
Hip flexor tendonitis
Hip flexor tendonitis also known as iliopsoas tendonitis or hip flexor tendinopathy causes pain and tenderness in the front of your hip. Iliopsoas tendonitis (hip flexor tendonitis) and iliopsoas bursitis are closely interrelated because inflammation of one inevitably causes inflammation of the other, due to their close proximity. Therefore, these 2 conditions are essentially identical in terms of presentation and management. Hip flexor tendonitis pain might be worse when you bend your hip. Your hip or groin area may feel sore to the touch. You might also hear or feel a click or snap if the tendon rubs across your hip bone as you walk.
Hip flexor tendonitis is noted to affect young adults more commonly, with a slight female predominance.
The two most common causes of hip flexor tendonitis are acute injury and overuse injury. The acute injury often involves eccentric contraction of the iliopsoas muscle or rapid flexion against extension force/resistance but may less commonly result from direct trauma. The overuse phenomenon may occur in any activity resulting in repeated hip flexion or external rotation of the femur.
Among dancers, a narrow bi-iliac width, greater abduction, decreased lateral rotation, and greater strength in the lateral rotators have been described more commonly with snapping hip syndrome, which is related to hip flexor tendonitis.
Rheumatoid arthritis may be a cause of iliopsoas bursitis.
A variety of terms have been used to describe and classify tendon injuries. Tendonitis is typically associated with an acute injury through which failure of the tendon fibers and disruption of the vascularized peritendinous connective tissue produces an acute inflammatory response within the tendon. Tendonitis may be acute, subacute, or chronic, depending on the duration of symptoms.
Peritendinitis is a condition in which an acute injury produces an inflammatory response in only the soft tissue surrounding a tendon, without disruption of the tendon fibers. On the other hand, tendinosis is often associated with chronic microtrauma to the tendon, such as repetitive overload. In the case of tendinosis, fiber failure tends to be characterized by intrasubstance failure, compared with peritendinous disruption, which occurs in tendinitis. Microscopic findings in tendinosis include fibrillar degeneration, angiofibroblastic proliferation, myxoid degeneration, fibrosis, and, occasionally, chronic inflammation.
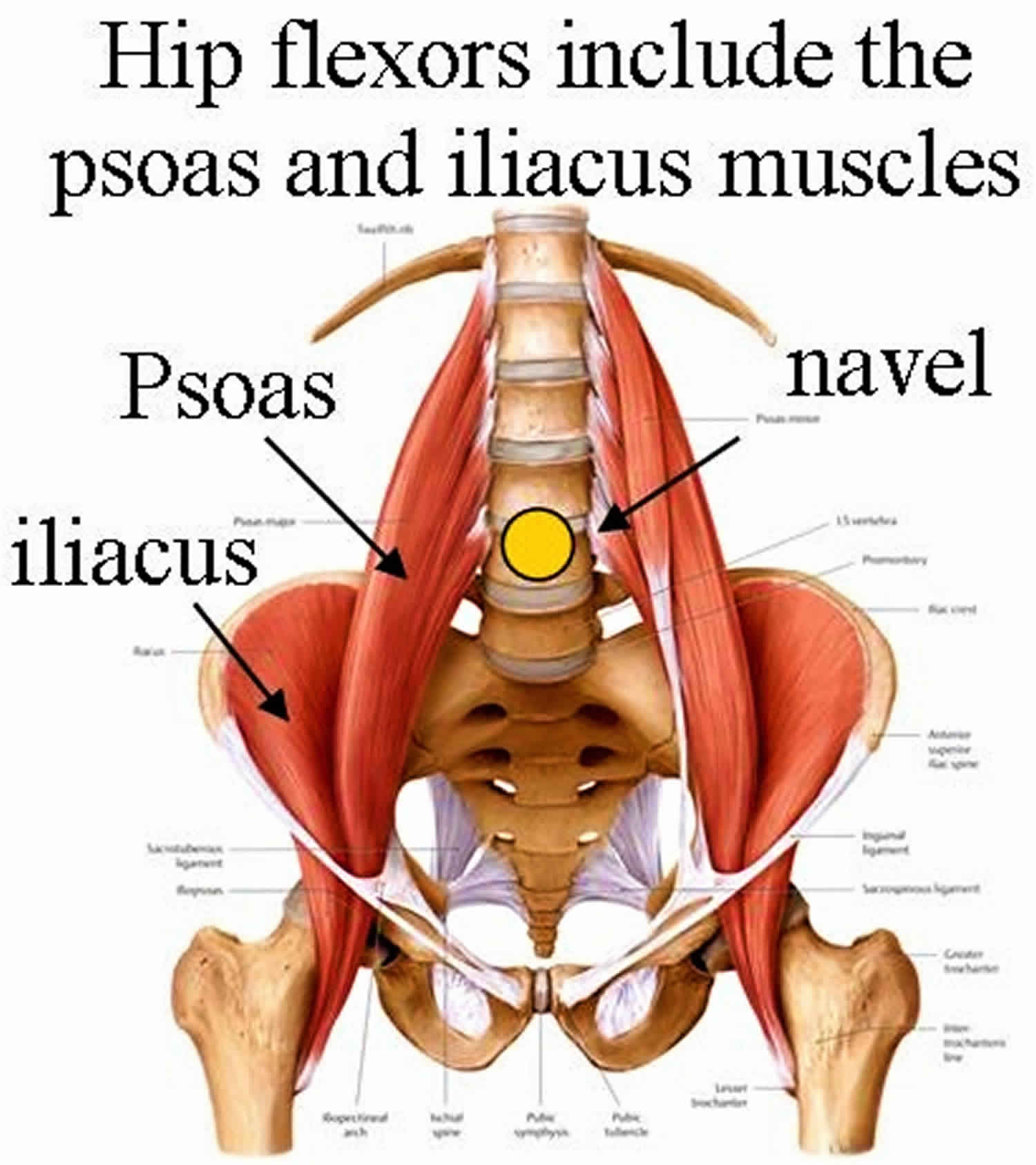
Figure 1. Hip flexors
Hip flexor anatomy
The pelvis links the trunk and lower extremities. The hip, a ball and socket joint, allows for 3 degrees of freedom. Range of motion (ROM) of the hip includes approximately 120° of flexion, 20° of extension, 40° of abduction, 25° of adduction, and 45° each of internal rotation and external rotation. The resting position of the hip is considered to be 30° of flexion and 30° of abduction.
The psoas and iliacus muscles originate from the lumbar spine (transverse processes t-12 and L1-5) and pelvis (superior anterior iliac crest), respectively, and are innervated by the upper lumbar nerve roots (ie, L1, L2, L3). These muscles converge to form the iliopsoas muscle, which inserts onto the lesser trochanter of the proximal femur as the iliopsoas tendon. The psoas major tendon exhibits a characteristic rotation through its course, transforming its ventral surface into a medial surface. The iliac portion of this tendon has a more lateral position, and the most lateral muscle fibers of the iliacus muscle insert onto the lesser trochanter without joining the main tendon.
The iliopsoas muscle passes anterior to the pelvic brim and hip capsule in a groove between the anterior inferior iliac spine laterally and iliopectineal eminence medially. The musculotendinous junction is consistently found at the level of this groove. The iliopsoas muscle functions as a hip flexor and external rotator of the femur.
An ilio-infratrochanteric muscular bundle has been described, which likely relates to the iliopsoas tendon. This muscular bundle arises from the interspinous incisure and anterior inferior iliac spine (above the origin of the rectus femoris muscle), courses along the anterolateral edge of the iliacus muscle, and inserts without a tendon onto the anterior surface of the lesser trochanter. The iliopsoas bursa lies between the musculotendinous junction and the pelvic brim. This bursa is the largest in the body and may extend proximally into the iliac fossa or distally to the lesser trochanter. Communication between this bursa and the hip joint occurs in approximately 15% of all adults.
Hip flexor tendonitis causes
Hip flexor tendonitis is an inflammation of the iliopsoas tendon or area surrounding the iliopsoas tendon. Major causes of hip flexor tendonitis are acute trauma and overuse resulting from repetitive hip flexion.
Acute injury and overuse injury are the two main causes of hip flexor tendonitis. The acute injury typically involves an eccentric contraction of the iliopsoas muscle, but also may be due to direct trauma. Overuse injury may occur in activities involving repeated hip flexion or external rotation of the thigh. Motions that call for repeated trunk flexion with hip flexion create a continuous shortening of the iliopsoas which can exacerbate iliopsoas tendonitis. Activities that may predispose to hip flexor tendonitis include dancing, ballet, resistance training, cycling, rowing, running (particularly uphill), track and field, soccer, and gymnastics.
During the adolescent growth spurt, the hip flexors tend to become relatively inflexible. This inflexibility can lead to problems in younger athletes because stress placed on the iliopsoas musculotendinous unit increases and general biomechanics are altered. Tightness of the iliopsoas, tensor fascia lata, or rectus femoris can lead to inhibition of the gluteus maximus, allowing for an anterior pelvic tilt. This in turn leads to adverse affects on the kinetic chain. Excessive anterior tilt can lead to increased lumbar lordosis with resultant stress on the lower lumbar discs, facet joints, and sacroiliac joints and may result in increased knee flexion at heel strike and during midstance phases of the gait cycle. The subsequent increase in eccentric load across the knee extensor mechanism may result in patellar tendon injuries. With increased knee flexion, compressive forces at the patellofemoral contact surface increase and may predispose to patellofemoral problems.
Hip flexor tendonitis prevention
Prevention of hip flexor tendonitis requires a focus on good flexibility and strength of the muscles of the hip. By following a few simple rules, the likelihood of hip strains can be reduced:
- Stretching should always be performed before and after sport.
- A warm up should be performed prior to sport which should involve some simple sport specific drills and range of motion exercises (eg. leg swings, jogging, jumping, direction changes whilst jogging, if playing soccer/football)
- Make sure the muscles of the hip are well conditioned through strengthening programs
- Working out regularly, instead of just on the weekends or only once in a while
- Training for a new sport or activity by gradually increasing the length and intensity of your workouts
- Stopping any activity that causes pain
- Not pushing yourself beyond your limits while exercising
Hip flexor tendonitis symptoms
Patients often present with complaints of an insidious onset of anterior hip or groin pain. As in other cases of tendonitis, initially the patient may note pain after onset of aggravating activity with resolution soon thereafter. This condition may progress to pain that persists during activity but subsides with rest, and eventually to pain during activity and at rest. The average time from initial onset of symptoms to diagnosis has been noted to range from 32-41 months.
At presentation, patients may note pain with specific sports-related activities, such as jogging, running, or kicking. Pain with simple activities, such as putting on socks and shoes, rising from a seated position with the hips flexed for some time, walking up stairs or inclines, or brisk walking may be reported.
Pain may radiate down the anterior thigh toward the knee.
Reports of an audible snap or click in the hip or groin commonly are reported and associated with internal snapping hip syndrome. In this syndrome, the inflamed iliopsoas tendon rolls over the iliopsoas bursa or head of the femur eliciting a palpable and audible snap.
Patients may report anterior knee pain consistent with patellar tendonitis or patellofemoral dysfunction, which may be the result of a tight iliopsoas muscle.
Hip flexor tendonitis diagnosis
Physical examination
Physical examination should focus on complete examination of the abdomen, hip, and groin. In females, absent definitive findings indicative of a musculoskeletal issue, a complete pelvic examination also should be considered.
Inspection
The hip may be held in slight flexion and external rotation to ease tension on the musculotendinous unit.
Gait may demonstrate a shortened stride length on the affected side and increased knee flexion in the heel strike and midstance phases.
Palpation
An anterior pelvic tilt may be appreciated due to subsequent tightening of the iliopsoas muscle.
Direct deep palpation to the area of the femoral triangle, which is bordered superiorly by the ilioinguinal ligament, medially by the adductor longus muscle, and laterally by the sartorius muscle, results in direct palpation of the iliopsoas musculotendinous junction. Inguinal lymph nodes should be unremarkable and pain free.
Tenderness over the iliopsoas tendon’s insertion may be noted by palpating the lesser trochanter under the gluteal fold with the patient lying in a prone position.
Functional testing
Functional testing includes resisted hip flexion at 15° with palpation of the psoas muscle below the lateral half of the inguinal ligament.
The patient also may be asked to sit with knees extended and subsequent elevation of the heel on the affected side. Pain caused by this maneuver (a positive Ludloff sign) is consistent with an iliopsoas tendonitis because the iliopsoas is the sole hip flexor activated in this position.
The snapping hip sign or extension test also may be performed. Start with the affected hip in a flexed, abducted, and externally rotated position (knee is flexed for ease of testing), and passively move the hip into extension. This may result in an audible snap or palpable impulse over the inguinal region. Pain associated with this maneuver is highly suggestive of iliopsoas tendonitis or bursitis.
Laboratory studies
Laboratory studies rarely are indicated if diagnosis of hip flexor tendonitis is certain.
If the diagnosis is unclear, a CBC count, erythrocyte sedimentation rate or C-reactive protein (CRP), rheumatoid factor, anticyclic citrullinated peptide antibody, antinuclear antibody, and urinalysis are helpful ancillary tests for distinguishing among several other causes of groin pain.
Imaging studies
Plain radiographs
Hip radiographs often are the initial imaging study obtained because diagnosis of hip flexor tendonitis may not be demonstrated clearly.
A pelvic anteroposterior radiograph and frog leg lateral radiograph of the affected hip often are adequate initial studies.
Radiographs typically are normal in cases of hip flexor tendonitis, but may demonstrate other bony pathology, which may contribute to the patient’s symptom complex.
Ultrasonography
Ultrasonography has been used more frequently as a noninvasive diagnostic adjunct in the diagnosis of muscle-tendon injuries. Demonstration of a thickened tendon is the usual finding 1.
Ultrasonography may demonstrate an excessive amount of fluid in the iliopsoas bursa consistent with iliopsoas bursitis, which may be either a primary or secondary problem.
Remember that ultrasonography is highly user-dependent and may not be the optimal test at institutions with personnel who are unfamiliar with ultrasonography use for this type of examination.
Magnetic resonance imaging (MRI)
MRI currently is the criterion standard in the ancillary evaluation of painful conditions of the hip and pelvis, particularly because many anatomical structures may be the origin of the pain. In a recent study of 19 endurance athletes with groin pain and an established clinical diagnosis, MRI was shown to reclassify 32% of the hips to a different etiology for the groin pain. These diagnoses included iliopsoas muscle tears and hip flexor tendonitis.
In evaluating musculotendinous injury, the spin-echo T2-weighted images demonstrate increased signal intensity associated with swelling and inflammation. However, in hemorrhage associated with a more severe musculotendinous injury, both the T1-weighted images and T2-weighted images depict a high-signal intensity.
In peritendinitis evaluation, increased fluid in the peritendinous tissue is detected on the spin-echo T2-weighted images or short T1 inversion recovery (STIR) sequence as a focus of high-signal intensity surrounding a normal tendon.
On the other hand, tendinosis is demonstrated on the spin-echo T1-weighted images as an area of higher signal intensity within the tendon associated with myxoid degeneration or angiofibroblastic proliferation. The spin-echo T2-weighted images may show an abnormal signal (usually less than that seen on the T1-weighted images) or a normal signal.
Lidocaine challenge test
Lidocaine challenge test may be performed in a challenging case of hip flexor tendonitis where cause of pain is unclear.
Utilizing an anterior approach through the femoral triangle, and under ultrasonographic guidance, an interventional radiologist or orthopedic surgeon attempts to bath the iliopsoas tendon with 1% lidocaine. In general, 10 mL of lidocaine administered via a 25-gauge spinal needle is adequate for local anesthesia.
Relief of symptoms after injection confirms diagnosis.
Hip flexor tendonitis treatment
Hip flexor tendonitis often is treated as follows:
- Rest. Take a break from your usual activities so that your muscles and tendons get a break.
- Ice. Putting an icepack on your hip for 10-15 minutes 3 to 4 times a day can help decrease pain and swelling. Do not put ice directly on your skin.
- Pain relievers, such as aspirin, ibuprofen, or naproxen, if recommended by your doctor, may help reduce pain and inflammation.
- If the pain persists, you an injection of a medicine called a corticosteroid may be recommended to help with pain. A peritendinous corticosteroid injection may be performed under ultrasonographic guidance with a combination of a local anesthetic (eg, 1% lidocaine) and a corticosteroid (eg, betamethasone, triamcinolone) 2. A study 3 that reported on patient outcomes up to 1 month after fluoroscopy-guided iliopsoas bursa injection for suspected iliopsoas tendinopathy found that fluoroscopy-guided iliopsoas bursa injection leads to a relevant improvement at 1 month or significant pain reduction after 15 min in most patients.
- In rare cases, surgery might be needed.
The average time from onset of symptoms to diagnosis typically ranges from months to years; therefore, most patients may present in the subacute or chronic phases of hip flexor tendonitis. Despite this, medical treatment during the acute phase consists of relative rest and avoidance of activities that cause pain. Rarely, crutches may be necessary if sufficient pain is associated with ambulation or activities of daily living. The application of ice for 20 minutes every 1-2 hours for the first 1-3 days is recommended in addition to a short course (eg, 5-14 d) of nonsteroidal anti-inflammatory drugs (NSAIDs) in order to potentially limit inflammation and assist with analgesia.
Intermittent episodes of pain may be experienced as the patient slowly starts to return to the activities of daily living and progresses in the strengthening program. At these times, short courses of analgesics may be required, in addition to activity modification.
Physical therapy
The primary objective of the acute rehabilitation phase is to alleviate pain, spasm, and swelling. A secondary issue, if necessary, is to return the patient to activities of daily living (eg, walking unassisted). A combination of medication, ice, rest, and gentle stretching assists these goals in coming to fruition. A pack of crushed ice in a damp cloth-covered ice bag applied for 20 minutes every 1-2 hours also can provide the patient with relief of pain, spasm, and inflammation.
In addition to relative rest (avoidance of activities that stress the iliopsoas muscle), a gentle stretching regimen can assist in reduction of spasm in the iliopsoas complex. Note that stretching must not immediately follow icing, when the sensitivity to pain is lessened, because a potential to overstretch exists. A gentle stretch for the iliopsoas muscle is demonstrated in the image below. Hold the stretch for a count of 20 seconds, relax for 30 seconds, and repeat the stretch 5 times. Caution patients to not hold their breath while maintaining a pain-free stretch.
If a normal gait is not present at the time of diagnosis, the patient needs to begin ambulation exercises with the assistance of crutches, gradually moving to partial weight bearing, progressing to full weight bearing, and, finally, walking without an antalgic gait and without assistance. The patient can practice walking in front of a full-length mirror to ensure that ambulatory rhythm and techniques are correct.
Passive and active range of motion exercises
A graduated flexibility and strengthening program guided by a physiotherapist may be necessary for more severe hip strains. Careful assessment by the physiotherapist to determine which factors have contributed to the development of the condition, with subsequent correction of these factors is also important to ensure an optimal outcome. The rehabilitation will involve moving the hip, first passively and then actively. This means initially, the hip is moved either by someone else or using your arms to assist the movement such that the injured muscle does not work during these movements. Following this hip movements are performed using the muscles that have been injured.
Here are some examples of typical rehabilitation exercises for your hip flexor strain. Start each exercise slowly. Ease off the exercise if you start to have pain.
Your doctor or physiotherapist will tell you when you can start these exercises and which ones will work best for you.
Hip flexor strain exercises
Pelvic tilt with marching
- Lie on your back with your knees bent and your feet flat on the floor.
- Tighten your belly muscles and buttocks, and press your lower back to the floor.
- Keeping your knees bent, lift and then lower one leg up off the floor, and then lift and lower your other leg like you are marching. Each time you lift your leg, hold that position for about 6 seconds before lowering your leg.
- Repeat 8 to 12 times.
Scissors
- Lie on your back with your knees bent at a 90-degree angle and your feet off the floor.
- Tighten your belly muscles and buttocks, and press your lower back to the floor.
- Slowly straighten one leg, and hold that position for about 6 seconds. Your leg should be about 30 centimeters off the floor. Bring that leg back to the starting position, and then straighten your other leg. Hold that position for about 6 seconds, and then switch legs again.
- Repeat 8 to 12 times.
Hamstring stretch (lying down)
- Lie flat on your back with your legs straight. If you feel discomfort in your back, place a small towel roll under your lower back.
- Holding the back of your affected leg for support, lift your leg straight up and toward your body until you feel a stretch at the back of your thigh.
- Hold the stretch for at least 30 seconds.
- Repeat 2 to 4 times.
Quadricep and hip flexor stretch (lying on side)
- Lie on your side with your good leg flat on the floor and your hand supporting your head.
- Bend your top leg, and reach behind you to grab the front of that foot or ankle with your other hand.
- Stretch your leg back by pulling your foot toward your buttock. You will feel the stretch in the front of your thigh. If this causes stress on your knee, do not do this stretch.
- Hold the stretch for at least 15 to 30 seconds.
- Repeat 2 to 4 times.
Hip flexor stretch (kneeling)
- Kneel on your affected leg and bend your good leg out in front of you, with that foot flat on the floor. If you feel discomfort in the front of your knee, place a towel under your knee.
- Keeping your back straight, slowly push your hips forward until you feel a stretch in the upper thigh of your back leg and hip.
- Hold the stretch for at least 15 to 30 seconds.
- Repeat 2 to 4 times.
Hip flexor stretch (edge of table)
- Lie flat on your back on a table or flat bench, with your knees and lower legs hanging off the edge of the table.
- Grab your good leg at the knee, and pull that knee back toward your chest. Relax your affected leg and let it hang down toward the floor until you feel a stretch in the upper thigh of your affected leg and hip.
- Hold the stretch for at least 15 to 30 seconds.
- Repeat 2 to 4 times.
Final stages – strength training
Initially exercises will be given that isolate and strengthen the injured muscle. Once the muscle regains its strength, a graduated return to running or sport specific activities is the final stage of rehabilitation to fully recondition the hip muscles. This should include the implementation of progressive acceleration and deceleration running drills before returning to sport.
Once there is full range of motion of the hip, full strength equal or greater than the uninjured leg, and you are able perform all of the fundamental skills of the required sport pain free, you are ready to return to sport.
Rehabilitation
The purpose of this rehabilitation phase is to return the patient to normal range of motion (ROM), strength, endurance, proprioception, and activity specific to the patient’s sport. Normal range of motion (ROM) can be accomplished by sustaining normal gait mechanics, maintaining a stretching regimen, and practicing good warm-up and cool-down techniques with exercise.
Stretching exercises that facilitate full ROM for the iliopsoas complex are demonstrated in the images below.
In addition to stretching for ROM, certain stretches can allow an anteriorly over-rotated pelvis to return to a more anatomical position. Stretching the rectus femoris (see the image below) promotes a neutral pelvic position and diminishes strain or spasm of the iliopsoas muscles. Instruct patients to hold the stretch as instructed in the Acute Phase of physical therapy.
In addition to stretching for return of normal pelvic alignment, strengthening the hamstrings provides a posterior force on the pelvic girdle and combats the stress of the iliopsoas pull on the anterior pelvis (see the images below). Iliopsoas muscle injury can cause lumbar lordosis and anterior pelvic tilt, both of which can be corrected by strengthening specific counteracting muscle groups.
Strengthening the abdominal musculature by performing sit-ups addresses both issues. Sit-ups performed by hooking ankles under an object or having them held fast can aggravate the lumbar lordosis and iliopsoas strain. Sit-ups or crunches executed with knees and hips flexed at 90° allows the iliopsoas to relax, with the effort concentrated on the rectus abdominis muscle, and preserves a neutral pelvic position (see the first image below). Exercises that strengthen the gluteus maximus also augment the ideal pelvic status.
Begin all strengthening exercises at a weight that the patient can comfortably lift or with an elastic band resistive device with which the patient controls the tension. Exercises should be pain-free and performed daily in 4 sets of 10-15 repetitions. As the weight becomes easier to lift, increase the resistance.
Endurance is gained through movement with low resistance over time. Exercises requiring repeated hip flexion or femoral external rotation can improve iliopsoas function if resistance is low. Examples of these exercises are cycling with low resistance, stair climbing on a machine with the setting on the lowest resistance, or walking. The workout should not produce pain but could fatigue the iliopsoas muscle. Use caution so that the musculature has time to recuperate prior to the next bout of endurance training. As the muscle recovers, endurance exercises can be performed daily, and resistance gradually can be increased with time of activity. Stretching the iliopsoas should occur following any strengthening and/or resistance exercises.
Recreational therapy
As tolerance to activity increases, the patient can begin easy resistance cycling, walking, and jogging (without terrain). In the recovery phase, the patient intends to gradually return to sport-specific activities, leading to full pain-free participation.
Other sports, such as soccer, competitive cycling, running, and gymnastics, all have a high demand of hip flexion combined with trunk flexion, which shortens the iliopsoas and can cause stress when the body demands hip flexion independent of trunk flexion. Maintaining a stretching and strengthening program is crucial and the patient should consider cross-training for lower extremity sports that allow for a more upright trunk.
Surgical therapy
Surgical intervention is not commonly used for hip flexor tendonitis; however, it is considered for those patients in whom typically prolonged nonsurgical management and a lidocaine injection trial fail 4.
The two surgical techniques that have been described are (1) complete release of the iliopsoas tendon and (2) partial release by transection of the posteromedial aspect of the iliopsoas tendon. Each approach has produced generally good results in terms of pain relief, with little documentation of significant residual weakness. Gruen et al 5 reported 73% of patients returned to previous athletic activities, with 45% also returning to their previous level of athletic participation following surgery. Hoskins et al 6 reviewed their experience with surgical correction by iliopsoas tendon fractional lengthening in 92 cases. Complications were noted in one third of patients and mostly included persistent hip pain, sensory deficits, and hip flexor weakness 7.
Ilizaliturri et al 8 conducted a randomized study of the short-term results of two different techniques of endoscopic iliopsoas tendon release for the treatment of internal hip flexor tendonitis. One group of patients (n = 10 [5 men, 2 women]; average age, 29.5 years) underwent endoscopic iliopsoas tendon release at the lesser trochanter; the second group (n = 9 [1 man, 8 women and 1 male]; average age, 32.6 years) underwent endoscopic transcapsular psoas release from the peripheral compartment. Both groups received hip arthroscopy of the central and peripheral compartments, and any associated injuries were identified and treated arthroscopically 8. Both groups received the same postoperative physical therapy as well as 400 mg of celecoxib daily for 21 days after surgery. There were no complications.
The investigators found statistical improvement in Western Ontario MacMaster (WOMAC) scores for both groups, but there was no difference in postoperative WOMAC results between the groups. Ilizaliturri et al concluded that iliopsoas tendon release at the level of the lesser trochanter or at the level of the hip joint using a transcapsular technique is effective and reproducible 8.
In 2014, Ilizaliturri et al 9 again evaluated the results of 2 different techniques of endoscopic iliopsoas tendon release in the treatment of internal snapping hip syndrome and concluded that both central compartment release and release at the lesser trochanter produced favorable results.
Dobbs et al 10 reported outcomes for surgical fractional lengthening of the iliopsoas tendon in adolescents (mean age 15 years). [10] At 4-year mean follow-up, all patients had returned to their preoperative level of activity without subjective weakness.
Byrd et al 11 described releasing the iliopsoas tendon arthroscopically, and in a small study, Anderson and Keene 12 evaluated whether athletes can return to full participation in their sport following arthroscopic iliopsoas tendon release. A total of fifteen athletes (2 college, 3 high school, 10 recreational) with painful snapping hips that did not have pain relief following anesthetic magnetic resonance arthrography received an ultrasonographic evaluation of their iliopsoas tendon and an anesthetic injection into the psoas bursa. All 15 patients had pain relief and were followed up with Byrd’s 100-point hip scoring system at 1.5, 3, 6,and 12 months after surgery. Anderson and Keefe 12 concluded that a return to college, high school, and recreational sports can be expected after arthroscopic release of the iliopsoas tendon.
A retrospective review by Mardones et al 13 also reported positive outcomes with arthroscopic iliopsoas tendon release and that iliopsoas tendinopathy can be associated with femoroacetabular impingement, in which failure to diagnose can lead to poor results and revision surgery.
References- Iagnocco A, Filippucci E, Riente L, Meenagh G, Delle Sedie A, Sakellariu G, et al. Ultrasound imaging for the rheumatologist XLI. Sonographic assessment of the hip in OA patients. Clin Exp Rheumatol. 2012 Sep-Oct. 30(5):652-7.
- Han JS, Sugimoto D, McKee-Proctor MH, Stracciolini A, d’Hemecourt PA. Short-term Effect of Ultrasound-Guided Iliopsoas Peritendinous Corticosteroid Injection. J Ultrasound Med. 2018 Oct 31.
- Agten CA, Rosskopf AB, Zingg PO, Peterson CK, Pfirrmann CW. Outcomes after fluoroscopy-guided iliopsoas bursa injection for suspected iliopsoas tendinopathy. Eur Radiol. 2015 Mar. 25 (3):865-71.
- Anderson CN. Iliopsoas: Pathology, Diagnosis, and Treatment. Clin Sports Med. 2016 Jul. 35 (3):419-33.
- Gruen GS, Scioscia TN, Lowenstein JE. The surgical treatment of internal snapping hip. Am J Sports Med. 2002 Jul-Aug. 30(4):607-13.
- Hoskins JS, Burd TA, Allen WC. Surgical correction of internal coxa saltans: a 20-year consecutive study. Am J Sports Med. 2004 Jun. 32(4):998-1001.
- Garala K, Power RA. Iliopsoas tendon reformation after psoas tendon release. Case Rep Orthop. 2013. 2013:361087.
- Ilizaliturri VM Jr, Chaidez C, Villegas P, Briseno A, Camacho-Galindo J. Prospective randomized study of 2 different techniques for endoscopic iliopsoas tendon release in the treatment of internal snapping hip syndrome. Arthroscopy. 2009 Feb. 25(2):159-63.
- Ilizaliturri VM Jr, Buganza-Tepole M, Olivos-Meza A, Acuna M, Acosta-Rodriguez E. Central compartment release versus lesser trochanter release of the iliopsoas tendon for the treatment of internal snapping hip: a comparative study. Arthroscopy. 2014 Jul. 30(7):790-5.
- Dobbs MB, Gordon JE, Luhmann SJ, Szymanski DA, Schoenecker PL. Surgical correction of the snapping iliopsoas tendon in adolescents. J Bone Joint Surg Am. 2002 Mar. 84-A(3):420-4.
- Byrd JW. Hip arthroscopy. J Am Acad Orthop Surg. 2006 Jul. 14(7):433-44.
- Anderson SA, Keene JS. Results of arthroscopic iliopsoas tendon release in competitive and recreational athletes. Am J Sports Med. 2008 Dec. 36(12):2363-71
- Mardones R, Via AG, Tomic A, Rodriguez C, Salineros M, Somarriva M. Arthroscopic release of iliopsoas tendon in patients with femoro-acetabular impingement: clinical results at mid-term follow-up. Muscles Ligaments Tendons J. 2016 Jul-Sep. 6 (3):378-383.





{kind=link}