
What is dacryocystitis
Dacryocystitis is infection of the tear (lacrimal) sac usually due to a blockage in the tear (nasolacrimal) duct. The tear sac is a small chamber into which tears drain. The usual cause of dacryocystitis is a blockage of the nasolacrimal duct, which leads from the tear sac into the nose. Dacryocystitis may occur suddenly (acute) or be longstanding (chronic). Dacryocystitis can be classified into acute or chronic and acquired or congenital 1.
There is a bimodal distribution of dacryocystitis with most cases either occurring just after birth in congenital dacryocystitis cases or in adults older than 40 years of age. Congenital dacryocystitis occurs in roughly 1 in 3884 live births. In adults, whites tend to be more affected. Females make up nearly 75% of all cases 2.
Serious morbidity and mortality are low with dacryocystitis. However, in congenital dacryocystitis, there can be significant morbidity and mortality if not treated promptly and appropriately.
Understanding the anatomy and flow of tears leads to a better understanding of dacryocystitis and potential multilevel involvement 3.
The flow of tears will usually begin with tear production by the lacrimal gland. The tears will lubricate the eye until they are collected into the superior and inferior puncta and drained into the superior and inferior canaliculi. From there, tears will drain into the common canaliculus. At this point, they will then pass through the valve of Rosenmuller into the lacrimal sac. The lacrimal sac will then collect the tears and flow down the nasolacrimal duct, pass through the distal valve of Hasner, and finally pass into the nasal cavity 4.
Figure 1. Eyes tear glands and anatomy
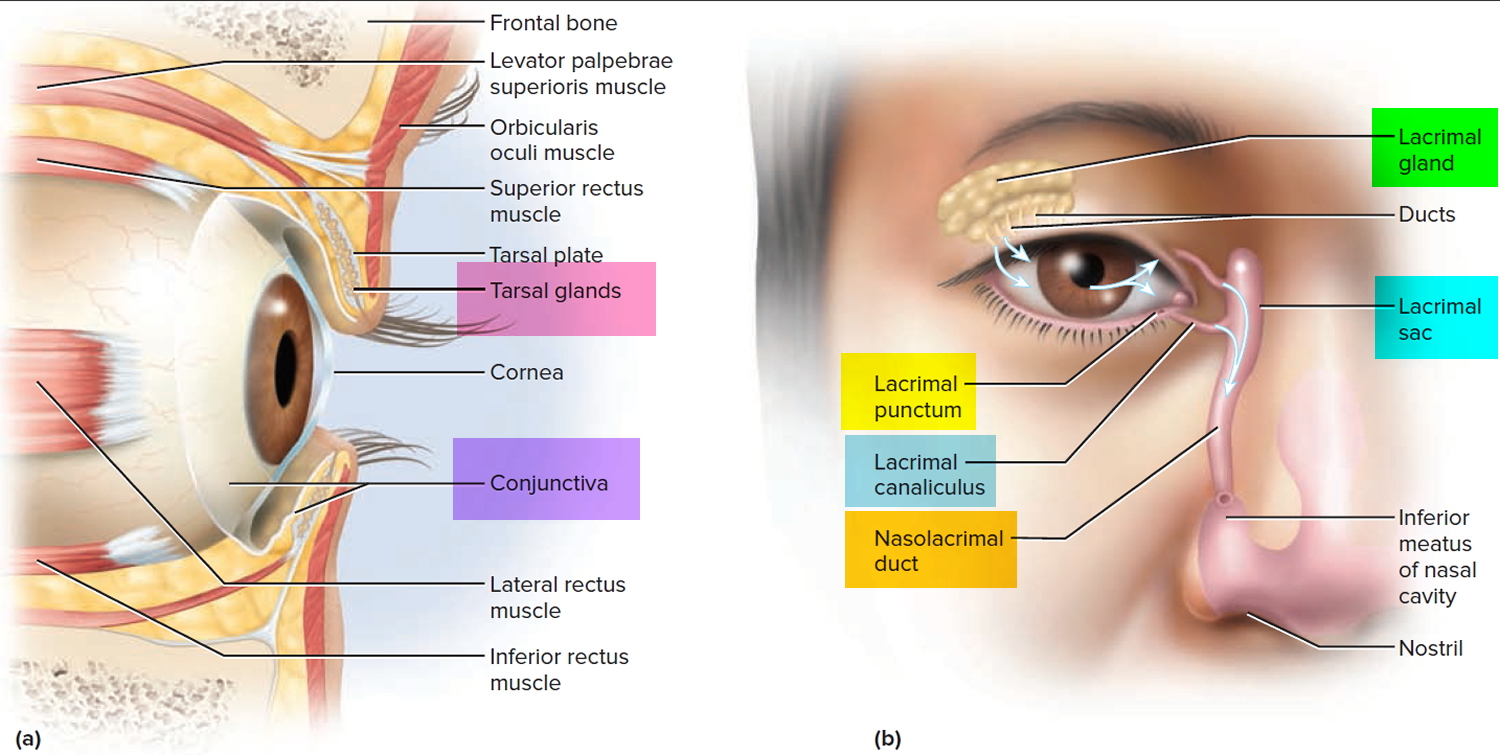
Figure 2. Dacryocystitis infant (congenital dacryocystitis)

Footnote: Acute dacryocystitis. A 4-week-old boy was brought to the emergency department after having drainage from both eyes for 2 days and redness and swelling under his left eye for 1 day. Physical examination revealed a temperature of 38.2°C, purulent drainage from both eyes, and a 1-cm erythematous, fluctuant mass inferior to the medial canthus of the left eye. The white-cell count was 14,000 per cubic millimeter (reference range, 7500 to 15,500). He received a diagnosis of acute dacryocystitis — infection of the nasolacrimal sac — resulting from congenital nasolacrimal duct obstruction. In rare instances, acute dacryocystitis can progress to orbital cellulitis, abscess, and meningitis. The patient received intravenous antibiotic agents, and the fever and eye drainage resolved after the first day of treatment. Culture of a specimen of the drainage fluid grew methicillin-sensitive Staphylococcus aureus. Cultures of urine, blood, and cerebrospinal fluid were negative. Congenital dacryocystitis is a serious disease associated with significant morbidity and mortality. If it is not treated promptly and aggressively, newborn infants can experience orbital cellulitis (because the orbital septum is formed poorly in infants), brain abscess, meningitis, sepsis, and death.
[Source 5 ]Acute dacryocystitis
In acute dacryocystitis, the area around the tear sac is painful, red, and swollen. The area around the eye may become red and watery and may ooze pus. This photo (Figure 1) shows a collection of pus (abscess) that has formed under the skin. Slight pressure applied to the tear sac may push thick material through the punctum (the opening at the inner corner of the eyelid near the nose). The dacryocystitis component will almost always require surgical management.
Figure 3. Acute dacryocystitis

Chronic dacryocystitis
Chronic dacryocystitis causes the skin over the small chamber into which tears drain (tear sac) to bulge. When pressure is applied, the bulge may not be painful, but a puslike or cheeselike material often comes out of the opening at the inner corner of the eyelid near the nose (punctum or tear duct). People with chronic dacryocystitis often also have chronic conjunctivitis (pink eye). Treatment involved intensive antibiotic therapy followed by a dacryocystorhinostomy.
Figure 4. Chronic dacryocystitis

Is dacryocystitis contagious?
No. Dacryocystitis usually occurs because of obstruction of the nasolacrimal duct and subsequent stagnation of tears in the lacrimal sac.
What causes dacryocystitis
Dacryocystitis usually occurs because of obstruction of the nasolacrimal duct and subsequent stagnation of tears in the lacrimal sac. There can be obstructions at any level of the nasolacrimal system. Stagnation of tears will provide a favorable environment for infectious organisms to propagate and proteinaceous debris to form. The lacrimal sac will then inflame causing the characteristic swelling in the inferomedial portion of the orbit.
The obstruction of the nasolacrimal duct may be an idiopathic inflammatory stenosis (primary acquired nasolacrimal duct obstruction) or maybe secondary to trauma, infection, inflammation, neoplasm, or mechanical obstruction (secondary acquired lacrimal drainage obstruction). Obstruction of the nasolacrimal duct leads to stagnation of tears in a pathologically closed lacrimal drainage system which can result in dacryocystitis.
- In children: Staphylococcus aureus, B-hemolytic Streptococcus and Pneumococcus and Haemophilus influenzae
- In adults: Staphylococcus epidermidis, Staphylococcus aureus, Streptococcus pneumoniae and Pseudomonas aeruginosa
An acute infectious state typically causes acute dacryocystitis. In the United States, the most common organism is Staphylococcus and Streptococcus species, followed by Haemophilus influenza and Pseudomonas aeruginosa.
Chronic dacryocystitis is a result of chronic obstruction due to systemic disease, repeated infection, dacryoliths, and chronic inflammatory debris of the nasolacrimal system. Some common systemic diseases include Wegener’s granulomatosis, sarcoidosis, and systemic lupus erythematosus.
Acquired dacryocystitis are typically due to repeated trauma, surgeries, medications, and neoplasms. Among traumatic causes of nasolacrimal obstruction, nasoethmoid fractures seem to be most common. Endonasal and endoscopic sinus procedures have the highest association. Common topical medications associated with acquired states are timolol, pilocarpine, dorzolamide, idoxuridine, and trifluridine. The most common systemic medications are fluorouracil and docetaxel. Primary lacrimal sac tumors and benign papillomas tend to be the most common neoplasms.
Congenital dacryocystitis are due to a membranous obstruction at the valve of Hasner in the distal nasolacrimal duct. Before delivery, the nasolacrimal system is filled with amniotic fluid. When the amniotic fluid fails to be expressed from the nasolacrimal system, it becomes purulent within a few days of delivery and becomes pathologic.
Risk factors for dacryocystitis
- Almost always related to nasolacrimal duct obstruction.
- Nasal pathologies like nasal septum deviation, rhinitis and inferior turbinate hypertrophy on the same side.
- Female is also a known risk factor for the development of this infectious condition due to narrow duct diameter.
- The presence of dacryoliths at various levels of the lacrimal drainage system.
- The occurrence of acute dacryocystitis being more prevalent with increasing age.
Dacryocystitis symptoms
Congenital dacryocystitis is a serious disease associated with significant morbidity and mortality. If it is not treated promptly and aggressively, newborn infants can experience orbital cellulitis (because the orbital septum is formed poorly in infants), brain abscess, meningitis, sepsis, and death.
Acquired dacryocystitis can be acute or chronic.
Acute dacryocystitis is heralded by the sudden onset of pain and redness in the medial canthal region.
Often the dacryocystitis infection is mild. Sometimes, the infection is severe and can cause fever. Sometimes a collection of pus (abscess) may form, which can rupture through the skin, creating a passage for drainage.
Acute dacryocystitis symptoms
- Sudden onset of pain, redness, and edema overlying the lacrimal sac area.
- It is not uncommon for the sac to rupture and fistulize through the skin. This fistula commonly closes after a few days of drainage.
- Conjunctival injection and preseptal cellulitis often occur in conjunction with acute dacryocystitis.
- More serious sequelae of acute dacryocystitis is the extension into the orbit with formation of an abscess and development of orbital cellulitis.
Chronic dacryocystitis symptoms
- Tearing is the most common presentation
- Mattering: This is caused by the obstruction of drainage of the mucous layer of the tear film with collection of debris and denuded epithelial cells from the surface of the eye.
- Chronic low grade bacterial infection inside the lacrimal sac.
Dacryocystitis complications
- Lacrimal fistula formation
- Lacrimal sac abscess
- Orbital cellulitis
- Meningitis
- Brain abscess formation
- Cavernous sinus thrombosis
- Severe sinusitis,
- Permanent loss of vision,
- Death.
Dacryocystitis diagnosis
A doctor bases the diagnosis of dacryocystitis on the symptoms and clinical examination findings in most cases.
- Blood counts may reveal leucocytosis.
- Antineutrophilic cytoplasmic antibody testing can be performed if granulomatosis with polyangiitis (formerly Wegener’s granulomatosis) is suspected. Likewise, antinuclear antibody (ANA) testing can be pursued if systemic lupus erythematosus is suspected.
- Imaging is rarely needed. In most cases it may reveal enlargement of the sac or foreign bodies or masses. Post traumatic cases or cases suspected of harboring an occult malignancy, Computer Tomography (CT) scan may be needed.
- Dacryocystography (DCG) and dacryoscintigraphy are useful to detect anatomical abnormalities.
- Subtraction dacryocystography with a CT scan is also useful in understanding anatomical features of the lacrimal sac and surrounding structures.
- The fluorescein dye disappearance test is useful in the clinic especially in those who cannot be syringed in the clinic. Prolonged retention of the dye usually more than 5 minutes indicates delayed drainage. The Jones test is useful to differentiate a functional block from an anatomical block.
- Nasal endoscopy is useful to rule out hypertrophy of the inferior turbinate, septal deviation and inferior meatal narrowing
Dacryocystitis treatment
- For acute dacryocystitis, antibiotics followed by surgery
- For chronic dacryocystitis, surgery
Acute dacryocystitis is usually treated with an antibiotic taken by mouth. If a fever is present or if the infection is severe, antibiotics given by vein may be required. Coverage should be aimed at gram-positive organisms, particularly antistaphylococcal agents. Applying warm compresses to the area several times a day also helps. After the acute infection resolves, doctors recommend that people have surgery to bypass the blockage (dacryocystorhinostomy [DCR]) so that infection does not recur. Dacryocystorhinostomy is also the main treatment for chronic dacryocystitis. Balloon dacryoplasty, nasolacrimal intubation, and nasolacrimal stenting have all been attempted with variable first-time success rates. If these therapies fail, evaluation for percutaneous dacryocystorhinostomy (DCR) or endonasal dacryocystorhinostomy is then pursued.
Treatment of congenital dacryocystitis includes conservative measures first. Crigler massage should be taught to parents or caregivers to perform at home. Topical antibiotics can be considered for acute flares. About 90% of congenital dacryocystitis will resolve by six months to one year of age with conservative measures. If conservative measures happen to fail, a referral is then made to ophthalmology for nasolacrimal probing. Nasolacrimal probing is successful in more than 70% of cases. If symptoms recur, balloon dacryoplasty, nasolacrimal intubation, or nasolacrimal stenting can be pursued. Ultimately, if these measures fail, then dacryocystorhinostomy by percutaneous or endonasal approach will serve as the definitive treatment.
Acute dacryocystitis treatment
- Application of heat
- Systemic (IV) antibiotics
- Percutaneous abscess drainage
- Dacryocystorhinostomy few weeks after acute infection resolves.
Chronic dacryocystitis treatment
Definitive treatment is a dacryocystorhinostomy, which can be performed as an external or internal endoscopic procedure. Relative contraindications to an internal endoscopic approach would be possible retained foreign body, dacryoliths, suspicion of tumor, or difficult intraoperative nasal visualization.
References- Taylor RS, Ashurst JV. Dacryocystitis. [Updated 2019 Mar 14]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470565
- Chen L, Fu T, Gu H, Jie Y, Sun Z, Jiang D, Yu J, Zhu X, Xu J, Hong J. Trends in dacryocystitis in China: A STROBE-compliant article. Medicine (Baltimore). 2018 Jun;97(26):e11318.
- Hinojosa-Azaola A, García-Castro A, Juárez-Flores A, Recillas-Gispert C. Clinical significance of ocular manifestations in granulomatosis with polyangiitis: association with sinonasal involvement and damage. Rheumatol. Int. 2019 Mar;39(3):489-495.
- Sáenz González AF, Busquet I Duran N, Arámbulo O, Badal Alter JM. Chronic dacryocystitis caused by sarcoidosis. Arch Soc Esp Oftalmol. 2019 Apr;94(4):188-191.
- Acute Dacryocystitis. N Engl J Med 2018; 379:474 DOI: 10.1056/NEJMicm1713250





{kind=link}