
What is intubation
Intubation is a medical procedure involving the insertion of an endotracheal tube into the airway (trachea). Endotracheal tubes are used to establish and maintain airway patency, prevent aspiration into the lungs, i.e. ‘secure’ the airway, and allow mechanical ventilation.
Intubation broadly serves two purposes:
- Maintaining patency of the airway.
- Securing the airway: This refers to protecting the lungs from aspiration of contaminants. Most endotracheal tubes have a cuff near their tip which, when inflated, provides a seal between the endotracheal tube tube and the tracheal wall, preventing leakage of e.g. gastric contents into the lung. This seal also allows for intermittent positive pressure ventilation (IPPV) of the lungs. Intubation is still the gold standard for securing an airway when compared to supraglottic airway devices.
Patients require an intubation under two sets of circumstances: failure to maintain a patent airway and the inability to oxygenate and ventilate the patient adequately 1. The causes of these circumstances can vary and include but are not limited to:
- Inability to protect the airway
- Inability to maintain oxygenation and/or ventilation
- Airway obstruction
- Current or expected clinical course concerning for airway compromise
- Diminished level of consciousness with concern for the loss of airway control (Glasgow coma scale less than 8)
- Hypoxemic or hypercarbic respiratory failure
- Cardiac arrest
- Risk of aspiration with vomiting, secretions, or blood
The wide range and variety of available endotracheal tubes, intubating aids, laryngoscopes, other devices designed to visualize the airway and glottis, anatomical routes, and of course patient characteristics, means a large number of techniques are used for intubation. In addition, clinicians might then also slightly modify these many technical approaches to suit their personal preferences and style. Consequently we end up with a myriad of techniques to place an endotracheal tube tube into the trachea.
Which anatomical route will the endotracheal tube tube take to the trachea?
- Oral intubation: Oral intubation is the most common approach
- Nasal intubation: The nasal route is useful in a number of scenarios, for example for some types of head & neck surgery and awake fiberoptic intubation
- Front of neck airway (FONA): This covers cricothyrotomy and tracheotomy access to the trachea
- Sub-mental intubation: A somewhat exotic rarely used approach to the airway through the floor of the mouth
Intubation anatomy
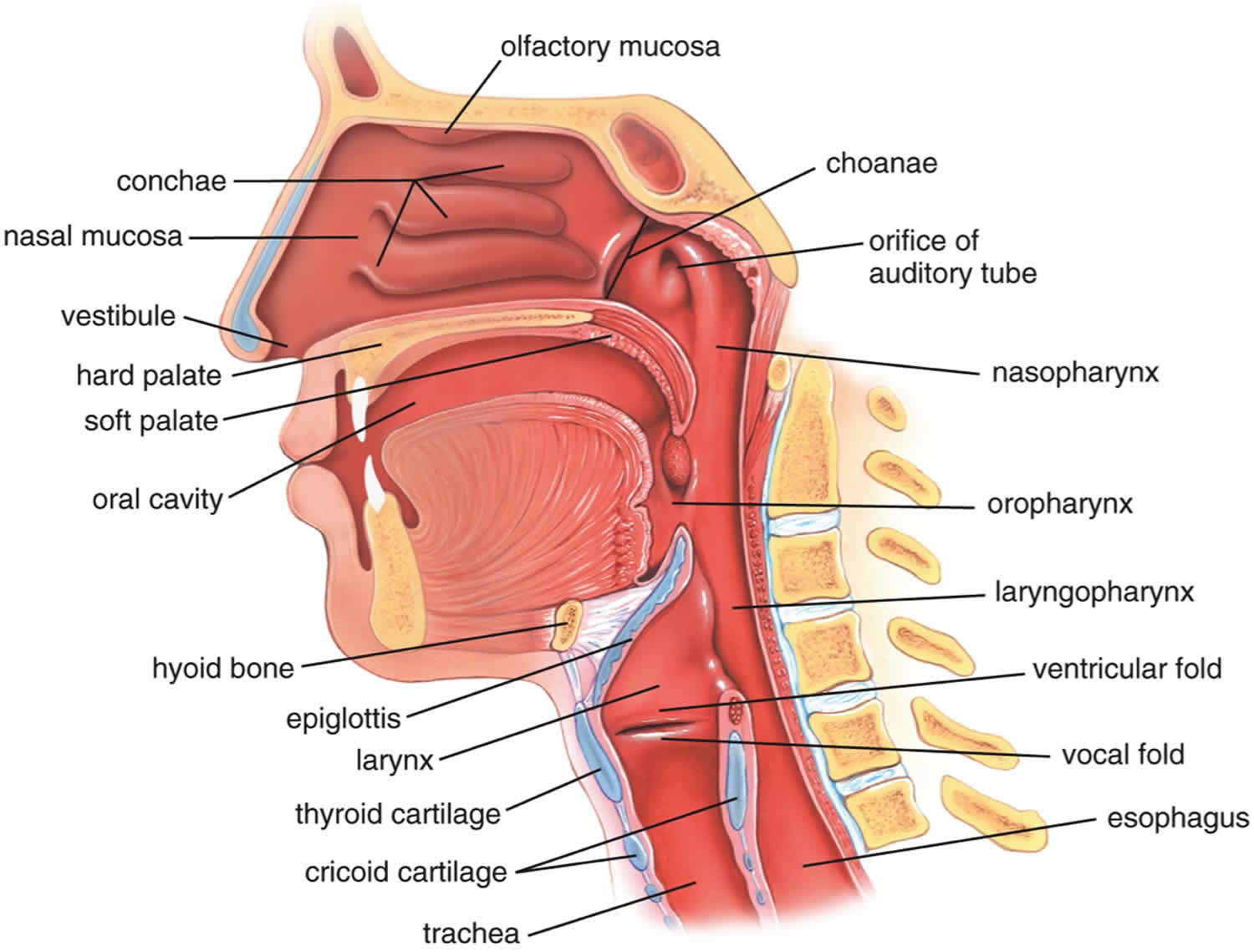
The upper airway comprises the nasal and oral cavities, the pharynx, and the larynx. The lower airway consists of the subglottic larynx, the trachea, and the bronchi. Airway management typically involves the upper airway, the focus of this chapter. The anatomy of the pharynx, larynx, and trachea are depicted in Figure 1.
The nasal cavity begins at the anterior nares and ends at the posterior end of the nasal septum where it channels into the nasopharynx via the posterior nasal apertures (choanae). The nasal cavity sits above the oral cavity and hard palate and rests below the skull base.
The hard palate provides the base of the cavity that runs horizontally and directly behind the anterior nares. The ceiling of the nasal cavity is formed from the narrow cribriform plate of the ethmoid bone. Lastly, both left and right lateral walls are established by the medial wall of the respected orbit superiorly and the maxillary sinus inferiorly.
The lateral nasal walls incorporate three structures, the turbinates, which project into the nasal passages as ridges of tissue and are responsible for maintaining moisture and warmth in the nasal cavity as air flows through.
The inferior turbinate is the largest of the 3 and projects along the complete lateral nasal wall. The inferior turbinates are often responsible for blocking nasal airflow when they are enlarged or inflamed. The middle turbinate projects into the central nasal cavity adjacent to the nasal septum. Finally, the superior turbinate, the smallest of the three, attaches to the skull base superiorly and the nasal wall laterally.
The nasal cavity is separated by a nasal septum consisting of both a cartilaginous part that sits anteriorly and a bony portion that rests more posteriorly. This septum separates the anterior nasal pathway into a left and a right side, where these 2 cavities eventually coalesce to form a single continuous cavity in the back of the nose (the nasopharynx).
The nasal cavity is lined by respiratory mucosa (histologically described as ciliated pseudostratified columnar epithelium) lying on an extremely vascular stroma. These cells produce serous secretions that aid in humidification of inspired air. The cilia help to trap unwanted debris from entering the lungs.
The nares serves as the functional beginning of the airway, namely warming and humidification of air. The mucosa of the nasal passage is extremely vascular and fragile and therefore susceptible to trauma. The nasal blood supply originates from branches of the internal and external carotid arteries. It is wise to consider the use of a vasoconstricting agent, when appropriate, to help avoid epistaxis which may obscure further attempts at securing the airway. Although patients tolerate nasal intubation better than oral intubation for a longer period of time, it is more important in an emergency to definitively secure the airway using a straightforward oral intubation if possible.
The sensory innervation of the upper airway is provided by branches of several cranial nerves. The mucous membrane of the nose is innervated anteriorly by the anterior ethmoid nerve (ophthalmic division of the trigeminal nerve) and posteriorly by the sphenopalatine nerve (maxillary division of the trigeminal nerve). The tongue is innervated by the lingual nerve on its anterior two-thirds (a branch of the facial nerve) and by the glossopharyngeal nerve posteriorly. The glossopharyngeal nerve also innervates the adjacent areas, including the palatine tonsils, the undersurface of the soft palate, and the roof of the pharynx.
Due to the high vascularity of the nasal cavity, minor trauma to any part of the tissue can cause bleeding to occur (epistaxis). The anterior nasal septum is particularly susceptible to developing epistaxis owing to the superficial location of the arterial plexus. This plexus is known as Kiesselbach’s area and is supplied by branches of the anterior and posterior ethmoid, superior labial, sphenopalatine and greater palatine arteries.
While considering normal nasal cavity anatomy, it is also important to understand that anomalies do often exist. Septal deviation is perhaps the most common anomaly which usually involves the cartilaginous aspect of the nasal septum. The deviation is most often due to trauma but can also be caused by continuous nasal congestion from recurrent sinus infections. Other variations to normal anatomy include conditions that result in unilateral obstruction such as nasal polyps, concha bullosa, and spurs. It is important to consider these anomalies during pre-anesthetic evaluation to minimize any complications as most of these variations will result in changes to airflow dynamics inside the nasal cavity. Nasal polyps or spurs may be unilateral which may dictate which side of the nose is more amenable to nasotracheal intubation 2.
The trachea or “windpipe,” measures 10 to 16.5 cm long and 2.5 cm (1 in.) in diameter, in an average adult. The trachea lies in front of the esophagus (Figure 1). The trachea is supported by 16 to 20 C (horseshoe) shaped rings of hyaline cartilage rings. The trachea is named for the corrugated texture imparted by these rings; you should be able to feel a few of these between your larynx and sternum. Like the wire spiral in a vacuum cleaner hose, the cartilage rings reinforce the trachea and keep it from collapsing when you inhale. The open posterior aspect of the trachea is flat, where it is spanned by a smooth muscle, the trachealis. The gap in the C allows room for the esophagus to expand as swallowed food passes by. The trachealis muscles contract or relax to adjust airflow. The trachea is a tubular structure that begins at the level of the fifth or sixth cervical vertebrae and bifurcates at the level of the fifth thoracic vertebra into two primary bronchi.
The lumen of the esophagus is normally closed because, unlike the airway, it has no skeletal support structures to hold it open. When the oral cavity is full of liquid or food, the soft palate is swung down (depressed) to close the oropharyngeal isthmus, thereby allowing manipulation of food and fluid in the oral cavity while breathing. When swallowing, the soft palate and parts of the larynx act as valves to ensure proper movement of food from the oral cavity into the esophagus. The soft palate elevates to open the oropharyngeal isthmus while at the same time sealing off the nasal part of the pharynx from the oral part. This prevents food and fluid from moving upward into the nasopharynx and nasal cavities. The epiglottis of the larynx closes the laryngeal inlet and much of the laryngeal cavity becomes occluded by opposition of the vocal folds and soft tissue folds superior to them. In addition, the larynx is pulled up and forward to facilitate the moving of food and fluid over and around the closed larynx and into the esophagus.
The neck contains the seven cervical vertebrae and associated muscles, parts of the alimentary and respiratory tracts and the thyroid gland. In the midline immediately anterior to the vertebrae is the pharynx, which continues as the cervical oesophagus. Anterior to these are the larynx and upper trachea with the thyroid gland. On each side of the organs, major vessels pass between the thorax and the head, accompanied by nerves and lymphatics.
Figure 1. Upper airway anatomy
Intubation tube
Endotracheal tubes are mostly made of polyvinylchloride (PVC) and are single-use. Endotracheal tubes have a number of characteristic features that are listed below. Polyvinylchloride (PVC), the material which most endotracheal tubes are made of, does not absorb x-rays. PVC tubes therefore contain a radio-opaque line, which makes them visible on chest radiographs. In addition, most endotracheal tubes (ETTs) have a pilot balloon with non-locking Luer connector and a metal spring valve through which the cuff can be inflated. The pilot balloon allows visual and tactile assessment of whether the cuff is inflated or not.
Endotracheal tubes tip design
Endotracheal tubes (ETTs) typically have a left-facing bevel at the tip and, as a second design feature, a Murphy eye.
The bevel is left-facing rather than right-facing to allow the endotracheal tube tip an easier pass through the vocal chords. Endotracheal tubes are usually placed with the right hand in a right-to-left direction towards the larynx (see Figure 2 below). Whilst an endotracheal tube with a bevelled tip is obviously easier to pass through the vocal chords, it is more likely to occlude when the opening makes contact with the tracheal wall. The Murphy eye provides an alternate gas passage should occlusion occur.
Figure 2. Endotracheal tube
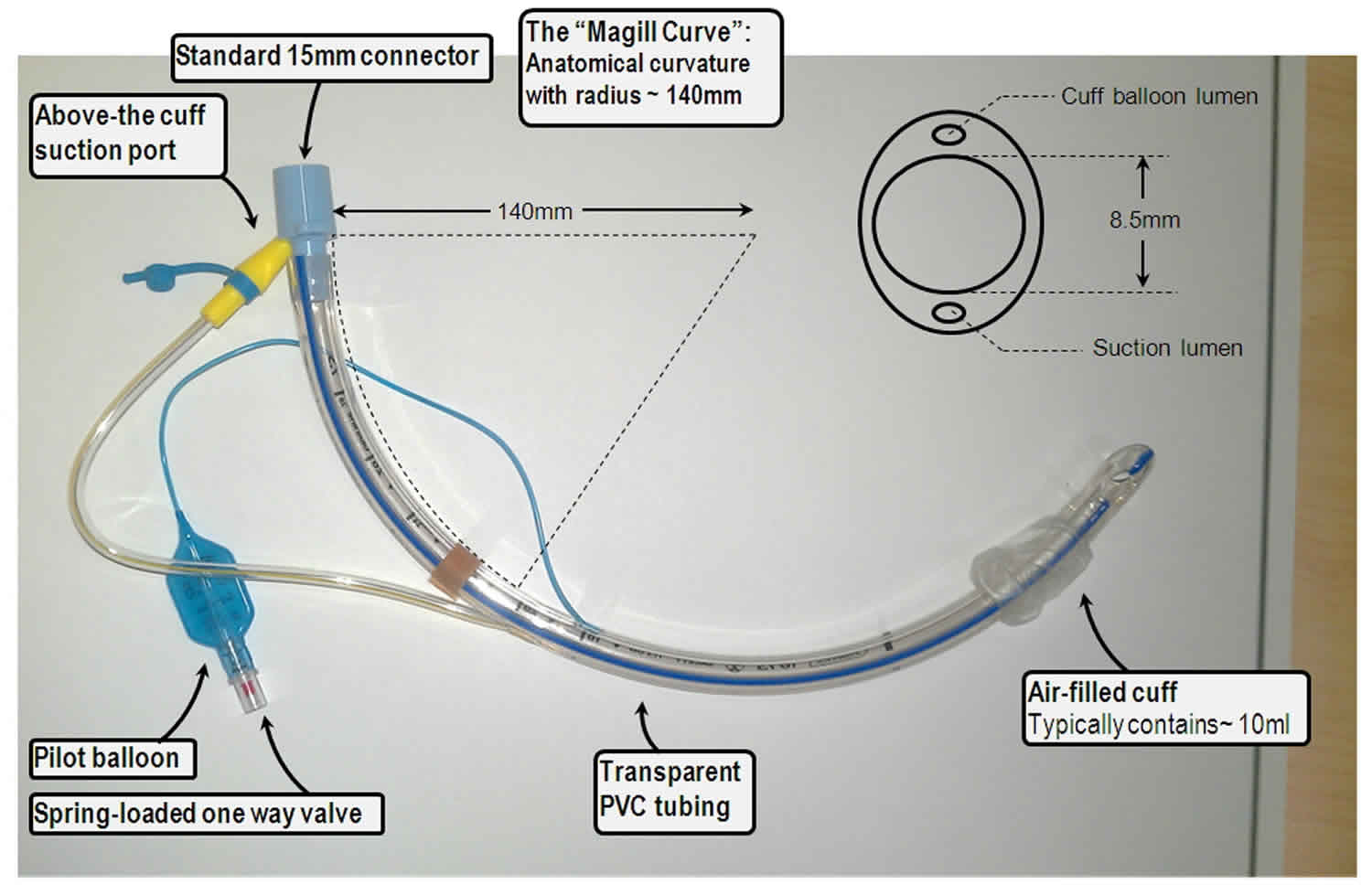 Figure 3. Murphy eye of an endotracheal tube
Figure 3. Murphy eye of an endotracheal tube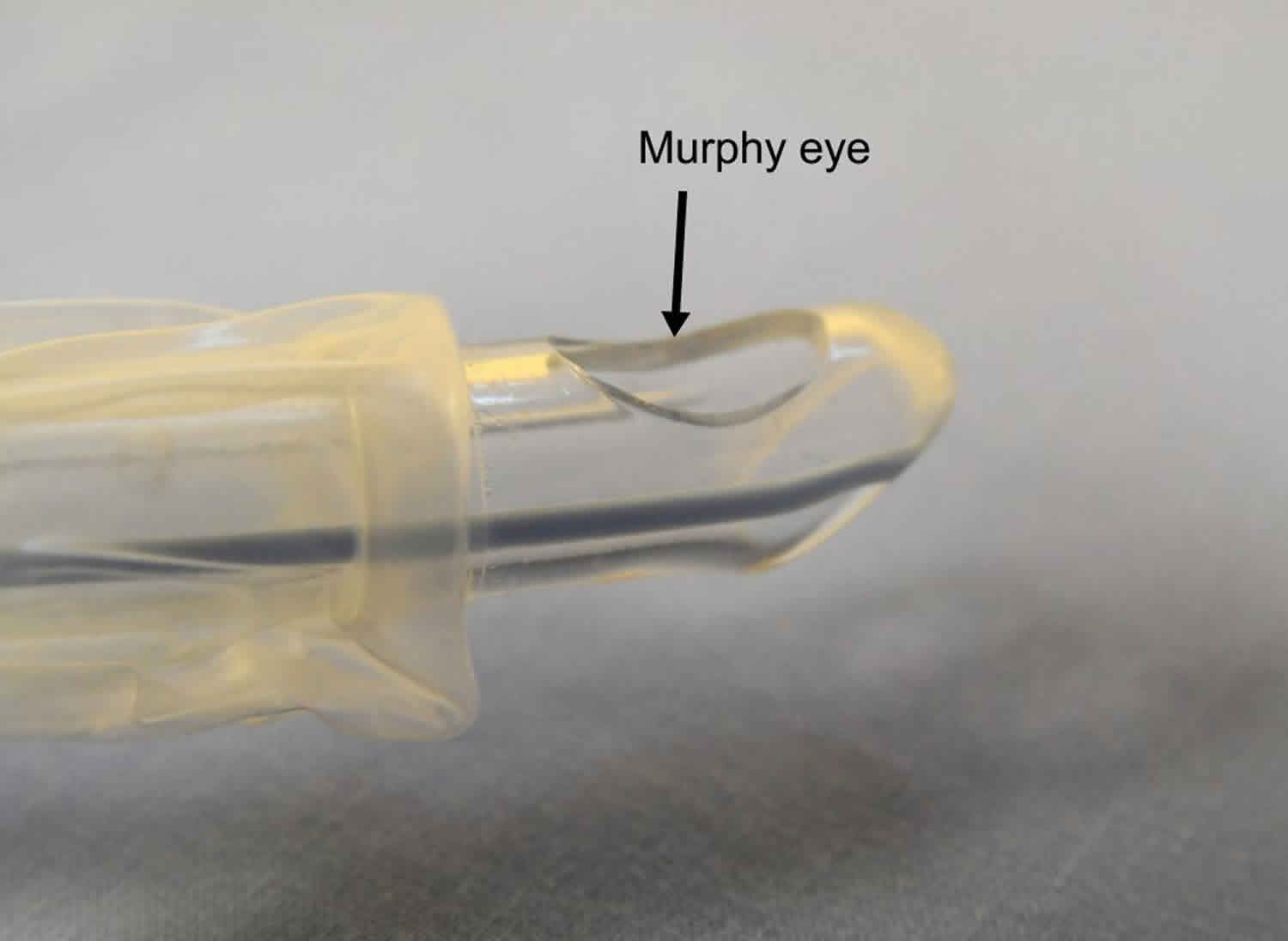
Cuff design
The majority of endotracheal tubes used in the operating room are of the low pressure- high volume type. These cuffs have a comparatively large volume and consequently large contact area between cuff and trachea. The cuff can develop folds in this contact area when inflated, resulting in an increased risk of aspiration secondary to regurgitated fluid tracking along these fold into the trachea.
In contrast, high pressure-low volume cuffs are thought to provide better protection against aspiration. Because of their much smaller cuff-trachea contact area and higher inflation pressures used, cuff folds are less likely to develop. The downside of this cuff type is that the higher cuff pressures are more likely to lead to tracheal mucosal ischemia. The cuff of the laser tube is of the high pressure- low volume design.
RAE tubes
RAE tubes are named after their inventors Ring, Adair and Elwyn who described the use of their novel oral preformed tube in pediatric patients in 1975 (Ring et al., 1975). RAE tubes were designed with the intention to facilitate intra-oral and some types of facial surgery by moving the part of the endotracheal tube tube outside of the patient away from the surgeon’s access.
RAE tube features
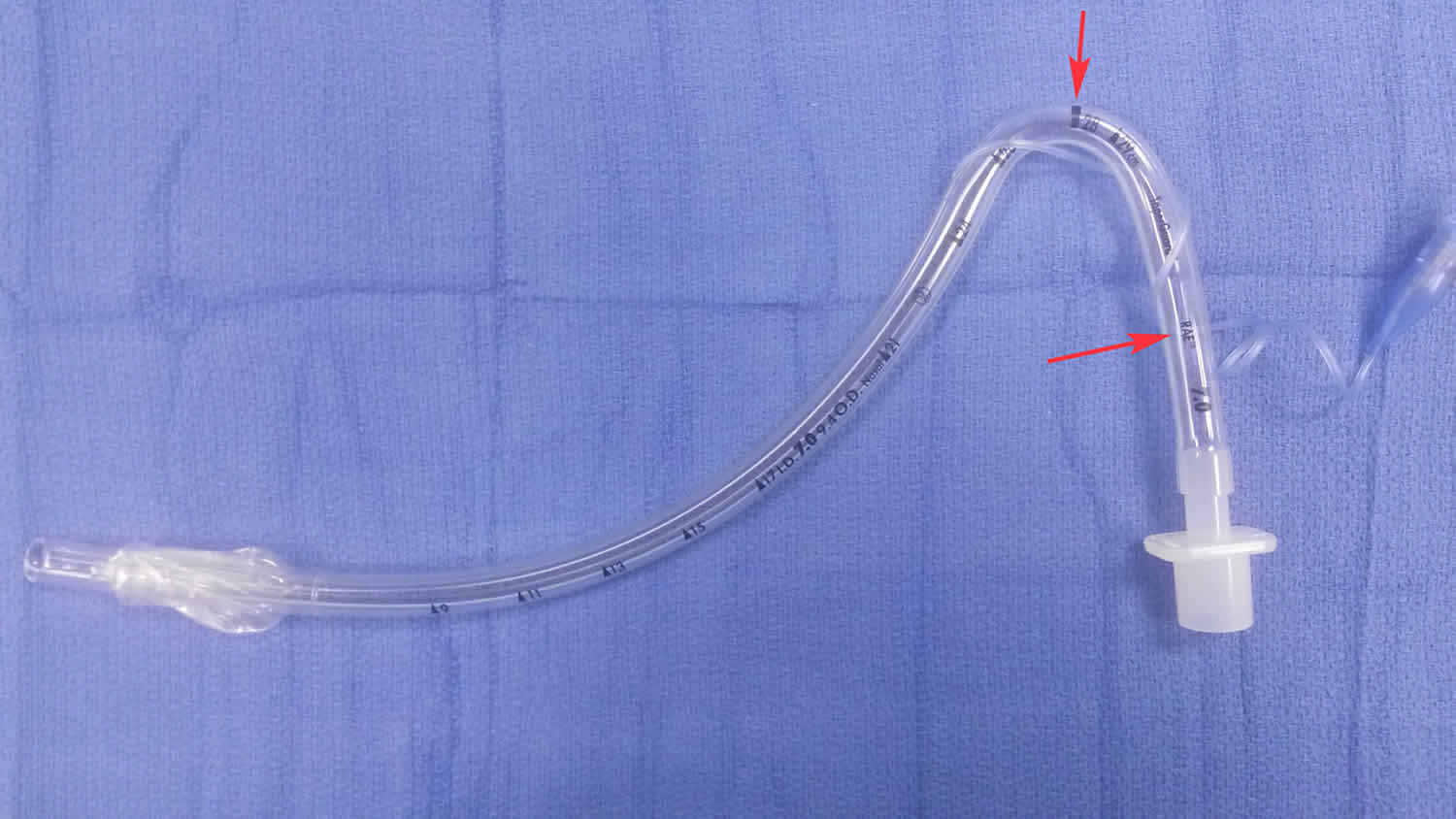
The distinguishing feature of RAE tubes in comparison to ‘standard’ endotracheal tube tubes is their pre-formed bend. The pre-forming during manufacturing reduces the risk of kinking and obstruction which could occur if a ‘standard’ endotracheal tube tube was bent into the same shape as a RAE tube. A black marker bar is imprinted on the tube at the point of maximum angle of the bend (see Figures 4 and 5 below).
RAE endotracheal tubes are otherwise designed the same way as ‘standard’ orotracheal tubes, i.e. they have the same left -facing bevelled tip, Murphy eye, cuff design, and length/ diameter markings.
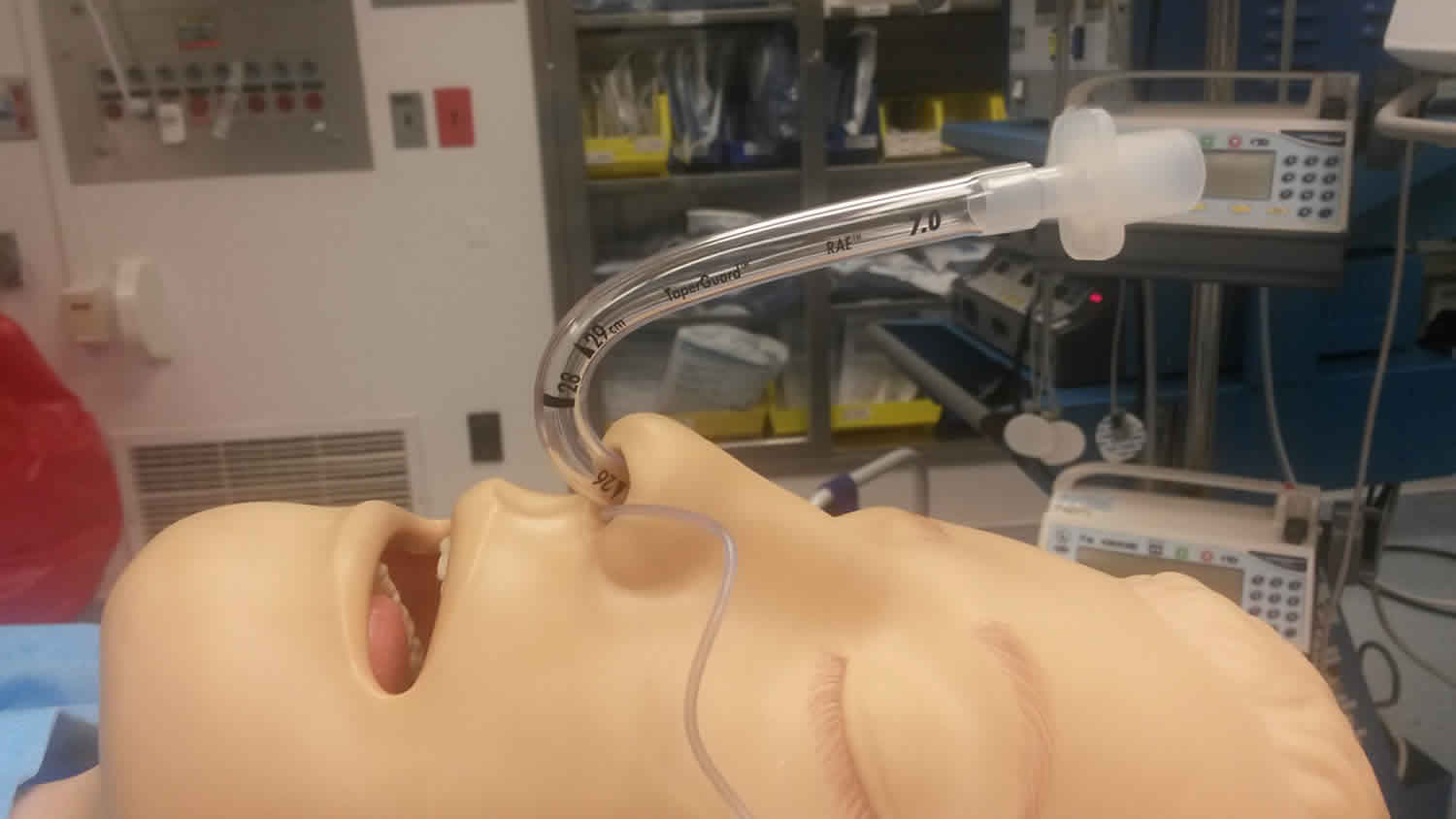
Oral RAE tubes are also described as ‘south-facing’, i.e. the tube connector facing towards the patient’s feet after placement, while nasal RAE tubes are also known as ‘north-facing’, i.e. the tube connector facing towards the patient’s head after placement.
RAE tubes uses
Oral RAE tube
The indications for placing an oral RAE tube are purely surgical, i.e. its use removes the tube connector and anesthetic breathing circuit from the surgical field or access to the surgical field.
Nasal RAE tube
Again, the indications for placing this type of endotracheal tube tube are mainly surgical as described above. The nasal RAE tube is also the ‘go-to’ device for many practitioners when performing an (awake) nasal fiberoptic intubation.
SPECIAL CONSIDERATIONS
Disadvantages of the RAE tube
One disadvantage of the nasal (and even more so the oral) RAE tube is that depth of tube insertion is very much pre-determined by the tube’s pre-formed shape, i.e. the bend of the oral and nasal RAE will always want to sit just at the lower lip and at the nostril respectively, not allowing you much flexibility as to how deeply you can place the tube into the trachea. In some patients, especially very tall or short ones, it might be difficult to achieve a good tube ‘fit’ together with the correct insertion depth which avoids accidental bronchial intubation or cuff placement between the vocal chords.
This problem can be avoided by using an armored/ reinforced tube instead of the oral or nasal RAE tube. The armored/ reinforced tube can be bent just as much (and more) as the RAE tube without kinking and obstructing.
Securing the RAE tube
Securing the nasal RAE tube is described in the ‘securing the endotracheal tube’ section.
The oral RAE tube is best secured by taping it (midline) to the skin between the lower lip and the chin. Use wide tape or a bio-occlusive dressing to get as big a surface area of contact between tube, skin and tape as possible.
Figure 4. Oral endotracheal tube (RAE tube)
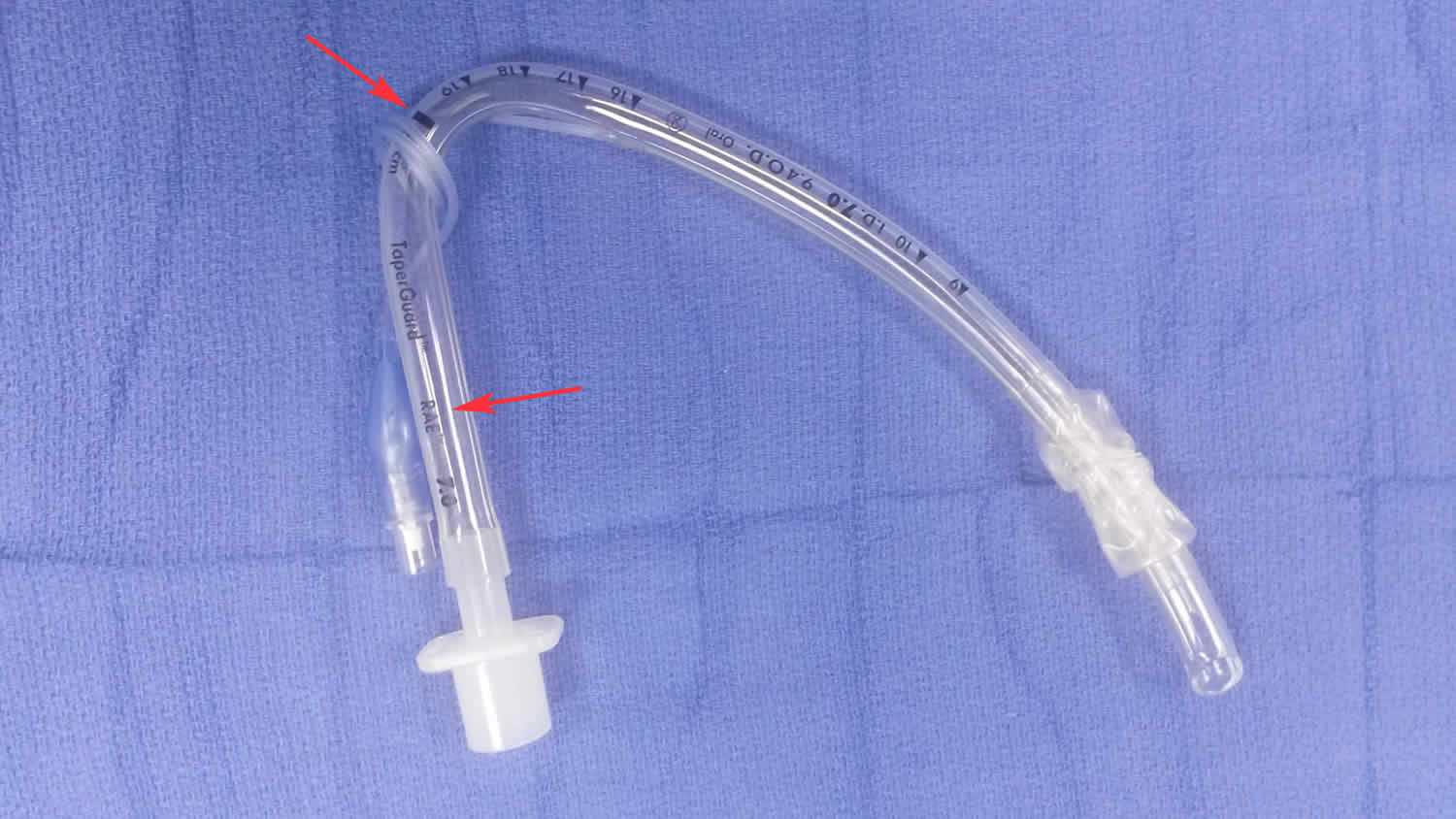
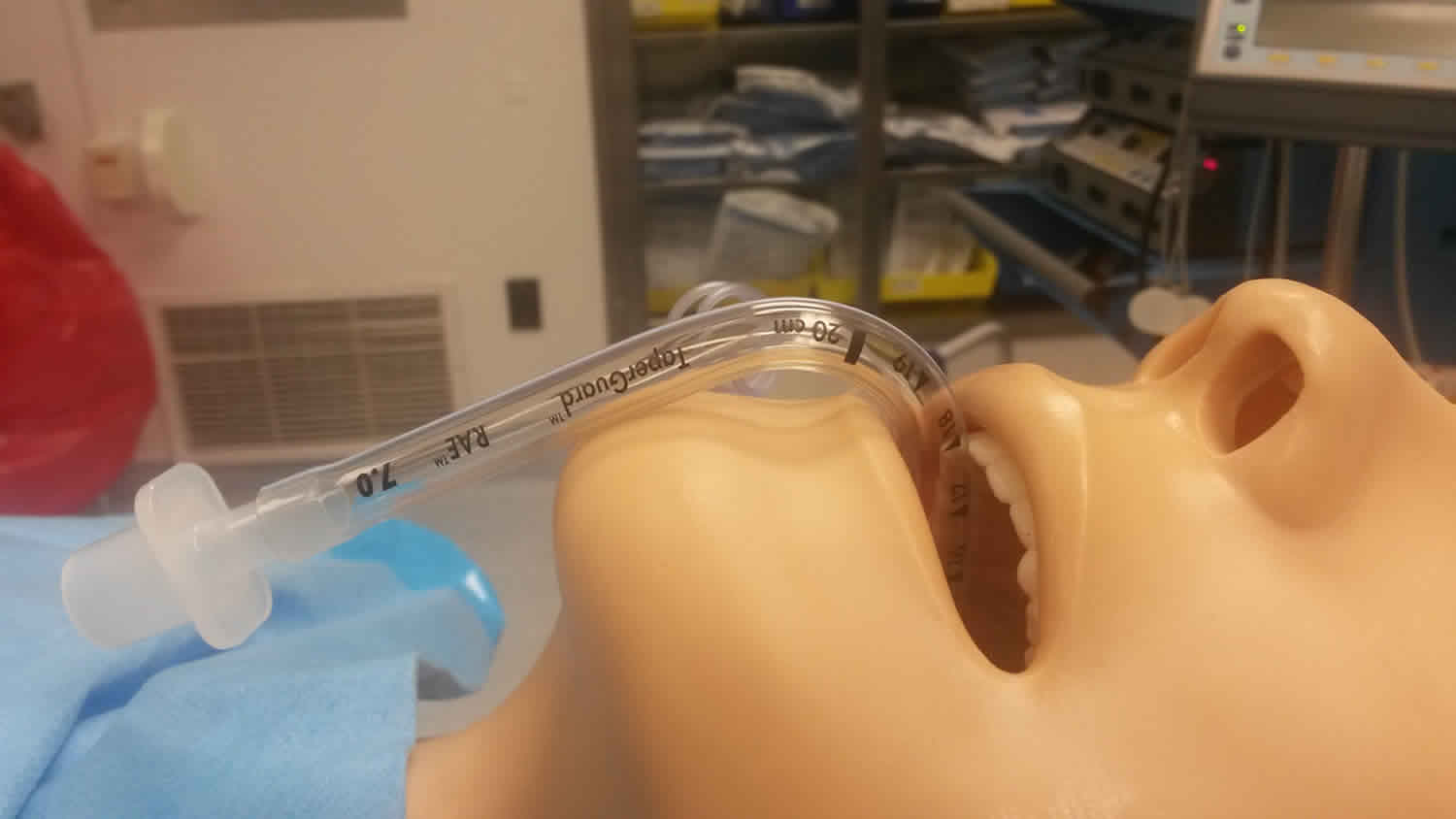
Figure 5. Nasal endotracheal tube (RAE tube)
Endotracheal intubation
Endotracheal intubation is a medical procedure in which a tube is placed into the windpipe (trachea) through the mouth or nose to provide an open airway. In most emergency situations, endotracheal intubation is placed through the mouth.
Whether you are awake (conscious) or not awake (unconscious), you will be given medicine to make it easier and more comfortable to insert the tube. You may also get medicine to relax.
Your doctor or emergency personnel will insert a device called a laryngoscope to be able to view the vocal cords and the upper part of the windpipe.
If the endotracheal intubation procedure is being done to help with breathing, a tube is then inserted into the windpipe and past the vocal cords to just above the spot above where the trachea branches into the lungs. The tube can then be used to connect with a mechanical ventilator to assist breathing.
Endotracheal intubation indication
Endotracheal intubation is done to:
- Keep the airway open in order to give oxygen, medicine, or anesthesia.
- Support breathing in certain illnesses, such as pneumonia, emphysema, heart failure, collapsed lung or severe trauma.
- Remove blockages from the airway.
- Allow the provider to get a better view of the upper airway.
- Protect the lungs in people who are unable to protect their airway and are at risk for breathing in fluid (aspiration). This includes people with certain types of strokes, overdoses, or massive bleeding from the esophagus or stomach.
Endotracheal intubation steps
Endotracheal intubation procedure is most often done in emergency situations, so there are no steps you can take to prepare.
Technique
Intubation technique may vary slightly depending on the operator and equipment used, but the following overarching principles should apply to all situations. The “P’s” of airway control and intubation have long been taught to help providers effectively and safely perform the procedure 3.
- Plan—providers should plan for the procedure and evaluate the environment to ensure the safety of patient and provider
- Preparation – the patient should be positioned as described above, all drugs, personal protective equipment, and instruments must be available. All providers should be understanding of and agreeable to the plan to intubate the patient, and how to best care for the patient post intubation. Use of a Broselow Tape is beneficial when treating pediatric patients to ensure appropriately sized equipment and medication doses.
- Protect – the cervical spine should be protected in the setting of trauma with an additional provider holding in-line stabilization.
- Preoxygenation—patients are typically provided high flow oxygen via a non-rebreather mask or ventilatory support with a BVM and supplemental oxygenation to prevent potential decompensation during laryngoscopy. These measures replace nitrogen in the airways with oxygen to create a reservoir for oxygen exchange during the procedure (Dunford). Apneic oxygenation via high flow nasal cannula may also be used to help maintain oxygen reserves during the peri-intubation period.
- Pretreatment—local protocols may call for the use of pretreatment medications to attenuate the physiologic response patients experience from intubation such as lidocaine to blunt the intracranial pressure response to laryngoscopy or atropine to offset bradycardia in pediatric patients. Studies have shown mostly equivocal findings in the OR for the use of premedication but no definitive evidence that it is beneficial in the prehospital setting 3.
- Local protocols set paralysis and Induction-indications and procedures to induce, sedate, or paralyze the patient and choice of medications available through medical direction. In general, agents with rapid onset and short durations are best to mitigate problems arising from a failed airway.
Placement with proof – Appropriate equipment and technique are utilized to place an endotracheal tube through the cords with direct visualization. ETCO2, chest rise and auscultation should all be used to confirm placement. - Postintubation management—Patients should be appropriately sedated after intubation to ensure comfort and safety per local protocols. Care must be made to avoid hypoxia, hypoventilation, and hyperventilation, all of which can be detrimental to long-term outcomes and mortality 4. Endotracheal tube CO2 monitoring with waveform capnography is the gold standard to ensure appropriate ventilation and continued evaluation of tube placement 5.
Adult
- Assess the patients airway for predictors of difficulty.
- Prepare all equipment to ensure rapid access if needed.
- Establish and verbalise an intubation plan.
- Test integrity of the cuff, pilot balloon and valve by confirming appropriate inflation/deflation prior to use.
- Lubricate the external surface of the endotracheal tube’s flexible distal tip with water-soluble lubricant.
- Elevate the patient’s head and place in the appropriate position to align the oral (OA), pharyngeal (PA) and laryngeal (LA) axes (neutral position with manual in-line stabilization (MILS) if cervical spine injury suspected).
- Open mouth and inspect oral cavity.
- Remove any dentures or removable plates from the mouth as required.
- Perform laryngoscopy.
- Suction as required.
- Consider laryngeal manipulation to optimize visualization of the larynx.
- Insert Frova intubating catheter.
- Whilst maintaining visualization of the larynx, request the airway assistant to place appropriately size endotracheal tube over the intubating catheter.
- Male: 8.0/9.0 mm
- Female: 7.0/8.0 mm
- Consider retraction of the corner of the patient’s mouth to optimize unobstructed passage of the endotracheal tube.
- Gently insert the endotracheal tube’s flexible distal tip through the vocal cords to position the vocal cords between the two (2) ring markers. If resistance is encountered, gently rotate the endotracheal tube anti-clockwise and attempt re-insertion.
- Male: 22–24 cm (at lips)
- Female: 20–22 cm (at lips)
- With right hand hold endotracheal tube firmly at the lips until correct placement (appropriate EtCO2 waveform) is confirmed and endotracheal tube is properly secured.
- Remove intubating catheter.
- Remove laryngoscope blade from mouth.
- Using a syringe, inflate the endotracheal tube cuff with the minimum amount of air required to provide an effective seal.
- Remove syringe from the endotracheal tube to effect the closing of the one-way valve, ensure pilot balloon remains inflated.
- Connect resuscitation bag and commence ventilation.
- Confirm correct tracheal placement by observing an appropriate continuous EtCO2 waveform (minimum of 6 ventilations of moderate tidal volume required for confirmation) and equal air entry.
- Secure endotracheal tube (cloth tie/commercial endotracheal tube holder) as appropriate.
- Consider insertion of bite block.
- Administer post intubation sedation as required (titrated aliquots of morphine/fentanyl and/or midazolam).
- Assess and adjust endotracheal tube cuff pressure as required.
Children
- Assess the patients airway for predictors of technical difficulty.
- Prepare all equipment to ensure rapid access if needed.
- Establish and verbalise an intubation plan.
- Test integrity of the cuff, pilot balloon and valve by confirming appropriate inflation/deflation prior to use.
- Lubricate the external surface of the endotracheal tube’s distal tip with water-soluble lubricant.
- Consider placing an intubating catheter in the endotracheal tube if the selected endotracheal tube internal diameter is ≥ 6mm)
- Position the patient in the optimal position to align the oral, pharyngeal and laryngeal axes (neutral position with manual in-line stabilization (MILS) if cervical spine injury suspected).
- Infant – slight elevation of the shoulders
- Small child – slight extension of the head
- Older child – extension of the head (elevation of the head may also be required). Open mouth and inspect oral cavity.
- Consider laryngeal manipulation to optimise visualization of the larynx.
- Whilst maintaining visualisation of the larynx, request the airway assistant to place appropriately sized endotracheal tube over the intubating catheter or place endotracheal tube directly into the larynx.
- Consider retraction of the corner of the patient’s mouth to optimize unobstructed passage of the endotracheal tube.
- Whilst maintaining visualisation of the larynx, gently insert the endotracheal tube’s distal tip through the cords to position the vocal cords at the ring marker.
- Neonate: 9.5 cm
- 6 months: 11 cm
- 1 year: size 12 cm
- > 1 year: age/2+12 cm
- If used, remove bougie.
- Remove laryngoscope blade from mouth.
- Connect resuscitation bag and commence ventilation.
- Confirm an audible air leak is present with cuff fully deflated.
- Using a syringe, inflate the endotracheal tube cuff to the effective sealing pressure but no higher than 20 cm H2O.
- Remove syringe from the endotracheal tube to effect the closing of the one-way valve, ensure pilot balloon remains inflated.
- Confirm correct placement by an appropriate continuous EtCO2 waveform (minimum of 6 ventilations of moderate tidal volume required for confirmation).
- Secure endotracheal tube (cloth tie/commercial endotracheal tube holder) as appropriate.
- Consider insertion of bite block.
- Administer post intubation sedation as required (titrated aliquots of morphine/fentanyl and/or midazolam).
- Assess and adjust endotracheal tube cuff pressure as required.
Infant and newborn
- Assess the patients airway for predictors of technical difficulty.
- Prepare all equipment to ensure rapid access if needed.
- Establish and verbalise an intubation plan.
- Lubricate the external surface of the endotracheal tube’s distal tip with water-soluble lubricant.
- Position the patient in the optimal position to align the oral, pharyngeal and laryngeal axes (neutral position with manual in-line stabilization (MILS) if cervical spine injury suspected).
- Consider laryngeal manipulation to optimise visualization of the larynx.
- Whilst maintaining visualisation of the larynx, place endotracheal tube directly into the larynx.
- Consider retraction of the corner of the patient’s mouth to optimise unobstructed passage of the endotracheal tube.
- Whilst maintaining visualisation of the larynx, gently insert the endotracheal tube’s distal tip through the cords to position the vocal cords at the ring marker.
- Whilst maintaining visualisation of the larynx, gently insert the endotracheal tube’s distal tip through the cords to position the vocal cords at the ring marker.
- Oral tube length (cm) = 6 + weight (kg)
- Remove laryngoscope blade from mouth.
- Connect resuscitation bag and commence ventilation.
- Confirm an audible air leak is present (cuff is to remain fully deflated).
- Confirm correct placement by an appropriate continuous EtCO2 waveform (minimum of 6 ventilations of moderate tidal volume required for confirmation).
- Secure endotracheal tube (cloth tie/commercial endotracheal tube holder) as appropriate.
Following this approach can mitigate potential problems and ensure a provider is enabled to respond to challenging situations if necessary. Proper preparation can also increase the likelihood of first-pass success. First-pass success is critical to help prevent many of the complications described below. Multiple attempts have been associated with an increased risk of intubation failure and complications 6. When using direct visualization technique or video laryngoscopy, there is no substitute for seeing the tube pass through the vocal cords to ensure proper placement. A provider must be well versed in the relevant anatomy of the larynx and posterior pharynx to obtain an adequate view of the patient’s airway. Exact technique varies with the laryngoscope blade choice, but a provider must control the tongue and epiglottis to visualize the vocal cords. The tongue is controlled by holding the laryngoscope in the provider’s left hand and sweeping it to the patient’s left. The epiglottis is controlled using the tip of the laryngoscope blade, directly when using a Miller blade or by inserting the blade tip into the vallecula when using a MAC blade, to expose the vocal cords. Once the cords are visualized, the endotracheal tube is inserted with the provider’s right hand until the balloon portion of the tube has just passed the vocal cords. The stylet is removed, the balloon inflated, and ventilation is provided using a resuscitation bag and reservoir. Placement is then confirmed with endotracheal tube CO2 colorimetric capnometry or monitored capnography, observing equal chest rise, and auscultation of all lung fields. Special care is taken to never “rock” the laryngoscope blade in an attempt to obtain a better view. The structures of the oropharynx and epiglottis are to be lifted up, in an anterior and caudal direction, to avoid damage to the teeth. Excessive force should be avoided as this could cause damage to the soft tissues as well. There will be times that direct laryngoscopy, or the use of the video laryngoscopy, will fail on the first attempt at intubation. A provider may have difficulty identifying the necessary anatomical landmarks, need to change equipment, or misplace the endotracheal tube. It is customary to allow repeated attempts, but it is generally considered a failed airway after three unsuccessful attempts 7. Providers should follow the guidance of their local protocols for the definition of a failed airway, the use of airway adjuncts, and the use of rescue devices. It is recommended that providers be skilled in bag valve mask ventilation as well as with the use of rescue supraglottic devices and surgical airways in the case of a failed airway 3. The most effective deterrents to a failed airway are proper training, experience, and practice 8. Numerous recommendations have been made for the best way to acquire and maintain competency with airway procedures, but there is no substitute for experience. The National Association of EMS Physicians (NAEMSP) provides consensus recommendations on the “ideal preparation for prehospital rapid sequence intubation” through its position statement and resource documentation on Drug-Assisted Intubation in the Prehospital Setting 3. Multiple studies have tried to identify the minimum experience required to become proficient with intubation and the necessary rate of use with the procedure to maintain competency. Anesthesia literature has reported that healthcare providers require 50 endotracheal intubations to reach a success rate of 90% 9. Wang et al. 10 found that a prehospital emergency personnel requires 4 to 12 endotracheal intubations a year to maintain competency. Such goals are difficult to reach for most prehospital providers because of a lack of quality operating room (OR) training time and exposure to field intubation in the clinical setting. Many emergency personnels only have the opportunity to perform a field intubation one time or less per year 10.
Endotracheal intubation complications
Endotracheal intubation complications include:
- Bleeding
- Infection
- Trauma to the voice box (larynx), thyroid gland, vocal cords and windpipe (trachea), or esophagus
- Puncture or tearing (perforation) of body parts in the chest cavity, leading to lung collapse
Nasal intubation
Nasotracheal intubation involves passing an endotracheal tube through the nose into the nasopharynx and the trachea; most commonly after induction of general anesthesia in the operating room. Nasotracheal intubation is a useful technique for patients undergoing intraoral surgery that has proven to be very safe and effective when used properly. Nasotracheal intubation is rarely performed in the emergency department but may be required in specific situations such as angioedema. Both blind and flexible nasal intubation may be utilized 11. The use of nasotracheal intubation permits administration of anesthetic gases without obfuscation of intraoral anatomy and is commonly used for procedures including dental, oropharyngeal and maxillofacial operations 12. Nasotracheal intubation is an essential skill for anesthesia providers. Due to the potential complications in performing nasotracheal intubation, it is recommended that nasotracheal intubation not be attempted by anyone who is not skilled at orotracheal intubation as well 13.
Nasal intubation indication
Indications for nasotracheal intubation include, but are not limited to the following:
- Intraoral and oropharyngeal surgery
- Complex intra-oral procedures involving mandibular reconstructive procedures
- Rigid laryngoscopy
- Dental surgery
- Maxillofacial or orthognathic surgery
Nasal intubation contraindications
Absolute nasotracheal intubation contraindications include:
- Suspected epiglottis
- Midface instability
- Previous history of old or recent skull base fractures
- Any known bleeding disorder that could predispose the patient to severe epistaxis
- Choanal atresia
- Patients that have experienced high-speed trauma or isolated facial trauma may have undiagnosed skull fractures that may result in nasotracheal tube placement into the brain. It is best to avoid nasotracheal intubation in these patients.
Relative contraindications include:
- Anything that could compromise the nasal air passage (large nasal polyps, foreign bodies)
- Recent nasal surgery
- History of frequent episodes of epistaxis
Nasal intubation steps
Equipment
Some of the necessary equipment needed to perform a nasotracheal intubation includes the following:
- Endotracheal tube (Nasal RAE or standard endotracheal tube)
- Lidocaine jelly or a water-soluble lubricant
- Magill forceps
- Laryngoscope
- Vasoconstricting nasal spray (oxymetazoline 0.05% or phenylephrine nose drops 0.25% to 1%)
- Syringe to inflate cuff
Preparation
A pre-anesthetic evaluation must be performed for each patient undergoing a procedure requiring anesthesia with a particular focus on identifying any potential risks or complications related to the upcoming procedure and composing an individualized plan for patient care. Often, the patient can relay important information regarding unilateral restriction or congestion and give some direction as to which side should be used for the nasotracheal intubation. If the patient interview does not yield information related to relative patency of one side versus the other, then either side of the nose may be used.
An anterior rhinoscopy may be performed (this is not a common practice) which gives the provider the ability to visualize the anterior portion of each nasal cavity. The main limitation of anterior rhinoscopy is the inability to provide any information regarding the posterior nasal cavity. To fully assess the pathway, a flexible fiber-optic bronchoscope may be passed into the nasopharynx 14.
Technique
Once the choice of laterality is determined, the provider may proceed with nasotracheal intubation. The first step to performing an nasotracheal intubation is a generous application of vasoconstricting spray bilaterally. Anesthetic topicalization may be applied via spray or by use of a lubricant that is impregnated with a local anesthetic.
After topicalization and application of vasoconstrictor, some practitioners advocate usage of a device to “dilate” the tissue, commonly a nasal airway. The necessity of dilation before intubation is a topic of debate in the anesthesiology community. Currently, only increased complications from repeated instrumentation of delicate structures. As of the time “dilation” is not a recommended practice 15.
Prior to intubation, the patient should be pre-oxygenated with FiO2 of 1.0 and ventilation assessed before muscle relaxant is administered.
It is important to lubricate the distal end of the nasotracheal tube, with the most common lubricants being either lidocaine or a plain, non-medicated water-soluble jelly.
After insertion into the nose, gentle pressure should be applied to advance the tube with the vector of force directed towards the posterior nasopharynx and the operating room table. Some manipulation will be required while placing the tube through the nasal cavity and some resistance will be encountered along the way.
If the amount of resistance felt is significant then the tube may be repositioned before attempting to advance further. A smaller-sized endotracheal tube may be needed if the anatomy cannot accommodate the passage. It is important to keep in mind that for the nasal RAE tube the diameter is proportional to the length of the tube so if a tube that is too small is chosen it may not advance far enough into the trachea for the balloon to be completely subglottic. Options include switching to a standard endotracheal tube, considering oropharyngeal intubation, or changing sides and approaching the contralateral nostril.
When the endotracheal tube has reached the posterior nasopharynx and passes the soft palate and into the oropharynx laryngoscopy will be performed, and Magill forceps used to advance the tube between the vocal cords and into the trachea. Once the endotracheal tube pilot balloon has passed the vocal cords and is inflated, the chest should be auscultated to confirm the positioning of the tube.
The position of the patient’s head should be noted during and after intubation with regards to the depth of the endotracheal tube. Flexion may advance the tube deeper into the trachea, which is usually of little clinical significance when using a nasal RAE since the likelihood of endobronchial intubation is low with an appropriately-sized tube. Perhaps more likely is the withdrawal of the tube with extension at the neck. If a relatively small tube is used for intubation, owing to a narrow nasal passage, the extension of the neck can force the balloon against the vocal cords and may lead to injury, balloon herniation or extubation.
The most common complication of nasotracheal intubation is epistaxis, which occurs with nearly every nasal intubation. Other complications include bacteremia (by introducing bacteria from the nasal cavity into the body due to trauma from the tube) and risk of perforation (retropharyngeal perforation or perforation of a piriform fossa). As mentioned previously, it is best to avoid nasal intubation in patients who have sustained high-speed trauma or isolated facial trauma due to the risk of inadvertent placement of the endotracheal tube into the brain.
Nasal intubation complications
The most common complication of nasotracheal intubation is epistaxis, which occurs with nearly every nasotracheal intubation. Other complications include bacteremia (by introducing bacteria from the nasal cavity into the body due to trauma from the tube) and risk of perforation (retropharyngeal perforation or perforation of a piriform fossa). As mentioned previously, it is best to avoid nasotracheal intubation in patients who have sustained high-speed trauma or isolated facial trauma due to the risk of inadvertent placement of the endotracheal tube into the brain.
References- Broderick ED, Reed JJ. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Feb 28, 2019. EMS, Pros And Cons Of Drug-Assisted Intubation
- Arslan Zİ, Türkyılmaz Z. Which nostril should be used for nasotracheal intubation with Airtraq NT®: the right or left? A randomized clinical trial. Turk J Med Sci. 2019 Feb 11;49(1):116-122.
- Wang HE, Davis DP, O’Connor RE, Domeier RM. Drug-assisted intubation in the prehospital setting (resource document to NAEMSP position statement). Prehosp Emerg Care. 2006 Apr-Jun;10(2):261-71
- Davis DP, Dunford JV, Poste JC, Ochs M, Holbrook T, Fortlage D, Size MJ, Kennedy F, Hoyt DB. The impact of hypoxia and hyperventilation on outcome after paramedic rapid sequence intubation of severely head-injured patients. J Trauma. 2004 Jul;57(1):1-8; discussion 8-10
- Davis DP, Dunford JV, Ochs M, Park K, Hoyt DB. The use of quantitative end-tidal capnometry to avoid inadvertent severe hyperventilation in patients with head injury after paramedic rapid sequence intubation. J Trauma. 2004 Apr;56(4):808-14
- Fouche PF, Stein C, Simpson P, Carlson JN, Doi SA. Nonphysician Out-of-Hospital Rapid Sequence Intubation Success and Adverse Events: A Systematic Review and Meta-Analysis. Ann Emerg Med. 2017 Oct;70(4):449-459.e20
- Wang HE, Lave JR, Sirio CA, Yealy DM. Paramedic intubation errors: isolated events or symptoms of larger problems? Health Aff (Millwood). 2006 Mar-Apr;25(2):501-9
- Bossers SM, Schwarte LA, Loer SA, Twisk JW, Boer C, Schober P. Experience in Prehospital Endotracheal Intubation Significantly Influences Mortality of Patients with Severe Traumatic Brain Injury: A Systematic Review and Meta-Analysis. PLoS ONE. 2015;10(10):e0141034
- Garza AG, Gratton MC, Coontz D, Noble E, Ma OJ. Effect of paramedic experience on orotracheal intubation success rates. J Emerg Med. 2003 Oct;25(3):251-6
- Wang HE, Balasubramani GK, Cook LJ, Lave JR, Yealy DM. Out-of-hospital endotracheal intubation experience and patient outcomes. Ann Emerg Med. 2010 Jun;55(6):527-537.e6
- Flexible nasotracheal intubation compared to blind nasotracheal intubation in the setting of simulated angioedema. Am J Emerg Med. 2019 Feb 11. pii: S0735-6757(19)30090-7. doi: 10.1016/j.ajem.2019.02.012. [Epub ahead of print] https://www.ncbi.nlm.nih.gov/pubmed/30772130
- Özkan ASM, Akbas S, Toy E, Durmus M. North Polar Tube Reduces the Risk of Epistaxis during Nasotracheal Intubation: A prospective, Randomized Clinical Trial. Curr Ther Res Clin Exp. 2019;90:21-26
- Parkey S, Erickson T, Hayden EM, Brown Iii CA, Carlson JN. Flexible nasotracheal intubation compared to blind nasotracheal intubation in the setting of simulated angioedema. Am J Emerg Med. 2019 Feb 11
- Yoo JY, Chae YJ, Lee YB, Kim S, Lee J, Kim DH. A comparison of the Macintosh laryngoscope, McGrath video laryngoscope, and Pentax Airway Scope in paediatric nasotracheal intubation. Sci Rep. 2018 Nov 26;8(1):17365
- Folino TB, Parks LJ. Nasotracheal Intubation. [Updated 2019 Mar 18]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK499967





{kind=link}