
What is heart block
Heart block is a condition where your heart beats more slowly or with an abnormal rhythm. Heart block is a problem that occurs with your heart’s electrical system. Your heart’s electrical system controls the rate and rhythm of heartbeats. “Rate” refers to the number of times your heart beats per minute. “Rhythm” refers to the pattern of regular or irregular pulses produced as the heart beats.
With each heartbeat, an electrical signal spreads across the heart from the upper chambers (atria) to the lower chambers (ventricles). As the heart electrical signal travels, the signal causes the heart to contract and pump blood. In cases of heart block, the electrical signals that progress from the heart’s upper chambers (atria) to its lower chambers (ventricles) are impaired. When those signals don’t transmit properly, the heart beats irregularly.
Heart block occurs if the electrical signal is slowed or disrupted as it moves through the heart.
There are several degrees of heart block.
Heart block can be present from birth (congenital) or develop later in life (acquired). Babies are more likely to have congenital heart block if they’re born with a heart defect, or if their mother has an autoimmune condition, such as lupus.
Symptoms of heart block depend on which type of heart block you have. First-degree heart block, the least serious type, may not cause any noticeable symptoms.
Second-degree heart block sometimes causes troublesome symptoms that need treatment, and third-degree heart block (complete heart block) – the most serious type – can sometimes be a medical emergency.
Heart block normally only needs to be treated if it’s causing symptoms. Your heart may need to be stabilized using a method called transcutaneous pacing (TCP), where pads are attached to your chest and electrical pulses are delivered through them to help restore your heart rate to normal. This procedure can be uncomfortable, so you may be given a sedative. This medication will make you feel drowsy, so you have little or no awareness of what’s going on around you.
Once your heartbeat has been stabilized, a permanent pacemaker may need to be fitted. A pacemaker is a small battery-operated device inserted under the skin of your chest. It sends frequent electrical pulses to keep your heart beating regularly.
Treatment for heart block usually works well. Deaths caused by heart block are rare.
The heart’s electrical system
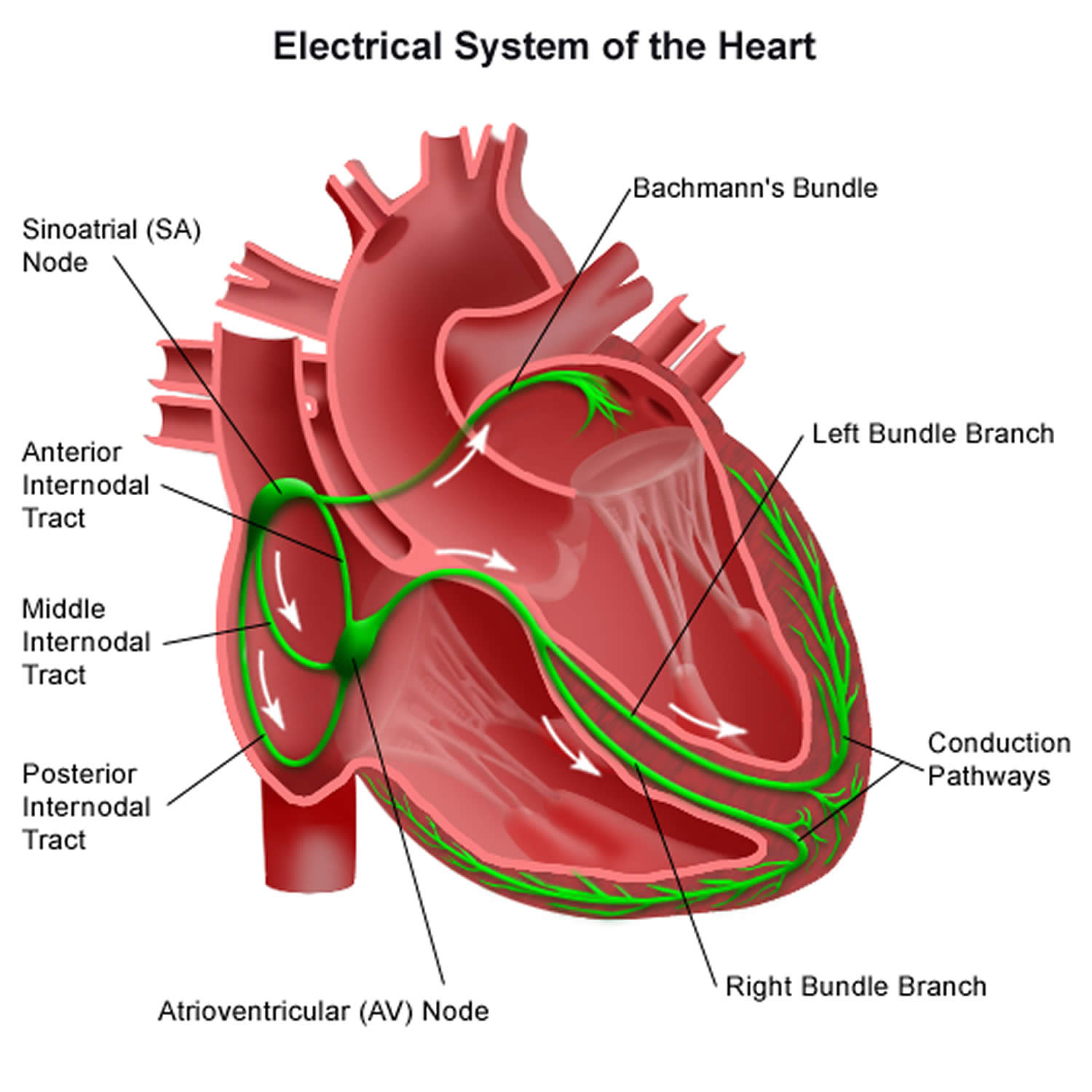
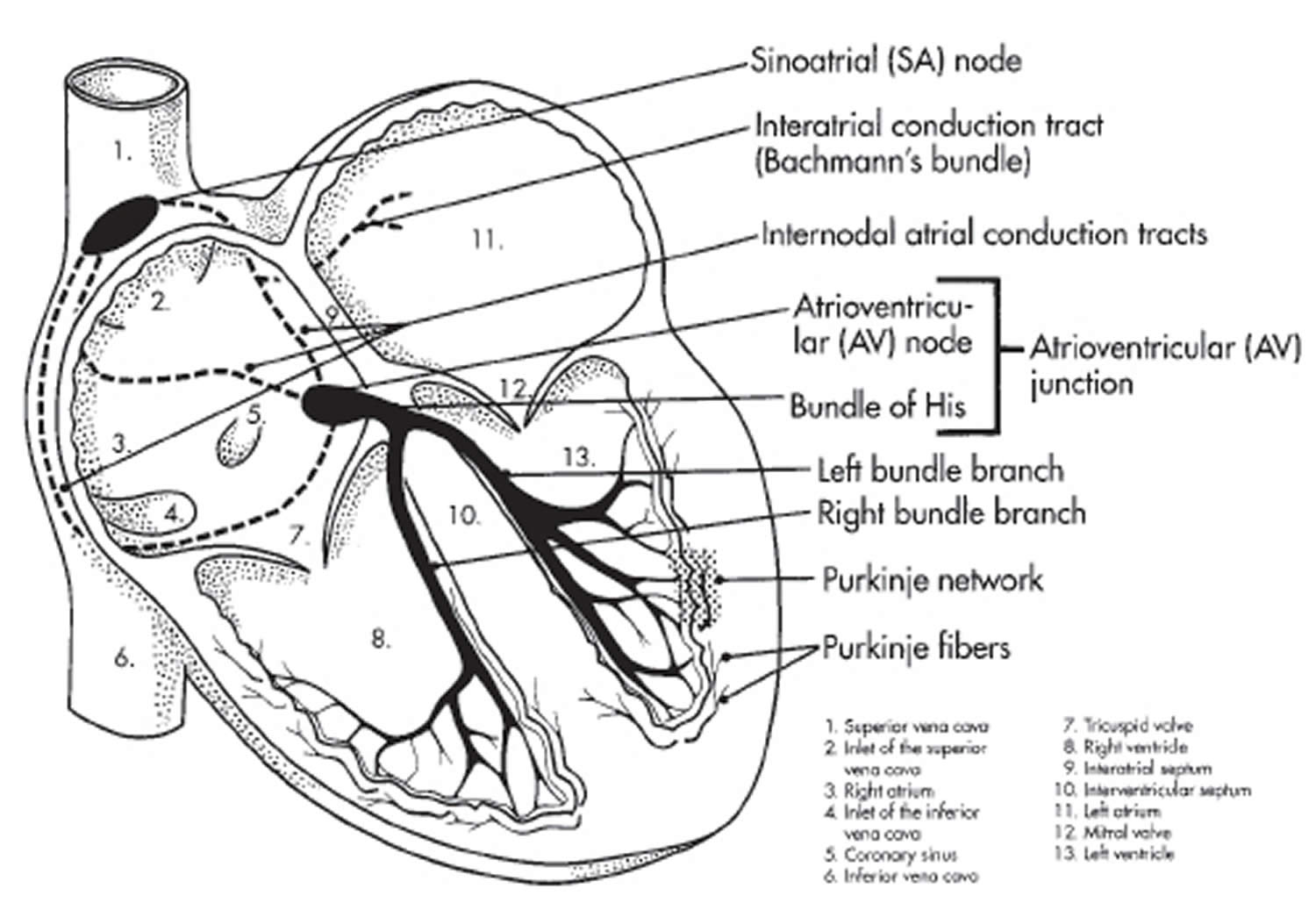
To understand arrhythmias, it helps to understand the heart’s internal electrical system. The heart’s electrical system controls the rate and rhythm of the heartbeat (see Figure 3).
Your heart’s electrical system is made up of three main parts:
- The sinoatrial (SA) node, located in the right atrium of your heart
- The atrioventricular (AV) node, located on the interatrial septum close to the tricuspid valve
- The His-Purkinje system, located along the walls of your heart’s ventricles
Each beat of your heart is set in motion by an electrical signal from within your heart muscle. The signal is generated as the vena cavae fill your heart’s right atrium with blood from other parts of your body. The signal spreads across the cells of your heart’s right and left atria. In a normal, healthy heart, each beat begins with a signal from the natural pacemaker called the sinoatrial (SA) node — or sinus node — an area of specialized cells in the right atrium. This is why the sinoatrial (SA) node sometimes is called your heart’s natural pacemaker. Your pulse, or heart rate, is the number of signals the SA node produces per minute. In a healthy adult heart at rest, the SA node sends an electrical signal to begin a new heartbeat 60 to 100 times a minute. (This rate may be slower in very fit athletes.)
The sinoatrial (SA) node produces electrical impulses that normally start each heartbeat. This natural pacemaker produces the electrical impulses that trigger the normal heartbeat. From the sinus node, electrical impulses travel across the atria to the ventricles, causing them to contract and pump blood to your lungs and body.
From the sinoatrial (SA) node, electrical impulses travel across the atria, causing the atrial muscles to contract and pump blood into the ventricles.
The electrical impulses then arrive at a cluster of cells called the atrioventricular (AV) node — usually the only pathway for signals to travel from the atria to the ventricles.
The atrioventricular (AV) node slows down the electrical signal before sending it to the ventricles. This slight delay allows the ventricles to fill with blood.
The signal is released and moves along a pathway called the bundle of His, which is located in the walls of your heart’s ventricles. From the bundle of His, the signal fibers divide into left and right bundle branches through the Purkinje fibers. These fibers connect directly to the cells in the walls of your heart’s left and right ventricles.
The signal spreads across the cells of your ventricle walls, and both ventricles contract. However, this doesn’t happen at exactly the same moment.
The left ventricle contracts an instant before the right ventricle. This pushes blood through the pulmonary valve (for the right ventricle) to your lungs, and through the aortic valve (for the left ventricle) to the rest of your body.
As the signal passes, the walls of the ventricles relax and await the next signal.
This process continues over and over as the atria refill with blood and more electrical signals come from the SA node.
When electrical impulses reach the muscles of the ventricles, they contract, causing them to pump blood either to the lungs or to the rest of your body.
When anything disrupts this complex system, it can cause the heart to beat too fast (tachycardia), too slow (bradycardia) or with an irregular rhythm.
Your heart’s electrical system controls all the events that occur when your heart pumps blood. The electrical system also is called the cardiac conduction system. If you’ve ever seen the heart test called an EKG (electrocardiogram), you’ve seen a graphical picture of the heart’s electrical activity.
Figure 1. The heart’s electrical system
Heart block causes
Some people are born with heart block – known as congenital heart block.
But more commonly, heart block develops later in life. This is known as acquired heart block and can be caused by:
- other heart conditions, such as a heart attack
- taking certain medicines
- other diseases, such as Lyme disease
- having heart surgery
Acquired heart block
Acquired heart block can affect people of any ages, but older people are more at risk.
There are several causes of acquired heart block, including:
- heart surgery – thought to be one of the most common causes of complete heart block
- being an athlete – some athletes get first-degree heart block because their hearts are often bigger than normal, which can slightly disrupt their heart’s electrical signals
- a history of coronary heart disease, heart attack or heart failure – this can leave the heart tissues damaged
- some diseases – such as myocarditis, cardiomyopathy, Lyme disease, sarcoidosis, Lev’s disease, diphtheria or rheumatic fever
- exposure to some toxic substances
- low levels of potassium (hypokalaemia) or low magnesium (hypomagnesemia) in the blood
- high blood pressure (hypertension) that isn’t well controlled
- cancer that’s spread from another part of the body to the heart
- a penetrating trauma to the chest – such as a stab wound or gunshot wound
Certain medications can also cause first-degree heart block, including:
- medication for abnormal heart rhythms – such as disopyramide
- medications for high blood pressure – such as beta blockers, calcium channel blockers, or clonidine
- digoxin – a medication used to treat heart failure
- fingolimod – used for treating certain types of multiple sclerosis
- pentamidine – used to treat some types of pneumonia
- tricyclic antidepressants – such as amitriptyline
Heart block types
There are three main types of heart block:
- AV (atrioventricular) heart blocks
- Bundle branch blocks
- Tachybrady syndrome
AV (atrioventricular) heart blocks
An AV heart block happens when the electrical impulses are delayed or blocked as they travel between your atria (the top chambers of your heart) and your ventricles (the bottom chambers of your heart).
There are three ‘degrees’ of AV heart block:
- First-degree heart block, which usually doesn’t cause symptoms or need treatment
- Second-degree heart block
- Third-degree (complete) heart block
AV heart block can be caused by coronary heart disease, congenital heart disease, cardiomyopathy, ageing of the electrical pathways in your heart, and some medicines. The type of treatment you’ll need will depend on the cause and symptoms. Some AV heart blocks may develop into higher degree AV heart blocks if they’re left untreated. Your doctor will be able to give you advice about this.
Some people always have AV heart block but in others the condition can come and go.
Bundle branch blocks
Bundle branch blocks happen when the electrical impulses travel through the bottom chambers of your heart (your ventricles) more slowly than normal because of a block in the electrical pathway. Bundle branch blocks will always cause symptoms and could be a sign of an underlying heart condition which you might need treatment for.
There are two types of bundle branch blocks:
Left bundle branch block
Left bundle branch block (LBBB) is usually caused by an underlying condition such as coronary heart disease, cardiomyopathy, thickening of the heart muscle (left ventricular hypertrophic cardiomyopathy) or ageing of the electrical pathway in your heart.
Right bundle branch blocks
Right bundle branch block (RBBB) can be caused by coronary heart disease, congenital heart disease, or some lung conditions. However it can also happen naturally in people with a normal heart and no heart problems.
Tachybrady syndrome
Tachybrady syndrome happens when your heart’s sinus node doesn’t work properly. Your sinus node (sometimes called your heart’s natural pacemaker) is responsible for telling your heart when to beat. If your sinus node doesn’t work properly, it can cause your heartbeat to become too fast or too slow, or switch between fast and slow rhythms. An example of this is when atrial flutter (a fast heart rhythm) alternates with a slow heart rhythm.
There might also be sudden pauses in the electrical activity in your heart, which could lead to you feeling dizzy, lightheaded, or sometimes collapsing.
The most likely cause of tachybrady syndrome is ageing of the electrical pathway in your heart but it can also be caused by coronary heart disease, for example after a heart attack, and some medicines. If you have tachybrady syndrome you might need a combination of medicines or have a pacemaker fitted.
First degree heart block
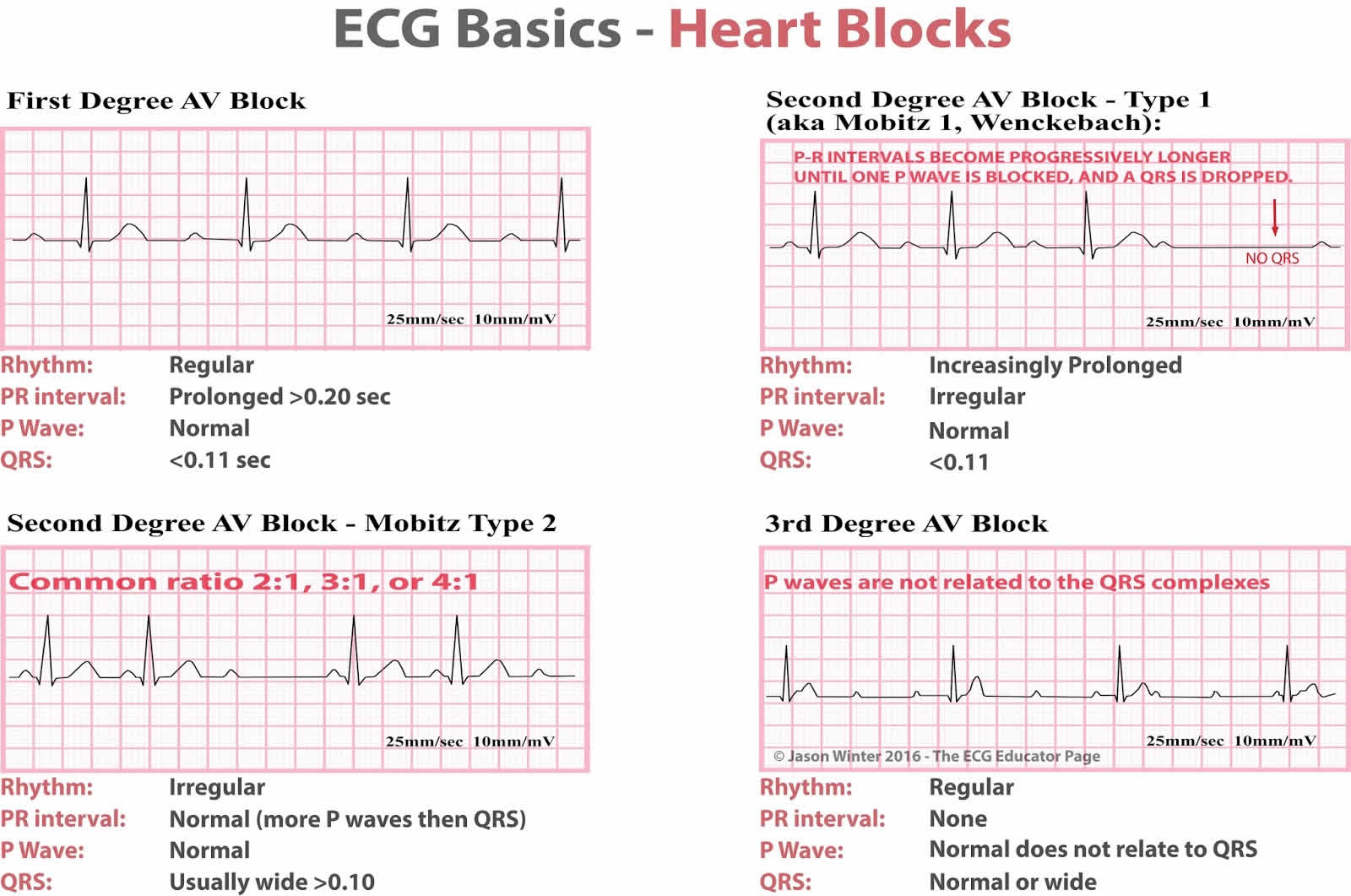
First-degree degree heart block or 1st degree atrioventricular (AV) block is defined as a PR interval of greater than 0.20 seconds on electrocardiography (ECG) without disruption of atrial to ventricular conduction (Figure 2) 1. First-degree degree heart block may cause dizziness or lightheadedness, or it may cause no symptoms at all and without significant complications. For the vast majority of patients, first-degree heart block may not require specific treatment beyond routine observation for worsening conduction delay. Regular evaluation is important, however, as affected patients have been shown to have an increased risk of developing atrial fibrillation (A Fib) or higher-degree atrioventricular (AV) block 2.
First-degree heart block occurs when the electrical impulse moves through the heart’s atrioventricular (AV) node more slowly than normal. This usually results in a slower heart rate.
Certain medications can cause first-degree heart block as a side effect:
- Digitalis: This medication is commonly used to slow down the heart rate. If it’s taken in high dosages or for a long period, digitalis can cause first-degree heart block.
- Beta blockers: These drugs inhibit the part of the nervous system that speeds up the heart. This can have the side effect of delaying electrical conduction within the heart, which can cause first-degree heart block.
- Calcium channel blockers: Among their other effects, calcium channel blockers can slow down the conduction within the heart’s AV node, resulting in first-degree heart block.
If you have first-degree heart block, it’s important to check in regularly with your doctor to monitor the condition. Between appointments with the doctor, you should take your pulse regularly and watch out for slower than normal heart rates.
Figure 2. 1st degree heart block
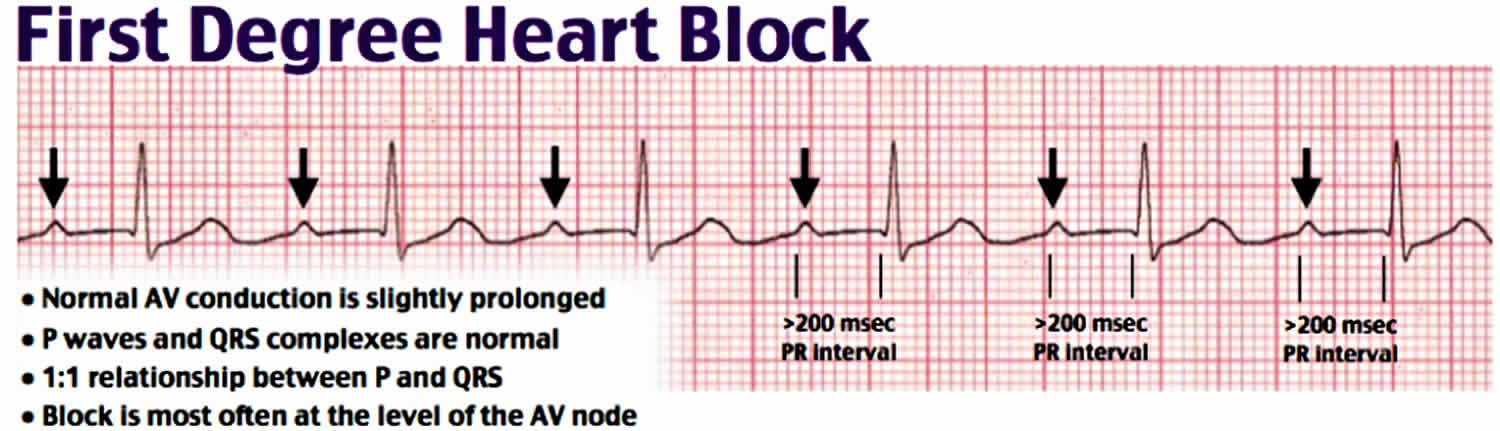
Footnote: EKG, cardiac complex noting a significantly prolonged PR interval (0.28 seconds) consistent with first degree heart block.
Second degree heart block
Second-degree heart block occurs when electrical signals from the heart’s upper chambers (atria) don’t reach the lower chambers (ventricles). This can result in “dropped beats.”
Symptoms of 2nd degree heart block include:
- Chest pain
- Fainting (syncope)
- Heart palpitations
- Breathing difficulties, such as shortness of breath (during exertion)
- Rapid breathing
- Nausea
- Excessive fatigue
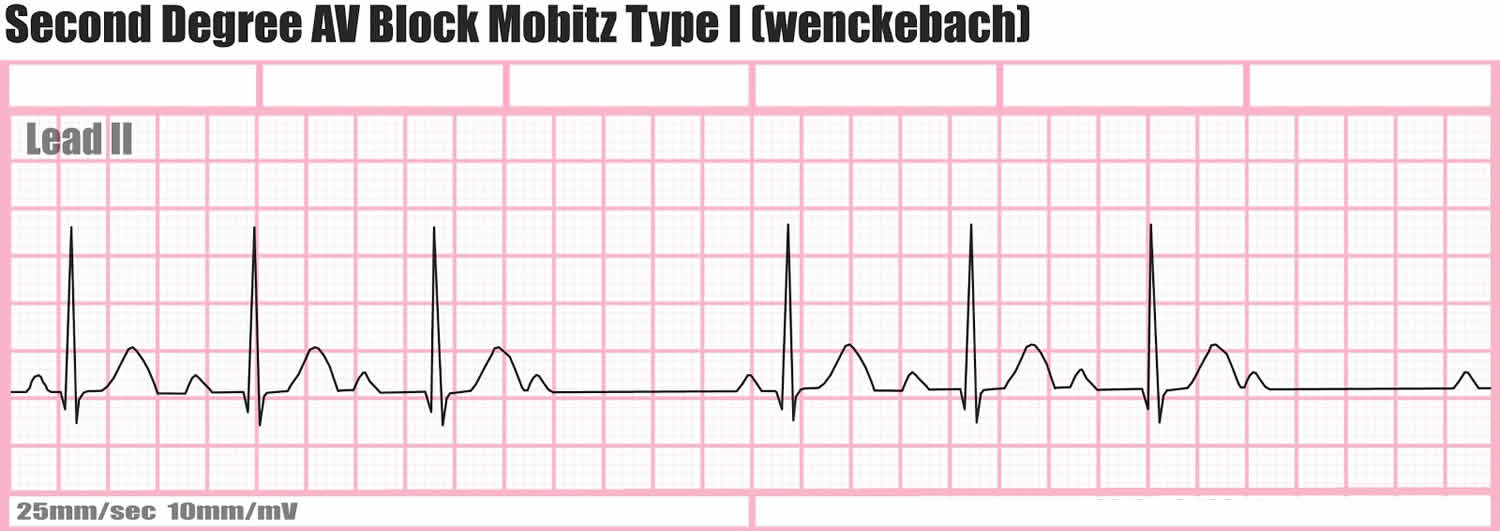
There are two types of second-degree heart blocks: Mobitz type I, also known as, Wenckebach and Mobitz type II 3.
2nd degree heart block type 1
Mobitz type 1 (Wenckebach block) is often a normal variant and seen in individuals with a high vagal tone without evidence of structural heart disease. However, this rhythm can result from inferior myocardial ischemia, medication toxicity (AV nodal blocking agents), hyperkalemia, cardiomyopathy (Lyme disease), or following cardiac surgery.
In Mobitz type 1 (Wenckebach block) there is a progressive prolongation of the PR interval (AV conduction) until eventually an atrial impulse is completely blocked 3. When an atrial impulse is completely blocked there will be a P wave without a QRS complex. This pattern is often referred to as a “dropped beat.” Mobitz type 1 (Wenckebach block) occurs because each depolarization results in the prolongation of the refractory period of the atrioventricular (AV) node. When an atrial impulse comes through the AV node during the relative refractory period, the impulse will be conducted more slowly, resulting in a prolongation of the PR interval. Eventually, an impulse comes when the AV node is in its absolute refractory period and will not be conducted. This will manifest on the ECG as a P wave that is not followed by a QRS complex. This non-conducted impulse allows time for the AV node to reset, and the cycle continues. This phenomenon leads to a grouped beating.
Mobitz type 1 (Wenckebach block) may not cause noticeable symptoms. Still, it can be a forerunner for the more serious type of second-degree heart block, Mobitz type 2. For this reason, Mobitz Type 1 should be monitored carefully by your doctor. Daily pulse checks on your own may also be advised.
Common drugs that are known to cause second-degree heart block include beta blockers, digoxin, calcium channel blockers and many antiarrhythmic agents. Recently the immunosuppressant agent, fingolimod, used to treat relapsing multiple sclerosis was also found to cause second-degree heart block 3.
Figure 3. Second degree heart block type 1
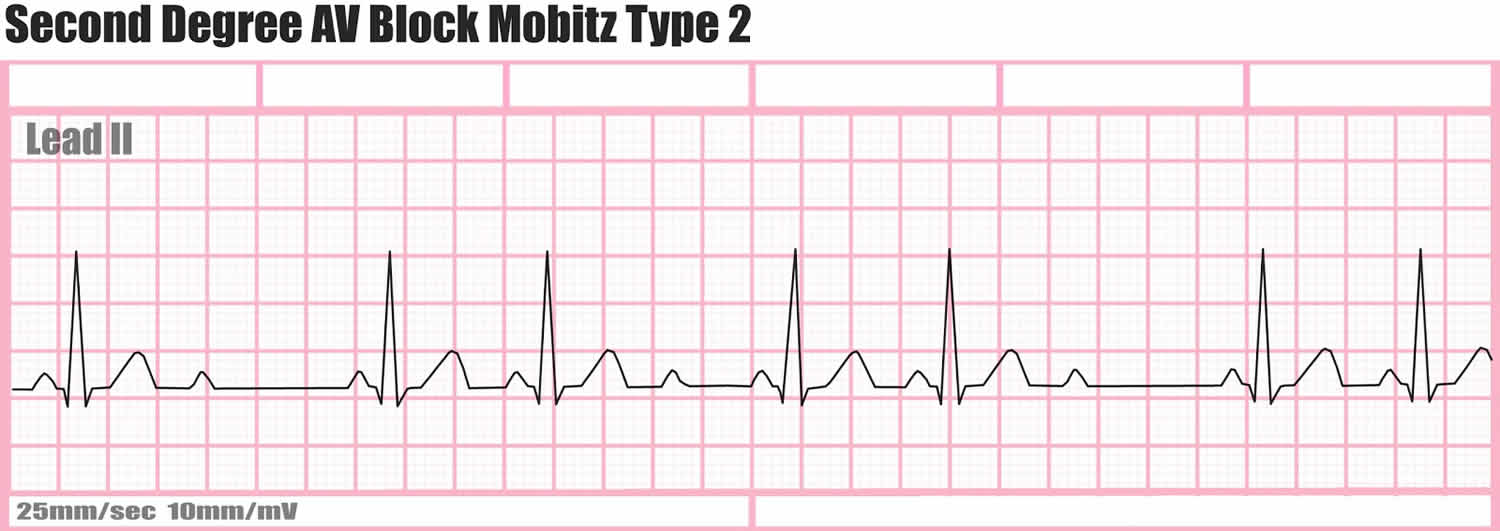
2nd degree heart block type 2
In this second-degree heart block Mobitz type 2, the heart doesn’t beat effectively. It impacts the heart’s ability to pump blood throughout the body. Often, a pacemaker is necessary to ensure that the heart will continue to beat regularly and efficiently.
Mobitz type 2 is rarely seen in patients without structural heart disease. It is often associated with myocardial ischemia and fibrosis or sclerosis of the myocardium. This rhythm often progresses to third-degree heart block (complete heart block).
In Mobitz type 2 there is a constant PR interval across the rhythm strip both before and after the non-conducted atrial beat. Each P wave is associated with a QRS complex until there is one atrial conduction or P wave that is not followed by a QRS. Mobitz type 2 is often a problem in the infra-nodal conduction system, and therefore, is associated with a widened QRS complex, bundle-branch block, or fascicular block. Be aware that if more than one P wave is not conducted this is no longer a Mobitz type 2 and is considered a high degree AV block.
Figure 4. Second degree heart block type 2
Third degree heart block
Third-degree heart block or complete heart block (sometimes called third-degree AV heart block) means that electrical signals can’t pass at all from the heart’s upper chambers (atria) to its lower chambers (ventricles). In the absence of electrical impulses from the sinoatrial node, the ventricles will still contract and pump blood, but at a slower rate than usual. This can affect the flow of blood to your body and brain.
Complete heart block is the most serious type of AV heart block. With third-degree heart block, the heart does not contract properly, and it can’t pump blood out to the body effectively.
Symptoms for third-degree heart block include:
- Chest pain
- Fainting (syncope)
- Dizziness
- Excessive fatigue
- Shortness of breath
Complete heart block may also cause fluid to build up in your body.
In some people, complete heart block is always there, while in others it comes and goes.
What causes complete heart block?
Most people with complete heart block have an underlying heart condition like coronary heart disease, cardiomyopathy or congenital heart disease.
It can also be caused by ageing of the electrical pathways in your heart (meaning you’re more likely to get it if you’re older), electrolyte imbalances, and some medicines in extreme cases.
An injury to the heart’s electrical conduction system during surgery can also cause third-degree heart block.
People with third-degree heart block require immediate medical attention. Their irregular and unreliable heartbeats heighten the risk of cardiac arrest.
A temporary or permanent pacemaker is used to treat third-degree heart block, providing a carefully timed electrical impulse to the heart muscle.
Figure 5. Third-degree heart block or complete heart block (sometimes called third-degree AV heart block)

Heart block symptoms
First-degree heart block
First-degree heart block doesn’t usually cause any noticeable symptoms. Most people only find out they have it when they’re tested for an unrelated medical condition.
Second-degree heart block
Most people with the less serious type of second-degree heart block, known as Mobitz type 1, won’t experience any symptoms.
But some people may experience:
- mild light-headedness or dizziness
- fainting
People with the more serious type of second-degree heart block, known as Mobitz type 2 heart block, are more likely to experience the above symptoms.
They may also experience:
- chest pain
- shortness of breath
- feeling very dizzy suddenly when standing up from a lying or sitting position – this is caused by having low blood pressure (hypotension)
Third-degree heart block
Symptoms of third-degree or complete heart block include:
- fainting – this can cause someone to collapse
- breathlessness
- extreme tiredness (fatigue), sometimes with confusion
- chest pain
- having a slow heart beat (bradycardia), or feeling a skipping, fluttering or pounding in your chest (palpitations)
If you experience severe symptoms or ones that come on very quickly, dial your local emergency services number to request an ambulance. These symptoms can be life threatening.
All types of heart block can increase your risk of developing other types of heart rhythm problems, such as atrial fibrillation (an irregular and abnormally fast heart rate).
Heart block diagnosis
Unless you’re experiencing symptoms, heart block is often diagnosed during routine tests for other conditions.
An electrocardiogram (ECG) is the main test used to diagnose heart block. It measures the electrical activity of your heart.
An ECG can be carried out at rest or while you’re exercising. Your doctor may ask you to wear a portable ECG monitor to get a reading over time. It provides a useful overall assessment of how well your heart is working.
The results of an ECG can also sometimes indicate the type of heart block you have.
It can often be challenging to separate the two types of second-degree heart blocks. A rhyme is often used to remember Mobitz type 1 or Wenckebach: “longer, longer, longer, DROP, now you have a Wenckebach.” This rhyme is alluding to the progressive prolongation of the PR interval before a non-conducted beat or the lack of a QRS complex after a P wave.
When a Mobitz type 1 has a fixed conduction ratio of 2:1, meaning 2 conducted beats to one non-conducted beat, it is difficult to differentiate between type 1 and type 2. In this scenario, it is recommended to assume the worst-case scenario and call this rhythm a “non-typeable second-degree AV block.” This should be managed like a Mobitz type 2 with transcutaneous or transvenous pacing until further workup can be completed.
Figure 6. Heart block ECG
Heart block treatment
For the vast majority of patients, first-degree heart block may not require specific treatment beyond routine observation for worsening conduction delay. If you have first-degree heart block, it’s important to check in regularly with your doctor to monitor the condition. Between appointments with the doctor, you should take your pulse regularly and watch out for slower than normal heart rates.
Treatment for a second-degree heart block Mobitz type 1 (Wenckebach block) is often not necessary. Occasionally second-degree heart block Mobitz type 1 blocks may result in bradycardia leading to hypotension. If hypotension and bradycardia occur, 2nd degree heart block type 1 blocks respond well to atropine. If unresponsive to atropine, pacing (transcutaneous or transvenous) should be initiated for stabilization.
Treatment for a second-degree heart block Mobitz type 2 involves initiating pacing as soon as this rhythm is identified. Second-degree heart block Mobitz type 2 blocks imply structural damage to the AV conduction system. This rhythm often deteriorates into complete heart block (3rd degree heart block). These patients require transvenous pacing until a permanent pacemaker is placed. Unlike second-degree heart block Mobitz type 1 (Wenckebach block), patients that are bradycardic and hypotensive with a 2nd degree heart block type 2 rhythm often do not respond to atropine.
All patients with heart block need lifelong follow up.
Treatments for complete heart block
- If you’re an adult with complete heart block that causes you to have a very slow heart rate, it’s likely your doctor will suggest that you have a pacemaker fitted.
- If you have complete heart block that was caused by a heart attack, you may only need a temporary pacemaker. If a normal heart rhythm hasn’t returned a few weeks after your heart attack, you might need to have a permanent pacemaker fitted.
- If you’re a young person with congenital heart disease with second-degree or third-degree heart block but you don’t have a slow heart rate or any symptoms, you may still need a pacemaker, but your specialist will discuss this with you.
- Oldroyd SH, Makaryus AN. Rhythm, Heart Block, First Degree. [Updated 2018 Oct 27]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2018 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK448164/
- Lewalter T, Pürerfellner H, Ungar A, Rieger G, Mangoni L, Duru F., INSIGHT XT study investigators. “First-degree AV block-a benign entity?” Insertable cardiac monitor in patients with 1st-degree AV block reveals presence or progression to higher grade block or bradycardia requiring pacemaker implant. J Interv Card Electrophysiol. 2018 Aug;52(3):303-306.
- Jones WM, Napier L. Rhythm, Atrioventricular Block, Second-Degree. [Updated 2018 Oct 27]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2018 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482359
- Heart Blocks. https://ecg-educator.blogspot.com/2016/02/heart-blocks.html





{kind=link}