
What is fibrous dysplasia
Fibrous dysplasia is an uncommon skeletal disorder in which bone-forming cells fail to mature and produce too much fibrous, or connective, tissue. Areas of healthy bone are replaced with this fibrous tissue. The replacement of normal bone in fibrous dysplasia can lead to pain, misshapen bones, and fracture, especially when it occurs in the long bones (arms and legs). When it occurs in the skull, there can also be a replacement of the normal bone with fibrous tissue, resulting in changes in the shape of the face or skull, pain, and, in rare circumstances, hearing or vision loss.
Fibrous dysplasia may appear in children, usually between the ages of 3 and 15 and young adults, and is present throughout life. About 70% of people with fibrous dysplasia have only one bone involved (monostotic), whereas other people have more than one bone involved (polyostotic). Fibrous dysplasia may occur alone, or as part of a condition known as the McCune-Albright syndrome. Boys are more often diagnosed with fibrous dysplasia than girls, except for McCune-Albright syndrome — which is more common in girls and affects the bones and skin and is associated with hormonal imbalance and often precocious (premature) puberty.
Fibrous dysplasia is subdivided into three types:
- Monostotic fibrous dysplasia: This is the least complicated form of fibrous dysplasia. It only affects one bone, most often the femur (thigh), tibia (shin), rib cage or one of the facial bones.
- Polyostotic fibrous dysplasia: This form of fibrous dysplasia, which affects a younger age group than the monostotic form, can involve numerous bones, sometimes more than half of all bones in the skeletal system.
In addition to bone deformity, this condition can lead to fractures, skin lesions and legs of different lengths. - McCune-Albright syndrome: This form of fibrous dysplasia, the most complex, is associated with abnormalities of the endocrine system. Some or all of the following problems can be involved:
- polyostotic fibrous dysplasia
- patches of pigmented skin (light brown or “café-au-lait” spots)
- early puberty (precocious puberty)
- excess growth hormone (gigantism or acromegaly)
- hyperparathyroidism
- vitamin D-resistant rickets
- hyperthyroidism (excess thyroid hormone)
- excess cortisol (Cushing’s syndrome)
- short stature because of the premature closing of growth plates in the affected bones
Fibrous dysplasia can affect any bone in the body. The most common sites are the bones in the skull and face, femur (thighbone), tibia (shinbone), humerus (upper arm), pelvis, and ribs 1. Although many bones can be affected at once—and affected bones are often found on one side of the body—the disease does not “spread” from one bone to another; that is, the pattern of which bones are involved is established very early in life and does not change with age.
Though many people with fibrous dysplasia do not have any symptoms, others may have bone pain, abnormally shaped bones (deformities), or an increased risk of fractures (broken bones). The problems a person experiences depend on which bones are affected, and may arise from compression and displacement of adjacent structures to the lesions. For example, the legs can be of different lengths, leading to a limp, the bones of the sinuses can be affected, leading to chronic sinus congestion or headache.
While there is no cure for fibrous dysplasia, the symptoms can be treated. Medications known as bisphosphonates can reduce pain and surgery may be used to treat fractures or to correct misshapen bones.
See your doctor if you or your child develops any of the following:
- Bone pain that increases with weight-bearing activity or doesn’t go away with rest
- Bone pain that interrupts sleep
- Difficulty walking or limping
- Unexplained swelling
- Changes in bone shape
- Difference in limb length
Figure 1. Polyostotic fibrous dysplasia

Footnote: A case of polyostotic fibrous dysplasia giving an appearance of pseudo-hypertelorism (upper row). The excess bone was contoured, a dorsal nasal augmentation was done with cranial bone graft and medial canthopexy was performed. The lower row shows the results 6 months postoperative.
[Source 2 ]Is there a cure for the disease so I can get rid of fibrous dysplasia for good?
In general, fibrous dysplasia cannot be cured at the present time. The only exception is if there is only one lesion in one bone and that lesion is completely eliminated by surgery. Often there are unidentified fibrous dysplasia cells in several bones and it is not possible to eliminate all of these by surgery. Some drug treatments have been identified that significantly diminish bone pain in long bones (arms, legs, ribs) in many patients with fibrous dysplasia. Bisphosphonate drugs such as alendronate (Fosamax) that is used for treating osteoporosis or pamidronate (Aredia) have been helpful for some people. These drugs are not effective in all people with fibrous dysplasia; but researchers are continuing to investigate other possible treatments.
Is fibrous dysplasia hereditary?
Fibrous dysplasia is not hereditary. You did not get fibrous dysplasia from your parents and you cannot pass it on to your children. Fibrous dysplasia is caused by a gene mutation that occurs sometime during development of a baby while it is still in the mother’s uterus. If the gene mutation occurs early in development, many tissues may be affected. If it occurs late in development, very few tissues may have the mutation. Because the gene mutation occurs before birth, fibrous dysplasia is considered a genetic disease. But unlike almost all other diseases it is not hereditary because it cannot exist in sperm or egg cells.
How rare is fibrous dysplasia?
Among bone tumors, fibrous dysplasia is fairly common; but it is a rare disease in the general population. Based on statistics from the Fibrous Dysplasia Foundation membership as of 2000, an incidence of one person with fibrous dysplasia out of every 15,000 – 30,000 people has been estimated. This estimate includes only people whose fibrous dysplasia causes symptoms that lead to a diagnosis using current medical technology. It is difficult to know how many people might have the disease, but will never know it because they don’t experience the complications that lead to a diagnosis. The estimated incidence suggests that between 9,000 and 18,000 people in the US will have a diagnosis of fibrous dysplasia in their lifetime.
What part of the body does fibrous dysplasia typically affect?
Monostotic fibrous dysplasia is the least complicated type of fibrous dysplasia. It affects only one bone and most often occurs in the ribs, thigh bone, shin bone, or one of the facial bones. For the polyostotic form, the lesions often occur in younger patients and can involve numerous bones, sometimes more than half of the bones in the skeletal system. The most common sites in polyostotic fibrous dysplasia include the skull, face, thigh bone, shin bones, upper arm, pelvis, and ribs. Although when multiple bones are affected, they are often found on one side of the body, the disease does not “spread” from one bone to another. In fact, the pattern in which bones are involved is established very early in life and does not change with age.
The distribution of bone sites for the Fibrous Dysplasia Foundation 318 members with monostotic fibrous dysplasia is as follows:
- Craniofacial (Head: skull/mandible/facial bones): 46%
- Lower limbs (legs/hips/pelvis): 45%
- Upper limbs (arm, hand): 6%
- Axial skeleton (ribs/spine/clavicle): 3%
An interesting finding from the analysis is that patients diagnosed with monostotic fibrous dysplasia were as likely to have the effected bone site in the skull (46%) as with all other bones in the body combined (54%). This appears to be somewhat significant since the skull contains only 29 of the body’s 206 bones and is a proportionately smaller bone mass when compared to the rest of the skeleton. There did not appear to be any difference in the reported bone sites between men and women with monostotic fibrous dysplasia.
How can people with fibrous dysplasia slow growth of bone lesions?
There are no treatments which can slow growth of the bone lesions in fibrous dysplasia. Bisphosphonates may be helpful for bone pain; however there is no evidence that they affect the bone lesions. Uncontrolled growth hormone excess increases growth of craniofacial fibrous dysplasia, so screening and treating patients for this is very important.
How is fibrous dysplasia going to affect my life now and in the future?
There is no simple answer for this question. The effects of fibrous dysplasia are as different as each person who has it. For some people, it has no impact at all, while others are so intensely impacted by fibrous dysplasia that they are forced to use a cane or a wheelchair, and have become disabled in some way, such as in partial loss of vision or mobility. Therefore, it is best to know exactly where your fibrous dysplasia exists and to regularly monitor its presence with medical check-ups. If you are aware of what is happening to your body, you are in a better position to control or minimize the impact of fibrous dysplasia on your life now and in the future.
Can people with fibrous dysplasiaparticipate in physical activities including contact sports, or should they avoid them?
Patients with fibrous dysplasia should use common sense in deciding what physical activities to participate in. Patients with a lot of fibrous dysplasia and high risk for fractures should likely avoid contact sports and other high risk activities.
Does craniofacial fibrous dysplasia pose risks for the brain?
Craniofacial fibrous dysplasia usually does not disrupt the vital structures in the skull, including the vessels or brain. Craniofacial cases may have associated cranial nerve deficits including vision and hearing loss 3. Rarely vision and hearing may be affected, so all patients should have these checked yearly.
Does fibrous dysplasia cause problems in pregnancy? Are there special precautions to take?
Many women with fibrous dysplasia/McCune-Albright syndrome have successful pregnancies. There is no evidence that pregnancy will make fibrous dysplasia worse or increase bone pain. Women who have fibrous dysplasia involving the spine, ribs or pelvis should consider seeing a high risk obstetrician (maternal-fetal-medicine) during pregnancy.
Women who have a history of precocious puberty continue have ovarian cysts in adulthood. This may lead to irregular and heavy bleeding. It may take these women longer to become pregnant. Consider seeing a fertility specialist if pregnancy is not achieved after 6-12 months of unprotected sex.
How can people with fibrous dysplasia treat and manage pain?
When a patient with fibrous dysplasia develops pain, the first step is to rule out orthopedic causes, such as fractures, bone cysts, and gait problems. Patients should also be checked for hypophosphatemia, which can worsen bone pain. For pain that is not related to these factors, the first steps in treatment should be conservative measures, including rest, massage, heat or cold packs, and over-the-counter medications such as ibuprofren and acetaminophen. For moderate or severe pain that does not respond to these treatments, intravenous bisphosphonates such as zoledronate and pamidronate may be helpful. These should be given at the lowest dose and frequency needed to control the pain. Because fibrous dysplasia is a chronic condition, long-term narcotic medications should be avoided if possible. If these medications are needed, they should be prescribed from a specialist as part of a multidisciplinary pain clinic.
Can fibrous dysplasia become cancerous?
Rarely, an affected area of bone can become cancerous 4. Malignant transformation to sarcoma is rare but can occur with a prior history of radiation therapy 5.
Do I have cancer and can fibrous dysplasia become malignant?
Fibrous dysplasia is not cancer. “Tumor” simply means abnormal growth. Tumors can be malignant (cancerous) or benign (non-cancerous). Many people prefer to use to term “lesion” generally meaning any defect to avoid confusion of fibrous dysplasia with malignant bone tumors.
Usually, for a cancer to form, several mutations have to occur in the same cell over time. The same mutation that causes fibrous dysplasia has been found in a few pituitary cancers and very rarely in different types of cancer. Since most people with fibrous dysplasia do not have these cancers, the fibrous dysplasia mutation does not seem to cause cancers by itself. It is possible for an fibrous dysplasia bone lesion to become cancerous; but this is very rare, occurring in less than 1% of fibrous dysplasia cases.
My doctor said fibrous dysplasia would subside after my teen years. Is this true?
Older medical texts often suggested that fibrous dysplasia lesions would stop growing once a child reached full adult stature. Many people do experience fewer problems with fibrous dysplasia after puberty, especially with fibrous dysplasia lesions in the legs and arms. However, some people continue to have problems with their fibrous dysplasia beyond puberty and first diagnosis of fibrous dysplasia may occur in adulthood 6.
Can bisphosphonate therapy stop the progression of fibrous dysplasia in adults?
To date, bisphosphonate therapy has not been shown to stop the progression of fibrous dysplasia in adults, however it does appear to decrease bone pain and improve the appearance of bone lesions on X-ray 7.
Is the long-term use of bisphosphonates for treatment of fibrous dysplasia associated with an increased risk for bone fracture?
We were unable to find information regarding an increased risk for bone fracture in people with fibrous dysplasia who undergo short or long-term treatment with bisphosphonates. Rare but serious complications have been described in patients who received bisphosphonate therapy for other indications (e.g., osteoporosis).
So far studies investigating the use of bisphosphonate therapies for treatment of fibrous dysplasia have been small and uncontrolled. Further information regarding the benefits and complications associated with bisphosphonate therapy for treatment of fibrous dysplasia is likely on the horizon. The National Institute of Dental and Craniofacial Research at the National Institutes of Health completed a three year, phase 2, clinical trial of Fosamax (Alendronate) for treatment of fibrous dysplasia. The clinical trial was entitled ‘Alendronate to Treat Polyostotic Fibrous Dysplasia and McCune-Albright Syndrome.’ Go here (https://www.clinicaltrials.gov/ct2/show/NCT00001728?cond=%22Fibrous+dysplasia%22) to view the study information. In our search, we were unable to find published results from the trial. You can contact the National Library of Medicine Customer Service for further assistance in searching the medical literature for published results.
What are the similarities of fibrous dysplasia with other diseases?
There are a number of diseases that have similar sounding names or similar features, but are not fibrous dysplasia. The following provides a brief synopsis of one of these diseases.
Cherubism is a rare, familial, usually painless disorder characterized by enlargement of the upper and lower jaw bones (maxilla and mandible) on both sides of the face (bilateral). The disease is transmitted in an autosomal dominant fashion. Those affected by the disease have unusual chubbiness and swelling of the face. The facial changes can vary considerably from person to person; they can be very mild to severely disfiguring. The facial changes are brought about by overgrowth of fibrous tissue around the jaw bones. The disease starts to appear around age 2 or 3 and continues to grow until the person affected reaches the age of 15-20. The size of the jaw then stabilizes and progressively becomes smaller until it is hardly noticeable. fibrous dysplasia and Cherubism have several features in common but differences also exist between these diseases. At times, it can be difficult to tell the difference between the two.
What are the Symptoms of fibrous dysplasia and McCune-Albright syndrome?
Some people with fibrous dysplasia may have no symptoms; the bone lesions may be found only because an X-ray was done for some other reason. Others, especially those with more bones involved, may have many. These symptoms may include pain, enlargement or deformity of the bone, and fractures due to the weakened bone. Very rarely the bone deformities may affect the ability to walk, or the function of nerves in the head that control vision or other senses. Those who have McCune-Albright syndrome may have a variety of endocrine problems such as early puberty or over-production of thyroid hormones.
What types of doctors or specialists are best suited for working with me on fibrous dysplasia?
Rather than one doctor, it may be better to gather a team of medical professionals and service providers to work with you on a treatment plan for your fibrous dysplasia, because fibrous dysplasia often affects people in different ways. For instance, in addition to your internist or general practitioner, you may need the services of many other specialists based on the seriousness of your particular circumstances and effected areas of the body. The following is a partial list of specialists and related areas of practice: (Please note: this is a suggested list only and does not take the place of medical advice.)
It is probably best to see specialists shortly after diagnosis to get a complete understanding of what aspects of the disease are present, and which are not. Try and get a sense of your doctor’s experience with fibrous dysplasia/McCune-Albright syndrome or other rare disorders. If he or she is inexperienced (or even if he or she isn’t), it’s often good to get second opinions – especially if a procedure, operation, or medication is being recommended.
- Jawbone, Skull (facial bones)
- Craniofacial surgeon (with experience in plastic and reconstructive surgery)
- Otolaryngology (ENT or ear, nose, and throat and problems related to sinuses)
- Neuro-opthamologist (to monitor vision and optic nerve issues, and test peripheral vision and depth of field)
- Maxillo-facial surgeon (jawbones, cheekbones)
- Dentist/orthodontist (teeth)
- Bones Below the Neck (arms, legs, spine, ribs)
- Orthopedist
- Rehabilitation Medicine doctor (physiatrist)
- Physical therapist (exercise/strength training/rehabilitation for overall reconditioning
- Occupational therapist (exercise/training for particular skills)
- Endocrine Issues (body chemistry/hormones, pregnancy)
- Endocrinologist (with specialty in bone-related conditions)
- Obstetrician/Gynecologist (for gynecologic and reproductive issues)
- Pain Management-Anesthesiologist
- Internist/Primary Care physician
- Mental health
- Psychologist (note: meets to discuss emotional issues relating to illness, moods, and/or problem behaviors using cognitive/intellectual methods. May work with a psychiatrist to prescribe medications)
- Psychiatrist
- Primary Care physician
- Stress Management Program (to develop strategies for coping with stress related to chronic illness)
- Alternative Care
- Massage therapist (pain management)
- Acupuncturist (pain management)
- Physical therapist
- Nutrition Counselor/Dietician (to help manage weight issues, issues connected with healthy eating)
- Health Club (for maintaining physical conditioning and to relieve stress)
Craniofacial fibrous dysplasia
Craniofacial fibrous dysplasia is a bone disease of the face and skull that replaces normal bone with fibrous-type tissue. This tissue is not as hard as normal bone, and because it is soft and stringy, it makes the bone more fragile and prone to break.
Craniofacial fibrous dysplasia may cause shifting of facial features and facial asymmetry, such as incorrect placement of the eyes, misalignment of the jaw, and other problems.
Craniofacial fibrous dysplasia signs and symptoms
Signs and symptoms of fibrous dysplasia affecting the skull may include:
Facial asymmetry
- Shifting facial structure that can affect any bone in the face
- Nasal airway obstruction
- Jaw and bite misalignment, in some cases making it difficult to chew and swallow
- Visual and hearing problems due to compression of the optic nerve or acoustic nerve
Additionally, children with craniofacial fibrous dysplasia may experience symptoms related to bone weakness in other parts of the body, including bone fractures or deformities, bone pain, or bone lesions which may stop growing when the child reaches puberty.
Children with polyostotic fibrous dysplasia may also experience:
- Endocrine gland problems, such as early puberty, thyroid disorders and related issues
- Unusual skin patches, called café-au-lait pigmentation, ranging from light brown to dark brown in color
Craniofacial fibrous dysplasia treatment
While several surgical options are available to treat facial fibrous dysplasia, your child’s treatment will depend on the location of the bones affected and the severity of the condition.
- Surgery is usually done through limited incision approaches and hidden incisions in the hair. This can help reduce visible scarring.
- If the affected areas of the face are small and easily accessible, treatment usually involves complete surgical removal (resection) of the area and reconstruction using a combination of bone grafts and materials such as titanium plates and screws.
- If the area affected is too large or too important to be removed, the size of the bone may be reduced to normal using a high speed burr.
- In some patients, a combination of bone reduction with a burr and bone grafting may be utilized.
- If the facial fibrous dysplasia is in an area where it is growing and compressing nerves, removing some of the surrounding bone can decompress the nerve.
- In severe cases where the jaw is displaced and malocclusion occurs, a combined therapy with orthodontics will utilize osteotomies (bone cuts) to reposition abnormally placed bones.
If surgery is required on a particular facial region such as the skull base, your plastic surgeon may work together with a neurosurgeon or ophthalmologist to ensure the most effective treatment. If your child’s condition involves the jaw, plastic surgeons will collaborate with orthodontists if needed.
Your child may need additional surgeries over the course of treatment for facial fibrous dysplasia. In severe cases, the excess bone may grow back over time and require repeated treatments.
After surgery for facial fibrous dysplasia, your child should expect to stay overnight in the Hospital. Depending on the complexity of the surgery required, your child may be hospitalized anywhere from one to several days.
Follow-up care
Your child will need to return for evaluation approximately one to two weeks after surgery. Regular follow-up visit will be needed and are commonly done every three months for the first year, and then yearly, based on your child’s condition.
In cases where the bone has been shaped or contoured — usually to preserve vital structures and because the disease affects a large volume of bone — recurrence of the bony overgrowth may occur and secondary procedures may be necessary.
During follow-up visits, your child’s physician will perform a physical exam and may order X-rays or CT scan of the affected area until your child reaches skeletal maturity. If your child was diagnosed with polyostotic fibrous dysplasia, he may also be referred to an endocrinologist for periodic testing of any endocrine or hormone related disorder.
Craniofacial fibrous dysplasia prognosis
Outcomes for children treated for craniofacial fibrous dysplasia have been excellent. Because fibrous dysplasia is persistent, continued clinical monitoring is essential in long-term management of the condition.
Fibrous dysplasia causes
Fibrous dysplasia is caused by a defective GNAS gene in the cells which encodes the cyclic AMP pathway-associated G-protein that form bone called Gsalpha (Gsα) and other affected tissues 8. GNAS mutations in fibrous dysplasia are known to occur at one of two amino acid residues: Arg201 (>95% of reported cases) 9 or Gln227 (<5%) 10. These mutations disrupt the intrinsic GTPase activity of Gsalpha (Gsα), causing constitutive activation of adenylyl cyclase and inappropriate cyclic AMP signaling. Involvement of the skin, bone, and endocrine systems is consistent with a mutational event early in embryogenesis, occurring prior to derivation of the 3 germ cell layers 8. The phenotype in individuals with fibrous dysplasia is thus the result of the distribution of tissues containing the GNAS mutation, and the role played by Gsα signaling in those tissues.
The gene mutation occurs at some point after conception, most likely early in fetal development. This means that the disorder is not inherited from an affected person’s parents, nor can an affected person with the condition pass it on to his or her children. The likelihood of getting fibrous dysplasia does not appear to be influenced by gender, race, ethnic background, geographic location, or by any environmental exposures.
The mutation results in the production of immature and irregular bone tissue. Most often the irregular bone tissue (lesion) is present at a single site on one bone. Less often multiple bones are affected, and there may be more than one lesion on multiple bones.
A lesion usually stops growing sometime during puberty. However, lesions may grow again during pregnancy.
The gene mutation associated with fibrous dysplasia occurs after conception, in the early stages of fetal development. Therefore, the mutation isn’t inherited from your parents, and you can’t pass it on to your children.
Scientists do not know why the fibrous dysplasia gene mutation occurs. The gene involved in fibrous dysplasia seems to be especially susceptible to mutations. Although fibrous dysplasia is rare, it occurs in males and females and in people of all races and from all parts of the world. It is likely that the mutation occurs randomly. There is nothing that a parent can do, either before or during pregnancy, that will cause or prevent the fibrous dysplasia mutation from happening.
Fibrous dysplasia symptoms
Fibrous dysplasia may cause no symptoms, mild symptoms, or severe symptoms. The most common symptoms of fibrous dysplasia are painful, misshapen, and/or broken bones (fractures). Fractures are more common between the ages of 6 and 10, but often persist into adulthood. The problems a person experiences depend on which bones are affected. For example, the legs can be of different lengths, leading to a limp and the need for a shoe lift. The bones of the sinuses can be affected, leading to chronic sinus congestion. Only very rarely do serious problems such as vision loss or cancer occur.
In rare cases, fibrous dysplasia is associated with abnormalities in the hormone-producing glands of the endocrine system. This may lead to precocious puberty, hyperthyroidism (excess thyroid hormone production), excess growth hormone (gigantism or acromegaly), and/or excess cortisol production (Cushing syndrome). If the face or skull bones are affected, hearing or vision loss may occur.
More severe fibrous dysplasia may cause:
- Bone pain, usually a mild to moderate dull ache
- Swelling
- Bone deformity
- Bone fractures, particularly in the arms or legs
- Curvature of leg bones
Fibrous dysplasia can affect any bone in the body, but the most commonly affected bones include the following:
- Thighbone (femur)
- Shinbone (tibia)
- Upper arm bone (humerus)
- Skull
- Ribs
- Pelvis
Rarely, fibrous dysplasia may be associated with a syndrome that affects the hormone-producing glands of your endocrine system. These abnormalities may include:
- Very early puberty
- Overactive hormone production
- Light brown spots on the skin
Increased bone pain also may be associated with the normal hormonal changes of the menstrual cycle or pregnancy.
Fibrous dysplasia complications
Severe fibrous dysplasia can cause:
- Bone deformity or fracture. The weakened area of an affected bone can cause the bone to bend. These weakened bones also are more likely to fracture.
- Vision and hearing loss. The nerves to your eyes and ears may be surrounded by affected bone. Severe deformity of facial bones can lead to loss of vision and hearing, but it’s a rare complication 3.
- Arthritis. If leg and pelvic bones are deformed, arthritis may form in the joints of those bones 11.
- Cancer. Rarely, an affected area of bone can become cancerous 4. This rare complication usually only affects people who have had prior radiation therapy 5.
Fibrous dysplasia diagnosis
The primary tool for diagnosis of fibrous dysplasia is an X-ray. The bones in people with fibrous dysplasia have a characteristic appearance on x rays, which is usually sufficient to make the diagnosis. While bone appears solid in an X-ray, a fibrous dysplasia lesion has a relative distinct appearance often described as “ground glass.” The condition may be diagnosed, therefore, even in a person with no symptoms who is getting an X-ray for other reasons.
An X-ray can also help your doctor determine how much of the bone is affected and whether there is any deformity in the bone.
In some cases, a doctor may need to obtain a small bone specimen (a biopsy) to confirm the diagnosis. This test uses a hollow needle to remove a small piece of the affected bone for microscopic analysis. The structure and arrangement of cells can confirm a fibrous dysplasia diagnosis.
Additional tests may be used to confirm a diagnosis or rule out other disorders:
- Other imaging tests, such as magnetic resonance imaging (MRI) or computed tomography (CT) may also be indicated. Computerized tomography and magnetic resonance imaging can produce cross-sectional or 3-D images of bone. These tools can help your doctor better characterize the quality of bone or a fracture associated with fibrous dysplasia.
- Bone scan. A bone scan is a nuclear imaging test. A small amount of radioactive tracer is injected into your bloodstream and taken up by damaged portions of bone. When your body is scanned with a specialized camera, the images can help a doctor identify multiple fibrous dysplasia lesions.
- The usefulness of gene testing is not clear. Since the mutated gene is only present in fibrous dysplasia tissues, it is best to test only the DNA from affected tissue, but even then, doctors do not know with certainty how useful such a test is.
Table 1. Recommended Evaluations Following Initial Diagnosis in Individuals with Fibrous Dysplasia/McCune Albright Syndrome
| Organ System | Evaluation | Comment | |
|---|---|---|---|
| Constitutional (growth) | Review growth 1 | For signs of poor growth, which could suggest hyperthyroidism | |
| For signs of rapid growth, which could indicate growth hormone excess &/or precocious puberty | |||
| IGF-1, random growth hormone, prolactin levels | |||
| Bone age | Advanced bone age may suggest the presence of precocious puberty. | ||
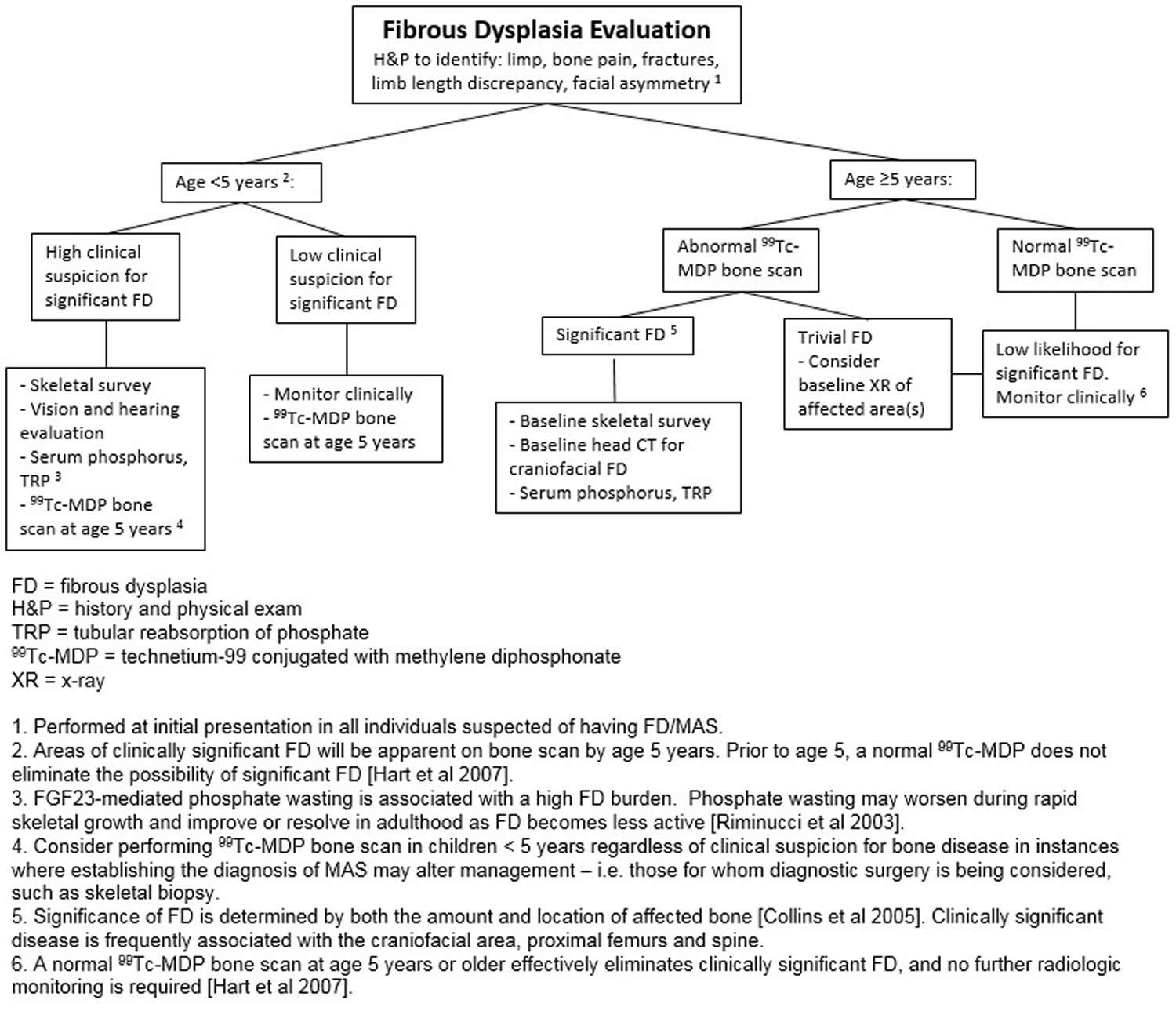
| Musculoskeletal 2 | Clinical evaluation for scoliosis | Further radiographic confirmation may be necessary. | |
| Total body bone scintigraphy 3 | The majority of clinically significant skeletal lesions are apparent on bone scan by age 5 yrs. | ||
| Radiographs (axial & appendicular) &/or CT (craniofacial) of areas of fibrous dysplasia | To more clearly evaluate extent & anatomy of lesions | ||
| Endocrine | Puberty (females) | Evaluation for signs & symptoms of precocious puberty | |
| Puberty (males) | Evaluation for signs & symptoms of precocious puberty | ||
| Serum LH, FSH, & testosterone levels | |||
| Testicular ultrasound | To evaluate for discrete hyper- & hypoechoic lesions & microlithiasis | ||
| Thyroid | Thyroid ultrasound | For signs of mixed cystic & solid lesions | |
| T3, free T4, & TSH levels | The primary biochemical abnormality is elevated T3 production, which may occur in the setting of normal T4 and free T4. | ||
| Adrenal | Assessment for signs & symptoms of Cushing syndrome | e.g., hypertension, facial plethora, abdominal obesity, developmental delay, failure to thrive | |
| If no signs or symptoms of hypercortisolism after age 3 yrs, no further evaluation needed | |||
| Renal | Serum phosphorus level | Verification by calculating tubular reabsorption of phosphorus | |
| Eyes | Evaluation by neuroophthalmologist | In those with craniofacial fibrous dysplasia | |
| ENT | Evaluation by otolaryngologist | In those with craniofacial fibrous dysplasia | |
| Evaluation by audiologist | |||
| Gastrointestinal | Serum amylase, lipase, AST, & ALT | ||
| Screening for symptoms of GERD | |||
| Other | Consultation w/clinical geneticist &/or genetic counselor | ||
Footnotes:
CT = computed tomography
GERD = gastroesophageal reflux disease
1. Including determining predicted adult height and mid-parental height
2. See Figure 2 for recommended evaluations of the skeletal system after diagnosis.
3. Collins et al 12
Figure 2. Fibrous dysplasia recommended evaluations of the skeletal system
Fibrous dysplasia treatment
Unfortunately, there is no cure for fibrous dysplasia. Treatment depends on the symptoms present:
- Fractures often require surgery, but can sometimes be treated with casting or splints 14. Surgery is most appropriate in cases where fractures are likely to occur, or where bones have become misshapen. Surgery may also be used to relieve pain.
- Medications known as bisphosphonates —approved by the U.S. Food and Drug Administration for the treatment of other bone diseases, are also used to relieve bone pain 15.
- Other healthy strategies such as physical activity and adequate intake of calcium, phosphorus, and vitamin D are also important.
Radiation therapy is not recommended for patients with fibrous dysplasia because it is associated with an increased risk of cancerous transformation.
Careful, long-term follow-up to monitor fibrous dysplasia is advised.
Medications
Osteoporosis medications called bisphosphonates help prevent bone loss by decreasing the activity of cells that normally dissolve bone. Some studies suggest that bisphosphonates may strengthen bones affected by fibrous dysplasia and may relieve bone pain.
Surgery
Your doctor may recommend surgery in order to:
- Correct a deformity
- Correct a difference in limb lengths
- Repair a fracture that does not heal with casting
- Prevent fractures
- Relieve pressure on a nerve, particularly if the lesion is in your skull or face
Surgery may involve removing the bone lesion and replacing it with a bone graft: bone from another part of your body, bone tissue from a donor or a synthetic material. In some cases a fibrous dysplasia lesion may develop again.
Your surgeon also may insert metal plates, rods or screws to prevent fractures or to stabilize a bone or bone graft.
Endocrine Follow-up
- Pituitary: Growth hormone (GH) and prolactin (PRL) excess are common in McCune-Albright syndrome (20%). The signs and symptoms can be very subtle. Growth hormone (GH) excess can worsen craniofacial bone disease.
- All patients should have an oral glucose tolerance test (OGTT) to assess for non-suppressible growth hormone (GH) at least once (GH > 2.0 ng/ml at 60 min on standard oral glucose tolerance test (OGTT) is diagnostic).
- Non-suppressible growth hormone (GH) with elevated insulin-like growth factor-1 (IGF-1) should be treated
- What to do with non-suppressible growth hormone (GH) and normal IGF-1 is not clear (these patients will have an abnormal overnight GH secretion pattern)
- Thyroid: Hyperthyroidism is common.
- Check thyroid function tests (TSH, FT4, T3, T4). T3 dominant hyperthyroidism is most common, 40%)
- Treat with an oral anti-thyroidal (methimazole, PTU)
- If definitive treatment is needed, we recommend surgery not radioiodine (thyroid cancer in McCune-Albright syndrome is rare, and radioiodine could be an additional risk factor beyond the Gs mutation).
- Annual ultrasound of the thyroid to follow lesions and biopsy clearly dominant, large or changing lesions.
- Parathyroid: Primary hyperparathyroidism is rare, secondary (to vitamin D deficiency) is common.
- Check ionized calcium or total calcium and PTH annually.
- Adrenal: Cushings in the neonatal period occurs, but has not been reported past the first year. Some cases of neonatal Cushings resolve spontaneously.
- Check adrenal reserve in resolved cases of neonatal Cushings.
- Renal: Phosphate wasting with or without hypophosphatemia, and/or rickets/osteomalacia is common (40%).
- Check serum phosphate and renal phosphate handling (second AM void or 24 hour urine for GFR).
- Treat frankly low or low-normal serum phosphate with low GFR
- Gonads: Precocious puberty in girls is common, precocious puberty in boys is less common, small testicular masses of leydig cell hyperplasia are common.
- Treat precocious puberty in girls with an aromatase inhibitor (preferred), or tamoxifen.
- Treat precocious puberty in boys with an aromatase inhibitor and an anti-androgen.
- Check for and treat secondary central precocious puberty in children with precocious puberty with a long-acting GnRH agonist.
- Check for Leydig cell masses in men with screening testicular ultrasounds suspicious masses should undergo excisional biopsy to exclude cancer.
Recommended for follow-up of patients with fibrous dysplasia/McCune-Albright syndrome
- Craniofacial: very common, especially skull base, vision loss is uncommon, hearing loss even more uncommon, sarcomatous degeneration is rare, while axial and appendicular fibrous dysplasia quiets with age, craniofacial bone disease probably continues to slowly progress.
- Find a craniofacial and neurosurgical team experienced in treating craniofacial fibrous dysplasia (https://fibrousdysplasia.org/resources-for-patients/physician-database/)
- Avoid surgery in the absence of visual or hearing impairment. (nerves may be surrounded by and unaffected by fibrous dysplasia bone for decades).
- Severe pain or severe disfigurement may be an indication for surgery as well.
- Annual vision testing by a neuro-ophthalmologist and annual hearing testing are recommended.
- Annual CT of skull and mandible are recommended.
- Screen for and treat all endocrinopathies which adversely affect bone.
- Little evidence that bisphosphonates are effective in craniofacial fibrous dysplasia (even for pain).
- Bone scan at baseline and at some interval, potentially every few years.
- Axial and Appendicular skeleton: very common, fractures frequent (esp. before 15 y.o.), shepherd’s crook deformity common, pain common, sarcomatous degeneration (cancer) rare.
- Find an orthopedic surgeon experienced with fibrous dysplasia (https://fibrousdysplasia.org/resources-for-patients/physician-database/)
- In general, less is better in the surgical treatment of fibrous dysplasia.
- Bracing may potentially be helpful
- Screen for and treat all endocrinopathies which adversely affect bone.
- Bone scan at baseline and at some interval, potentially every few years.
- Bisphosphonates can decrease pain and markers of bone turnover, probably no effect on course of disease or fracture rate.
- Maintaining strength is important. Swimming is an excellent exercise, cycling is good also.
Fibrous dysplasia life expectancy
Individuals with milder forms of fibrous dysplasia often live normal, otherwise healthy lives and can expect a normal life expectancy. However, the prognosis is as widely variable as fibrous dysplasia itself, and is based on the bones affected, whether other structures such as nerves are affected, whether fractures occur and what complications you have.
Fibrous dysplasia can affect many bones in the body, but once it has established in the skeleton, it doesn’t spread.
References- Fibrous Dysplasia Overview. https://www.bones.nih.gov/health-info/bone/additional-bone-topics/fibrous-dysplasia
- Sharma RK. Hypertelorism. Indian J Plast Surg. 2014;47(3):284-92. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4292104
- Boyce AM, Brewer C, DeKlotz TR, Zalewski CK, King KA, Collins MT, Kim HJ. Association of Hearing Loss and Otologic Outcomes With Fibrous Dysplasia. JAMA Otolaryngol Head Neck Surg. 2018 Feb 01;144(2):102-107
- Ruggieri P, Sim FH, Bond JR, Unni KK 1994 Malignancies in fibrous dysplasia. Cancer 73:1411-1424
- Qu N, Yao W, Cui X, Zhang H. Malignant transformation in monostotic fibrous dysplasia: clinical features, imaging features, outcomes in 10 patients, and review. Medicine (Baltimore). 2015 Jan;94(3):e369
- FAQs about FD/MAS. https://fibrousdysplasia.org/disease-information/faqs/
- Silverman SL. Bisphosphonate use in conditions other than osteoporosis. Annals of the New York Academy of Sciences. 2011; 1218:33-37. http://www.ncbi.nlm.nih.gov/pubmed/20946575
- Boyce AM. Fibrous Dysplasia. [Updated 2015 Sep 14]. In: Feingold KR, Anawalt B, Boyce A, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK326740
- Lumbroso S, Paris F, Sultan C 2004 Activating Gsalpha mutations: analysis of 113 patients with signs of McCune-Albright syndrome–a European Collaborative Study. The Journal of clinical endocrinology and metabolism 89:2107-2113
- Idowu BD, Al-Adnani M, O’Donnell P, Yu L, Odell E, Diss T, Gale RE, Flanagan AM 2007 A sensitive mutation-specific screening technique for GNAS1 mutations in cases of fibrous dysplasia: the first report of a codon 227 mutation in bone. Histopathology 50:691-704
- Kushare IV, Colo D, Bakhshi H, Dormans JP. Fibrous dysplasia of the proximal femur: surgical management options and outcomes. J Child Orthop. 2014 Dec;8(6):505-11
- Collins MT, Kushner H, Reynolds JC, Chebli C, Kelly MH, Gupta A, Brillante B, Leet AI, Riminucci M, Robey PG, Bianco P, Wientroub S, Chen CC. An instrument to measure skeletal burden and predict functional outcome in fibrous dysplasia of bone. J Bone Miner Res. 2005;20:219–26
- Boyce AM, Florenzano P, de Castro LF, et al. Fibrous Dysplasia/McCune-Albright Syndrome. 2015 Feb 26 [Updated 2018 Aug 16]. In: Adam MP, Ardinger HH, Pagon RA, et al., editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2019. Available from: https://www.ncbi.nlm.nih.gov/books/NBK274564
- Fibrous Dysplasia. http://www.childrenshospital.org/conditions-and-treatments/conditions/f/fibrous-dysplasia
- Fibrous dysplasia. https://www.mayoclinic.org/diseases-conditions/fibrous-dysplasia/symptoms-causes/syc-20353197





{kind=link}