fleck SJ. Cardiovascular adaptations to resistance training. Med Sci Sports Exerc. 1988;20:S146-51. https://www.ncbi.nlm.nih.gov/pubmed/3057314
- Hurley BF, Kokkinos PF. Effects of weight training on risk factors for coronary heart disease. Sports Med. 1987;4:231-8. https://www.ncbi.nlm.nih.gov/pubmed/3306865
- Miller WJ, Sherman WM, Ivy JL. Effect of strength training on glucose tolerance and post-glucose insulin response. Med Sci Sports Exerc. 1984;16:539-43. https://www.ncbi.nlm.nih.gov/pubmed/6392812
- Layne JE, Nelson ME. The effect of progressive resistance training on bone density: a review. Med Sci Sports Exerc. 1999;31:25-30. https://www.ncbi.nlm.nih.gov/pubmed/9927006
- Koffler KH, Menkes A, Redmond RA, et al. Strength training accelerates gastrointestinal transit in middle-aged and older men. Med Sci Sports Exerc. 1992;24:415-9. https://www.ncbi.nlm.nih.gov/pubmed/1560736
- Evans WJ. Exercise training guidelines for the elderly. Med Sci Sports Exerc. 1999;31:12-7. https://www.ncbi.nlm.nih.gov/pubmed/9927004
- Ewart CK. Psychological effects of resistive weight training: implications for cardiac patients. Med Sci Sports Exerc. 1989;21:683-8.
- Thein-Nissenbaum JM, Rauh MJ, Carr KE, Loud KJ, McGuine TA: Associations between disordered eating, menstrual dysfunction, and musculoskeletal injury among high school athletes. J Orthop Sports Phys Ther 2011;41(2):60-69.
- Rauh MJ, Nichols JF, Barrack MT: Relationships among injury and disordered eating, menstrual dysfunction, and low bone mineral density in high school athletes: A prospective study. J Athl Train 2010;45(3):243-252.
- American College of Sports Medicine. The Female Athlete Triad. https://www.acsm.org/docs/brochures/the-female-athlete-triad.pdf
- Hoch AZ, Pajewski NM, Moraski L, et al: Prevalence of the female athlete triad in high school athletes and sedentary students. Clin J Sport Med 2009;19(5):421-428.
- Amino Acids. 2013 Aug;45(2):231-40. doi: 10.1007/s00726-013-1506-0. Epub 2013 May 5. Role of protein and amino acids in promoting lean mass accretion with resistance exercise and attenuating lean mass loss during energy deficit in humans. https://www.ncbi.nlm.nih.gov/pubmed/23645387
- Dietary protein for athletes: from requirements to optimum adaptation. Phillips SM, Van Loon LJ. J Sports Sci. 2011; 29 Suppl 1():S29-38. https://www.ncbi.nlm.nih.gov/pubmed/22150425/
- Contemporary issues in protein requirements and consumption for resistance trained athletes. Wilson J, Wilson GJ. J Int Soc Sports Nutr. 2006 Jun 5; 3():7-27. https://www.ncbi.nlm.nih.gov/pubmed/18500966/
- Comparison of body composition, exercise and nutritional profiles of female and male body builders at competition. Sandoval WM, Heyward VH, Lyons TM. J Sports Med Phys Fitness. 1989 Mar; 29(1):63-70. https://www.ncbi.nlm.nih.gov/pubmed/2770270/
- A systematic review of dietary protein during caloric restriction in resistance trained lean athletes: a case for higher intakes. Helms ER, Zinn C, Rowlands DS, Brown SR. Int J Sport Nutr Exerc Metab. 2014 Apr; 24(2):127-38. https://www.ncbi.nlm.nih.gov/pubmed/24092765/
- Muscle substrate utilization and lactate production. MacDougall JD, Ray S, Sale DG, McCartney N, Lee P, Garner S. Can J Appl Physiol. 1999 Jun; 24(3):209-15. https://www.ncbi.nlm.nih.gov/pubmed/10364416/
- Nutrition guidelines for strength sports: sprinting, weightlifting, throwing events, and bodybuilding. Slater G, Phillips SM. J Sports Sci. 2011; 29 Suppl 1():S67-77. https://www.ncbi.nlm.nih.gov/pubmed/21660839/
- A reduced ratio of dietary carbohydrate to protein improves body composition and blood lipid profiles during weight loss in adult women. Layman DK, Boileau RA, Erickson DJ, Painter JE, Shiue H, Sather C, Christou DD. J Nutr. 2003 Feb; 133(2):411-7. https://www.ncbi.nlm.nih.gov/pubmed/12566476/
- Energy expenditure, satiety, and plasma ghrelin, glucagon-like peptide 1, and peptide tyrosine-tyrosine concentrations following a single high-protein lunch. Smeets AJ, Soenen S, Luscombe-Marsh ND, Ueland Ø, Westerterp-Plantenga MS. J Nutr. 2008 Apr; 138(4):698-702. https://www.ncbi.nlm.nih.gov/pubmed/18356323/
- Low-carbohydrate diets and performance. Cook CM, Haub MD. Curr Sports Med Rep. 2007 Jul; 6(4):225-9. https://www.ncbi.nlm.nih.gov/pubmed/17617997/
- Anabolic and catabolic hormones and energy balance of the male bodybuilders during the preparation for the competition. Mäestu J, Eliakim A, Jürimäe J, Valter I, Jürimäe T. J Strength Cond Res. 2010 Apr; 24(4):1074-81. https://www.ncbi.nlm.nih.gov/pubmed/20300017/
- Pituitary–gonadal axis during prolonged total starvation in obese men. Suryanarayana BV, Kent JR, Meister L, Parlow AF. Am J Clin Nutr. 1969 Jun; 22(6):767-70. https://www.ncbi.nlm.nih.gov/pubmed/5789477/
- Moderate energy restriction with high protein diet results in healthier outcome in women. Mero AA, Huovinen H, Matintupa O, Hulmi JJ, Puurtinen R, Hohtari H, Karila TA. J Int Soc Sports Nutr. 2010 Jan 25; 7(1):4. https://www.ncbi.nlm.nih.gov/pubmed/20205751/
- Decrease of serum total and free testosterone during a low-fat high-fibre diet. Hämäläinen EK, Adlercreutz H, Puska P, Pietinen P. J Steroid Biochem. 1983 Mar; 18(3):369-70. https://www.ncbi.nlm.nih.gov/pubmed/6298507/
- Diet and serum sex hormones in healthy men. Hämäläinen E, Adlercreutz H, Puska P, Pietinen P. J Steroid Biochem. 1984 Jan; 20(1):459-64. https://www.ncbi.nlm.nih.gov/pubmed/6538617/
- Bird SP. Strength nutrition: maximizing your anabolic potential. Strength Cond J. 2010;32:80–86. doi: 10.1519/SSC.0b013e3181d5284e.
- Macronutrient content of a hypoenergy diet affects nitrogen retention and muscle function in weight lifters. Walberg JL, Leidy MK, Sturgill DJ, Hinkle DE, Ritchey SJ, Sebolt DR. Int J Sports Med. 1988 Aug; 9(4):261-6. https://www.ncbi.nlm.nih.gov/pubmed/3182156/
- Macronutrient considerations for the sport of bodybuilding. Lambert CP, Frank LL, Evans WJ. Sports Med. 2004; 34(5):317-27. https://www.ncbi.nlm.nih.gov/pubmed/15107010/
- A perspective on fat intake in athletes. Pendergast DR, Leddy JJ, Venkatraman JT. J Am Coll Nutr. 2000 Jun; 19(3):345-50. https://www.ncbi.nlm.nih.gov/pubmed/10872896/
- International Society of Sports Nutrition position stand: nutrient timing. Kerksick C, Harvey T, Stout J, Campbell B, Wilborn C, Kreider R, Kalman D, Ziegenfuss T, Lopez H, Landis J, Ivy JL, Antonio J. J Int Soc Sports Nutr. 2008 Oct 3; 5():17. https://www.ncbi.nlm.nih.gov/pubmed/18834505/
- Aragon AA, Schoenfeld BJ. Nutrient timing revisited: is there a post-exercise anabolic window? J Int Soc Sports Nutr. 2013;10:5. doi: 10.1186/1550-2783-10-5. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3577439/





{kind=link}