Echovirus infection
Echoviruses is short for Enteric Cytopathic Human Orphan viruses, which are members of the Enterovirus genus in the Picornaviridae family that can lead to infections in different parts of the body, and skin rashes 1. Echoviruses make up the largest Enterovirus subgroup, consisting of 29 serotypes 2. Echoviruses are common human pathogens that cause a range of illnesses, from minor febrile illness to severe, potentially fatal conditions (eg, aseptic meningitis, encephalitis, paralysis, myocarditis) 3. Individual serotypes have different temporal patterns of circulation and cause different clinical manifestations. Changes in circulating serotypes and variations in the genotype of the same subtype can be associated with large-scale outbreaks 4.
Echovirus infections are common. In the United States, they are most common in the summer and fall. You can catch the Echovirus if you come into contact with stool contaminated by the virus, and possibly by breathing in air particles from an infected person.
Serious infections with ECHO viruses are much less common but can be significant. For example, some cases of viral meningitis (inflammation of the tissue that surrounds the brain and spinal cord) is caused by an ECHO virus.
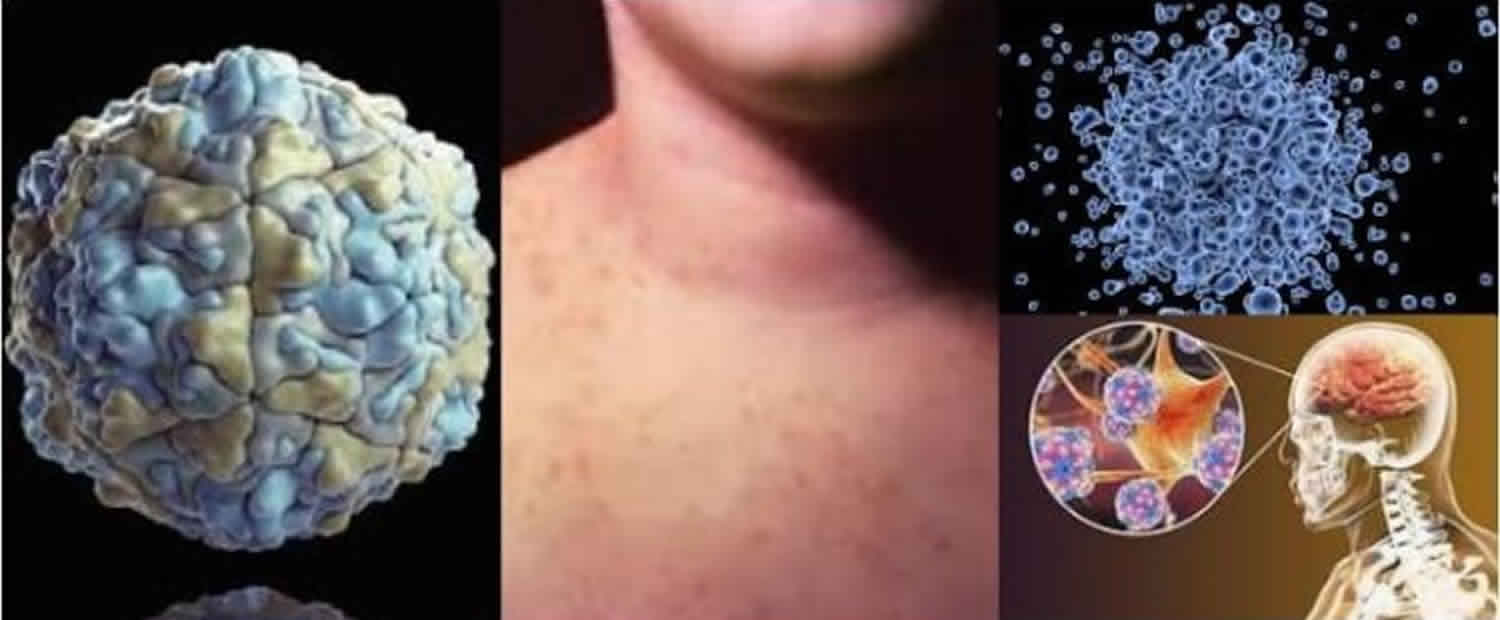
Echoviruses are small nonenveloped viruses with an icosahedral configuration. A capsid composed of 60 subunits is formed from 4 proteins—VP1 to VP4 2. These proteins play important roles in terms of determining host range and tropism and in delivering the RNA genome into the cytoplasm of the host’s cells 5. Echoviruses are infective over a wide range of pH (3-10) and are resistant to ether and alcohol.
Echoviruses were originally classified into 34 serotypes. Echovirus 10 has been reclassified as reovirus 1 and echovirus 28 as rhinovirus 1. Echovirus 9 is now recognized as the same as coxsackievirus A23. Echovirus 22 and 23 have been reclassified as members of the Parechovirus genus, and echovirus 34 is a variant of coxsackievirus A24 6.
Echoviruses were first isolated from the feces of asymptomatic children in the context of epidemiological studies of polioviruses. The viruses produced cytopathic effects in cell cultures but failed to cause detectable pathologic lesions in suckling mice 7. Most echoviruses are no longer considered orphans.
Echovirus infection transmission
Human echoviral infection occurs via fecal-oral transmission. Host susceptibility depends on the presence of specific cellular membrane receptor proteins that bind different enteroviral types along taxonomic lines. Decay-accelerating factor appears to be a major echovirus receptor, binding many echovirus serotypes, including 6, 7, 11, 12, 20, 21, 29, and 33. Echovirus serotypes 1 and 8 bind to the α2 subunit of the very late antigen integrin molecule.
The neonatal Fc receptor (FcRn) has recently been recognized as a pan-echovirus receptor expressed on intestinal enterocytes (primary site of infection) and liver hepatocytes and microvascular endothelial cells lining the blood-brain barrier (secondary sites of infection), potentially explaining enhanced susceptibility of neonates to echovirus infection 8.
Following ingestion of fecally contaminated material, viral replication begins in the pharynx or gut. The precise site of viral entry and initial replication in the GI tract is not well established, but researchers have demonstrated the presence of enteroviruses in mucosal M cells. Ileal lymphoid tissue demonstrates enteroviral replication within 1-3 days after ingestion. The maximal duration of viral excretion is 3-4 weeks in the pharynx and 5-6 weeks in stool.
Following replication, enteroviruses spread to regional lymph nodes and cause subclinical transient viremia. During this low-grade viremia, the virus spreads to reticuloendothelial tissues, including the liver, spleen, bone marrow, and distant lymph nodes. Secondary sites of infection include the central nervous system (CNS), liver, spleen, bone marrow, heart, and lungs. More than 90% of echoviral infections are asymptomatic. When disease occurs, symptoms vary from undifferentiated febrile illness to severe illness, depending on the age, gender, and immune status of the host and the subgroup, serotype, and enteroviral strain 9.
Echovirus infection prevention
The ubiquitous nature of echoviruses, and of enteroviruses in general, and the ease of person-to-person transmission complicate prevention of echoviral infections. As in other enteroviral infections, good overall public health like hand-washing, especially when you are in contact with sick people and adequate clean and potable water, sanitation, and clean living conditions, can act as deterrents.
Currently, no vaccines are available for echovirus infections.
Echovirus symptoms
Echovirus symptoms depend on the site of infection and may include:
- Croup (breathing difficulty and harsh cough)
- Mouth sores
- Skin rashes
- Sore throat
- Chest pain if the infection affects the heart muscle or sac-like covering around the heart (pericarditis)
- Severe headache, mental status changes, fever and chills, nausea and vomiting, sensitivity to light, if the infection affects the membranes covering the brain and spinal cord (meningitis)
Acute aseptic meningitis
More than 90% of community-acquired cases of viral meningitis are caused by group B coxsackieviruses or echoviruses. The most common serotypes are group B coxsackievirus serotypes 2-5 and echovirus serotypes 4, 6, 9, 11, 16, and 30.
Aseptic meningitis is most commonly associated with echovirus 30 3.
Encephalitis
Enteroviruses, including poliovirus, account for 10%-20% of proven cases of viral encephalitis. This ranks behind arboviruses, herpes simplex virus, and lymphocytic choriomeningitis viruses.
Many serotypes have been implicated as causes of encephalitis; coxsackievirus types A9, B2, and B5 and echovirus types 6 and 9 are the serotypes reported most often. The evidence linking each of these serotypes to encephalitis is quite variable.
Paralysis and other neurologic complications of echovirus infections
Sporadic cases of flaccid motor paralysis are associated with echoviruses 6 and 9.
Less frequently implicated serotypes include echoviruses 1-4, 7, 11, 14, 16-18, and 30 10.
Rash
The virus can be isolated from the vesicular lesions of patients with hand-foot-and-mouth disease; therefore, these lesions appear to be a direct result of viral invasion of the skin after viremia.
Serotypes associated with rubellalike rash include coxsackievirus A9 and echoviruses 2, 4, 11, 19, and 25.
Vesicular herpetiform eruptions have been linked to coxsackievirus A9 and echovirus 11.
Respiratory tract infection
Among the echoviruses, serotype 11 is the most firmly established cause of respiratory disease, although serotypes 4, 8, 9, 20, 22, and 25 may also be causal agents.
In volunteers infected experimentally and, occasionally, in patients with naturally acquired disease, some coxsackieviruses and echoviruses may be linked with pneumonia. The role of enteroviruses in lower respiratory illness is not clearly defined; at present, they should be thought of as rare causes of pneumonia.
Herpangina
Group A coxsackieviruses (serotypes 1-10, 16, and 22) most commonly are recovered from patients with herpangina. Other less commonly isolated serotypes from herpangina include group B coxsackieviruses 1-5 and echoviruses 3, 6, 9, 16, 17, 25, and 30.
Epidemic pleurodynia
Group B coxsackievirus is the most important cause of epidemic pleurodynia. Less common agents implicated as a cause of pleurodynia include some group A coxsackieviruses and echoviruses 1, 6, 9, 16, and 19 11.
Chronic meningoencephalitis
This is seen in agammaglobulinemic and immunocompromised hosts.
Echoviruses (and polioviruses) can cause persistent and even fatal CNS infections in immunocompromised patients. Picornaviruses require an extracellular phase for cell-to-cell transfer, providing an opportunity for the virus to be inactivated by antibody-mediated mechanisms.
Most cases have been caused by echoviruses, including types 5, 6, 7, 11, and 27.
Myopericarditis
Enteroviruses appear to be the most common viral etiology of acute myopericarditis. In older children and adults, the disease can range from asymptomatic cardiac involvement to intractable heart failure and death.
Experimental studies in murine models strongly suggest that viral replication occurs in myocytes and results in myocyte necrosis and focal infiltration by inflammatory cells.
A chronic inflammatory process can persist, with variable degrees of fibrosis and loss of myocytes 9.
Hepatitis
Fulminant hepatitis has been reported with echovirus 9, 18, and 25 in persons receiving anti-CD 20 antibody 12.
Echovirus infection complications
Complications vary with the site and type of echovirus infection. Heart infections may be deadly, while most other types of infection improve on their own.
Acute aseptic meningitis
Complications (eg, febrile seizures, complex seizures, lethargy, coma, movement disorders) occur early in the course of aseptic meningitis in 5-10% of patients.
Adults may experience a more prolonged period of fever and headache than infants and children; some adult patients may require weeks to return to normal activity.
Paralysis and other neurologic complications
Paralytic disease caused by nonpolio enteroviruses characteristically is less severe than poliovirus-associated paralysis. In fact, muscle weakness is more common than flaccid paralysis, and the paresis is usually not permanent.
Cranial nerve involvement occasionally has resulted in complete unilateral oculomotor palsy. Cases of fatal bulbar involvement are rare.
Guillain-Barré syndrome and transverse myelitis have been reported in a small number of patients in association with echovirus.
Echovirus diagnosis
Because echovirus illness is often mild and has no specific treatment, testing for echovirus is often not done.
If needed, ECHO virus can be identified from:
- Rectal culture
- Spinal fluid culture
- Stool culture
- Throat culture
Until recently, echoviral infections were diagnosed via isolation of the virus in cell culture. The diagnosis can be proven by isolating the virus in blood, cerebrospinal fluid (CSF), tissue, or pericardial fluid. Pharyngeal and stool cultures may be helpful but are not diagnostic, as asymptomatic shedding can persists for several weeks after acute infection.
Polymerase chain reaction (PCR)
Reverse transcriptase polymerase chain reaction (RT-PCR) and nucleic acid sequence–based amplification are rapid, sensitive, and specific methods of detecting echoviral RNA in clinical specimens. The quick turnaround time offers advantages in terms of patient management decisions.
Reverse transcriptase polymerase chain reaction (RT-PCR) has detected echoviral RNA from cerebrospinal fluid (CSF), throat swabs, serum, and stool samples 13. Quality control is essential to minimize laboratory cross-contamination and false-positive results.
Serology
Serologic testing for echoviral infection has limited value. The results are slow, depend on acute and convalescent titers, and are not type-specific. Regardless of titer, a single antibody result is most often useless.
Radiography
Myopericarditis produces enlargement of the cardiac silhouette on chest radiography in approximately 50% of cases, due to either pericardial effusion or cardiac dilatation.
Echocardiography
Echocardiography may confirm the presence of acute ventricular dilatation, decreased cardiac ejection fraction, or pericardial effusion.
Electrocardiography (ECG)
Pericarditis and myocarditis produce electrocardiographic changes ranging from ST-segment elevation or nonspecific ST-segment and T-wave abnormalities. Severe myocardial disease may lead to the development of Q waves, ventricular tachyarrhythmias, and all degrees of heart block.
Echovirus treatment
Most echoviral infections almost always clear up on their own. No specific medicines are available to fight the echovirus. Medical treatment is supportive and symptomatic. Immune system treatment called intravenous immunoglobulin (IVIg) may help people with severe ECHO virus infections who have a weakened immune system with persistent echoviral infection. The role of IVIG in serious infections has not been subjected to adequate clinical trials. Nonrandomized trials in neonates and children with myocarditis treated with IVIG showed improved recovery in ventricular function compared with children treated without IVIG 14.
Antibiotics are not effective against the Echovirus, or any other virus.
Pleconaril, an experimental agent with in vitro activity against most enteroviruses, was evaluated in clinical trials, in a study of 79 patients, those treated with the agent demonstrated modest benefit. But Pleconaril has not been approved by the FDA for use as an antiviral agent 15.
Echovirus infection prognosis
People who have the less severe types of ECHO virus illness should recover completely without treatment. Infections of organs such as the heart may cause severe disease and can be deadly.
References- ECHO virus. https://medlineplus.gov/ency/article/001340.htm
- Echovirus Infection. https://emedicine.medscape.com/article/216564-overview
- Khetsuriani N, Lamonte-Fowlkes A, Oberst S, Pallansch MA. Enterovirus surveillance–United States, 1970-2005. MMWR Surveill Summ. 2006 Sep 15. 55(8):1-20.
- Yarmolskaya MS, Shumilina EY, Ivanova OE, Drexler JF, Lukashev AN. Molecular epidemiology of echoviruses 11 and 30 in Russia: different properties of genotypes within an enterovirus serotype. Infect Genet Evol. 2015 Mar. 30:244-8.
- Ruecker RR. Picornaviridae and their replication. Fields BN, Knipe DM, eds. Virology. 2nd ed. New York: Raven Press; 1990. 507.
- King AQM, Brown F, Christian P, et al. Picornaviridae. Andrew M.Q. King, , Michael J. Adams, , Eric B. Carstens, and Elliot J. Lefkowitz. Ninth report of the International Committee on Taxonomy of Viruses. New York: Academic Press; 2012. 855-880.
- Echoviruses of Enteroviruses Infection. http://virology-online.com/viruses/Enteroviruses6.htm
- Morosky S, Wells AI, Lemon K, Evans AS, Schamus S, Bakkenist CJ, et al. The neonatal Fc receptor is a pan-echovirus receptor. Proc Natl Acad Sci U S A. 2019 Feb 26. 116 (9):3758-3763.
- Romero JR and Modlin JF. Coxsackieviruses, echoviruses, and newer enteroviruses. Bennett JE, Dolin R, Blaser MJ, eds. Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases. 8th ed. Philadelphia, PA: Elsevier Inc.; 28 Aug 2014. Vol 2: 2080-90.
- Dhole TN, Ayyagari A, Chowdhary R, Shakya AK, Shrivastav N, Datta T, et al. Non-polio enteroviruses in acute flaccid paralysis children of India: vital assessment before polio eradication. J Paediatr Child Health. 2009 Jul-Aug. 45 (7-8):409-13.
- Bell EJ, Grist NR. ECHO viruses, carditis, and acute pleurodynia. Am Heart J. 1971 Jul. 82(1):133-5.
- Nicolini LA, Canepa P, Caligiuri P, Mikulska M, Novi G, Viscoli C, et al. Fulminant Hepatitis Associated With Echovirus 25 During Treatment With Ocrelizumab for Multiple Sclerosis. JAMA Neurol. 2019 Apr 8.
- Kupila L, Vuorinen T, Vainionpäa R, Marttila RJ, Kotilainen P. Diagnosis of enteroviral meningitis by use of polymerase chain reaction of cerebrospinal fluid, stool, and serum specimens. Clin Infect Dis. 2005 Apr 1. 40(7):982-7.
- Drucker NA, Colan SD, Lewis AB, Beiser AS, Wessel DL, Takahashi M, et al. Gamma-globulin treatment of acute myocarditis in the pediatric population. Circulation. 1994 Jan. 89(1):252-7.
- Desmond RA, Accortt NA, Talley L, Villano SA, Soong SJ, Whitley RJ. Enteroviral meningitis: natural history and outcome of pleconaril therapy. Antimicrob Agents Chemother. 2006 Jul. 50(7):2409-14.





{kind=link}