Corneal transplant surgery
A corneal transplant also known as keratoplasty, is a surgical procedure that replaces a disc-shaped segment of an unhealthy cornea with a similarly shaped piece of healthy donor cornea. A corneal transplant surgery is also called a corneal graft or keratoplasty. Only human donor tissue can be used in corneal transplantation surgery. A human donor is someone who chooses to donate (give) his or her corneas after their death to people who need them. All donated corneas are carefully tested to make sure they are healthy and safe to use.
Corneal transplant is the oldest and most common form of human transplantation (other than blood transfusion), with first successful full thickness corneal transplant performed in 1905 by Eduard Konrad Zirm 1. While full-thickness corneal transplant techniques have not changed much over the past century, lamellar corneal transplant techniques have evolved rapidly.
There are different types of corneal transplants. In some cases, only the front and middle layers of the cornea are replaced. In others, only the inner layer is removed. Sometimes, the entire cornea needs to be replaced.
Various anesthetic techniques are possible for a corneal transplant. A cornea transplant can be carried out under general anesthetic (where you’re unconscious) or local anesthetic (where the area is numbed and you’re awake).
Corneal transplant surgery usually takes 1 to 2 hours. In most cases, a corneal transplant procedure usually takes less than an hour and, depending on your circumstances, you either leave hospital the same day or stay overnight.
Your surgeon will remove the center part of your diseased cornea and replace it with a part of a cornea from a donor.
Your surgeon may replace all of your cornea, the outer layers or just the inner layer. If the corneal transplant surgery involves the transplantation of the outer cornea, the new outer cornea is held in place with stitches, which usually stay in for more than 12 months.
An endothelial transplant (EK) doesn’t require stitches. It’s held in place by an air bubble until a few days later, when it naturally sticks to the deep layer of the cornea.
You should be able to go home the same day or the day after your cornea transplant. Your healthcare team will give you eye drops and sometimes medication to take home.
Do not swim or lift anything heavy until you have checked with your surgeon.
Regular exercise should help you to return to normal activities as soon as possible. Before you start exercising, ask the healthcare team or your doctor for advice.
Most people make a good recovery. It may take up to 2 years for your vision to improve. You may need to have an operation to change the shape of the cornea.
Your healthcare team will arrange for you to come back to the clinic regularly so they can check that the transplant is healing well and for signs of rejection.
Conditions that require a corneal transplant
The two most common reasons for requiring a corneal transplant are:
- bullous keratopathy – a condition in which the cornea becomes permanently swollen
- Keratoconus – a corneal dystrophy where the cornea is coneshaped rather than dome-shaped
- Fuchs’ dystrophy, where cells in the inner layer of the cornea are not working effectively
Other reasons are:
- lattice, granular, macular and Fuch’s dystrophy
- eye injury
- herpes virus infection of the eye
- corneal scarring due to trauma
- hereditary or congenital corneal clouding
- severe bacterial infection.
Days or weeks before your corneal transplant
Your ophthalmologist will talk with you about corneal transplant surgery. You will discuss why you need this surgery, how it can help you see better, and what you can expect during and after surgery.
Once you decide to have a corneal transplant, a date will be chosen for surgery. That date may change if a good donor cornea is not ready for you at that time.
Tell your ophthalmologist about all the medicines you take. He or she will tell you if you can keep taking them before surgery.
You may need to stop using blood thinners before surgery. You may need to visit your primary care doctor for a physical exam and perhaps other tests. This is to make sure you are healthy enough to have the transplant surgery.
You will not be able to drive after the transplant surgery. You should make arrangements for someone to drive you home after surgery.
The day of your corneal transplant surgery
A corneal transplant is done as an outpatient procedure.
Here is what will happen just before and during corneal transplant surgery.
- Eye drops will be put in your eyes. You may be given other medicine to help you relax.
- Your eye surgeon will use either local or general anesthesia so you do not feel pain. He or she will then put a device on your eye to keep it open. Even though your eye is open, you will see very little or nothing at all because of the anesthesia.
- Your eye surgeon will have chosen how to transplant the healthy donor cornea based on your specific need.
- In some cases, he or she may remove a circular part of your cornea and replace it with a matching portion of the donor cornea, stitching it into place.
- Sometimes he or she will remove only a very thin layer of cells from the front of the cornea, replacing them with donor tissue and stitching it into place.
- In other cases, only the damaged inner layer of the cornea is removed and a thin disc of healthy donor tissue is placed on the back surface of the cornea. An air bubble is then put in the eye to push this new cell layer into place so the cornea can heal properly.
- Sometimes your ophthalmologist may repair other eye problems during the same surgery, such as cataracts.
- After surgery, your ophthalmologist usually tapes a shield over your eye to keep it safely covered. You will be monitored after surgery to make sure you recover from the anesthesia and can go home safely.
- Your ophthalmologist will explain what to do to care for yourself at home after surgery.
After your corneal transplant surgery
The day after your corneal transplant surgery, you will need to go back to your ophthalmologist’s office to have your eyes checked.
The stitches from surgery may or may not need to be removed. This depends on how quickly you heal, the health of your eye, and the type of stitches used.
As you recover from surgery, these are things you need to do to care for your eye:
- Use the eye drops exactly as the ophthalmologist prescribed.
- Do not press on or rub your eye.
- If needed, take over-the-counter pain medicine. Ask your doctor which ones you can take.
- Wear eyeglasses or an eye shield to protect your eyes.
- Talk with your ophthalmologist about when you can get back to doing your normal daily routine.
Call your ophthalmologist if you have concerns or questions about how to care for yourself at home.
Depending on the type of transplant you had and how your eye heals, it can take a year or more to fully recover from this surgery.
Cornea Donor Eligibility
Any cornea deemed suitable for transplantation can be grafted into any recipient, regardless of recipient age, race, and blood type 2. Eye banks, in concert with guidance from the Eye Bank Association of America and Food and Drug Administration (FDA), help set policies and procedures that guide suitability determinations for cornea transplantation and proper storage and handling of transplant tissue. There is a 24-hour window of opportunity from the time of a donor’s death to procure a cornea and place it in storage media. Unlike organ donation, in which procurement is extremely limited by time and the immediate availability of a potential recipient, corneoscleral tissue can be stored and used up to 14 days after procurement before it expires 2.
Willingness to become an organ, tissue, and eye donor is coordinated through the Donor Registry. Registration is a binding contract for potential donors. Donor registration at the Department of Motor Vehicles is connected to the Donor Registry, and is also a binding contract. Families of a deceased individual also impact the donation status of their loved ones. FDA requires that the next-of-kin participate in an extensive medical history questionnaire regarding the donor’s health. This is an opportunity to obtain important information about the donor’s life – travel history, infection history, sexual history, drug and alcohol abuse, and other information – in order to gain a better understanding of donor eligibility. If the family refuses to provide this information, donation is not pursued.
Contraindications in a donor’s past medical history that limit or prevent the donation of his or her corneas
Diseases Transmissable by Corneal Transplantation:
- Rabies
- Hepatitis B
- Creutzfeldt-Jakob disease
- Retinoblastoma
- Bacterial/Fungal keratitis
- Bacterial/Fungal endophthalmitis
Diseases Likely Transmissable by Corneal Transplantation:
- HIV
- Herpes Simplex Virus
- Prion disease
Other Diseases of Exclusion:
- Hepatitis C
- Human T-Cell Lymphotrophic Virus
- Ocular adenocarcinoma
- Malignant tumors of the anterior segment
- Reye syndrome
- Subacute sclerosing panencephalitis
- Progressive multifocal leukoencephalopathy
- Leukemias
- Active disseminated lymphomas
- Active infectious endocarditis
- Active septicemia
- Dementia of unknown cause
- Recipient of non-synthetic dura mater graft
- Down syndrome
- Congenital rubella
- High-risk behavior or incarceration in prison
- Prior refractive surgery (may not exclude from endothelial keratoplasty)
Cornea Procurement and Release for Surgery
Procuring donated organs, tissue, and eyes is a 24-hour-a-day commitment. Upon notification of eyes in need of procurement, a technician is sent to the procurement site – typically an operating room, hospital room, morgue, funeral home, or any other designated procurement site that meets the aseptic criteria for procuring tissue. The recovery technician identifies the donor and compares the registry information with the patient information on his or her medical chart. A post-mortem blood draw is performed for serological testing. The recovery technician also completes a full body examination, noting specifically any signs of disease, high-risk behavior, and identification marks. A penlight examination of the eyes is performed, noting findings such as epithelial exposure, scars, and arcus senilis. The procurement is performed using aseptic surgical technique. If the eyes donated are designated for transplantation, only the cornea is procured. If the eyes donated are designated for research purposes, the entire globe is procured. If requested, the sclera can also be procured and prepared for a scleral patch graft.
Death-to-procurement protocols are established by individual eye banks. eyes donated for transplantation must be placed in storage media within 24 hours of the time of death. Corneal storage is an important element of cornea transplantation that has increased the opportunity for successful corneal procurement and surgery. Corneas are kept in cold storage medium at 4˚ C after procurement and during processing. The Eye Bank uses Optisol-GS (Bausch & Lomb, Irvine, CA) as their storage medium, which contains dextran, ascorbic acid, vitamin B12, gentamycin and streptomycin. Once the cornea is placed into storage media, it must be used within 14 days. After this time, the cornea is no longer considered suitable for transplantation.
Once ocular tissue arrives at Eye Bank, 3 distinct reviews are performed, and each tissue must clear all required reviews in order to be deemed suitable for transplantation. First, Eye Bank staff members conduct a review of serological testing, which is performed at a certified lab using post-mortem blood drawn at the time of tissue procurement. Special attention is given to results of infectious disease testing, including hepatitis B, hepatitis C, HIV 1 and 2, and syphilis. At Eye Bank, a positive screening test for any of these infectious diseases render the tissue unsuitable for transplantation or research, and a confirmatory test is not performed. An exception applies when testing for syphilis, in which the screening test has a high false positive rate, and thus a confirmatory test is utilized.
Second, eye bank staff members conduct an extensive chart review of the donor’s past history. While paying particularly close attention to the medical history during the last week of the donor’s life, they also look back in the medical history for items such as previous infections, travel history, behavioral risks such as intravenous drug use, and evidence of neurodegenerative disorders. While certain findings can prohibit donation completely, others can result in restrictions on donation. For example, at Eye Bank, donors with a history of diabetes mellitus are not prepared for Descemet membrane endothelial keratoplasty due to increased risk of graft preparation failure 3. In addition, there are age restrictions for cornea donation specific to Eye Bank. For example, for Descemet membrane endothelial keratoplasty prepared corneas, the donor age must be between 50-75 years old. For all other cornea transplants, the donor age can be between 2 and 75 years old.
What is the cornea?
Your eye has a number of layers. The cornea is the ‘window of the eye’ – is the clear dome-shaped outer layer in front of your eye and the main focusing element. The cornea helps to focus light rays on to the retina (the light-sensitive film at the back of the eye). This “picture” is then transmitted to the brain.
Sometimes the cornea can become diseased due to injury or infection, dramatically affecting your vision. Disease of the cornea causes the transparent outer layer of the front of your eye to become cloudy. If other treatments do not help, a corneal transplant can be performed to improve your vision.
There are many causes for the cornea becoming diseased. The 3 common causes that need surgery are keratoconus (where the surface of the cornea becomes cone-shaped, causing blurred vision), endothelial decompensation (where the cornea becomes swollen and cloudy), and scarring.
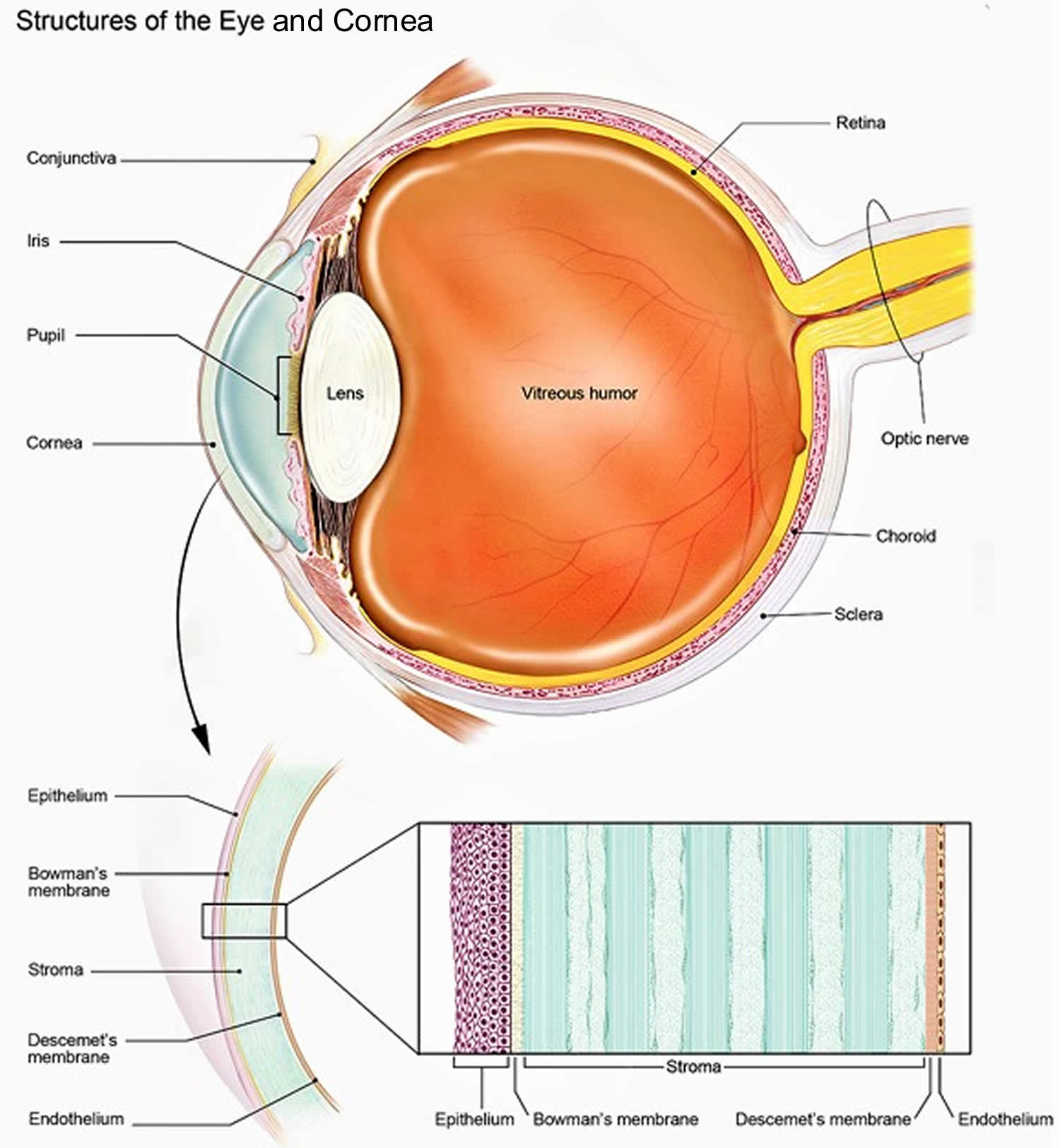
Figure 1. Structures of the cornea
How long does a corneal transplant last?
A corneal transplant can last decades with proper care. Around 95% of full-thickness (penetrating) cornea transplants in low-risk conditions, such as keratoconus, last at least 10 years.
Do I have to take rejection drugs after a cornea transplant?
Different types of corneal transplants are offered depending on what part of the cornea is damaged. All cornea transplant patients use a topical corticosteroid as local anti-rejection treatment. This may be for a long period of time or may be stopped after a year or more depending on the type of transplant performed. In high-risk cornea transplant cases, oral immune suppression therapy may be added to the topical therapy.
Are there any alternatives to a corneal transplant?
Different types of glasses and contact lenses may help.
Some types of keratoconus may be treated by surgery where a small plastic ring is placed in the cornea.
If you have endothelial decompensation, eye drops may be helpful.
All these measures become less effective as the disease gets worse.
What is keratoconus
Keratoconus is an eye disorder where the cornea (the transparent layer of the eye that covers the pupil and iris) becomes thin and changes from being dome-shaped to cone-shaped, resulting in distorted vision. Keratoconus affects between 1 in 3,000 to 1 in 10,000 people.
The exact cause of keratoconus is unknown. There may be a genetic link, and it’s more common in people with multiple allergic conditions, such as eczema and asthma.
Keratoconus is one of the most common reasons for corneal transplantation in younger patients.
Keratoconus doesn’t usually appear until the early teens, but can occasionally occur earlier.
Many cases of keratoconus are mild and can be managed by using contact lenses or glasses.
But in some patients it can progress to the point where a cornea transplant is necessary.
Keratoconus symptoms usually progress slowly and include:
- blurred or distorted vision;
- eyesight that is worsening and requiring many changes in prescription for glasses or contact lenses; and
- sensitivity to light and glare.
Keratoconus causes
The exact cause of keratoconus is not known. However, there are some factors that may be associated with an increased risk of keratoconus, including:
- repeated vigorous eye rubbing;
- atopy an inherited tendency to develop certain allergic conditions (such as hay fever, allergic conjunctivitis, eczema and asthma);
- certain inherited or genetic disorders (including Down syndrome); and
- a family history of keratoconus.
Keratoconus diagnosis and tests
An ophthalmologist (eye doctor) can diagnose keratoconus by examining your eyes and performing vision tests. A slit lamp examination (where your doctor uses a special instrument to view the eyes) can help determine the shape of your cornea.
Imaging of the eyes can also help in the diagnosis of keratoconus. Computerized corneal mapping using so-called optical scanning techniques can take images of the cornea and measure its thickness and shape.
Keratoconus treatment
Treatment for keratoconus depends on how severe it is and how quickly the disease is progressing.
Lenses
Blurred vision associated with mild to moderate keratoconus can be treated with eye glasses or contact lenses. For keratoconus that is getting progressively worse, rigid contact lenses are often preferred because they can be used to stabilise the shape of the cornea as well as improve vision.
There are several other specialized types of contact lenses that can also be used in the treatment of keratoconus.
Surgery
Surgery may be required to treat people with severe keratoconus and those who cannot tolerate wearing contact lenses.
One option is the insertion of plastic intracorneal ring segments, which can help improve the shape of the cornea, slow progression of the disease and improve vision.
In severe cases, corneal transplants may be needed to treat keratoconus.
Corneal collagen cross-linking
A new treatment for keratoconus is emerging, called corneal collagen cross-linking. In this treatment, riboflavin (vitamin B2) eye drops are applied to the cornea, followed by exposure to ultraviolet A (UVA) light. This treatment aims to strengthen and stiffen the cornea and stop (or slow) progression of the disease.
Trials for this potential new treatment are still ongoing, and this type of treatment is not suitable for everyone.
Corneal transplant types
1) Full thickness corneal transplant
Your entire cornea may need to be replaced if both the front and inner corneal layers are damaged. This is called penetrating keratoplasty (PK), or full thickness corneal transplant. Your diseased or damaged cornea is removed. Then the clear donor cornea is sewn into place.
During this procedure, a circular piece of damaged cornea from the center of your eye is removed and replaced with the donated cornea.
In most cases, a circular cutting instrument (similar to a cookie cutter) called a trephine is used to remove the damaged cornea.
The new cornea is held in place by tiny stitches, which sometimes form a star-like pattern around the edges. You may be able to see the stitches faintly after the operation.
The operation may be done under local anesthetic or general anesthetic, and usually takes about 45 minutes.
If local anesthetic is used, you won’t be able to see through the eye during the operation as the anesthetic temporarily stops the eye working.
Most people have to stay in hospital for a night after a full-thickness cornea transplant.
Full-thickness corneal transplant has a longer recovery period than other types of corneal transplants. Getting complete vision back after penetrating keratoplasty may take up to 1 year or longer.
With a full-thickness corneal transplant, there is a slightly higher risk than with other types of corneal transplants that the cornea will be rejected. This is when the body’s immune system attacks the new cornea tissue.
2) Partial thickness corneal transplant
Sometimes the front and middle layers of the cornea are damaged. In this case, only those layers are removed. The endothelial layer, or the thin back layer, is kept in place. This transplant is called deep anterior lamellar keratoplasty (DALK) or partial thickness corneal transplant. Deep anterior lamellar keratoplasty (DALK) is commonly used to treat keratoconus or bulging of the cornea.
Healing time after deep anterior lamellar keratoplasty (DALK) is shorter than after a full corneal transplant. There is also less risk of having the new cornea rejected.
There are several different techniques your surgeon may use, depending on which layers of the cornea are transplanted.
Generally, these techniques can be broken down into transplants involving the front portion of the cornea and those involving the back portion.
Most of these procedures are carried out using cutting instruments, such as a trephine, although lasers are sometimes used.
These procedures can be carried out using either local or general anaesthetic, and you may be able to go home on the same day of the procedure.
Transplanting the front portion of the cornea
The main techniques for transplanting the front parts of the cornea include:
- anterior lamellar keratoplasty (ALK) – removing and replacing only the outer (front) layers of the cornea
- deep anterior lamellar keratoplasty (DALK) – removing and replacing the outer and middle layers of the cornea, leaving the inner (back) layers intact
As with a penetrating keratoplasty, stitches are used to fix the donated cornea in place during both of these procedures.
3) Endothelial keratoplasty
In some eye conditions, the innermost layer of the cornea called the “endothelium” is damaged (see Figure 1). This causes the cornea to swell, affecting your vision. Endothelial keratoplasty is a surgery to replace this layer of the cornea with healthy donor tissue. It is known as a partial transplant since only this inner layer of tissue is replaced. These techniques allow faster visual recovery and have a lower risk of complications. Stitches are not used during either of these procedures. Instead, the donated tissue is held in place using a temporary air bubble.
There are a few types of endothelial keratoplasty. They are known as:
- Descemet’s Stripping (Automated) Endothelial Keratoplasty DSAEK (or DSEK) – replacing the inner lining of the cornea together with about 20% of the corneal supporting tissue (corneal stroma)
- Descemet’s Membrane Endothelial Keratoplasty (DMEK) – replacing only the inner layer of cells of the cornea
Each type removes damaged cells from an inner layer of the cornea called Descemet’s membrane. The damaged corneal layer is removed through a small incision. Then the new tissue is put in place. Just a few stitches—if any—are needed to close the incision. Much of the cornea is left untouched. This lowers the risk of having the new cornea cells being rejected after surgery.
Some things to know:
- With DSEK/DSAEK surgery, the donor tissue may be easier to transplant and position because it is thicker than the donor tissue in DMEK surgery.
- In DMEK surgery, the donor tissue is thin and can be more difficult to transplant. But, the recovery is quicker because the transplant tissue is thinner.
- Your eye surgeon will choose the type of surgery based on your cornea’s condition.
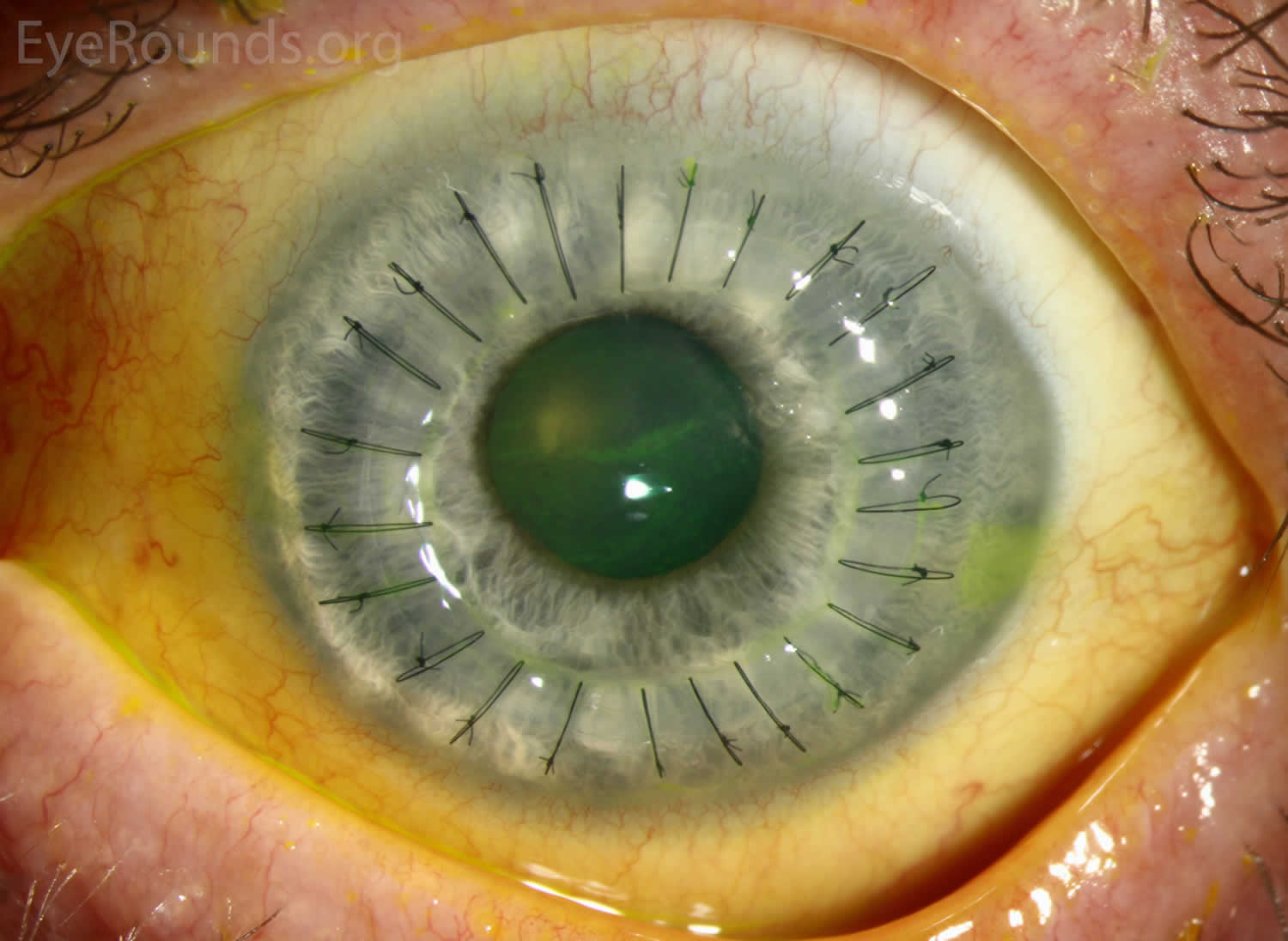
Full-thickness corneal transplant
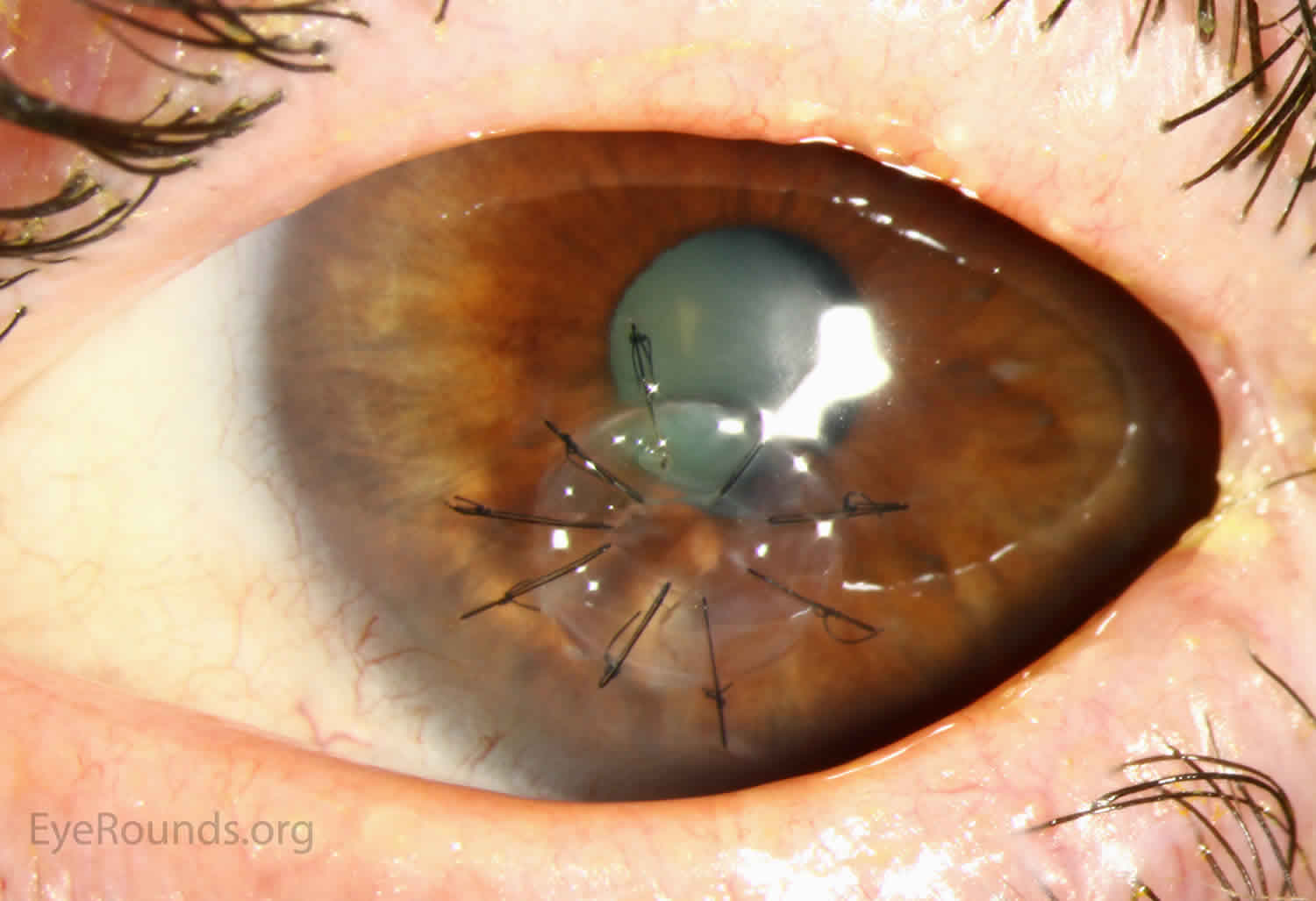
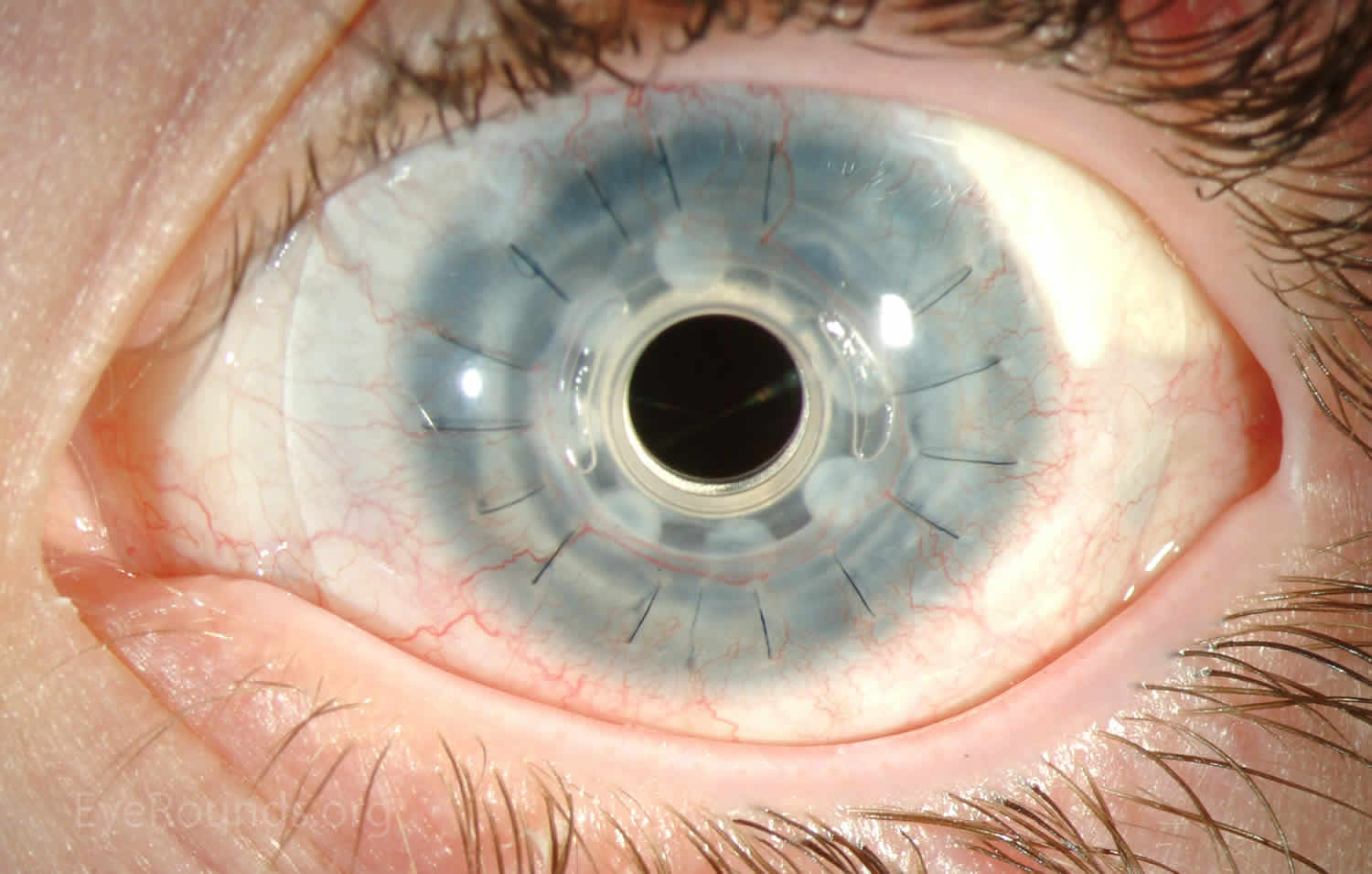
Full-thickness transplant procedure also called penetrating keratoplasty is a corneal transplant surgery in which a trephine of an appropriate diameter is used to make a full-thickness resection of the patient’s cornea, followed by placement of a full-thickness donor corneal graft. Interrupted and/or running sutures are placed in radial fashion at equal tension to minimize post-operative astigmatism (Figure 2). Later, the sutures are removed selectively to reduce the amount of astigmatism present. A corneal transplant can last decades with proper care. While once the most prominent type of corneal transplant, full-thickness corneal transplant has been supplanted by partial thickness techniques for endothelial dysfunction without significant stromal scarring. Full-thickness corneal transplants are performed primarily for visually significant stromal scarring, opacities with an uncertain status of the endothelium or significant posterior corneal involvement, corneal ectasia (such as keratoconus and pellucid marginal degeneration, especially if there is history of hydrops), combined stromal and epithelial disease (such as Peters anomaly), and infectious or non-infectious corneal ulcerations or perforations 4. A variant of the procedure, the mini-full-thickness corneal transplant, can be used to treat more focal defects in the cornea (Figure 3).
Full-thickness corneal transplant grants the ability to treat disease in the epithelial, stromal, and endothelial layers. A full-thickness graft also eliminates optical interface related visual problems that may exist with lamellar transplants with a stroma-stroma interface.
However, postoperative recovery time is relatively long, sometimes taking years to achieve best-corrected visual acuity. Frequently, there is substantial postoperative refractive error due to high regular or irregular astigmatism of the graft, and a higher chance of requiring rigid gas permeable contact lens wear to correct astigmatic error. There is a higher risk of allograft rejection compared with other keratoplasty types. Additionally, PKs carry a higher lifetime risk of wound dehiscence due to the compromised tectonic strength that comes from a full-thickness wound.
Figure 2. Full-thickness corneal transplant
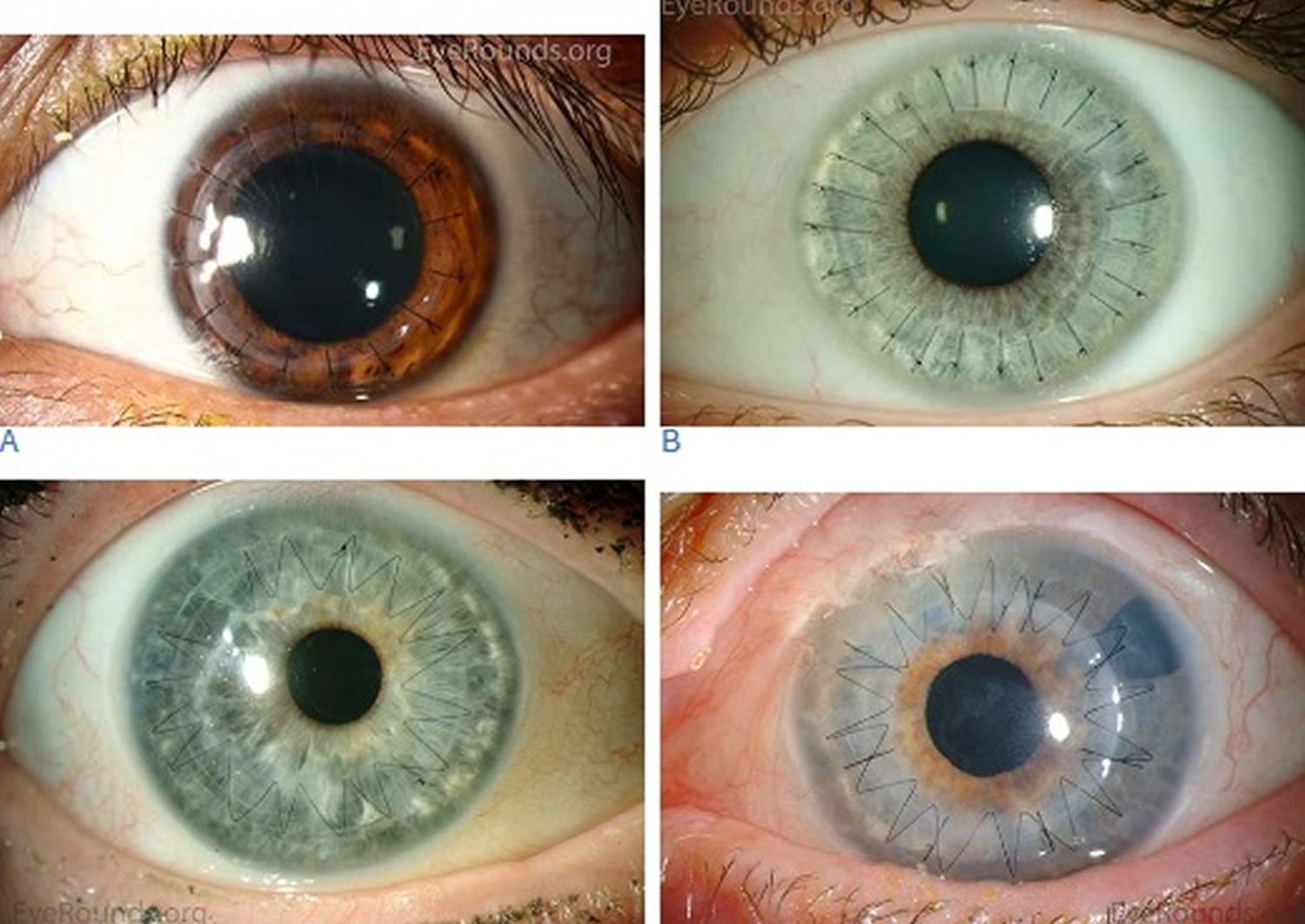
Figure 4. Mini-full-thickness corneal transplant
Partial thickness corneal transplant
Partial thickness corneal transplant also called deep anterior lamellar keratoplasty, is a partial-thickness cornea transplant procedure that involves selective transplantation of the corneal stroma, leaving the native Descemet membrane and endothelium in place 5. A trephine of an appropriate diameter is used to make a partial-thickness incision into the patient’s cornea, followed by pneumodissection or manual dissection of the anterior stroma. This is followed by placement of a graft prepared from a full-thickness punch in which the donor endothelium-Descemet membrane complex has been removed. The intention is to preserve the patient’s Descemet membrane and endothelium. Similar to full-thickness corneal transplant, the graft is secured with interrupted and/or running sutures (Figure 5) and these are then selectively removed post-operatively.
Partial thickness corneal transplant is useful for processes involving the corneal stroma in the presence of healthy endothelium. Examples include corneal ectasia (such as keratoconus in the absence of hydrops), corneal scars that are not full-thickness, and corneal stromal dystrophies 6.
Because it is not a full-thickness procedure, the resultant wound is stronger than that of a full-thickness corneal transplant. Leaving the host endothelium intact significantly decreases the risk of endothelial rejection.
Partial thickness corneal transplant surgery is more complex and difficult to perform than full-thickness corneal transplant. If the Descemet membrane is perforated intraoperatively, the surgeon must convert to a full-thickness corneal transplant. The “big bubble” technique makes dissection more consistent and is the preferred technique 7.
Figure 5. Partial thickness corneal transplant
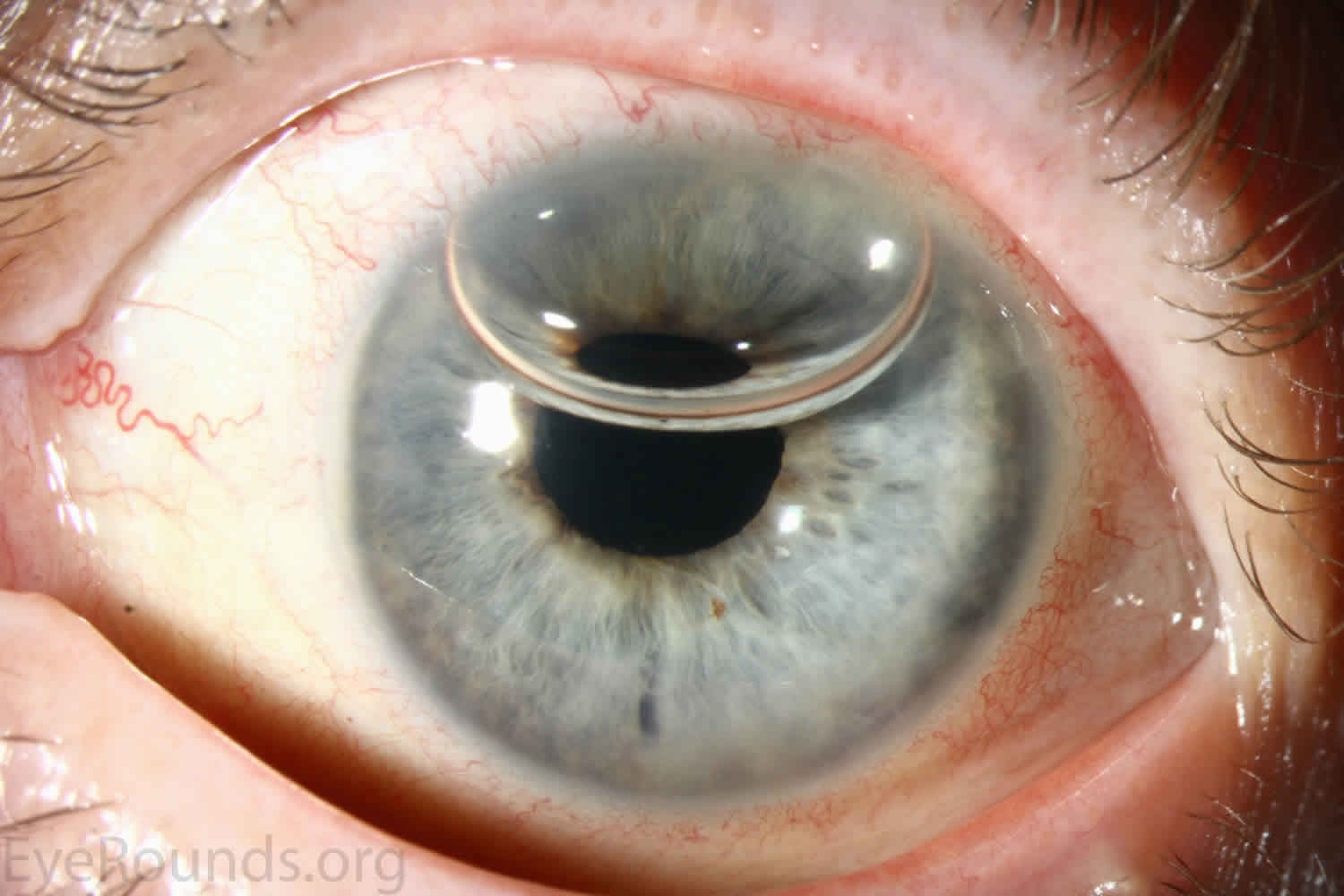
Descemet Stripping Automated Endothelial Corneal Transplant
Descemet Stripping Automated Endothelial Keratoplasty is a partial thickness cornea transplant procedure that involves selective removal of the patient’s Descemet membrane and endothelium, followed by transplantation of donor corneal endothelium in addition to donor corneal stroma 8. The transplanted tissue is approximately 100-200 microns thick. If the endothelium of the graft makes contact with any surgical instruments, it will be damaged and the graft may fail; therefore, the surgical procedure is designed to avoid contacting the donor endothelium. A tunneled corneoscleral incision is created, the recipient endothelium and Descemet membrane is removed, the graft is folded and inserted with non-coapting forceps (forceps that do not meet at the tips), and an air bubble is placed in the anterior chamber to support graft adherence. The procedure is used to treat corneal edema in the setting of endothelial dystrophies (such as Fuchs corneal dystrophy and posterior polymorphous corneal dystrophy), pseudophakic bullous keratopathy, iridocorneal endothelial (ICE) syndrome, endothelial failure in the setting of prior intraocular surgery or of a previous full-thickness corneal transplant graft, and other causes of corneal endothelial dysfunction 9.
Descemet Stripping Automated Endothelial Corneal Transplant offers the advantage of relatively rapid healing time and visual rehabilitation. Compared to full-thickness corneal transplant and partial-thickness corneal transplant, there is less risk of graft rejection and suture-related complications. There is minimal topographic change to the corneal curvature. A somewhat predictable hyperopic shift results (typically 0.8-1.5 D), making intraocular lens selection easier when performing staged or simultaneous cataract surgery.
Postoperative visual acuity can be very good, but there is some limitation from the effects of the stroma-to-stroma graft-host interface. There is also a risk of postoperative graft dislocation.
Descemet Membrane Endothelial Corneal Transplant
Descemet Membrane Endothelial Keratoplasty is a partial-thickness cornea transplant procedure that involves selective removal of the patient’s Descemet membrane and endothelium, followed by transplantation of donor corneal endothelium and Descemet membrane without additional stromal tissue from the donor 10. The graft tissue is merely 10-15 microns thick. Similar to Descemet Stripping Automated Endothelial Keratoplasty (DSAEK), direct contact with the Descemet Membrane Endothelial Keratoplasty graft tissue should be avoided to prevent endothelial cell damage and graft failure. A clear corneal incision is created, the recipient endothelium and Descemet membrane are removed, and the graft is loaded into an inserter. After injecting the tissue into the anterior chamber, the surgeon orients and unscrolls the graft, and a bubble of 20% sulfur hexafluoride (SF6) is placed in the anterior chamber to support graft adherence (Figure 6). A variation known as Descemet membrane automated endothelial keratoplasty (DMAEK) utilized an automated preparation of the donor tissue that left a rim of donor stroma peripherally for easier tissue handling, but the procedure is no longer performed due to advances in Descemet Membrane Endothelial Keratoplasty that have allowed for easier insertion and manipulation of the graft tissue.
The indications for Descemet Membrane Endothelial Keratoplasty (DMEK) are similar to those for Descemet Stripping Automated Endothelial Keratoplasty (DSAEK), including endothelial dystrophies (such as Fuchs corneal dystrophy and posterior polymorphous corneal dystrophy), pseudophakic bullous keratopathy, iridocorneal endothelial (ICE) syndrome, and other causes of corneal endothelial dysfunction 11.
Descemet Membrane Endothelial Keratoplasty offers the most rapid visual rehabilitation of any keratoplasty technique to date 10. Final visual acuity can be outstanding due to minimal optical interface effects. Because less tissue is transplanted, there is a lower risk of allograft rejection and less long-term reliance on topical steroids compared with other types of keratoplasty. Discontinuation of topical steroids can be considered at or before 1 year after the procedure, especially for patients with elevated intraocular pressure.
Because of thinness, fragility, and its characteristic scrolling properties (with the endothelium facing outward), the donor tissue can be difficult to handle and contribute to technical difficulties with the procedure. There is a higher risk of graft edge lifts compared with Descemet Stripping Automated Endothelial Keratoplasty (DSAEK), sometimes requiring a re-bubble procedure.
Figure 6. Descemet Membrane Endothelial corneal transplant
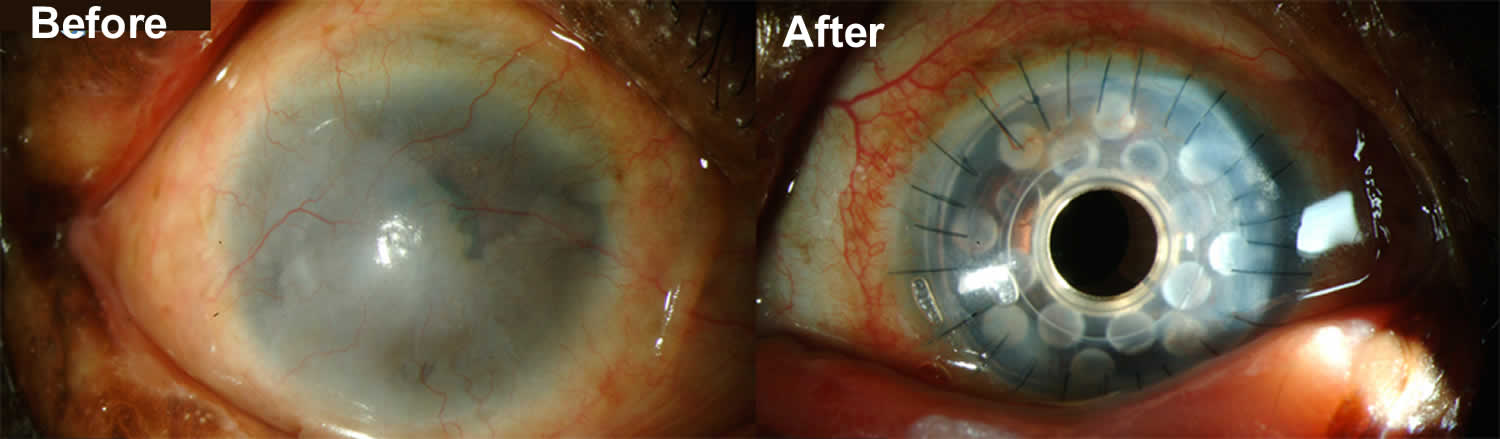
Keratoprosthesis
Keratoprosthesis implantation is a procedure that involves full-thickness removal of the cornea and replacement by an artificial cornea 12. The Boston Type I Keratoprosthesis is currently the most commonly used keratoprosthesis device in the US. It consists of a clear plastic polymethylmethacrylate optic and back plate sandwiched around a corneal graft and secured with a titanium locking ring (see Figures 7 and 8). After the device is assembled, a partial-thickness trephination is performed on the host cornea. Full-thickness resection of the patient’s cornea is then completed using curved corneal scissors. The keratoprosthesis is then secured to host tissue using interrupted or running sutures. Generally, patients who have a history of multiple failed full-thickness corneal transplants are candidates for a keratoprosthesis transplant. Other indications include severe keratitis or ocular surface disease resulting from limbal stem cell failure, such as Stevens-Johnson syndrome, ocular cicatricial pemphigoid, aniridia and chemical injury 13. The Boston Type II Keratoprosthesis is a similar device with a longer optic designed to extend through an opening made in the upper eyelid. It is indicated for the most severe cicatrizing ocular surface diseases.
Keratoprosthesis placement offers relatively fast visual rehabilitation. The devices are amenable for use in many situations in which other types of corneal transplant are not an option.
There is significant long-term risk of complications for those with a keratoprosthesis. Because the keratoprosthesis is a foreign body, there is risk of infection or extrusion of the device. Post-operative glaucoma is common and intraocular pressure is difficult to evaluate as the hard optic makes traditional tonometry impossible. For this reason, glaucoma tube shunts are typically placed at the time of the corneal transplant. The Diaton is currently the preferred way to measure intraocular pressure in these patients in our institution. Patients can form retroprosthetic membranes requiring treatment with a Nd:YAG laser or surgical membranectomy 14.
Figure 7. Artificial cornea implantation components
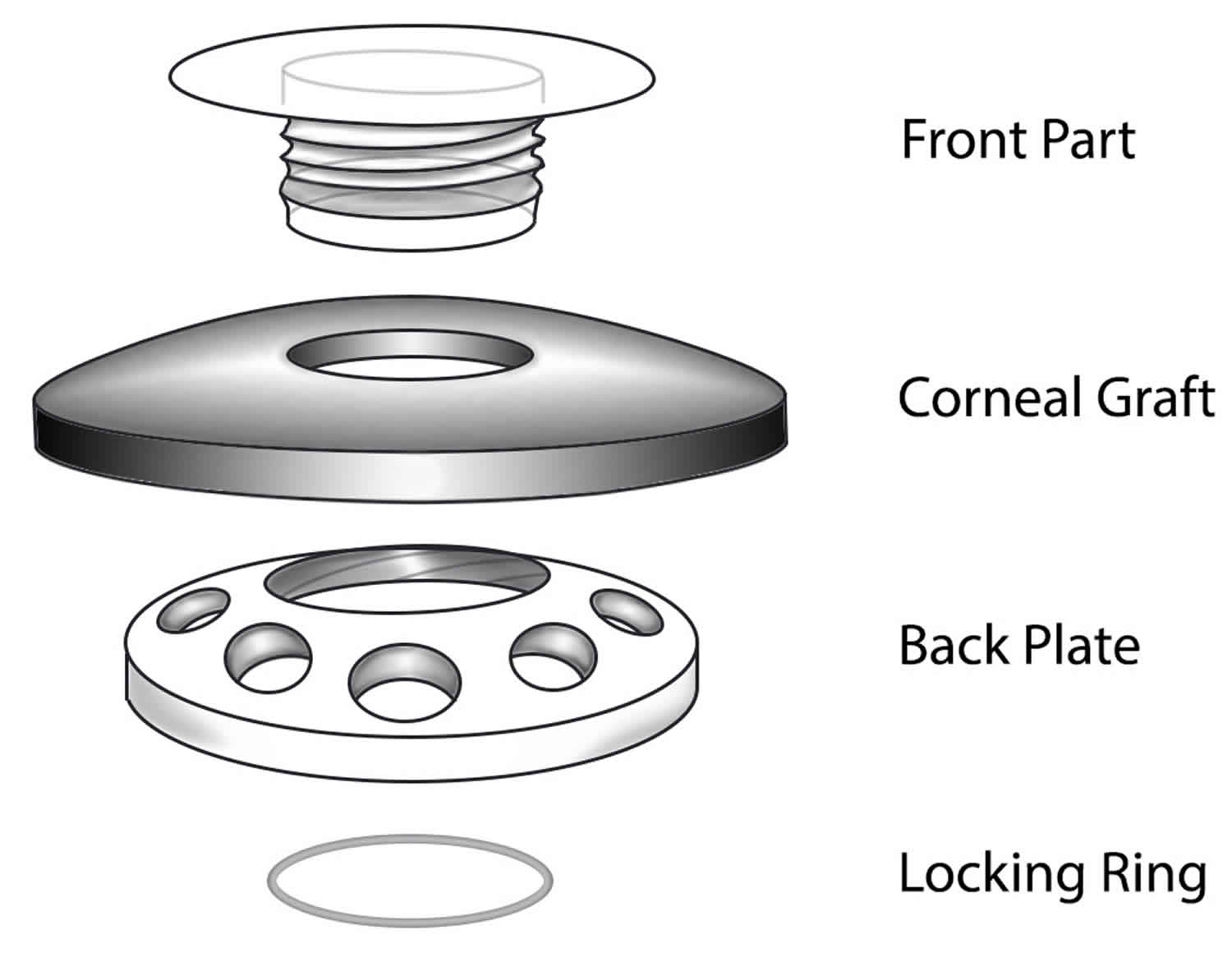
Figure 8. Artificial cornea implantation
Corneal transplant recovery time
The recovery time for a cornea transplant depends on the type of transplant you have.
It takes about 18 months to enjoy the final results of a full-thickness transplant, although it’s usually possible to provide glasses or a contact lens much earlier.
Recovery is usually faster after replacing just the outer and middle layers (DALK).
Endothelial transplants (EK) tend to have a faster recovery time of months or even weeks.
It’s important to take good care of your eye to improve your chances of a good recovery.
This means not rubbing your eye and avoiding activities such as contact sports and swimming until you’re told it’s safe.
Corneal transplant success rate
Corneal transplantation is regarded as the most successful solid organ transplantation procedure 15. Niziol et al. 16 performed a study in 2013 with follow-up averaging 10 years and found that corneal rejection after full-thickness corneal transplant for keratoconus occurred in 44% of grafts, but only 8% of grafts actually failed. While long-term rejection data is not yet available for the newer endothelial corneal transplant procedures, lesser rejection rates have been demonstrated after Descemet Membrane Endothelial Keratoplasty (DMEK) (0.7%) and Descemet Stripping Automated Endothelial Keratoplasty (DSAEK) (9%) than full-thickness corneal transplant (17%) at 2 years in patients on the same postoperative steroid regimen and treated for similar indications 17. This may be secondary to reduced antigen load in the thinner graft tissue. Modern treatment efforts can account for the vast difference between graft rejection and failure. However, graft rejection still remains a significant cause of corneal graft failure 15. The most effective intervention is early recognition and prompt treatment with topical steroid drops. If the patient notices any redness, pain, or decreased vision, it is critical to seek prompt treatment to maximize chances of reversing the rejection episode.
Vision after corneal transplant
Most people who receive a cornea transplant will have their vision at least partially restored. What you can expect after your cornea transplant depends on the reason for your surgery and your health. For people with a deeply scarred or swollen cornea, transplant surgery can restore clear vision.
The time it takes for your vision to return after a cornea transplant can range from as little as a few weeks up to a year or more.
It’s likely you’ll need corrective lenses (either glasses or contact lenses), even after your vision returns.
In some cases, a small operation called arcuate keratotomy or laser treatment is used to correct vision problems after your eyes have healed.
Vision correction after corneal transplant surgery
Your vision may initially be worse than before your corneal transplant surgery as your eye adjusts to the new cornea. It may take several months for your vision to improve.
Once the outer layer of your cornea has healed — several weeks to several months after surgery — your eye doctor will work to make adjustments that can improve your vision, such as:
- Correcting unevenness in your cornea (astigmatism). The stitches that hold the donor cornea in place on your eye may cause dips and bumps in your cornea, making your vision blurry in spots. Your doctor may correct some of this by releasing some stitches and tightening others.
- Correcting vision problems. Refractive errors, such as nearsightedness and farsightedness, can be corrected with glasses, contact lenses or, in some cases, laser eye surgery.
Corneal transplant rejection
In some cases, your body’s immune system may mistakenly attack the donor cornea. This is called rejection, and it may require medical treatment or another cornea transplant.
Rejection is quite a common problem, with symptoms of rejection occurring in about 1 in 5 full-thickness corneal transplants, although only about 5% of low-risk grafts actually fail because of this.
Serious rejection is rare after deep anterior lamellar keratoplasty (DALK).
Rejection can occur a few weeks after a cornea transplant, but it’s more common after several months.
Your risk of complications and cornea rejection continues for years after your cornea transplant. For this reason, expect to see your eye doctor annually.
Cornea rejection can often be managed with steroid eye drops if treatment begins as soon as you notice symptoms.
Signs and symptoms of cornea rejection
You should seek emergency specialist advice if you notice these symptoms after having a cornea transplant:
- Loss of vision – particularly foggy or clouded vision
- Eye pain
- Redness
- Sensitivity to light (photophobia)
Rejection occurs in about 10 percent of cornea transplants.
Corneal transplant complications
As well as rejection, there’s a risk of further problems after cornea transplant surgery.
These can include:
- astigmatism – where the cornea is not a perfectly curved shape
- glaucoma – where pressure builds up in the eye as a result of trapped fluid
- uveitis – inflammation of the middle layer of the eye
- retinal detachment – where the thin lining at the back of your eye called the retina begins to pull away from the blood vessels that supply it with oxygen and nutrients
- the original eye disease (such as keratoconus) returning
- wounds from surgery reopening
- internal infection as a result of surgery wounds
General complications:
- pain
- bleeding
- infection
Specific complications:
- heavy bleeding inside your eye
- inflammation in your other eye
- leak at your wound
- increase in eye pressure
- failure of the transplant
- transferring infection from the donor
Organ rejection is when the body’s immune system sees transplanted tissue as something that shouldn’t be there and tries to get rid of it. Rejection is a problem for up to 3 out of 10 people who have a corneal transplant.
Warning signs of your body trying to reject your cornea transplant include:
- eye pain
- being extra sensitive to light
- redness of the eye
- cloudy or hazy vision
Tell your ophthalmologist right away if you have any of these signs. He or she might be able to stop the rejection with medicine.
Even when corneal transplants work as they should, other eye problems could limit the quality of your vision. For instance, the new cornea might not be curved regularly (called astigmatism). Or you could have an eye disease such as macular degeneration, glaucoma, or diabetic retinopathy.
Some people may need more than one corneal transplant. The first transplant could be rejected, or other problems might occur. However, a repeat transplant has a higher rate of rejection than the first one.
References- Zirm EK. Eine erfolgreiche totale Keratoplastik (A successful total keratoplasty). 1906. Refractive & corneal surgery. Jul-Aug;5(4):258-61.
- Corneal Transplantation: From Donor to Recipient. https://webeye.ophth.uiowa.edu/eyeforum/tutorials/Cornea-transplant-donor-to-recipient/index.htm
- Greiner, MA, Rixen, JJ, Wagoner, MD, et al. Diabetes mellitus increases risk of unsuccessful graft preparation in Descemet membrane endothelial keratoplasty: a multicenter study. Cornea. 2014; 33(11): 1129-1133
- Ing JJ, Ing HH, Nelson LR, Hodge DO, Bourne WM. Ten-year postoperative results of penetrating keratoplasty. Ophthalmology. 1998 Oct;105(10):1855-65.
- Deep Anterior Lamellar Keratoplasty (DALK). https://webeye.ophth.uiowa.edu/eyeforum/tutorials/Cornea-Transplant-Intro/3-DALK.htm
- Fontana L, Parente G, Tassinari G. Clinical outcomes after deep anterior lamellar keratoplasty using the big-bubble technique in patients with keratoconus. American journal of ophthalmology. 2007 Jan;143(1):117-24
- Anwar M, Teichmann KD. Big-bubble technique to bare Descemet’s membrane in anterior lamellar keratoplasty. Journal of cataract and refractive surgery. 2002 Mar;28(3):398-403.
- Descemet Stripping Automated Endothelial Keratoplasty (DSAEK). https://webeye.ophth.uiowa.edu/eyeforum/tutorials/Cornea-Transplant-Intro/4-DSAEK.htm
- Price MO, Price FW, Jr. Descemet stripping with endothelial keratoplasty for treatment of iridocorneal endothelial syndrome. Cornea. 2007 May;26(4):493-7.
- Descemet Membrane Endothelial Keratoplasty (DMEK). https://webeye.ophth.uiowa.edu/eyeforum/tutorials/Cornea-Transplant-Intro/5-DMEK.htm
- Melles GR. Posterior lamellar keratoplasty: DLEK to DSEK to DMEK. Cornea. 2006 Sep;25(8):879-81.
- Keratoprosthesis. https://webeye.ophth.uiowa.edu/eyeforum/tutorials/Cornea-Transplant-Intro/6-kprosth.htm
- Zerbe BL, Belin MW, Ciolino JB, Boston Type 1 Keratoprosthesis Study G. Results from the multicenter Boston Type 1 Keratoprosthesis Study. Ophthalmology. 2006 Oct;113(10):1779 e1-7.
- Greiner MA, Li JY, Mannis MJ. Longer-term vision outcomes and complications with the Boston type 1 keratoprosthesis at the University of California, Davis. Ophthalmology 2011;118(8):1543-50.
- Krachmer JH, Mannis MJ, Holland EJ. Cornea: Fundamentals, Diagnosis, and Management: Mosby Elsevier; 2011.
- Niziol LM, Musch DC, Gillespie BW, Marcotte LM, Sugar A. Long-term outcomes in patients who received a corneal graft for keratoconus between 1980 and 1986. American journal of ophthalmology. 2013 Feb;155(2):213-9 e3.
- Anshu A, Price MO, Price FW Jr. Risk of corneal transplant rejection significantly reduced with Descemet’s membrane endothelial keratoplasty. Ophthalmology 2012 Mar; 119(3):536-40.





{kind=link}