What is glomerular filtration
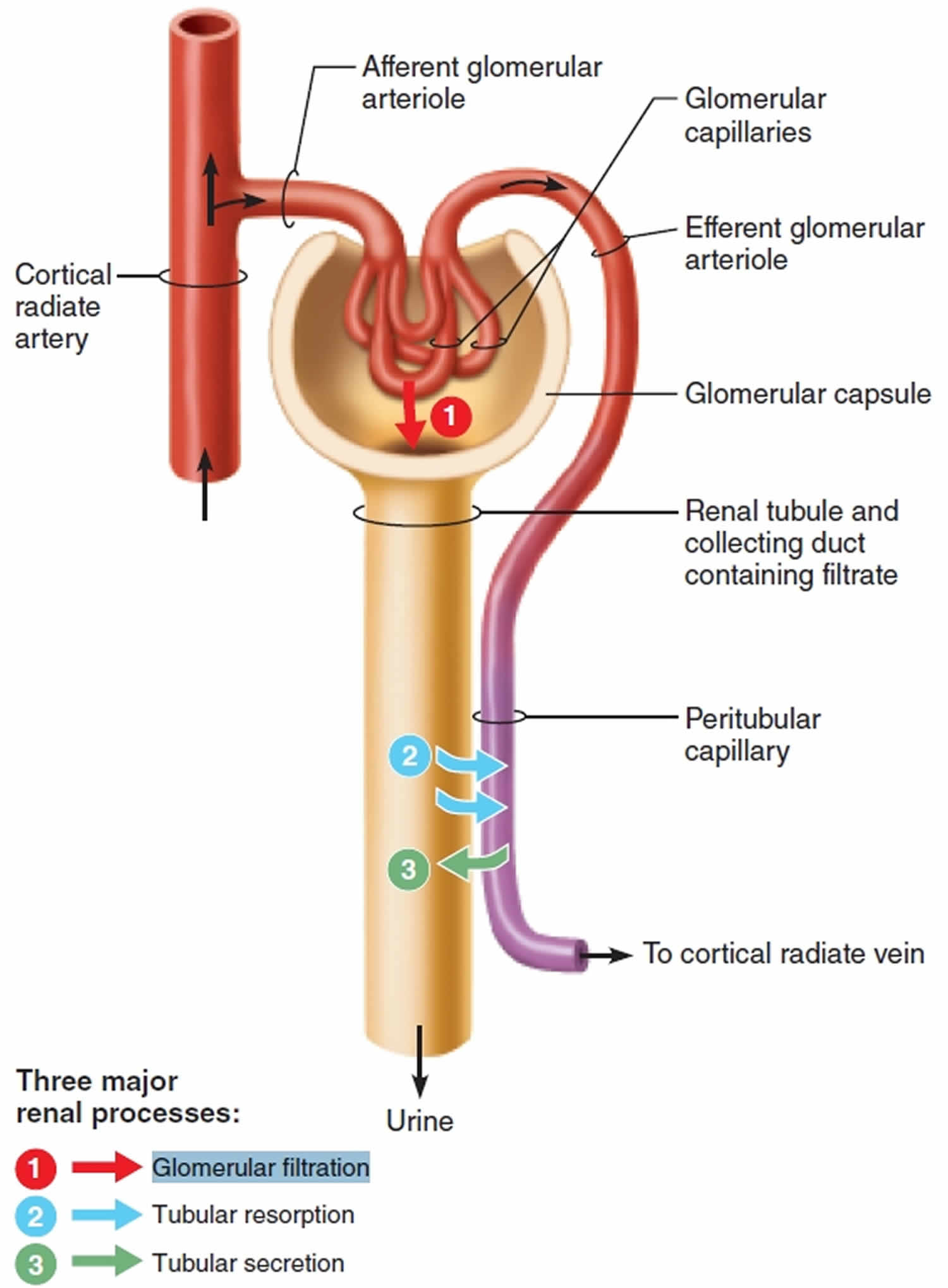
Glomeruli are tiny filters in the kidneys that allow waste products to be removed from the blood, while preventing the loss of important constituents, including proteins and blood cells. Glomerular filtration is the first step of urine production, where water and most solutes in blood plasma move across the wall of glomerular capillaries, where they are filtered and move into the glomerular capsule and then into the renal tubule. To produce urine, nephrons and collecting ducts perform three basic processes—glomerular filtration, tubular reabsorption, and tubular secretion (Figure 4). During glomerular filtration, water and solutes pass from blood plasma into the capsular space. The fluid that enters the capsular space is called the glomerular filtrate. The fraction of blood plasma in the afferent arterioles of the kidneys that becomes glomerular filtrate is the filtration fraction. Although a filtration fraction of 0.16–0.20 (16–20%) is typical, the value varies considerably in both health and disease. On average, the daily volume of glomerular filtrate in adults is 150 liters in females and 180 liters in males. More than 99% of the glomerular filtrate returns to the bloodstream via tubular reabsorption, so only 1–2 liters about 1–2 qt) is excreted as urine.
The glomerular filtration rate (GFR) refers to the amount of blood that is filtered by the glomeruli per minute. As a person’s kidney function declines due to damage or disease, the filtration rate decreases and waste products begin to accumulate in the blood. The normal level of glomerular filtration rate (GFR) varies according to age, sex, and body size. Normal glomerular filtration rate (GFR) in young adults is approximately 120 to 130 mL/min per 1.73 m² and declines with age 1. In adults, the GFR averages 125 mL/min in males and 105 mL/min in females. Homeostasis of body fluids requires that the kidneys maintain a relatively constant glomerular filtration rate (GFR). If the glomerular filtration rate (GFR) is too high, needed substances may pass so quickly through the renal tubules that some are not reabsorbed and are lost in the urine. If the glomerular filtration rate (GFR) is too low, nearly all the filtrate may be reabsorbed and certain waste products may not be adequately excreted.
The glomerular filtration rate (GFR) is the best test to measure your level of kidney function and determine your stage of kidney disease. Your doctor can calculate it from the results of your blood creatinine test, your age, body size and gender. Your glomerular filtration rate (GFR) tells your doctor your stage of kidney disease and helps the doctor plan your treatment. If your glomerular filtration rate (GFR) number is low, your kidneys are not working as well as they should. The earlier kidney disease is detected, the better the chance of slowing or stopping its progression.
Two tests are used routinely to check for kidney disease:
- A blood test checks your GFR (glomerular filtration rate), which tells how well your kidneys are filtering.
- A urine test checks for albumin in your urine, a sign of kidney damage.
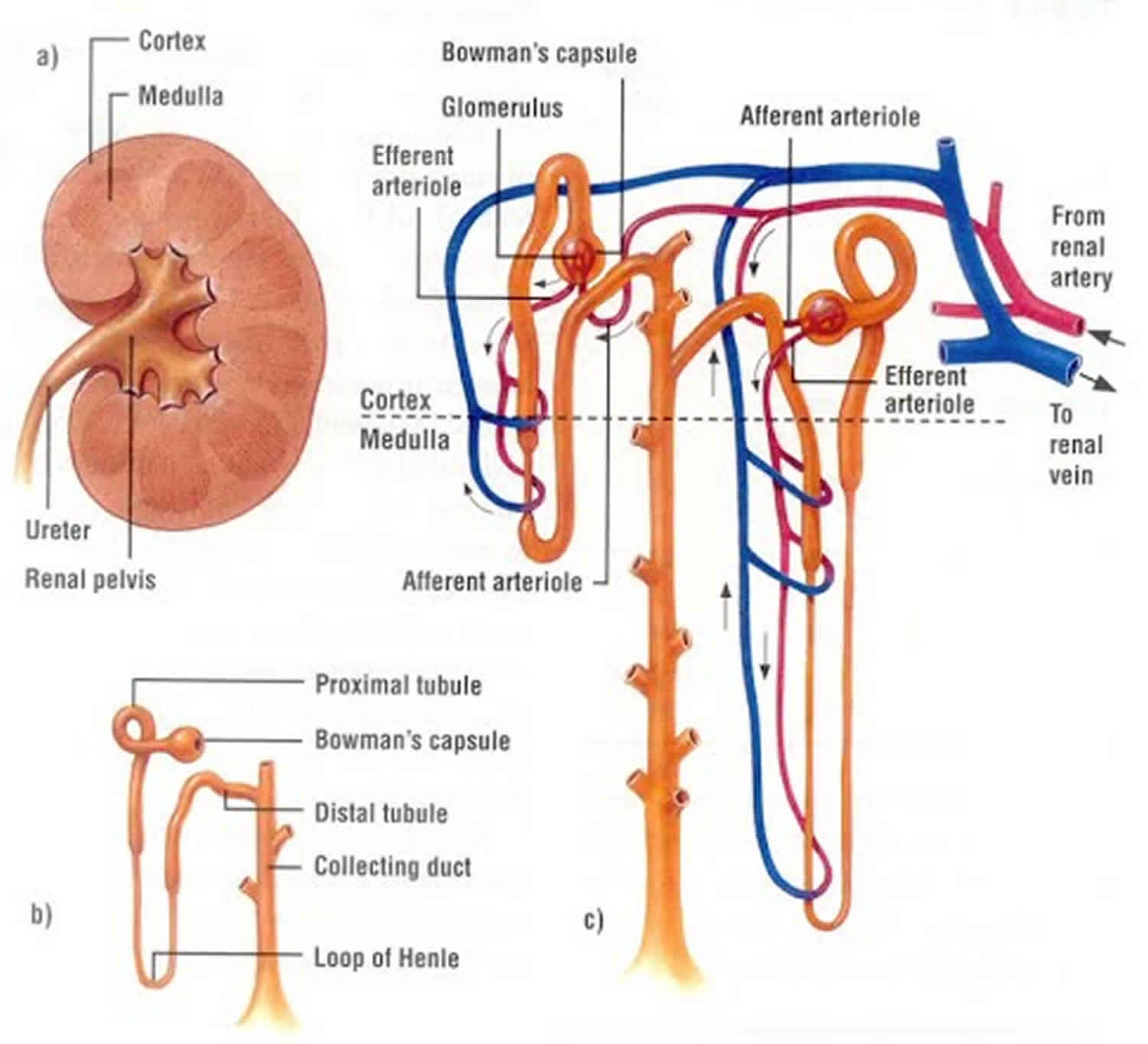
Figure 1. Kidney anatomy
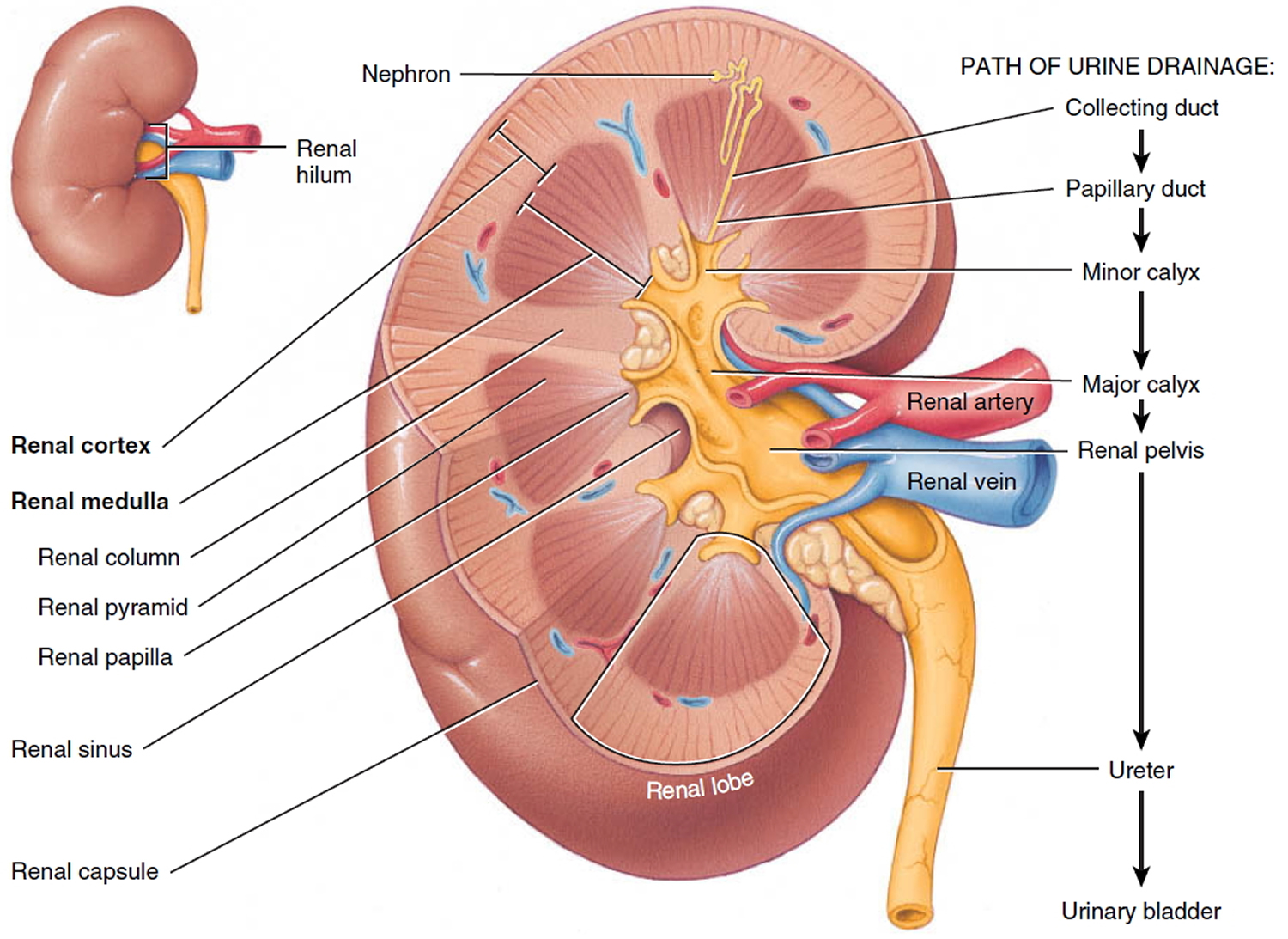
Figure 2. Kidney structure
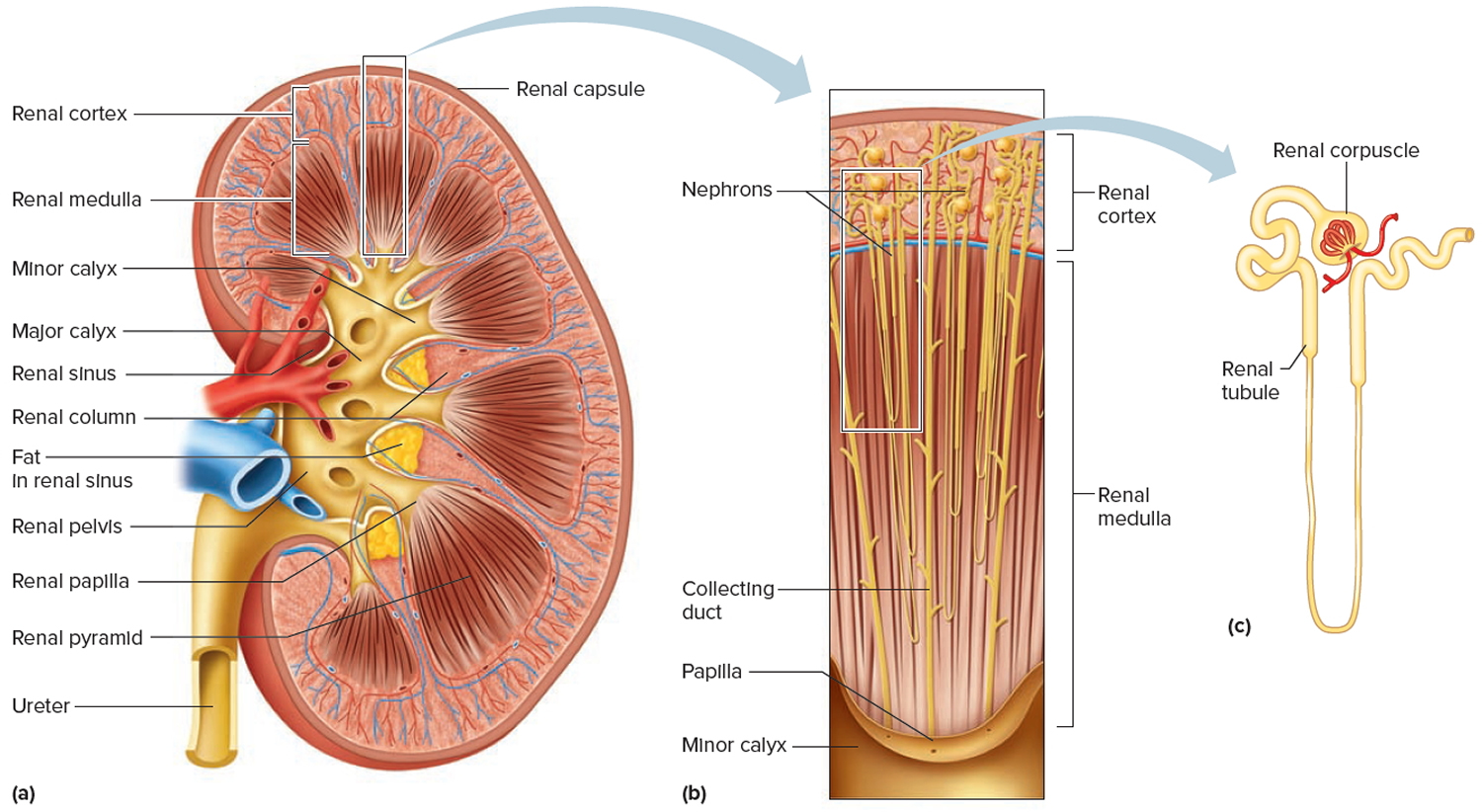
Figure 3. Microcirculation of the kidney
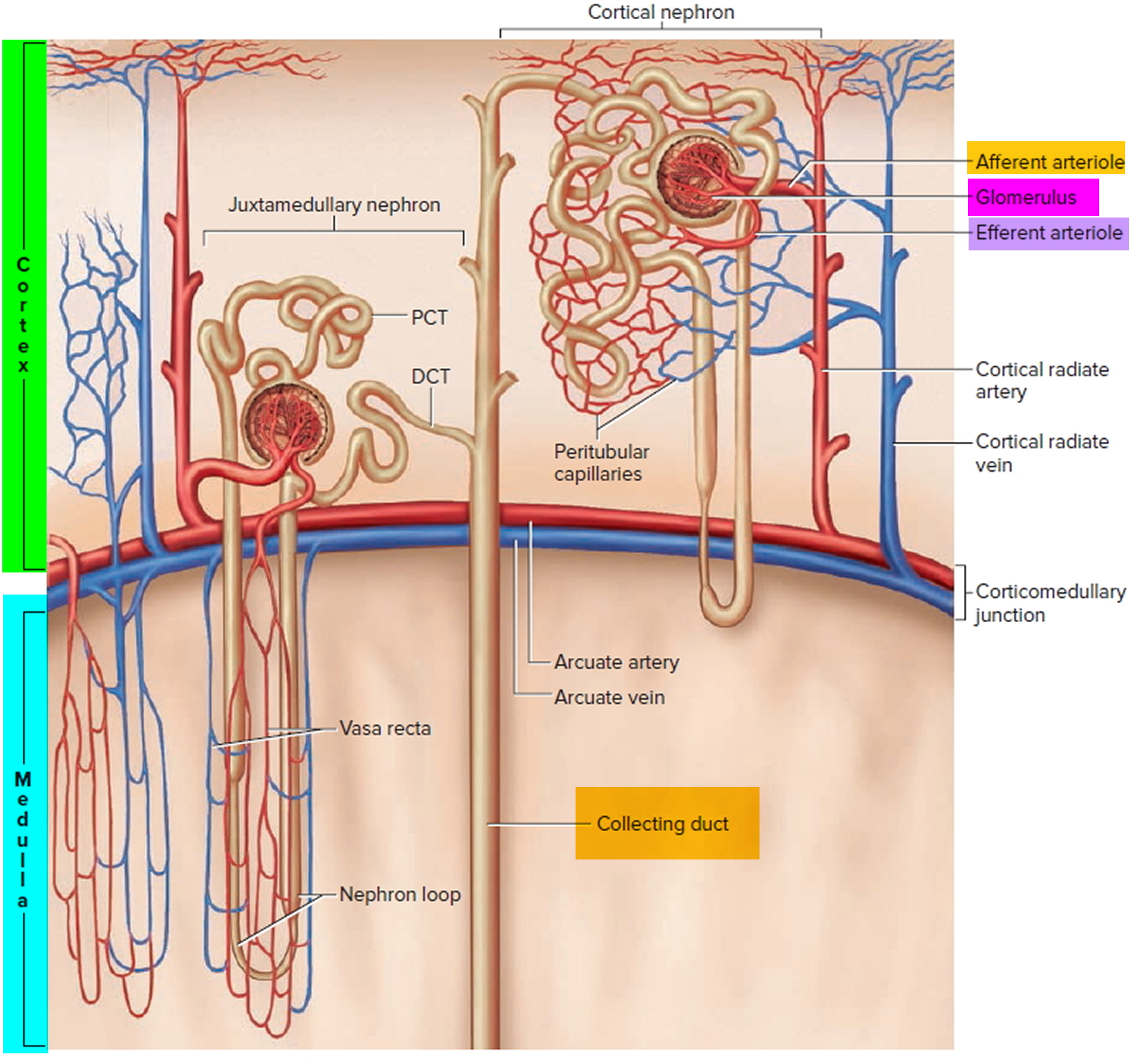
Note: DCT = distal convoluted tubule; PCT = proximal convoluted tubule
Where does glomerular filtration occur?
- Glomerular filtration. In the first step of urine production, water and most solutes in blood plasma move across the wall of glomerular capillaries, where they are filtered and move into the glomerular capsule and then into the renal tubule.
- Tubular reabsorption. As filtered fluid flows through the renal tubules and through the collecting ducts, tubule cells reabsorb about 99% of the filtered water and many useful solutes. The water and solutes return to the blood as it flows through the peritubular capillaries and vasa recta. Note that the term reabsorption refers to the return of substances to the bloodstream. The term absorption, by contrast, means entry of new substances into the body, as occurs in the gastrointestinal tract.
- Tubular secretion. As filtered fluid flows through the renal tubules and collecting ducts, the renal tubule and duct cells secrete other materials, such as wastes, drugs, and excess ions, into the fluid. Notice that tubular secretion removes a substance from the blood. Solutes and the fluid that drain into the minor and major calyces and renal pelvis constitute urine and are excreted. The rate of urinary excretion of any solute is equal to its rate of glomerular filtration, plus its rate of secretion, minus its rate of reabsorption.
By filtering, reabsorbing, and secreting, nephrons help maintain homeostasis of the blood’s volume and composition. The situation is somewhat analogous to a recycling center: Garbage trucks dump garbage into an input hopper, where the smaller garbage passes onto a conveyor belt (glomerular filtration of plasma). As the conveyor belt carries the garbage along, workers remove useful items, such as aluminum cans, plastics, and glass containers (reabsorption). Other workers place additional garbage left at the center and larger items onto the conveyor belt (secretion). At the end of the belt, all remaining garbage falls into a truck for transport to the landfill (excretion of wastes in urine).
Figure 4. Glomerular filtration process
Glomerular filtration membrane
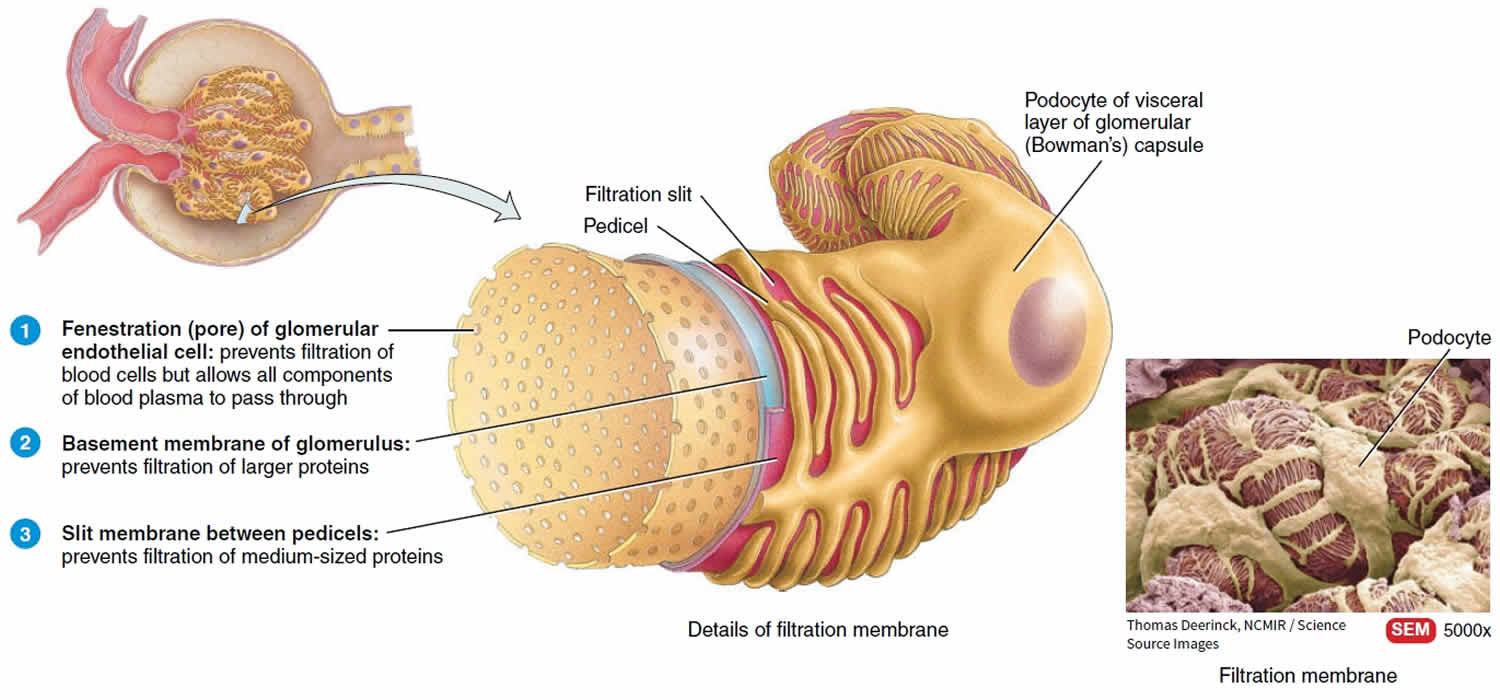
Together, the glomerular capillaries and the podocytes, which completely encircle the capillaries, form a leaky barrier known as the filtration (endothelial–capsular) membrane (Figure 5). This sandwich like assembly permits filtration of water and small solutes but prevents filtration of most plasma proteins and blood cells. Substances filtered from the blood cross three filtration barriers—a glomerular endothelial cell, the basement membrane, and a filtration slit formed by a podocyte (Figure 5):
- Glomerular endothelial cells are quite leaky because they have large fenestrations (pores) that measure 0.07–0.1 𝜇m in diameter. This size permits all solutes in blood plasma to exit glomerular capillaries but prevents filtration of blood cells. Located among the glomerular capillaries and in the cleft between afferent and efferent arterioles are mesangial cells (mes- = in the middle; -angi- = blood vessel). These contractile cells help regulate glomerular filtration.
- The basement membrane, a layer of acellular material between the endothelium and the podocytes, consists of minute collagen fibers and negatively charged glycoproteins. The pores within the basement membrane allow water and most small solutes to pass through. However, the negative charges of the glycoproteins repel plasma proteins, most of which are anionic; the repulsion hinders filtration of these proteins.
- Extending from each podocyte are thousands of footlike processes termed pedicels (little feet) that wrap around glomerular capillaries. The spaces between pedicels are the filtration slits. A thin membrane, the slit membrane, extends across each filtration slit; it permits the passage of molecules having a diameter smaller than 0.006–0.007 𝜇m, including water, glucose, vitamins, amino acids, very small plasma proteins, ammonia, urea, and ions. Less than 1% of albumin, the most plentiful plasma protein, passes the slit membrane because, with a diameter of 0.007 𝜇m, it is slightly too big to get through.
Figure 5. Glomerular filtration membrane
Glomerular Filtration Pressure
The principle of filtration—the use of pressure to force fluids and solutes through a membrane—is the same in glomerular filtration with glomerular capillaries as in blood capillaries elsewhere in the body. However, the volume of fluid filtered by the renal corpuscle is much larger than in other blood capillaries of the body for three reasons:
- Glomerular capillaries present a large surface area for filtration because they are long and extensive. Mesangial cells (mes- = in the middle; -angi- = blood vessel) regulate how much surface area is available. When mesangial cells are relaxed, surface area is maximal, and glomerular filtration is very high. Contraction of mesangial cells reduces the available surface area, and glomerular filtration decreases.
- The glomerular filtration membrane is thin and porous (see Figure 5). Despite having several layers, the thickness of the filtration membrane is only 0.1 mm. Glomerular capillaries also are about 50 times leakier than blood capillaries in most other tissues, mainly because of their large fenestrations (pores).
- Glomerular capillary blood pressure is high. Because the efferent arteriole is smaller in diameter than the afferent arteriole, resistance to the outflow of blood from the glomerulus is high. As a result, blood pressure in glomerular capillaries is considerably higher than in blood capillaries elsewhere in the body.
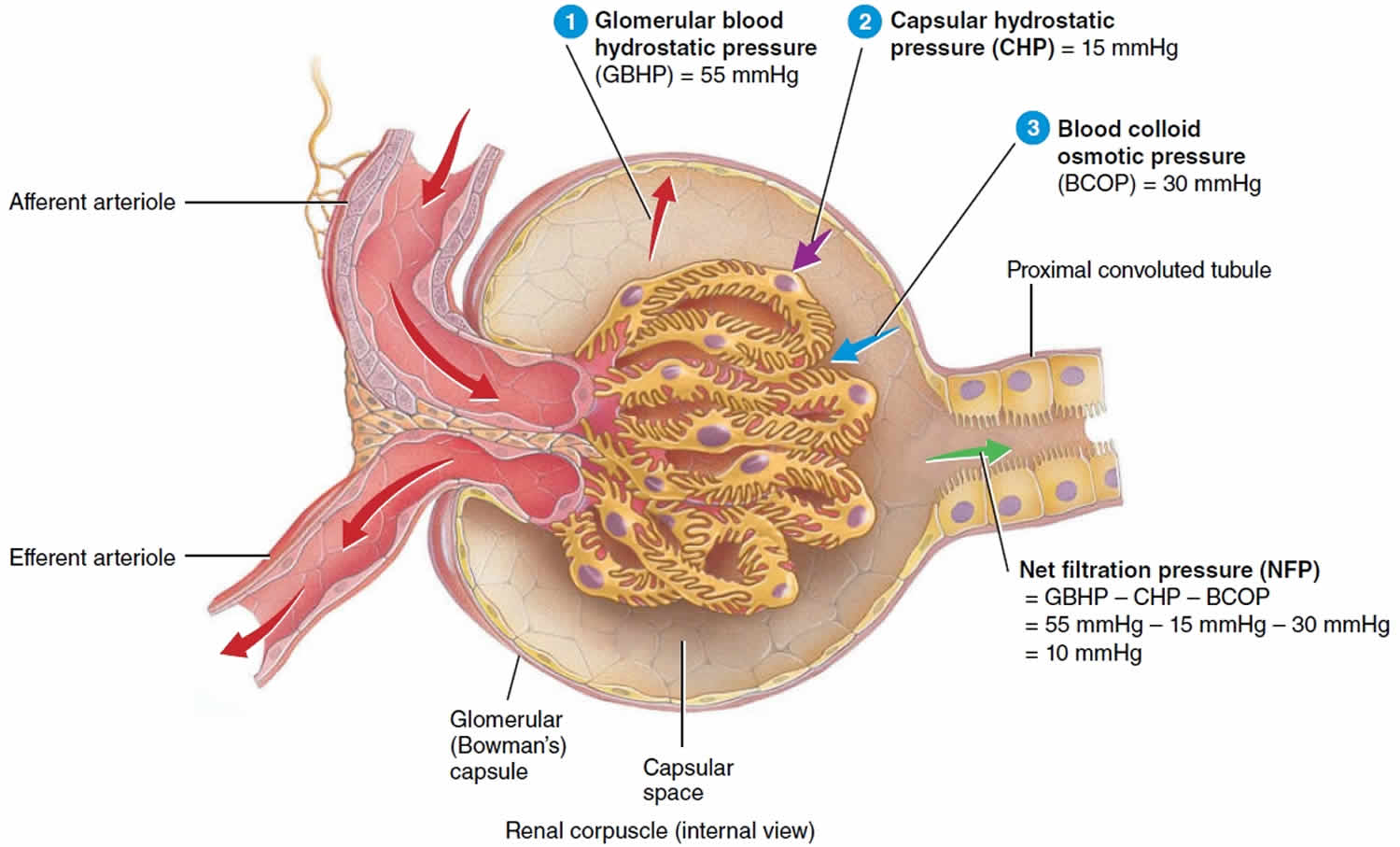
Glomerular filtration depends on three main pressures. One pressure promotes filtration and two pressures oppose filtration (Figure 6).
Glomerular blood hydrostatic pressure promotes filtration, whereas capsular hydrostatic pressure and blood colloid osmotic pressure oppose filtration.
- Glomerular blood hydrostatic pressure (GBHP) is the blood pressure in glomerular capillaries. Generally, glomerular blood hydrostatic pressure (GBHP) is about 55 mmHg. It promotes filtration by forcing water and solutes in blood plasma through the filtration membrane.
- Capsular hydrostatic pressure (CHP) is the hydrostatic pressure exerted against the filtration membrane by fluid already in the capsular space and renal tubule. Capsular hydrostatic pressure (CHP) opposes filtration and represents a “back pressure” of about 15 mmHg.
- Blood colloid osmotic pressure (BCOP), which is due to the presence of proteins such as albumin, globulins, and fibrinogen in blood plasma, also opposes filtration. The average blood colloid osmotic pressure (BCOP) in glomerular capillaries is 30 mmHg.
Net filtration pressure (NFP), the total pressure that promotes filtration, is determined as follows:
Net filtration pressure (NFP) = glomerular blood hydrostatic pressure (GBHP) − capsular hydrostatic pressure (CHP) − blood colloid osmotic pressure (BCOP)
By substituting the values just given, normal net filtration pressure (NFP) may be calculated:
Net filtration pressure (NFP) = 55 mmHg − 15 mmHg −30 mmHg = 10 mmHg
- Thus, a pressure of only 10 mmHg causes a normal amount of blood plasma (minus plasma proteins) to filter from the glomerulus into the capsular space.
Figure 6. Glomerular filtration pressure
What is glomerular filtration rate
Glomerular filtration rate (GFR) is the best test to measure your level of kidney function and determine your stage of kidney disease. Glomerular filtration rate (GFR) test measures the level of creatinine in the blood and uses the result in a formula to calculate a number that reflects how well the kidneys are functioning, called the estimated GFR or eGFR. Your doctor can calculate it from the results of your blood creatinine test, your age, body size and gender. Your glomerular filtration rate tells your doctor your stage of kidney disease and helps the doctor plan your treatment. If your glomerular filtration rate number is low, your kidneys are not working as well as they should. The earlier kidney disease is detected, the better the chance of slowing or stopping its progression.
Glomerular filtration rate (GFR) is approximately 120 ml per min (180 L per day). Average urine output, on the other hand, averages only about 1.5 L daily. Glomerular filtration rate (GFR) represents the flow of plasma from the glomerulus into Bowman’s space over a specified period and is the chief measure of kidney function 2. The kidneys receive 20% to 25% of the cardiac output (about 1.0 to 1.1 liters per minute) with the blood entering individual glomerular tufts via the afferent arteriole and exiting through the efferent arteriole. Of this renal blood flow, only the plasma can cross the structures comprising the glomerulus. Thus, the renal plasma flow (RPF) is a more accurate expression and is calculated as follows: renal blood flow x (1-hematocrit). The renal plasma flow (RPF) is approximately 600 to 720 ml per minute. Within the plasma, organic and inorganic solutes are freely filtered- meaning that they can be found in the ultrafiltrate (the fluid in Bowman’s space) and plasma at the same concentrations.
Glomerular filtration rate (GFR) is directly related to the pressures that determine net filtration pressure; any change in net filtration pressure will affect glomerular filtration rate. Severe blood loss, for example, reduces mean arterial blood pressure and decreases the glomerular blood hydrostatic pressure. Filtration ceases if glomerular blood hydrostatic pressure drops to 45 mmHg because the opposing pressures add up to 45 mmHg. Amazingly, when systemic blood pressure rises above normal, net filtration pressure (NFP) and glomerular filtration rate increase very little. Glomerular filtration rate is nearly constant
when the mean arterial blood pressure is anywhere between 80 and 180 mmHg.
The mechanisms that regulate glomerular filtration rate operate in two main ways:
- By adjusting blood flow into and out of the glomerulus and
- By altering the glomerular capillary surface area available for filtration.
Glomerular filtration rate (GFR) increases when blood flow into the glomerular capillaries increases. Coordinated control of the diameter of both afferent and efferent arterioles regulates glomerular blood flow. Constriction of the afferent arteriole decreases blood flow into the glomerulus; dilation of the afferent arteriole increases it. Three mechanisms control glomerular filtration rate: renal autoregulation, neural regulation, and hormonal regulation.
Chronic kidney disease (CKD) is associated with a decrease in kidney function that is often progressive. Chronic kidney disease can be seen with a variety of conditions, including diabetes and high blood pressure. Early detection of kidney dysfunction can help to minimize the damage. This is important as symptoms of kidney disease may not be noticeable until as much as 30-40% of kidney function is lost.
Measuring glomerular filtration rate directly is considered the most accurate way to detect changes in kidney status, but measuring the glomerular filtration rate (GFR) directly is complicated, requires experienced personnel, and is typically performed only in research settings and transplant centers. Because of this, the estimated GFR (eGFR) is usually used.
Glomerular filtration rate (GFR) is the rate in milliliters per minutes at which substances in plasma are filtered through the glomerulus, in other words, the clearance of a substance from the blood. The characteristics of an ideal marker of glomerular filtration rate are as follows:
- It should appear endogenously in the plasma at a constant rate
- It should be freely filtered at the glomerulus
- It can be neither reabsorbed nor secreted by the renal tubule
- It should not undergo extrarenal elimination.
As no such endogenous marker currently exists, exogenous markers of glomerular filtration rate are used.
The best method for directly determining the glomerular filtration rate (GFR) is a procedure called an “inulin clearance.” It involves introducing a fluid containing the marker molecule inulin, a polysaccharide (NOT insulin) into your veins (IV – intravenous infusion) and then collecting timed urines over a period of hours 3. The urine volumes are noted and the inulin in each sample is measured to allow determination of the glomerular filtration rate (GFR). Other exogenous markers used are radioisotopes such as chromium-51 ethylene-diamine-tetra-acetic acid (51 Cr-EDTA), and technetium-99-labeled diethylene-triamine-pentaacetate (99 Tc-DTPA). The most promising exogenous marker is the non-radioactive contrast agent, iohexol, especially in children. The inulin clearance test and other methods of determining GFR, such as those that use radioactive markers, are not routinely ordered and are primarily performed in research settings.
The inconvenience associated with the use of exogenous markers, specifically that testing has to be performed in specialized centers, and the difficulty to assay these substances, has encouraged the use of endogenous markers.
Creatinine
The most commonly used endogenous marker for assessment of glomerular function is creatinine. The calculated clearance of creatinine is used to provide an indicator of glomerular filtration rate. This involves the collection of urine over a 24-hour period or preferably over an accurately timed period of 5 to 8 hours since 24-hour collections are notoriously unreliable. Creatinine clearance is then calculated using the equation:
- C = (U x V) / P
C = Creatinine clearance, U = urinary concentration, V = urinary flow rate (volume/time i.e., ml/min), and P = plasma concentration
Creatinine clearance should be corrected for body surface area. Improper or incomplete urine collection is one of the major issues affecting the accuracy of this test, hence timed collection is advantageous. Furthermore, due to tubular secretion, creatinine overestimates glomerular filtration rate by around 10% to 20%.
Creatinine is the by-product of creatine phosphate in muscle, and it is produced at a constant rate by the body. For the most part, creatinine is cleared from the blood entirely by the kidney. Decreased clearance by kidney results in an increased blood creatinine. The amount of creatinine produced per day depends on muscle bulk, and thus, there is a difference in creatinine ranges between males and females with lower creatinine values in children and those with decreased muscle bulk. Diet also influences creatinine values. Creatinine can change as much as 30% after ingestion of red meat. As glomerular filtration rate increases in pregnancy lower creatinine values are found in pregnancy. Additionally, serum creatinine is a later indicator of renal impairment-renal function is decreased by 50% before a rise in serum creatinine is observed.
Serum creatinine is also utilized in glomerular filtration rate estimating equations such as the Modified Diet in Renal Disease (MDRD) and the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation. These eglomerular filtration rate equations are superior to serum creatinine alone since they include race, age, and gender variables. glomerular filtration rate is classified into the following stages based on the kidney disease.
Glomerular filtration rate formula
The estimated GFR (eGFR) is a calculation based on a serum creatinine test. Creatinine is a muscle waste product that is filtered from the blood by the kidneys and released into the urine at a relatively steady rate. When kidney function decreases, less creatinine is eliminated and concentrations increase in the blood. With the creatinine test, a reasonable estimate of the actual GFR can be determined.
Different equations may be used to calculate estimated GFR (eGFR). The following two are most common and require a person’s blood creatinine result, age, and assigned values based upon sex and race.
- Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) creatinine equation (2009)—recommended by the National Kidney Foundation for calculating eGFR in adults
- Modification of Diet in Renal Disease Study (MDRD) equation—some laboratories continue to use this equation
The results reported using one equation versus the other will not be identical but should give a healthcare practitioner similar information.
A different set of CKD-EPI calculators was published in 2012. These equations use the result of a cystatin C test. There is also a modified equation for people 18 and under that takes the blood urea nitrogen (BUN) level into consideration along with the factors listed above.
The National Kidney Foundation recommends using the CKD-EPI Creatinine Equation (2009) to estimate glomerular filtration rate (GFR):
CKD-EPI Creatinine Equation (2009) 4
Expressed as a single equation:
eGFR = 141 x min(SCr/κ, 1)α X max(SCr /κ, 1)-1.209 X 0.993Age X 1.018 [if female] X 1.159 [if Black]
Abbreviations / Units
- eGFR (estimated glomerular filtration rate) = mL/min/1.73 m²
- SCr (standardized serum creatinine) = mg/dL
- κ = 0.7 (females) or 0.9 (males)
- α = -0.329 (females) or -0.411 (males)
- min = indicates the minimum of SCr/κ or 1
- max = indicates the maximum of SCr/κ or 1
- age = years
If you have had a recent creatinine or cystatin C measurement, you can calculate the eGFR by using one of the calculators for people 19 years of age or older on the National Kidney Foundation (NKF) web site.
An online adult GFR calculator is available here (https://www.kidney.org/professionals/KDOQI/gfr_calculator)
For children and teens younger than 19 the online children GFR calculator is available here (https://www.kidney.org/professionals/KDOQI/gfr_calculatorPed)
Clinical Use
- Recommended method for estimating GFR in adults.
- Designed for use with laboratory creatinine values that are standardized to IDMS.
- Estimates GFR from serum creatinine, age, sex, and race.
- More accurate than the MDRD Study equation, particularly in people with higher levels of GFR.
- Based on the same four variables as the MDRD Study equation, but uses a 2-slope “spline” to model the relationship between estimated GFR and serum creatinine, and a different relationship for age, sex and race.
- Some clinical laboratories are still reporting GFR estimates using the Modification of Diet in Renal Disease Study (MDRD) Study equation. The National Kidney Foundation has recommended that clinical laboratories should begin using the CKD-EPI equation to report estimated GFR in adults.
- Developed in 2009 by the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI).
Why are factors such as age, sex, and race used in eGFR calculations?
This is because these factors are known to affect the level of creatinine in the blood. Creatinine is a waste product produced by muscles from the breakdown of a compound called creatine. According to the National Kidney Foundation, men tend to have more muscle mass than women so their creatinine levels tend to be higher. African Americans have a higher average muscle mass and generate more creatinine. As you age, you lose muscle mass and thus have lower blood creatinine levels for the same kidney function the older you get.
Besides measuring blood creatinine, are there other ways of estimating GFR?
Yes, a set of new Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) calculators was published in 2012 5. One uses the measure of a substance called cystatin C instead of creatinine to calculate eGFR while the other uses measures of both blood creatinine and cystatin C to estimate GFR. Cystatin C is a relatively small protein that is produced throughout the body by all cells that contain a nucleus and is found in a variety of body fluids, including the blood. It is produced, filtered from the blood by the kidneys, and broken down at a constant rate. Unlike creatinine, cystatin C is not significantly affected by muscle mass.
CKD-EPI Creatinine-Cystatin Equation 2012 5:
eGFR = 135 × min(SCr/κ, 1)α X max(SCr/κ, 1)-0.601 X min(Scys/0.8, 1)-0.375 X max(Scys/0.8, 1)-0.711 X 0.995Age X 0.969 [if female] X 1.08 [if black]
Abbreviations / Units
- eGFR (estimated glomerular filtration rate) = mL/min/1.73 m2
- SCr (serum creatinine) = mg/dL
- Scys (standardized serum cystatin C) = mg/l
- κ = 0.7 (females) or 0.9 (males)
- α = -0.248 (females) or -0.207 (males)
- min(SCr/κ or 1) = indicates the minimum of SCr/κ or 1
- max(SCr/κ or 1) = indicates the maximum of SCr/κ or 1
- min(Scys/0.8, 1) = indicates the minimum of Scys/0.8, 1
- max(Scys/0.8, 1) = indicates the maximum of Scys/0.8, 1
- age = years
According to the National Kidney Foundation, the newer CKD-EPI equations may be useful for assessing kidney function in people who have differences in diet, such as vegans, very high or very low muscle mass (e.g., body builders or those with muscle-wasting diseases), or for those who have changing muscle mass. They also may be useful for identifying people diagnosed with chronic kidney disease who have the highest risk of complications.
How is estimated GFR (eGFR) used?
The estimated glomerular filtration rate (eGFR) is used to screen for and detect early kidney damage, to help diagnose chronic kidney disease (CKD), and to monitor kidney status. It is a calculation based on the results of a blood creatinine test along with other variables such as age, sex, and race (e.g., African-American, non-African American), depending on the equation used.
The National Kidney Disease Education Program, American Society of Nephrology, and the National Kidney Foundation all recommend that an estimated glomerular filtration rate (eGFR) be calculated every time a creatinine blood test is done. The creatinine test is ordered frequently as part of a routine comprehensive metabolic panel (CMP) or basic metabolic panel (BMP), or along with a blood urea nitrogen (BUN) test to evaluate the status of a person’s kidneys.
Creatinine, along with estimated glomerular filtration rate (eGFR), is often used to monitor people with known chronic kidney disease (CKD) and those with conditions such as diabetes and high blood pressure (hypertension) that may lead to kidney damage.
Other tests that may be done at the same time to help detect kidney damage and/or evaluate kidney function are:
- Urine albumin (microalbumin) and albumin/creatinine ratio (ACR)—used to screen people with chronic conditions, such as diabetes and hypertension, that put them at an increased risk of developing kidney disease; increased levels of albumin in the urine may indicate kidney damage.
- Urinalysis—may be used to help detect signs of kidney damage, such as the presence of blood or casts in the urine
When is estimated glomerular filtration rate (eGFR) ordered?
A creatinine test and estimated glomerular filtration rate (eGFR) may be ordered when a healthcare practitioner wants to evaluate a person’s kidney function as part of a health checkup or if kidney disease is suspected. Signs and symptoms of kidney disease may include:
- Swelling or puffiness, particularly around the eyes or in the face, wrists, abdomen, thighs, or ankles
- Urine that is foamy, bloody, or coffee-colored
- A decrease in the amount of urine
- Problems urinating, such as a burning feeling or abnormal discharge during urination, or a change in the frequency of urination, especially at night
- Mid-back pain (flank), below the ribs, near where the kidneys are located
- High blood pressure (hypertension)
As kidney disease worsens, symptoms may include:
- Urinating more or less often
- Feeling itchy
- Tiredness, loss of concentration
- Loss of appetite, nausea and/or vomiting
- Swelling and/or numbness in hands and feet
- Darkened skin
- Muscle cramps
An estimated glomerular filtration rate (eGFR) may be repeated if the initial result is abnormal to see if it persists.
The test is usually ordered periodically when a person has a chronic kidney disease (CKD) or a condition such as diabetes or hypertension that is associated with an increased risk of kidney damage.
What does abnormal glomerular filtration rate mean?
Changes in GFR are used to define and diagnose several pathologies. Acute kidney injury (previously acute renal failure) is an abrupt increase in serum creatinine (generally over days) and is largely reversible. Alternatively, chronic kidney disease (CKD) is often irreversible damage and persistent over at least 3 months.
Estimated glomerular filtration rate (eGFR) results are reported as milliliters/minute/1.73 m² (mL/min/ 1.73 m²). Because some laboratories do not collect information on a patient’s race when the sample is collected for testing, they may report calculated results for both African Americans and non-African Americans. The healthcare practitioner uses the result that applies to the particular patient in order to interpret the results correctly.
A normal estimated glomerular filtration rate (eGFR) for adults is greater than 90 mL/min/1.73 m², according to the National Kidney Foundation. (Because the calculation works best for estimating reduced kidney function, actual numbers are only reported once values are less than 60 mL/min/1.73 m²).
An eGFR below 60 mL/min/1.73 m² suggests that some kidney damage has occurred. The test may be repeated to see if the abnormal result persists. Chronic kidney disease (CKD) is diagnosed when a person has an eGFR less than 60 mL/min/1.73 m² for more than three months.
A person may have some kidney damage even with an eGFR greater than 90 mL/min/1.73 m². Other evidence, such as increased urine albumin, may indicate some degree of kidney damage. Thus, a person’s estimated glomerular filtration rate (eGFR) should be interpreted in relation to the person’s clinical history and presenting conditions.
Chronic kidney disease is staged as follows:
The following table summarizes estimated GFR and the stages of kidney damage in chronic kidney disease (CKD)
| Kidney damage stage | description | estimated gfr (ML/MIN/1.73M2) | other findings |
|---|---|---|---|
| 1 | Normal or minimal kidney damage with normal GFR | 90+ | Protein or albumin in urine may be high, cells or casts rarely seen in urine |
| 2 | Mild decrease in GFR | 60-89 | Protein or albumin in urine may be high, cells or casts rarely seen in urine |
| 3a | Mildly to moderately decrease in GFR | 45-59 | |
| 3b | Moderately to severely decrease in GFR | 30-44 | |
| 4 | Severe decrease in GFR | 15-29 | |
| 5 | Kidney failure (end-stage renal disease) | <15 |
Many medications are eliminated renally and are therefore relevant to a discussion of kidney function, the mechanism of several of them directly affect GFR. NSAIDs and ACE inhibitors (or angiotensin receptor blockers) both decrease GFR by different mechanisms. NSAIDs inhibit prostaglandin synthesis. PGI2 and PGE2 normally dilate the afferent arteriole, so NSAIDs are afferent constrictors. Angiotensin II normally constricts the efferent arteriole, so ACE inhibitors (or angiotensin receptor blockers) dilate the afferent arteriole. Note that endogenously produced compounds (PGE2 and Angiotensin II) increase the GFR, and exogenous medications decrease the GFR (NSAIDS and ACEi or ARBs). This is why taking NSAIDs on ACEi (or ARB) is a relative contraindication, especially with other renally active drugs like diuretics.
Another method of evaluating kidney function and potentially estimating GFR
Another method of evaluating kidney function and potentially estimating GFR involves the measurement of the blood level of cystatin C. There is increasing interest in the use of this test for these purposes and several studies have been performed comparing calculations of eGFR using creatinine, cystatin C, or both. According to the National Kidney Foundation, two meta-analyses concluded that cystatin C is superior to creatinine as a marker of kidney function. The NKF also states that a formula for calculating eGFR that includes both blood creatinine and cystatin C values may improve that estimate (see below).
The creatinine clearance test also provides an estimate of kidney function and of the actual GFR. However, in addition to the serum creatinine, this test requires a timed urine collection (24 hours) for urine creatinine measurement in order to compare blood and urine creatinine concentrations and to calculate the clearance.
The actual amount of creatinine that a person produces and excretes is affected by their muscle mass and by the amount of protein in their diet. Men tend to have higher creatinine levels than women and children.
A person’s GFR decreases with age and some illnesses and usually increases during pregnancy.
A slightly different equation should be used to calculate the eGFR for those under the age of 18 (see below). The eGFR equations are not valid for those who are 70 years of age or older because muscle mass normally decreases with age.
An eGFR may not be as useful for those who differ from normal creatinine concentrations. This may include people who have significantly more muscle (such as a body builder) or less muscle (such as a muscle-wasting disease) than the norm, those who are extremely obese, malnourished, follow a strict vegetarian diet, ingest little protein, or who take creatine dietary supplements.
The eGFR may also be affected by a variety of drugs, such as gentamicin, cisplatin, and cefoxitin that increase creatinine levels, and by any condition that decreases blood flow to the kidneys.
The calculation for eGFR is intended to be used when kidney function and creatinine production are stable. If a creatinine level is measured when the kidney function is changing rapidly, such as with acute kidney failure, then it will not give a useful estimate of the filtration rate.
What other findings might suggest kidney dysfunction?
Diabetics and others at risk for developing kidney disease may be monitored for small amounts of albumin in their urine by performing a urine albumin test. The presence of albumin and other plasma proteins as well as blood in the urine can all be signs of potential kidney damage.
Identify cause of chronic kidney disease (CKD)
- Cause of chronic kidney disease (CKD) is classified based on presence or absence of systemic disease and the location within the kidney of observed or presumed pathologic-anatomic findings on kidney biopsy or imaging.
- Determining the cause of chronic kidney disease (CKD) distinguishes whether the patient has a systemic condition or a localized condition in the kidney such as glomerular disease because this functionality affects management.
- It is anticipated that the cause of disease will not be known with certainty for many patients with chronic kidney disease (CKD) but can be either inferred or not known.
| Examples of systemic diseases affecting the kidney | Examples of primary kidney diseases (absence of systemic diseases affecting the kidney) | |
|---|---|---|
| Glomerular diseases | Diabetes, systemic autoimmune diseases, systemic infections, drugs, neoplasia (including amyloidosis) | Diffuse, focal or crescentic proliferative glomerulonephritis; focal and segmental glomerulosclerosis; membranous nephropathy, minimal change disease |
| Tubulointerstitial diseases | Systemic infections, autoimmune, sarcoidoisis, drugs, urate, environmental toxins (lead, aristolochic acid), neoplasia (myeloma) | Urinary-tract infections, stones, obstruction |
| Vascular diseases | Atherosclerosis, hypertension, ischemia, cholesterol emboli, systemic vasculitis, thrombotic microangiopathy, systemic sclerosis | ANCA-associated renal limited vasculitis; fibromuscular dysplasia |
| Cystic and congenital diseases | Polycystic kidney disease, Alport’s syndrome, Fabry’s disease | Renal dysplasia, medullary cystic disease, podocytopathies |
| Genetic diseases are not considered separately because some diseases in each category are now recognized as having genetic determinants. | ||
- Lindeman RD, TobinJ, ShockNW. Longitudinal studies on the rate of decline in renal function with age, J Am Geriatr Soc, 1985, vol. 33, pg. 278-85
- Kaufman DP, Knohl SJ. Physiology, Glomerular Filtration Rate (GFR) [Updated 2018 Apr 19]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2018 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK500032
- Gounden V, Jialal I. Renal Function Tests. [Updated 2018 May 25]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2018 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK507821
- CKD-EPI Creatinine Equation 2009. https://www.kidney.org/content/ckd-epi-creatinine-equation-2009
- CKD-EPI Creatinine-Cystatin Equation 2012. https://www.kidney.org/content/ckd-epi-creatinine-cystatin-equation-2012





{kind=link}