Coffin Lowry syndrome
Coffin-Lowry syndrome also called mental retardation with osteocartilaginous abnormalities, is a rare genetic disorder that affects many parts of the body. The signs and symptoms are usually more severe in males than in females, although the features of Coffin-Lowry syndrome range from very mild to severe in affected women.
Males with Coffin-Lowry syndrome typically have severe to profound intellectual disability and delayed development. Affected women may be cognitively normal, or they may have intellectual disability ranging from mild to profound. Beginning in childhood or adolescence, some people with Coffin-Lowry syndrome experience brief episodes of collapse when excited or startled by a loud noise. These attacks are called stimulus-induced drop episodes.
Most affected males and some affected females have distinctive facial features including a prominent forehead, widely spaced and downward-slanting eyes, a short nose with a wide tip, and a wide mouth with full lips. Characteristic facial features may include an underdeveloped upper jawbone (maxillary hypoplasia), an abnormally prominent brow, downslanting eyelid folds (palpebral fissures), widely spaced eyes (hypertelorism), large ears, and/or unusually thick eyebrows. These features become more pronounced with age. Soft hands with short, tapered fingers are also characteristic of Coffin-Lowry syndrome. Additional features of Coffin-Lowry syndrome include short stature, an unusually small head (microcephaly), progressive abnormal front-to-back and side-to-side curvature of the spine (kyphoscoliosis), unusual prominence of the breastbone (sternum) (pectus carinatum) and other skeletal abnormalities.
Coffin-Lowry syndrome is caused by changes (mutations) in the RPS6KA3 gene and is inherited in an X-linked dominant pattern. Males are usually more severely affected than females. The incidence of Coffin Lowry syndrome is uncertain, but researchers estimate that the disorder affects 1 in 40,000 to 50,000 people 1.
Coffin-Lowry syndrome treatment is symptomatic. Genetic counseling is recommended for families.
Figure 1. Coffin Lowry syndrome

Footnote: (a–d) Facial views of a boy with Coffin Lowry syndrome at different ages showing evolution during infancy of facial gestalt. (a) At 9 months, (b) at 18 months, (c) at 3 years, and (d) at 6 years. Note the large forehead, hypertelorism, downslanting palpebral fissures, long philtrum, anteverted nares, and thick lips. This boy carries an RPS6KA3 intragenic duplication previously reported. (e–g) Views of the hands of the same patient. Note the typical broad tapering fingers (e) at 9 months, (f) at 18 months, and (g) at 5 years.
[Source 2 ]Are there any foods or supplements that have been shown to benefit people with Coffin-Lowry syndrome?
Limited information about the effects of diet on Coffin Lowry syndrome is available. ATF4 mediation of NF1 functions in osteoblast reveals a nutritional basis for congenital skeletal dysplasia, that discusses how a high-protein diet prevented and reversed the skeletal findings associated with Coffin Lowry syndrome in mice 3. In this study 3, the diet was provided from the first day of gestation to 28 days of age and resulted in a greater number of mice surviving past one month of life. When these mice returned to a normal diet after one month of age, they began to show symptoms of Coffin Lowry syndrome which suggested to authors that the diet may also be effective after birth, if continued. Although the mouse studies are encouraging, the impact of a high-protein diet in humans with Coffin Lowry syndrome has not yet been researched.
Is Coffin Lowry syndrome progressive?
Some aspects of the syndrome are progressive. Facial coarsening and skeletal involvement become more pronounced with age. Some motor and coordination neurological problems do not express themselves until later in childhood and may result in decreased mobility. Bone degeneration may occur starting in the late teen years which can lead to a higher incidence of broken bones. This is especially problematic for those who also have drop episodes as they are prone to spine and neck injuries from the repeated falls. Depression or behavior problems may develop. Life expectancy may be reduced in individuals who have severe cardiac problems, respiratory complications, or severe progressive kyphoscoliosis.
What developmental milestones are normal for Coffin Lowry syndrome?
Note: The following information is anecdotal, based on data gathered from letters written by family members of individuals affected by Coffin-Lowry syndrome 4.
Walking
Usually somewhere around 2-3 years. Many children have a more or less normal gait with mild coordination and balance issues. In some cases, walking may appear normal if unsteady for the first few years, and then somewhere between ages 4-7, the child’s gait may slowly change to a more wide-stanced gait, knees somewhat bent. Sometimes the left leg will drag behind the right. Often this so-called “ataxic” gait is associated with drop episodes, and the two characteristics will emerge about the same time. Both are most likely neurological in origin.
Speech
Speech is always impaired to some degree. Some acquire substantial oral communication, whereas a minority, especially in those with hearing impairment, never speak. A few basic sounds emerge between birth and 4 years, then between 4-6 years, 2-3 word short sentences usually emerge. Speech will continue to evolve and grow slowly over many years. Most can generally be understood even by strangers. Despite the limited verbal abilities, the communications skills are good. They usually understand (receptive language) much better than they can speak (expressive language) so their understanding is often underestimated.
Toilet training
Most children with intellectual disabilities can be toilet trained by age 7, including Coffin-Lowry children. Watch for the normal signs of readiness: awareness that they have soiled, and a desire to be changed. As with all other things, toilet training will take longer with Coffin Lowry syndrome children. Children need to be able to follow at least 5 actions in sequence to be toilet trained, so they may need assistance for some years. Some are never toilet trained. Watch for constipation, which is very common due to low muscle tone and inactivity and can lead to painful and dangerous bowel blockages.
Self-care
Many will eventually learn to handle their own personal hygiene and dress themselves, but some may always have trouble with fasteners such as buttons or tying the laces of their shoes. Pull-on pants, pull-over tops, and shoes with Velcro closures are wonderful for this and help give them a sense of independence and accomplishment.
Reading/Writing/Math
This varies a great deal by individual; writing is dependant on their fine motor control. Many will learn a few simple words – their name, the names of their family members, etc. Some do not learn to read or write at all. They tend to have very good memories.
Social/Emotional
Developmentally, this is the area least affected. Most Coffin-Lowry individuals are capable of a full range of emotions, and tend to be very friendly, cheerful and loving. A minority exhibit behavior issues.
Coffin Lowry syndrome causes
Mutations in the RPS6KA3 gene cause Coffin-Lowry syndrome. This gene provides instructions for making a protein that is involved in signaling within cells. Researchers believe that this protein helps control the activity of other genes and plays an important role in the brain. The protein is involved in cell signaling pathways that are required for learning, the formation of long-term memories, and the survival of nerve cells. Gene mutations result in the production of little or no RPS6KA3 protein, but it is unclear how a lack of this protein causes the signs and symptoms of Coffin-Lowry syndrome.
Some people with the features of Coffin-Lowry syndrome do not have identified mutations in the RPS6KA3 gene. In these cases, the cause of the condition is unknown.
Coffin Lowry syndrome inheritance pattern
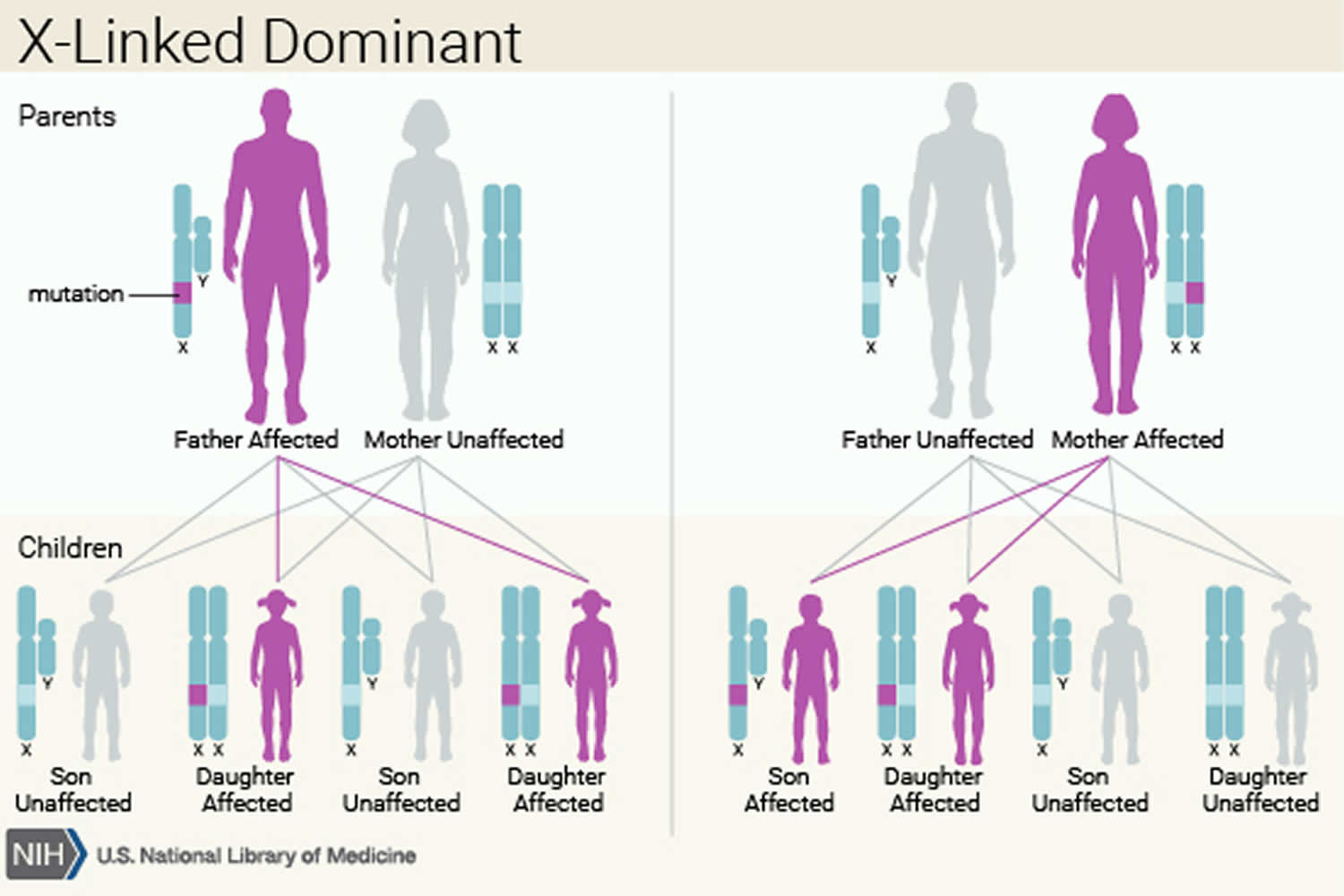
Coffin Lowry syndrome is inherited in an X-linked dominant pattern. A condition is considered X-linked if the mutated gene that causes the disorder is located on the X chromosome, one of the two sex chromosomes. The inheritance is dominant if one copy of the altered gene in each cell is sufficient to cause the condition. In most cases, males (who have one X chromosome in each cell) experience more severe signs and symptoms of the disorder than females (who have two X chromosomes in each cell). A characteristic of X-linked inheritance is that fathers cannot pass X-linked traits to their sons.
Between 70 percent and 80 percent of people with Coffin-Lowry syndrome have no history of the condition in their families. These cases are caused by new mutations in the RPS6KA3 gene. The remaining 20 percent to 30 percent of affected individuals have other family members with Coffin-Lowry syndrome.
Figure 2. Coffin Lowry syndrome X-linked dominant inheritance pattern
People with specific questions about genetic risks or genetic testing for themselves or family members should speak with a genetics professional.
Resources for locating a genetics professional in your community are available online:
- The National Society of Genetic Counselors (https://www.findageneticcounselor.com/) offers a searchable directory of genetic counselors in the United States and Canada. You can search by location, name, area of practice/specialization, and/or ZIP Code.
- The American Board of Genetic Counseling (https://www.abgc.net/about-genetic-counseling/find-a-certified-counselor/) provides a searchable directory of certified genetic counselors worldwide. You can search by practice area, name, organization, or location.
- The Canadian Association of Genetic Counselors (https://www.cagc-accg.ca/index.php?page=225) has a searchable directory of genetic counselors in Canada. You can search by name, distance from an address, province, or services.
- The American College of Medical Genetics and Genomics (http://www.acmg.net/ACMG/Genetic_Services_Directory_Search.aspx) has a searchable database of medical genetics clinic services in the United States.
Coffin Lowry syndrome symptoms
The symptoms of Coffin-Lowry syndrome tend to be more severe in males, although symptoms in affected females can range from none to the same severity seen in males. The characteristic facial features seen in affected males become more easily identifiable in late childhood and adulthood. The face is characterized by a prominent forehead and eyebrows, narrowing of both temples, scarce hair on the scalp, thickened eyebrow ridges, downslanting eyelid slits, wide-set eyes, thickened upper eyelids, a broad nasal bridge with a thick dividing cartilage (septum), thick prominent lips, an open mouth, prominent chin and ears.
Limb abnormalities may include large soft hands with double-jointed thick fingers that taper toward the tips, an unusual prominent transverse crease (hypothenar) and a shortened big toe. In males, the skin is loose and may stretch easily. Many bone abnormalities may also occur such as thickening of facial bones, shortening of the long bones, and pointed or sunken breast bone. Abnormal front-to-back and side-to-side curvature of the spine may also be present (kyphosis and scoliosis) and progresses with age. Affected individuals usually have short stature. A smaller than average head size (microcephaly) and dental abnormalities are common. Hearing loss is sometimes associated with Coffin-Lowry syndrome. In rare cases, vision loss may occur. Heart problems may be present and can be life threatening.
Affected males may have severe to profound intellectual disability. Intelligence in affected females ranges from normal to profound intellectual disability. Severely affected children may have no speech development.
Some affected individuals experience episodes of brief collapse without loss of consciousness (drop attacks) that occur following an unexpected noise or emotional event.
Coffin Lowry syndrome diagnosis
X-ray and neuroimaging studies may be helpful in confirming a diagnosis of Coffin-Lowry syndrome. Decreased ribosomal S6 kinase activity in cultured fibroblast or transformed lymphoblast cells from a male indicates Coffin-Lowry syndrome. Studies of enzyme activity cannot be used to diagnose an affected female.
Molecular genetic testing on a blood specimen or cells from a cheek swab is available to identify mutations in the RPS6KA3 gene. This testing can be used to confirm but not rule out the diagnosis of Coffin-Lowry syndrome because not all affected individuals have a detectable mutation.
Coffin Lowry syndrome treatment
No specific treatment for Coffin Lowry syndrome exist. Affected individuals should have regular cardiac, hearing and visual examinations. Proper management of patients with Coffin Lowry syndrome, includes surveillance by performing regular hearing, dental, and vision tests; annual heart examinations; and periodic monitoring for kyphoscoliosis which can be life threatening if the cardiorespiratory system becomes compromised. Medications such as valproate, clonzapam or selective serotonin uptake inhibitors might be prescribed for drop attacks. Surgery may be performed for skeletal deformities 5.
Genetic counseling is recommended for families.
Coffin Lowry syndrome prognosis
There is no “cure” for Coffin-Lowry Syndrome. However, specific symptoms, developmental delays and behaviors can be treated or addressed. A developmental evaluation should be done to determine if delays exist. Your physician can refer you to a center in your area serving developmentally disabled children, associations for intellectually disabled citizens, and in the special education departments of local school districts. If delays are noted, the child should be enrolled in an appropriate setting answering his specific needs. This often requires a “team approach” that includes physician, speech and language therapy, occupational therapy, physical therapy and vocational training. As with all children, early mental stimulation is important for brain development and especially so for children with Coffin Lowry syndrome.
Your child should have regular medical examinations to watch his or her progress. Since you see your child every day, you may notice that something is different before your family doctor will. In Coffin Lowry syndrome, scoliosis may be present as early as birth or as late as the teenage years, with the average being early grade school years. Unexplained falls may develop which are neurological in origin and may be controlled with various medications. Sleep apnea is common and if untreated, the chronic oxygen deprivation can cause cardiac problems and loss of cognitive function. Fainting spells could be an indicator of a heart condition. If behavior problems occur, first rule out any underlying physical cause; for example, head banging may be an indication that the child is in discomfort from chronic ear infections.
Ongoing management:
- Vision and hearing testing as appropriate
- Cardiac studies should be done during childhood
- Repeated every 5-10 years
- Monitor for the development of progressive kyphoscoliosis
- Intervention to prevent progression as appropriate
- The following should be suspicion for narrowing of spinal canal or spinal cord compression injury:
- Abnormal gait
- Bowel/bladder habits
- Expression of pain
- Neurological changes
- Abnormal tendon reflexes
- Awareness of “drop episodes”
- Allows early intervention to minimize occurrence of triggering stimuli
- Trial of antiepileptic medication may be indicated
- Significant social resources may be required to support women with Coffin Lowry syndrome.
- Coffin Lowry syndrome. https://ghr.nlm.nih.gov/condition/coffin-lowry-syndrome
- Marques Pereira, P., Schneider, A., Pannetier, S. et al. Coffin–Lowry syndrome. Eur J Hum Genet 18, 627–633 (2010). https://doi.org/10.1038/ejhg.2009.189
- Elefteriou F, Benson MD, Sowa H, et al. ATF4 mediation of NF1 functions in osteoblast reveals a nutritional basis for congenital skeletal dysplasiae. Cell Metab. 2006;4(6):441–451. doi:10.1016/j.cmet.2006.10.010 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2756713
- Coffin Lowry syndrome Frequently Asked Questions. http://www.clsf.info/faq/FAQ2.html
- Pereira PM, Schneider A, Pannetier S, Heron D, Hanauer A. Coffin-Lowry syndrome. European Journal of Human Genetics. 2009





{kind=link}